
Abstract
Objective
Weakness of the mucosal free margin is common in secondary cleft lip deformities. However, the incidence is rarely reported after a long-term follow-up. We evaluated the evolution of patient mucosal free margin after primary repair and until the end of growth.
Design
Blinded retrospective study (photography and chart reviews).
Setting
Tertiary care hospital; private practice.
Patients
Forty-eight patients with unilateral cleft lip with or without cleft palate who underwent primary nasolabial repair between 1996 and 2004 were followed up until their end of growth marked at 18 and 16 years of age for male and female patients, respectively.
Interventions
Primary nasolabial repair using a straight-line closure without a triangular flap on the vermilion was performed; if needed, a revision surgery was performed at 5 years of age (85%).
Main Outcome Measure:
The contour of the mucosal free margin was classified into nodular, smooth, and recessed types at 1, 5, and 10 years and at the end of growth.
Results
At 1 year of age, the nodular type was more common (58%). However, the recessed type was more common (75%) at the end of growth. The mucosal free margin continued to change after 10 years of age. At the end of growth, half of the patients with incomplete cleft experienced center weakness, and the others had cleft-side weaknesses.
Conclusions
Patients with incomplete clefts showed favorable results at early ages. However, two-thirds of the patients with complete and incomplete clefts showed focal weakness at the end of growth.
Introduction
In secondary cleft lip deformities, weakness of the mucosal free margin, which was previously called “whistling deformity,” has been frequently observed even in recent years. Correction along the labial free margin is frequently required for unilateral and bilateral cleft lip.1–3 The revision rates of lip deformities have been reported in the literature, typically based on a single surgeon's experience.1,3–6 Among these, correction of the mucosal free margin was the most common procedure.1,3
However, the incidence rate of the free margin deformity is not clearly reported in current literature, especially in long-term follow-ups beyond the end of growth. This study was performed to evaluate how the mucosal free margin of the upper lip evolves from primary repair to the end of growth.
