
Abstract
Objective
To study the efficacy and safety profile of ketorolac in cleft palate surgery.
Design
Retrospective analysis of patients who underwent primary cleft palate surgery and received either postoperative ketorolac or opioids.
Setting
Tertiary care children's hospital.
Patients, Participants
Eighty-nine patients enrolled who were all younger than 36 months of age, not dependent on a gastrostomy tube, with no history of bleeding disorders, and had undergone their primary cleft palate procedure by one specific surgeon between January 2010 and June 2019.
Interventions
n/a.
Main Outcome Measure
Morphine equivalent dose (MED), Face, Legs, Activity, Cry, Consolability (FLACC) score, length of stay (LOS), total oral intake (mL), total oral intake/LOS, and postoperative adverse events between ketorolac and no ketorolac groups.
Results
MED, FLACC score, and LOS were significantly lower in the ketorolac group compared to the no ketorolac group. One patient in the ketorolac group had a bleeding event.
Conclusions
Use of ketorolac significantly decreased narcotic usage and pain scores as reported by the FLACC score. Moreover, postoperative bleeding was rare in both ketorolac and no ketorolac groups.
Introduction
Cleft palate is one of the most common congenital malformations (Wantia and Rettinger, 2002). Priorities of patient safety and sufficient pain control are of utmost importance during repair, as the patient's airway and digestive tract are both altered. Common postoperative challenges for these patients include pain control and an efficient return to baseline oral intake. Opioids have traditionally been used postoperatively, but they have known adverse effects, including postoperative nausea and vomiting, oversedation, and respiratory depression (Reena et al., 2016). In the setting of the current opioid abuse epidemic, ketorolac has become a favorable non-narcotic alternative for pain control.
Over the past decade, the utility of ketorolac in the management of acute perioperative pediatric pain has expanded (American Society of Anesthesiologists Task Force on Acute Pain Management, 2012). Peer-reviewed evidence supports the efficacy and safety profile of ketorolac down to infancy, inclusive of those patients less than 6 months of age in select populations (Jalkut, 2014). Some providers prefer to avoid the use of ketorolac when postoperative bleeding is a concern as ketorolac theoretically increases bleeding risk by inhibiting platelet function (Brasher et al., 2014).
Prior studies have looked at ketorolac use and the risk of bleeding following other types of surgeries. A meta-analysis by Chan and Parikh (2014) identified an increased risk of bleeding after tonsillectomy in adults, but not in children. Gobble et al. (2014) published a meta-analysis that investigated 27 double-blinded randomized control trials analyzing surgical procedures ranging from cholecystectomy to tonsillectomy to hysterectomy. They found that postoperative bleeding was not significantly increased with ketorolac compared with controls, and that adverse effects were not statistically different between the groups. Pain control was also found to be superior with ketorolac compared with controls.
The plastic surgery literature has limited evidence regarding outcomes following postoperative NSAID use, especially with ketorolac. Stephens et al. (2015) conducted a review of the drug's safety and found that the rate of postoperative hematomas in 115 aesthetic facial procedures that used ketorolac was equivalent to the control group. That review also showed a reduction in postoperative narcotic use and improved pain scores within ketorolac study groups. A systematic review and meta-analysis by Kelley et al. (2016) stated that ibuprofen provides equivalent pain control to narcotics with no increased risk of bleeding. Hush et al. (2019) was the only study found that specifically investigated cleft palate surgery. They compared the effects of an opioid based postoperative protocol to a multimodal pain protocol that included one dose of perioperative ketorolac in addition to local nerve blocks, gabapentin, and other modalities. It found no increased bleeding events among the 50 patients in the multimodal ketorolac group. Stein et al. (2021) was the only article we found that attempted to examine the effects of ketorolac on postoperative pain control after cleft palate surgery. They found that a single dose of IV ketorolac after a primary palatoplasty was safe and effective, as no significant postop hemorrhage occurred and Face, Legs, Activity, Cry, Consolability (FLACC) scores were similar between groups. However, because their study had limitations in directly observing analgesic benefits, and the importance of this topic that deserves more attention, we designed this retrospective control study.
