
Abstract
Background
Adverse airway events (AAEs) are rare but devastating complications following palatoplasty. The purpose of this study is to evaluate patient risk factors for their effect on these complications. We hypothesize that prolonged operative time and the presence of multiple medical comorbidities are risk factors for AAEs.
Design
Retrospective cohort study.
Setting
Participant hospitals in the Pediatric American College of Surgeons National Surgical Quality Improvement Program year 2016–2019.
Patients
Cases of palatoplasty in children under 3 years of age.
Outcomes
Adverse airway events including postoperative reintubation or any requirement of postoperative mechanical ventilation.
Results
A total of 6668 patients met inclusion criteria. The median operative time was 126 min (IQR 82). AAEs were identified in 107 (1.6%) patients. The incidence of risk factors was found to increase with age and AAEs were more prevalent in younger and older patients. Although patients in the older age groups had significantly higher burden of comorbidities, differences in age were not independently associated with AAEs. Following multivariable logistic regressions, operative times greater than 2 h, ASA class ≥3, >3 medical comorbidities, and black race were found to be significant independent risk factors.
Conclusions
In this large, retrospective database study in palatoplasty, increased operative time, ASA classification ≥3, multiple comorbidities, and black race were independently associated with AAEs.
Introduction
Cleft palate is an uncommon congenital defect with an incidence of 1 per 1594 live births in the United States. 1 Cleft palate occurs in conjunction with cleft lip in 6.64 per 10 000 live births. 2 Untreated cleft palate can have a detrimental impact on speech development, hearing, and feeding, and may negatively affect a child's livelihood due to the ensuing speech difficulties as well as the cosmetic deformity compared to peers.3,4 Cleft palate severity can be classified using the Veau system, from being limited to the soft palate only (Veau I) to a complete bilateral cleft (Veau IV), and there are different surgical approaches to each. 4 While there are multiple techniques for repair, cleft palate repair is typically performed around twelve months of age with a low incidence of complication.5–7 However, complications following repair do occur and can be severe. These can include wound dehiscence, palatal fistula, bleeding, infections, velopharyngeal insufficiency, and airway complications.8–13 Awareness of potential patient and case-based risk factors can alert providers to prepare with prophylactic and therapeutic measures in higher risk children undergoing repair. Previously published studies have examined the impact of cleft severity based on Veau classification, operative time, staging, and operative technique, among other factors.14–19 However the risk factors surrounding short-term airway complications following repair remains unclear. Prior single-institution studies have examined these complications, but these have been limited in power and scope.
Using a large national pediatric surgical database, this study aims to identify potential risk factors for adverse airway events in the short-term (30-day) period following cleft palate repair, with an emphasis on clarifying differences in age, operative time, and burden of comorbid conditions and their impact on the occurrence of airway complications.
Methods
Study Design
For this retrospective cohort study, we used the American College of Surgeons Pediatric National Surgical Quality Improvement Program (NSQIP-P) database for procedures between 2016 to 2019. Data from a total of 120 centers were included.
Study Sample
From the NSQIP-P database, we included pediatric patients under 3 years of age undergoing cleft palate repair as identified by Current Procedural Terminology (CPT) codes 42 200 (Palatoplasty for cleft palate, soft and/or hard palate only), 42 205 (Palatoplasty for cleft palate, with closure of alveolar ridge; soft tissue only), 42 220 (Palatoplasty for cleft palate, secondary lengthening procedure), and 42 235 (Repair of anterior palate, including vomer flap).
Study Variables
The NSQIP-P tracks individual short-term adverse events which occur within 30 postoperative days. The primary outcome is to determine the incidence and risk factors associated with any adverse airway event (AAE), as defined by the need for postoperative reintubation, or any requirement of postoperative mechanical ventilation. These two conditions are listed as separate variables in the NSQIP-P and were combined into a single outcome variable in our study.
The primary predictor variable was total operative time in minutes, and operative time was stratified into short (0–2 h), intermediate (2–3 h), and long (greater than 3 h). The database also collects information about other medical comorbidities such as existing seizure disorder, any hematologic disorder, or structural CNS disorder. These comorbidities were grouped into larger system-based comorbidity groups. Additionally, the total burden of medical comorbidities was assessed as a risk factor by grouping into 1, 2–3, or >3 total medical comorbidities. Other variables included in the NSQIP-P were patient demographics including age, gender, race, and American Society of Anesthesiologists (ASA) class and these were also analyzed as potential secondary predictors. Patients were also stratified into age groups of <10 months, 10–14 months, and >14 months to assess for any potential effect of age. Due to a lack of sufficient reporting in the dataset, Veau classification was not included in the analysis.