Methods
Design and Patients
The study was reviewed and approved by the Committee for Medical Ethics of XXXX University XXXXX Review Board. Retrospective photography and chart review were performed for patients with unilateral complete and incomplete cleft lip, with or without cleft palate, who underwent primary nasolabial repair performed by the senior author (XXXX.) between April 1, 1996 and May 31, 2004. Patients who were followed up until the end of growth, herein defined as until 16 and 18 years of age for female and male patients, respectively, were included in the study. Patients were excluded if they had undergone unscheduled revision surgery, except for those performed at 5 years of age (scheduled revision surgery) or those who had a syndromic diagnosis or lesser-form cleft lip. Cases with a Simonart's band were classified as incomplete cleft. We performed scheduled revision surgery, as needed, at 5 years of age and at the end of growth. Scar massage was not applied. Photographs captured before the revision surgery were used for evaluation.
Outcome Measurement
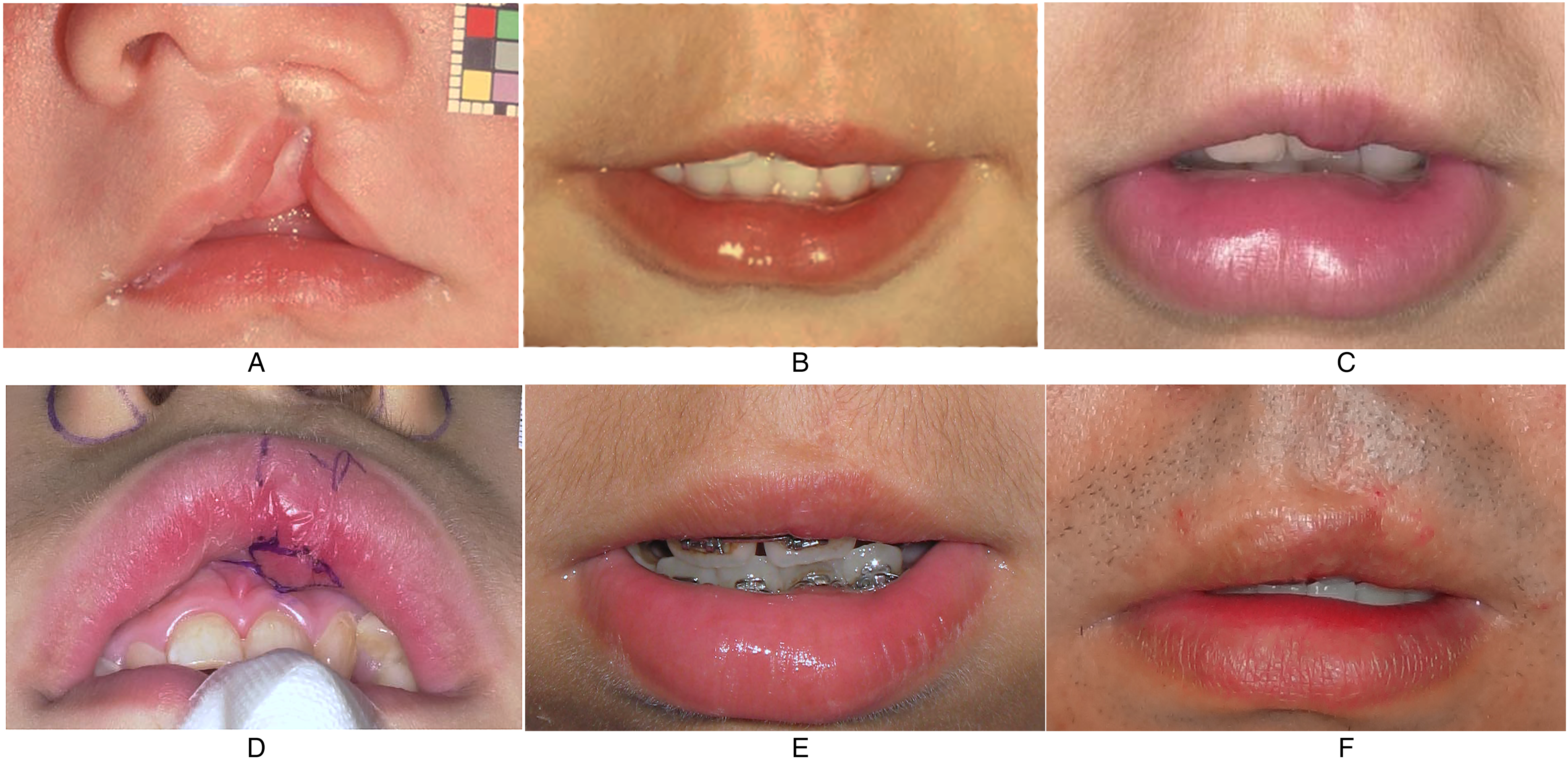
The contour of the mucosal free margin was classified into 3 types based on frontal view photographs of the patient at 1, 5, 10, and 18 years of age in male patients (and at 16 years in female patients) (Figure 1). The 3 types include nodular, smooth, and recessed. The nodular type indicated free margin with a convex tip as a nodule without any recessed parts. The smooth type indicated smooth or natural contour without nodular or recessed parts. The recessed type indicated free margin with a recessed or weak portion. Subsequently, the patients were subdivided based on the prior location of the recessed portion, whether at the center or cleft side (Figure 1). A third person collected the data and created ungrouped photographs for evaluation. Two independent plastic surgeons classified the contour into 3 categories and subdivisions twice in a blinded manner. Any disagreement between the surgeons was resolved by consensus.
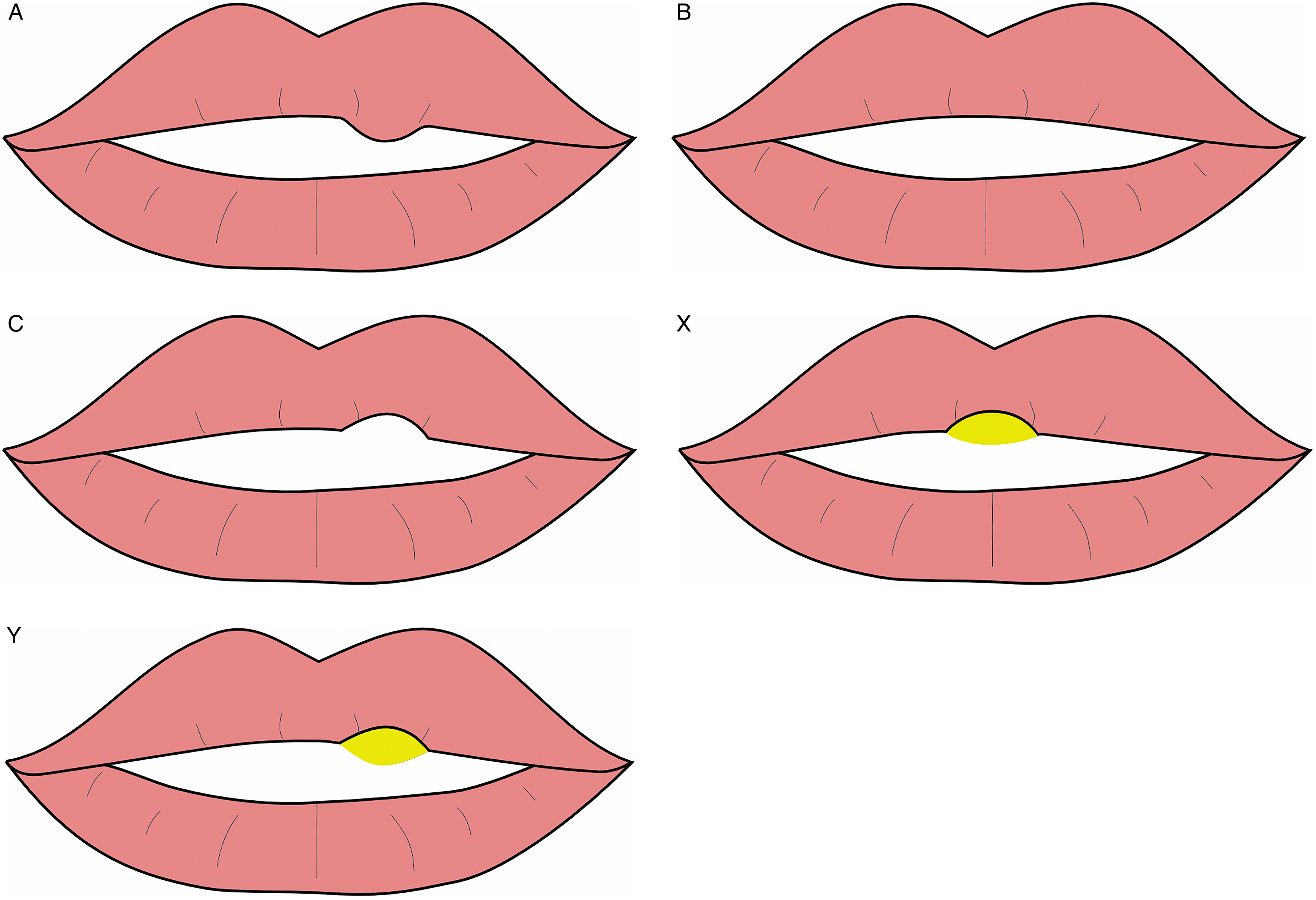