At our tertiary children's hospital, one of the surgeons who performs the majority of the cleft palate surgeries routinely used opioids to manage postoperative pain. In 2015, however, she began utilizing ketorolac and acetaminophen in order to decrease opioid use. We designed a retrospective review to compare postoperative course and outcomes between two groups of patients operated on by this single surgeon: patients who received IV ketorolac and those who did not. Specifically, we will compare narcotic and other analgesic use, oral intake, hospital length of stay, and any adverse events related to surgery, especially bleeding.
Methods
Data Source
This study was approved by the appropriate institutional review board prior to data collection. All patients who underwent primary cleft palate surgery at a tertiary care children's hospital by one cleft surgery-trained ENT surgeon between January 2010 and June 2019 were identified. Patients over the age of 36 months, with bleeding disorders, undergoing revision surgeries, and/or who were g-tube dependent, were excluded. Patients who had g-tubes were excluded due to the inability to consistently measure oral intake. Patient charts were retrospectively reviewed to gather all data. Initial data collected included patient demographics, comorbidities including documented chromosomal and cardiac anomalies, patient weight, specific surgical approach, intraoperative/postoperative analgesics administered, and patient outcomes, including any adverse events.
Ketorolac Versus Nonketorolac Groups
Patients were divided into either the ketorolac or nonketorolac group based on the ordered postoperative pain regimen. Patients who underwent surgery between January 2010 and December 2014 were in the nonketorolac group while patients who underwent surgery from January 2015 to June 2019 were in the ketorolac group. Pain control protocols are summarized in the flowchart of Figure 1. Patients in both groups received IV Morphine as needed in the postanesthesia care unit (PACU) following surgery. However, in the ketorolac group, patients received one dose of IV ketorolac intraoperatively followed by IV ketorolac scheduled every 6 h until they could tolerate oral (PO) intake; at this point, IV ketorolac was changed to oral ibuprofen until patient discharge. PO acetaminophen was alternated with NSAID therapy.