Data Collection and Analysis
Two-tailed t-tests, Chi-square tests followed by post-hoc Bonferroni correction, and multivariate logistic regression analyses were used for statistical analysis. Statistical analysis was performed using SPSS (IBM Corp. Released 2020. IBM SPSS Statistics Version 27.0. Armonk, NY, USA). Descriptive statistics including frequency of AAEs were extracted from the dataset. Univariate analyses were used to determine if the patient's demographic characteristics, length of operation time, and grouped comorbidities were risk factors for AAEs. The effect of concurrent procedures was determined with a two-tailed t-test. Following univariate analysis, any variable with a P value < .20 was chosen for inclusion in a multivariable logistic regression model. Significance in the multivariate logistic regression model was set at P < .05.
Results
A total of 6668 cases were included from the 2016–2019 NSQIP-P dataset. The average age of all patients was 405.6 ± 157.5 days (13.3 ± 5.2 months). A summary of patient demographics can be found in Table 1. A total of 107 (1.6%) patients experienced an AAE. An American Society of Anesthesiologists (ASA) classification greater than 3 was found in 1121 (18.3%) patients compared to ASA 1 or 2 in 5437 (81.5%) patients. Ten patients were not assigned an ASA class and, therefore, were not included in analyses involving the ASA class variable.