Three types of contours for mucosal free margins and their subdivisions. Three types: nodular (A), the free margin has a convex tip or fullness as a nodule without any recessed part; smooth (B), the contour is smooth or natural contour without any nodular or recessed part; and recessed (C), the free margin with a recessed or weak portion. Subdivision: center (x), the recessed part is in the center of the upper lip; cleft side (y), the recessed part is on the cleft side.
Surgical Technique in Primary Repair
One-stage primary nasolabial repair was performed in patients weighing >4.0 kg at approximately 1 to 3 months of age. In lip repair, abridged rotation-advancement with a small triangular flap at the vermilion-cutaneous junction was performed. A vermilion triangular flap was not used, and the vermilion was directly closed. Intraoral/vestibular mucosa was closed using the rotation-advancement method and the closure line was curved and Z-plasty was performed on the vestibule. During the nose repair, total repositioning of the malpositioned lower lateral cartilage and septum was performed.
Surgical Technique in Secondary Lip Revisions
Scheduled revision surgery was performed at 5 years of age, as needed. The performed procedure is provided in the Supplementary Table S1. We performed Z-plasty, reduction, or reconstruction of orbicularis oris muscle.
Statistical Analysis
Differences in data regarding the subdivision were analyzed using the chi-square test for independence. The test was conducted with IBM SPSS Statistics for Windows, Version 23.0 (IBM Corp.). In all analyses, P < .05 was considered statistically significant, and P values were two-tailed.
Results
A total of 151 patients who underwent primary repair of the unilateral cleft lip during the study period were identified. However, 103 patients were excluded from the study for the following reasons: they were either lost to follow-up or complete 4-point photographs were unavailable (n = 94); underwent an unscheduled revision surgery at an age other than 5 years old (n = 4); had a syndromic diagnosis (n = 3); or had a lesser-form cleft lip (n = 2). Thus, 48 patients were available for analysis. Many of the patients underwent a scheduled revision surgery at 5 years old (85%, n = 41/48). Details of the study population are shown in Supplementary Table S1.