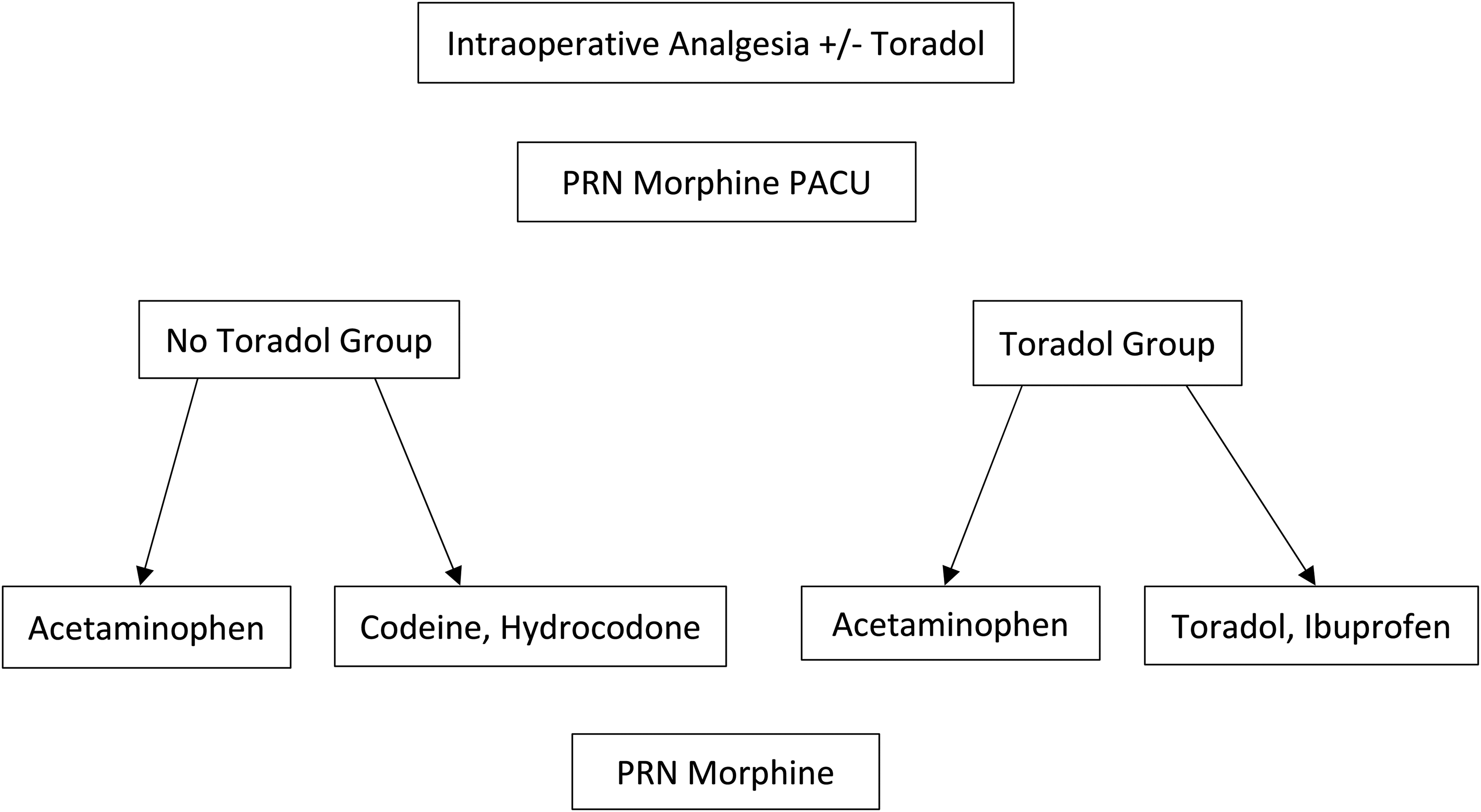
Study method—a breakdown of how patients’ pain was treated intraoperatively, in the PACU, and postoperatively based on which study group they were assigned to (ketorolac or nonketorolac).
In the nonketorolac group, there was more variability to the exact regimen used. Patients received an opiate intraoperatively followed by acetaminophen and additional opiates (Hydrocodone, codeine, or Morphine) as needed postoperatively. The nonketorolac group did not receive any NSAIDs. All procedures were performed by the same surgeon, an otolaryngologist trained in cleft surgery.
Outcome Measurements
Variables recorded for each patient included total narcotic usage, total postoperative oral intake in milliliters, hospital length of stay in hours (LOS), total postoperative oral intake divided by length of stay (mL/h), and total FLACC pain score during hospitalization. To determine total narcotic usage, we converted all types of narcotics to their morphine equivalent doses (MEDs). Doing this allowed us to maintain a standardized variable despite the use of different drugs. Oral intake was analyzed for each postoperative day and added together to determine the total. LOS was recorded as the number of hours between the time of initial hospitalization to time of discharge. To account for the variability of oral intake based on how long patients were hospitalized, we divided total oral intake by total length of stay to more accurately compare patients. The FLACC score is a method of assessing pain for children between the ages of 2 months and 7 years, or for those patients unable to communicate their pain. The acronym stands for Face, Legs, Activity, Cry, Consolability (FLACC) and the subjective score ranges from 0 to 10 with 0 being no pain. These numbers were reported by the nursing staff every 8 h and were summed to give a total score for each patient's hospitalization. We also gathered data on any adverse events that were reported within the first 60 postoperative days including postoperative bleeding and readmissions.
Statistical Analysis
We used SAS statistical software to perform all statistical analyses of our data. After calculating the average and standard deviations of reported continuous variables, we compared the two groups with a t-test and a Mann-Whitney U test and set a P-value threshold of .05.