Demographics, Case Attributes, and Risk Factors for the Overall Study Population and in Cases with or Without AAEs.
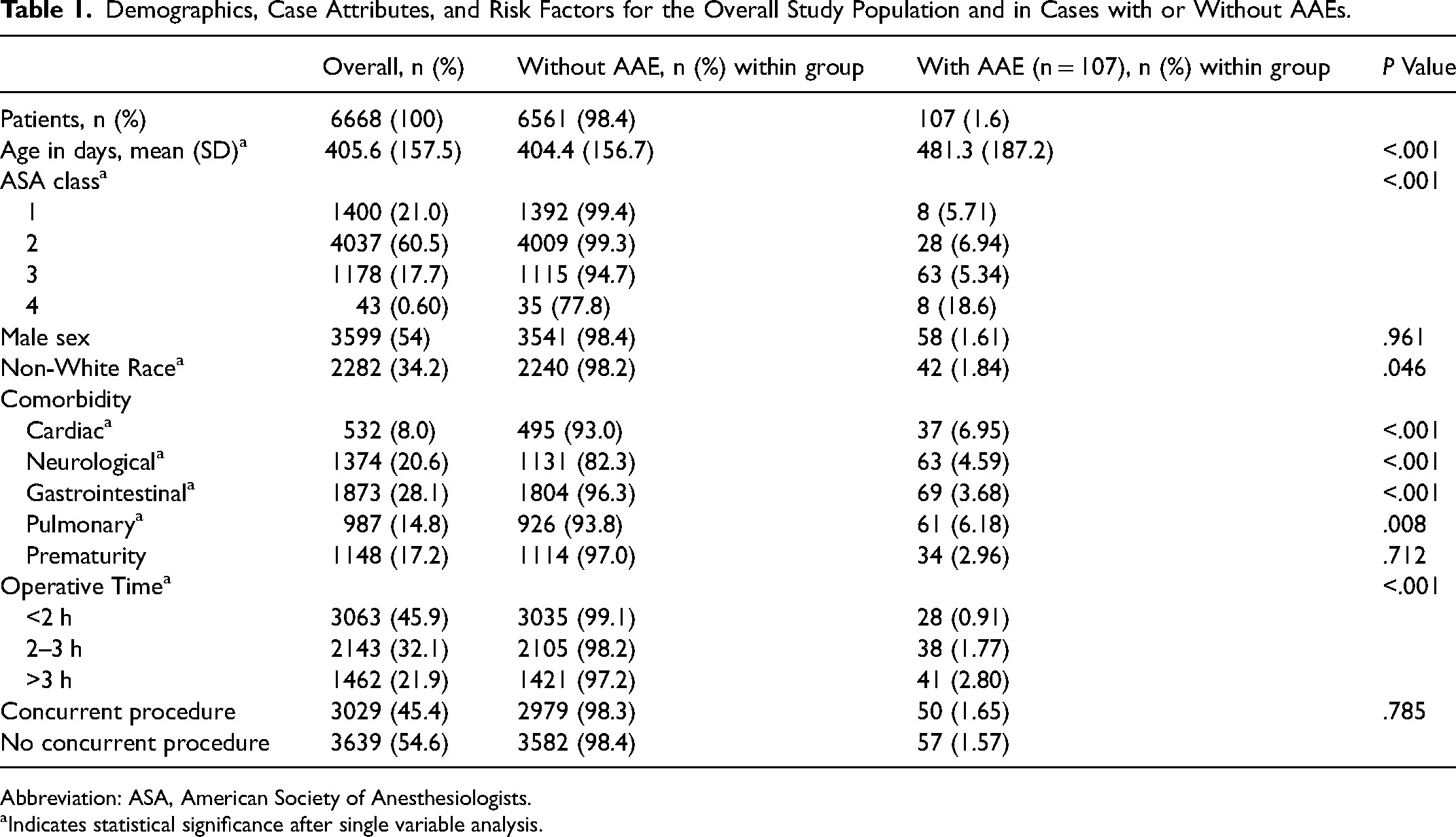
Abbreviation: ASA, American Society of Anesthesiologists.
Indicates statistical significance after single variable analysis.
Total numbers of the different patient comorbidities can be found in Table 1. Gastrointestinal comorbidities were the most frequent in 1873 (28.1%) of patients. The distribution of the comorbidity burden by age groups can be seen in Table 2.
Distribution of Risk Factors Stratified by age Groups <10 Months, 10–14 Months, and >14 Months of age.
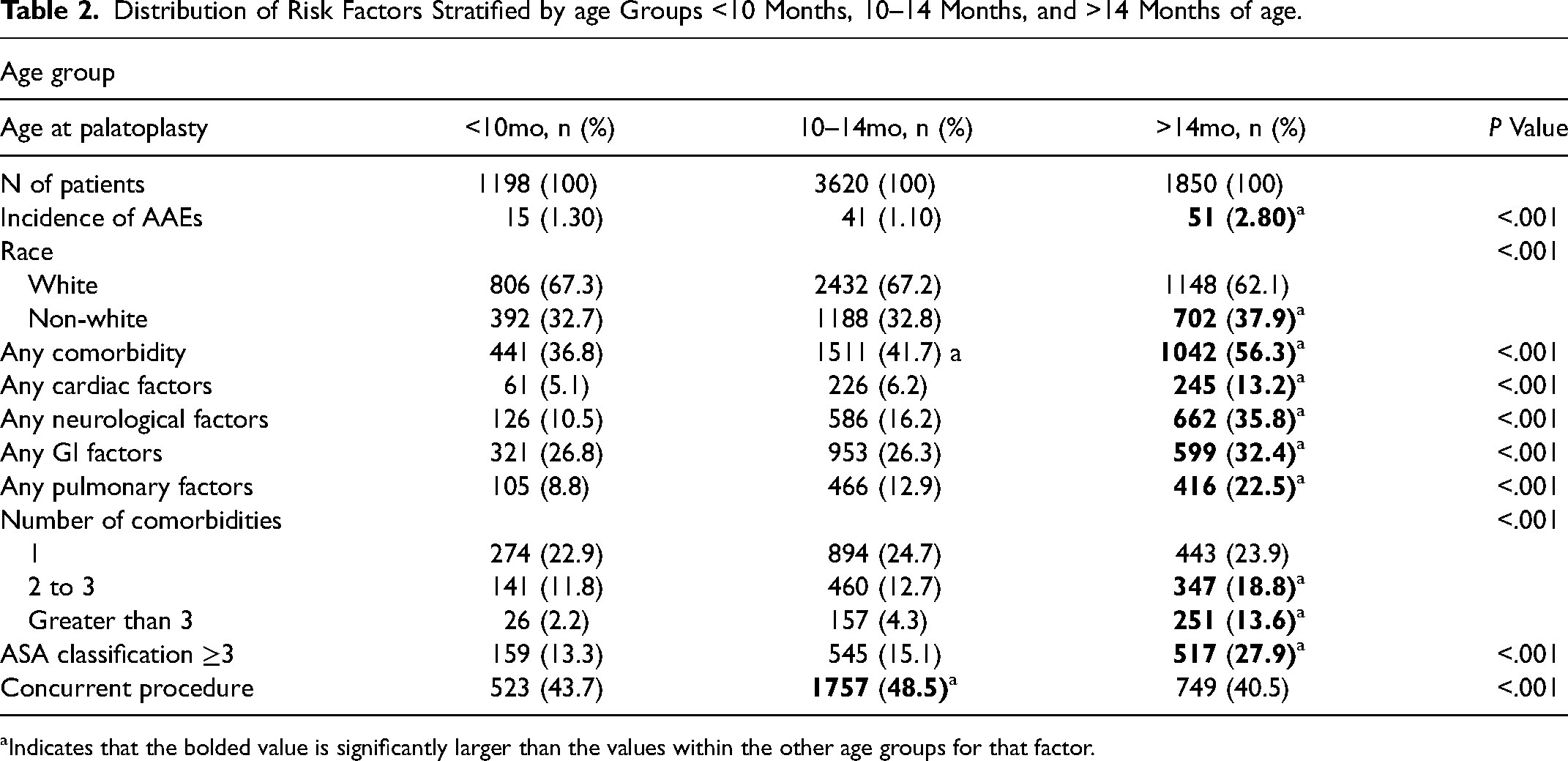
Indicates that the bolded value is significantly larger than the values within the other age groups for that factor.
Stratifications of operative times can also be found in Table 1. The overall median operative time was 126 min (IQR 82) (Figure 1). Operative times were the shortest in cases with a duration of less than two hours (45.9%), followed by intermediate (32.1%). Longer operative times greater than three hours