The contour of the mucosal margin for the entire study population is shown in Figure 2. At 1 year of age, the nodular type was the most common (58%, n = 28/48). However, at the end of growth, the recessed type was more common than the nodular type (75%, n = 36/48).
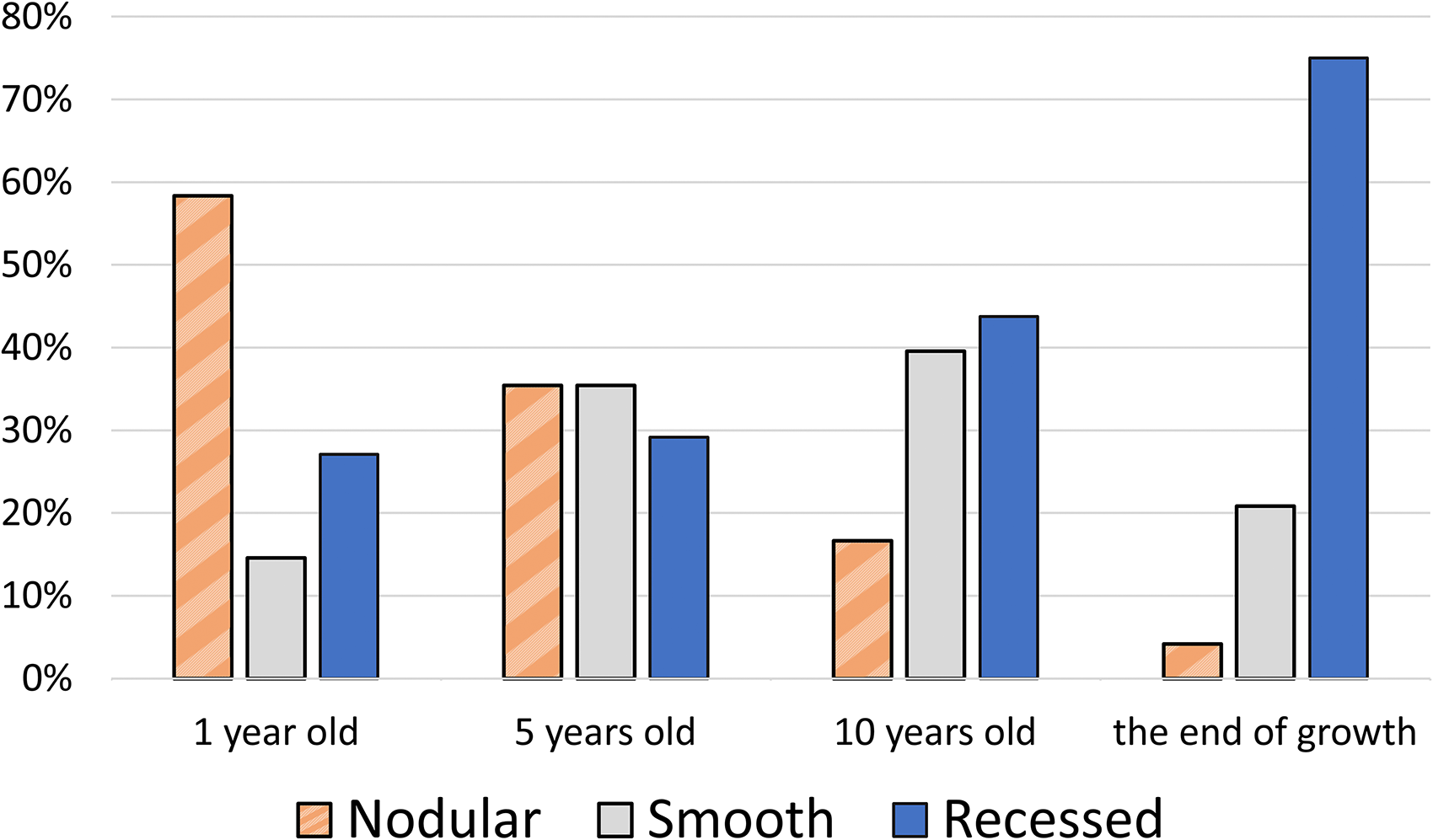
The contour of the mucosal free margin in the entire study population at 1, 5, and 10 years and at the end of growth.