Results
Demographics and Characteristics
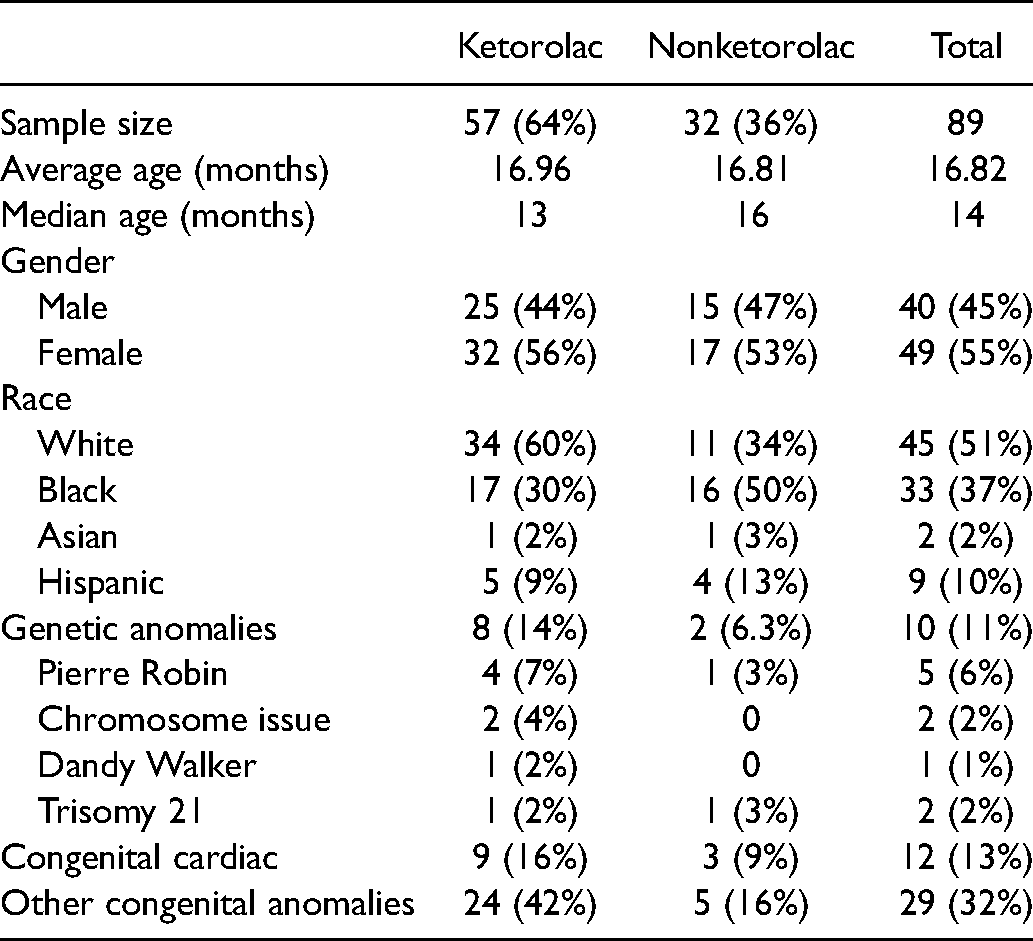
From January 2010 to June 2019, a total of 89 patients underwent primary cleft palate repair after exclusions with an average age of 16 months. Males encompassed 45% of the cohort. The majority of the cohort was White (51%), followed by Black, Hispanic, and Asian. Of the total 89 patients, 57 were included in the ketorolac group and 32 were included in the nonketorolac group. Genetic syndromes were present in 10 (11%) patients, congenital cardiac abnormalities were present in 12 (14%), and other congenital anomalies (not including cardiac) were present in 29 (33%). A breakdown of gender, race, age, and comorbid conditions between groups can be seen in Table 1.
Patient Demographics and Comorbidities.
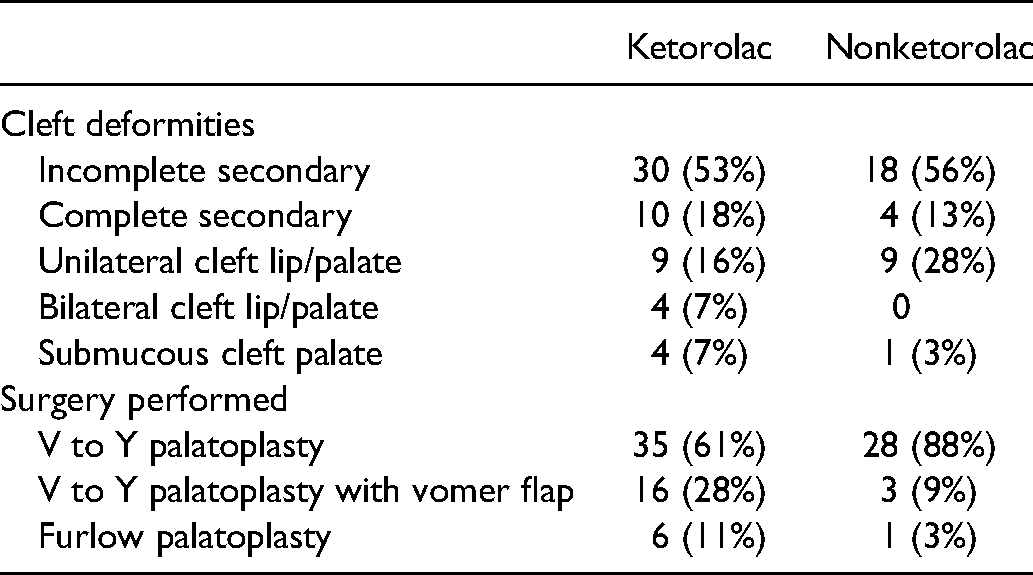
The most common cleft deformity in our patient sample was incomplete secondary cleft palate (54%), followed by unilateral cleft lip/palate (20%), then complete secondary (16%), then submucous cleft palate (6%), and bilateral cleft lip/palate (4%). Appropriate cleft lip surgery was performed on all cleft lip patients before cleft palate surgery.