were the least common (21.9%). AAE rates were the lowest after shorter operative times at 0.91%, 1.77% after intermediate operative times, and 2.8% of patients after longer operative times (P < .001).
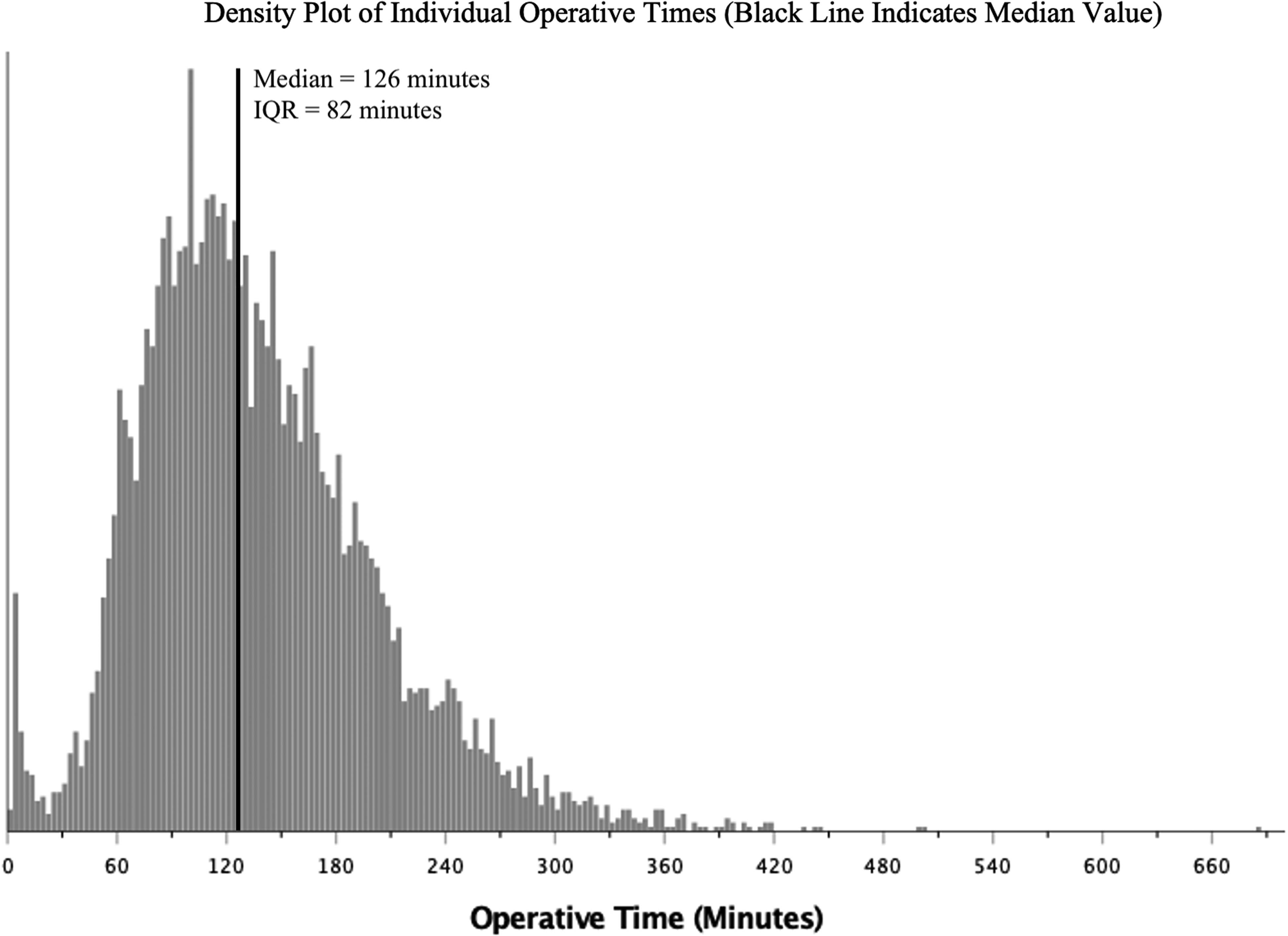
Distribution of case operative times.
Using univariate and multivariate analyses, risk factors for AAEs were evaluated including patient demographics and operative time. The results of the univariate tests are summarized on Tables 1 and 2. A statistically significant association was identified with AAE and the following demographic variables: age, ASA class, race. All medical comorbidities (cardiac, neurological, gastrointestinal, pulmonary) showed a significant association with AAEs. Additionally, operative time showed a significant relationship with AAEs following the univariate analysis. Prematurity was not found to have a significant association with AAEs (P = .712). Gender and a concurrent procedure also did not show a significant relationship with incidence of AAEs.
Following single-variable analysis with post-hoc analysis, significant differences in risk factor distribution were found between the age groups (<10 months, 10–14 months, and >14 months) (Table 2). Notably, the most complications occurred in the oldest group, and the total comorbidity burden was generally higher in the oldest age group. Significant demographic characteristics, all medical comorbidities, and operative time were included in the subsequent multivariate analysis. The presence of any concurrent procedure showed a significant increase in operative time, from an average length of 129.9 min to 144.9 (Table 3). Although the presence of a concurrent procedure added to average of operative time of 15 min, it was not associated with increased AAEs (Table 1).
Effect of the Presence of Concurrent Procedures on Operative Time and Anesthesia Time.

Using the multivariable logistic regression model (Figure 2), independent risk factors for AAEs included intermediate (OR, 1.79 [95% CI, 1.00 to 2.97]) or longer (OR, 2.46 [1.48 to 4.08]) operative times when compared to operative times of less than two hours (P < .05). Other significant risk factors included an ASA Class ≥3 (OR, 3.20 [1.87, 5.50]) and having greater than 3 medical comorbidities (OR, 8.63 [4.42 to 16.33]) (P < .05). Race and concurrent procedures were not found to be significant risk factors for AAEs in this model. Frequencies of concurrent procedures were tabulated in (Supplementary Table 1).