One surgeon performed all surgeries, employing three different techniques, as exhibited in Table 2. Sixty-three (71%) patients underwent v to y palatoplasty, 19 (21%) had v to y palatoplasty with vomer flap, and 7 (8%) underwent Furlow palatoplasty.
Cleft Deformity and Palate Surgery Technique by Study Group.
We documented concurrent procedures done at the time of cleft palate surgery since these could have an impact on postoperative pain. These are shown in Table 3. Pressure equalization (PE) tube placement was the most common concurrent procedure, followed by circumcision.
Concurrent Procedures by Study Group.
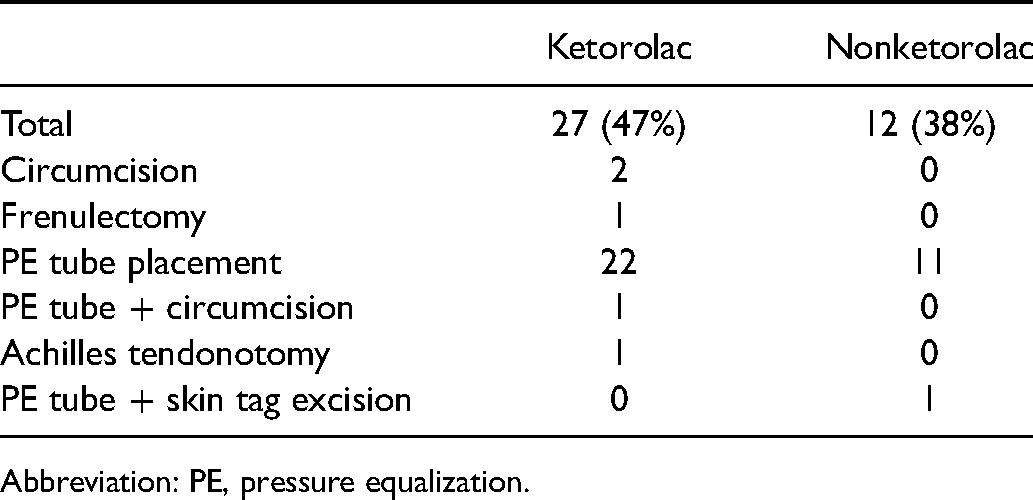
Abbreviation: PE, pressure equalization.
Outcomes Between Ketorolac Versus Nonketorolac Groups
Our primary outcomes between groups are described in Table 4. The average total FLACC pain score was lower in the ketorolac versus the nonketorolac group at 26 versus 42 (p < 0.001). The average MED in patients in the ketorolac group was 1.4 mg compared to 10.6 mg in the nonketorolac group (P < .0001). The ketorolac group demonstrated a slightly shorter LOS compared to the nonketorolac group (69 vs 78 h), although this was not statistically significant. Total oral intake was slightly greater in the nonketorolac group compared to the ketorolac group; however, when accounting for the variability in LOS, the total oral intake per hour in the hospital was similar (17 vs 19 mL/h). Neither of these differences in oral intake demonstrated statistically significant variance.
Primary Outcomes and Statistical Values Between Study Groups.

Abbreviation: LOS, length of stay.