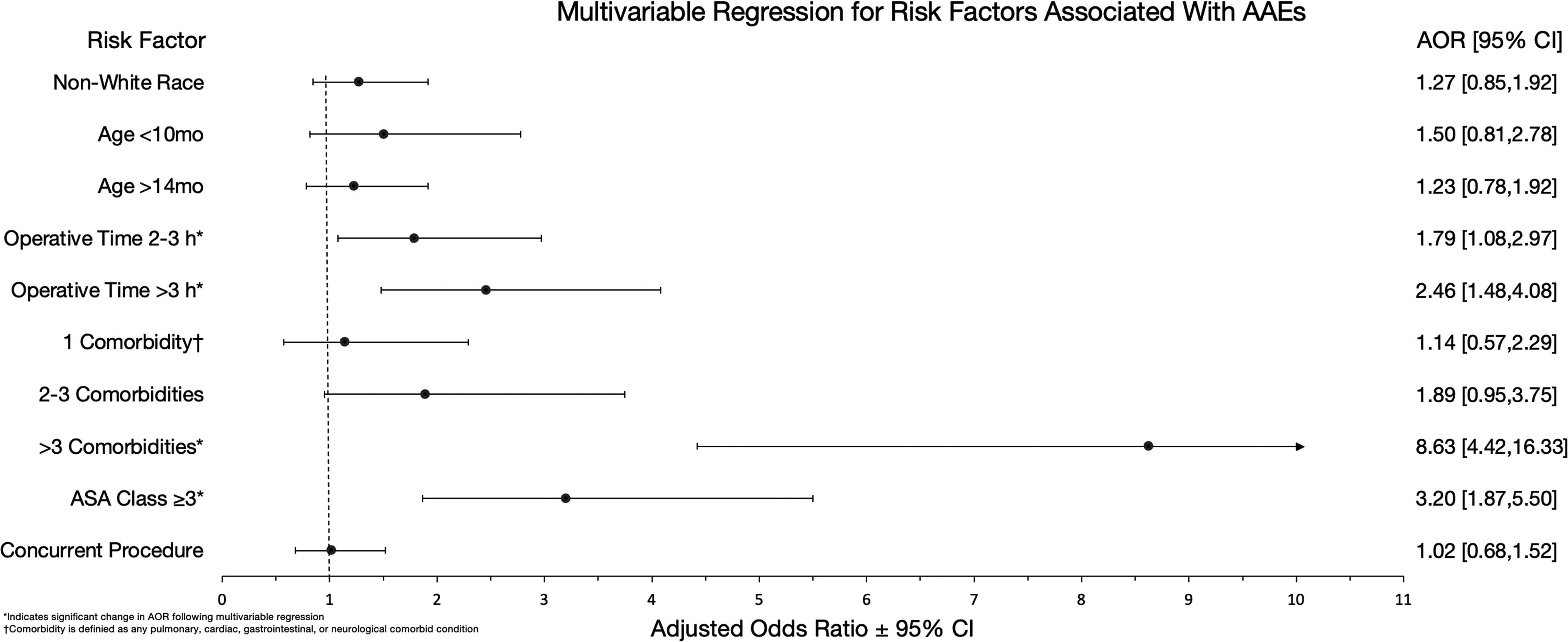
Independent risk factors for adverse airway events following multivariable analysis.
A second logistic regression was performed for subgroup analysis to determine the effects of race on the likelihood of experiencing an AAE. Compared to white, a black race was more likely to have an AAE (OR, 1.81 [1.04, 3.16]) (P < .05) (Table 4). The Asian race had a positive OR of 1.18 but was not statistically significant. Other races were not included in the model because they did not experience an AAE.
Effect of Race on the Risk of AAEs, Controlled for Other Factors Following Multivariable Analysis.

Controlled for age, operative time, presence of any medical comorbidity, ASA class, and concurrent procedure.
Discussion
Cleft palate repair is associated with a unique subset of risks and complications. This study used the pediatric NSQIP database to identify risk factors for short-term AAEs. We hypothesized that increased operative times, in addition to an increased burden of comorbidities, would be key risk factors for these devastating complications. In this study, we specifically aimed to generate objective findings regarding the number of comorbidities, age range, and other patient and case factors as they relate to the risk of experiencing an AAE.
Our results demonstrated that having greater than three medical comorbidities is an independent risk factor for AAEs after cleft palate repair. In a retrospective study of 4571 children, Ligh et al. demonstrated that medical comorbidity, in addition to feeding problems and failure to thrive, was a key predictor for higher accrued hospital charges for patients undergoing cleft lip or palate repair. 20 While our study did not specifically examine the economic impact, the patients with comorbidities had a higher incidence of complications which theoretically led to increased length of stay and total costs. While outside the scope of the present study, future studies should provide updated figures on the economic impact of complications following cleft palate repair and other pediatric craniofacial procedures. Chouairi et al. found in their 2019 study using the same NSQIP-P database, that Veau IV clefts, or complete bilateral clefts, had a higher burden of comorbidities compared to their less severe counterparts. 14 However, despite the higher comorbidity burden, their cohort did not show a difference in 30-day adverse events. Their study chose to stratify by Veau classification; this was not available for the present study due to underreporting. Additionally, the present study was focused on AAEs.