Adverse Events
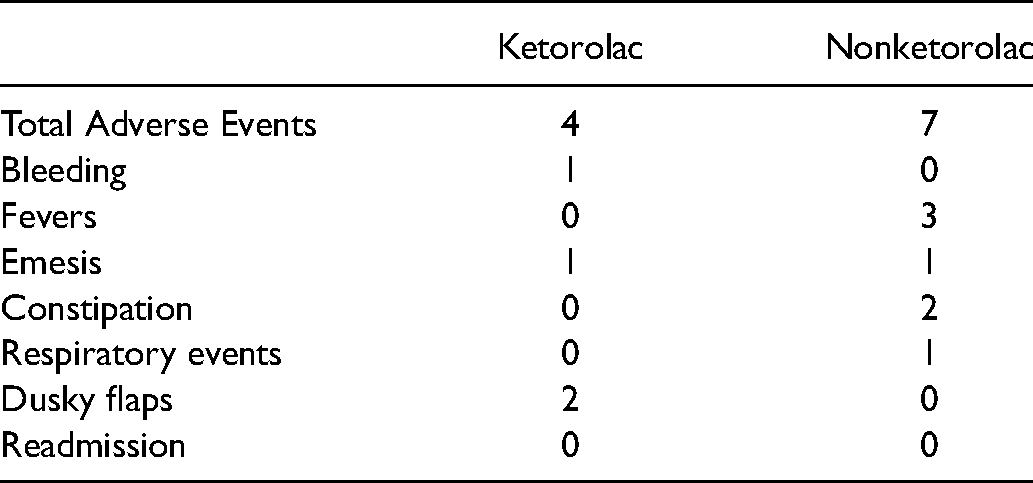
A total of four adverse events occurred in the ketorolac group compared to seven in the nonketorolac group, as described in Table 5. There was one case of postoperative bleeding in the ketorolac group, compared to none in the nonketorolac group. Additional complications in the ketorolac group included one case of emesis and two dusky flaps (slight venous congestion of the flaps whose only clinical consequence was a prolonged hospital stay to ensure flap viability.) In the nonketorolac group, there were three cases of postoperative fever, one case of emesis, two cases of constipation, and one respiratory complication. This respiratory complication involved significant postoperative tongue edema that required intubation for 4 days after surgery to guarantee a safe airway. There was no reported incidence of complications from respiratory depression in either group.
Adverse Events by Study Group.
Discussion
Overall, there is limited evidence on the safety and efficacy of intravenous ketorolac in pediatric plastic surgery procedures, and more specifically, in cleft palate surgery. In a surgical procedure where pain control, airway management, respiratory drive, and swallowing function are all major factors in the postoperative course, alternatives to a traditional opioid approach are highly valued. In our experience, the concern for an increased risk of postoperative hemorrhage has created reluctance toward the widespread use of ketorolac and other NSAIDs after cleft palate surgery. For this reason, we created this retrospective study to examine the safety and efficacy of ketorolac on postoperative pain control after cleft palate surgery.
Our study demonstrated a statistically significant decrease in narcotic usage for patients who were treated with ketorolac compared to those who were not. Both patient cohorts were prescribed as-needed opioid medications in the PACU. The nonketorolac group patients were managed with scheduled Tylenol and varied opioids, including codeine, hydrocodone, morphine, and hydromorphone. The ketorolac group patients were treated intraoperatively with a dose of IV ketorolac that continued as scheduled until they were able to tolerate PO ibuprofen, usually around POD1-3; they were also treated with Tylenol and as-needed morphine for break-through pain. We totaled the doses of opioid medications given throughout the hospitalization for all patients and found that the ketorolac group's MED average (in milligrams) was 1.4 compared to 10.6 in the no ketorolac group. This reached statistical significance with a P-value of <.001. A similar study investigating a single IV dose of ketorolac following their procedure (Stein et al., 2021) did not find this significant decrease in narcotic usage. This could be related to the difference in intervention protocols, as our study administered IV ketorolac intraoperatively and postoperatively and their protocol involved administration of a single dose of IV ketorolac postop. One can imagine the benefits of decreased narcotic usage in infants in general, but especially in those who have recently undergone upper airway surgery. Due to the retrospective nature of the study, we were unable to fully capture the expected benefits of decreased narcotic usage. As shown in the adverse event data (Table 5), two patients in the nonketorolac group had a prolonged hospitalization for constipation, a known side effect of opioids, as opposed to no patients in the ketorolac group. There were no documented events of decreased respiratory drive in either group; there was one patient in the no ketorolac group who had postoperative tongue edema requiring prolonged intubation, but none of the feared respiratory complications of opioid use were captured in this patient cohort.