Mets et al. demonstrated that bronchopulmonary dysplasia/chronic lung disease and cerebral palsy were significantly associated with readmission and increased hospital length of stay. 15 Blough et al., using the 2012–2015 years of the NSQIP-P database, concluded that higher ASA classification, nutritional support, and neuromuscular disorders were positive predictors for additional ventilation requirements. 21 Our study expands on this work by using a more contemporary sample to identify the significant association of operative duration with adverse airway events. We also chose to study grouped medical comorbidities in order to assess any possible compounding effects on risk that would otherwise not be identified when studied individually. Their study's neuromuscular disorders variable, which was captured as a comorbid condition in our study, as well as ASA class, both show comparable results to our outcomes. Taken together, the varied positive, negative, and neutral effects of medical comorbidity on short-term postoperative complications may suggest that for particular complications, certain medical comorbidities may play a larger role than others. Investigations highlighting postoperative complications that are especially pervasive or detrimental in this patient population and detailing the specific risk factors that may lead to them would be a next step for future study.
The median operative time in this study was 126 min. Intermediate and longer operative times were independent risk factors for AAEs similar to prior data. 22 However, investigations into the effect of operative duration on complications after cleft palate repair are somewhat sparse. Our results also present an association between operative time over two hours with increased AAE risk, with even greater risk past 3 h. Longer operative times are congruent with other aspects of the operation, such as longer time under anesthesia and longer duration of airway manipulation during the palate repair, among other factors. These factors can have a compounding effect on one another which poses more stress on the child and increasing the likelihood for complication. To our knowledge, operative time thresholds for cleft palate repair do not exist yet, however our results suggest that aiming to remain under 2 h can be a possible starting point. It is important to keep in mind that these results do not suggest that technique be compromised for speed in the operating room and that other variables to reducing operative time can be considered. Working with operating room staff who are trained and familiar with cleft surgery, optimal surgical setup, and other relevant intraoperative variables can all be feasible changes to make the time in the operating room more efficient. Possible confounding variables to our result is the variation in technique, level of surgeon experience, or trainee involvement that may be implicated in longer operative times. Additionally, the database lacks sufficient information on the severity of the cleft palate for every patient. Logically, more severe clefts would imply the need for a longer operation time, and thus, a higher complication rate.
Protocols for Enhanced Recovery After Surgery (ERAS) which are aimed to truncate and improve the post-operative recovery period, have been recently developed for many pediatric procedures, including cleft palate repair. Multiple studies have demonstrated that ERAS protocols for cleft care have been effective in reducing post-operative narcotic usage, improved oral intake, and decreased hospital length of stay.23–25 Derivative protocols directed at minimizing postoperative airway and other complications could be developed and implemented which may prove to be fruitful.
The majority of palate repairs within our study cohort occurred in repairs in patients aged 10–14 months. The older (>14 month) age group demonstrated higher proportions of risk factors including comorbidity burden and an ASA class greater than 3. And, although the incidence of AAEs was higher in the youngest and oldest groups, our analysis ultimately did not find age under 10 months or above 14 months to be a statistically significant risk factor for AAEs. The lack of independent risk from patient's age suggests that other patient or surgeon-based risk factors weigh more heavily for the patient's outcome. While there is general agreement that cleft palate repair should occur prior to 18 months, the optimal timing of cleft palate repair remains a subject of debate, with degrees of variation between individual surgeons. For patients under 6 months of age, Peck et al. demonstrated a two-fold increase in risk for 30-day complications and a 4–5-fold increase in reoperation or readmission. 26 Other studies have supported the claim that earlier palate closure does not offer significantly better speech outcomes. 27 Our results also show some similarity to the age-related protection reported by Peck et al.: in children older than 6 months of age, their study did not show a significant risk for wound dehiscence, and we did not find an increased AAE risk for children older than 6 months in our study. Our subgroup analysis also identified that children of black race were more likely to experience an AAE compared to their white counterparts. Race-based differences in surgical outcomes have been diligently discussed. More relevant to the present study is the conclusion brought forth by Wu et al., who demonstrated that black children undergoing cleft palate operations were more likely to experience more complications, length of stay, higher hospital charges, and other negative outcomes. 28 Our results are also consistent with this unfortunate conclusion, and we reemphasize the importance of early intervention with high quality care for these minority patients in an effort to improve the health inequity and lead to improved outcomes.