Pain scores recorded by nursing staff as FLACC score were significantly decreased in the ketorolac group. As explained in the results section, FLACC stands for face, legs, activity, cry, and consolability which is a subjective method of assessing pain for children between the ages of 2 months and 7 years that ranges from 0 to 10 with 0 being no pain. This score was reported by the nursing staff every 8 h and all scores were added up to give a total score for each patient's hospitalization. Merkel et al. (1997) showed the FLACC scale to have a high interrater reliability and to be a valid pain assessment tool. The average total FLACC score for the nonketorolac cohort was significantly higher [42] than the ketorolac group [26], with a P-value <.001. There is a possibility of chronological bias as the nonketorolac patients were treated between 2010 and 2015, whereas the ketorolac patients were treated more recently between 2015 and 2019. Although there is no clear cause for bias in the way the FLACC score would be recorded differently during those two time periods, it is possible nurses may have received different training or instruction to influence the assessment and documentation of these scores. However, it is also possible that this result indicates decreased pain during hospitalization in the infants of the ketorolac group compared to those in the nonketorolac group. Stein et al. (2021) also used the FLACC score to evaluate ketorolac's analgesic efficacy and found no significant difference between the groups. Again, this score is difficult to compare across institutions, or even time periods, because of its inherent subjectivity. Their study required nurses to check more often, every 15 min in the first postoperative hour, and once every hour afterwards. The less frequent checks from our study could have given the patient more time to recover and allowed the ketorolac analgesic effects to set in.
We were surprised to note that there was no difference in oral intake recorded between the two groups. We expected that decreased pain would correlate with increased oral intake. We looked at oral intake as a total recorded during the hospitalization (mL) and as total divided by length of stay (mL/h). Neither of these measures showed a significant difference between our two cohorts. This outcome was dependent on oral intake as recorded by the bedside RN on the med/surg floor, and thus may not be the most reliable measure.
In addition, the LOS was decreased in the ketorolac group, but not to a statistically significant degree. We expected that the group with superior pain management would exhibit a decreased length of stay with an accelerated discharge date. Our results demonstrated an average LOS of 69 h in the ketorolac group compared to 78 h in the nonketorolac group with a P-value of .25. Decisions for discharging the patient are made by physician assessment and family readiness; both of which are based on multiple factors such as oral intake, pain control, and overall health of the infant. Again, there is the possibility of chronological bias due to the differing time periods of treatment of our two groups. Overall, management decisions may have subconsciously evolved over time with the surgeon who oversaw the timing of discharge planning. In addition, our study suffers from a limited sample size due to its retrospective nature. If the patient sample size were increased, this number may have reached statistical significance.
Another purpose of our study was to examine the safety of ketorolac by measuring adverse events. Postoperative bleeding events were very rare in all patients of our study with only one patient having a documented bleeding event. This patient was a 19-month-old female with unilateral cleft lip and palate who underwent v-y palatoplasty and vomer flap in 2016. Although the patient had multiple congenital anomalies including microcephaly, patent foramen ovale, dysmorphic facies, clinodactyly along with cleft lip and palate, she had no documented history of easy bleeding, abnormal coagulation labs, or platelet dysfunction. The patient received intraoperative ketorolac and about 15 min after completion of the surgery, the patient was noted to have bleeding from her mouth in the postanesthesia care unit. Bleeding was visualized at the roof of mouth on the right side and did not stop with the application of Afrin-soaked gauze, which required a return to the operating from for an exam under anesthesia. No active hemorrhage was identified so the mouth was irrigated and Surgicel was applied to the right lateral margin of the repair. There were no other documented bleeding events in either patient cohort. Because bleeding is such a rare event in cleft palate surgery, a larger sample size would be required to prove any significant difference between the ketorolac and nonketorolac groups. The Stein et al. (2021) study also found no differences in bleeding between their ketorolac and nonketorolac groups. Our results add further evidence to support the safety of ketorolac use in cleft palate surgery.
Conclusion
In conclusion, ketorolac can be safely given for postoperative pain management in primary cleft palate surgery. It decreases length of stay, significantly decreases use of narcotics, and significantly decreases patient pain as measured by nursing staff.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.