The vast majority (85.9%) of concurrent procedures in our study cohort were myringotomy and tympanostomy tube insertion. As a standalone procedure, myringotomy and tympanostomy have a low risk of complications. 29 This low morbidity procedure is an unlikely culprit to increase complication rates, especially AAEs, even in combination with palatoplasty, and this is supported by our data. While our results did show a significant 11.6%, or 15-min, increase in operative time in cases with concurrent procedures compared to those without, a concurrent procedure did not demonstrate a significant association with increased AAEs on univariable and multivariable tests. Thus, AAEs in the group of patients undergoing concurrent procedures are unlikely due to the presence of the concurrent procedure itself as they are usually well-tolerated. Moreover, since the majority of concurrent procedures did not have airway involvement, increased AAEs in cases with longer operative times are not necessarily the result of longer anesthesia time, but likely the result of another factor such as increased duration of tongue compression. In cleft palate repair, tongue and cheek retraction is usually achieved with a Dingman-Grabb mouth retractor. In order for the Dingman to improve operative field visibility, part of its function is to depress and put pressure on the tongue. The constant tongue pressure has been suspected to be a potential cause of airway obstruction secondary to macroglossia or lingual edema which occurs following its removal.30,31 In fact, because of its known risk for postoperative lingual edema, studies have been performed to monitor Dingman applied tongue pressure throughout palate repair and further verify its potential contribution towards airway complications. 32 Additionally, operative time is likely to be a more accurate predictor of AAEs compared to anesthesia time. While operative time probably encompasses the entire duration of Dingman placement, anesthesia time may not. A longer anesthesia time can be due to difficult foley catheter placement or peripheral IV placement, among other factors, making it a suboptimal measure. Furthermore, while our group was not able to analyze individual concurrent procedures for their standalone potential for AAEs, we suspect that certain procedures, particularly those that involve additional airway manipulation such as bronchoscopy, may compound the effects of prolonged Dingman retraction and increase the risk for airway obstruction.
There are limitations to consider when evaluating the results of our study. Large administrative databases such as the ACS-NSQIP-P have inherent reporting errors, sampling bias, and lack of detail due to coding restraints. As previously mentioned, there was a lack of data on cleft severity or Veau classification within our dataset. The severity of the cleft can dictate the length and technical challenge of the operation and have a large role in operation length and outcomes. Additionally, isolated cleft palate and postoperative airway complications are higher in syndromic patients and in Pierre Robin sequence,33–36 but this data was not available in the database. Furthermore, there is a general lack of preoperative or other intraoperative variables specific to cleft palate repair that may help clarify other potential risk factors or confounding sources. This database also does not collect surgeon or hospital case volume. Theoretically, surgeons with more experience and pediatric hospitals specializing in cleft care would yield better results as has been previously reported in the development of postoperative fistula. 37
Conclusions
Overall, our study reports a low incidence of AAEs in the 30-day period following cleft palate repair by using a prospectively maintained nationwide database of patients in the United States. We demonstrated that longer operative times greater than 3 h, or a higher burden of medical comorbidities were the most impactful risk factors for postoperative AAEs. Due to heterogenous nature of the database used, we believe that our results are generalizable and provide evidence for these risks. The results presented can be useful in identifying high-risk patients who may benefit from optimization of their care by referral to higher volume surgeons or centers or consideration of postoperative ICU admission to minimize risk and improve outcomes.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231156509 - Supplemental material for Comorbidity and Operative Time are Stronger Predictors than Age for Palatoplasty Adverse Airway Events, A NSQIP-P Study of 6668 Cases
Supplemental material, sj-docx-1-cpc-10.1177_10556656231156509 for Comorbidity and Operative Time are Stronger Predictors than Age for Palatoplasty Adverse Airway Events, A NSQIP-P Study of 6668 Cases by Victor Yu, MS, Jason Pham, BS, Lydia Lukomski, BS, Jeremy Joseph, MD, MS, and Yifan Guo, MD in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The case information used this study is deidentified and available to all institutions complying with ACS NSQIP-P data use agreement.
Note
The ACS NSQIP-P databases are the source of information for this study. Data extrapolated, statistical analysis performed, and conclusions reached are not verified by the ACS NSQIP-P. All results are the work done by authors of this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.