A comparison between patients with complete and incomplete clefts is shown in Figure 3. At 1 year of age, the nodular type of margin was more common in patients with incomplete cleft than in patients with complete cleft (complete: 35%, n = 8/23; incomplete: 80%, n = 20/25). However, the recessed margin was more common at the end of growth both in patients with complete and incomplete clefts (complete: 78%, n = 18/23; incomplete: 72%, n = 18/25).
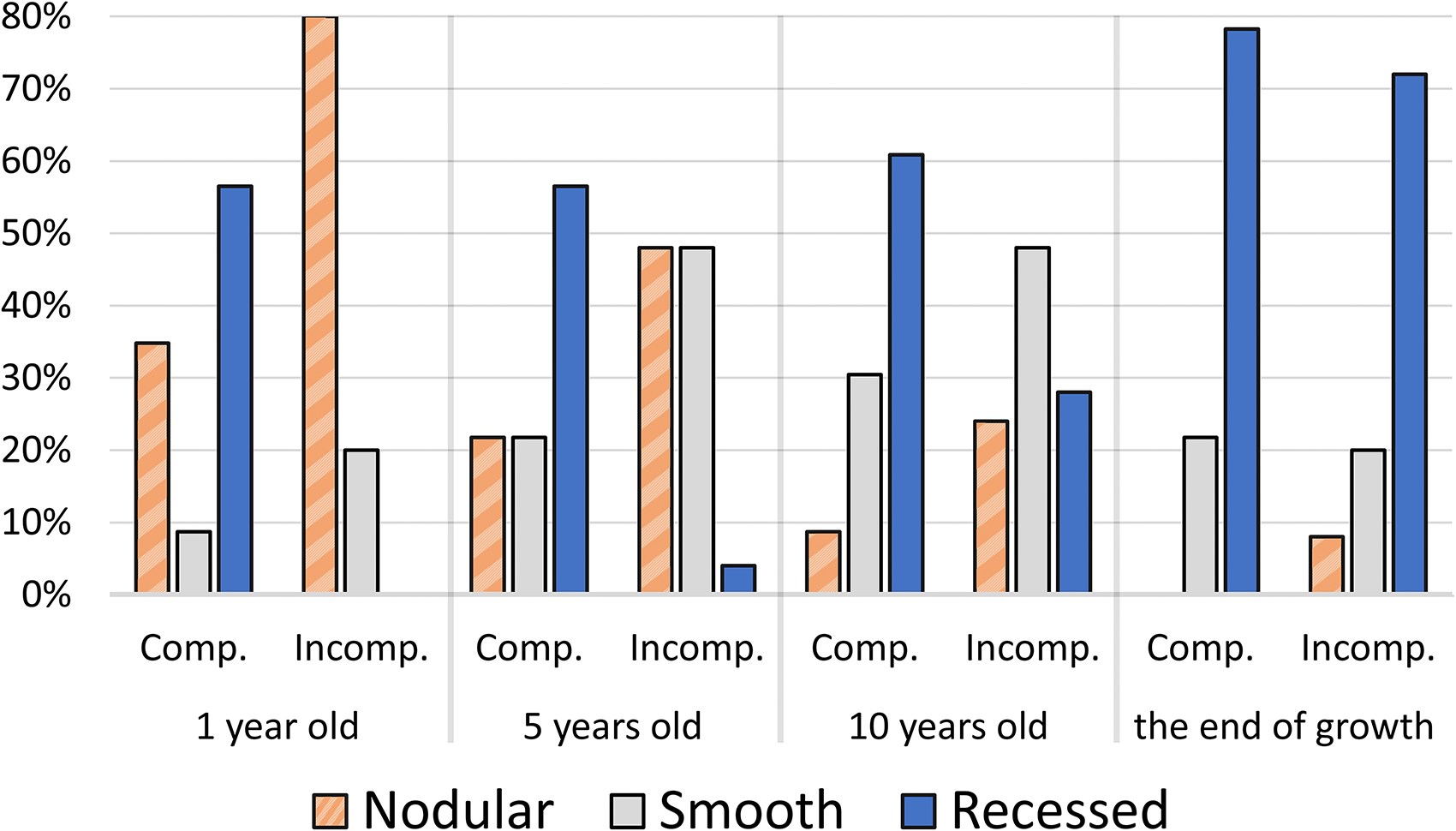
The contour of the mucosal free margin comparing patients with complete and incomplete clefts at 1, 5, and 10 years and at the end of growth.
The changes in the mucosal margin through the 4 points of growth are shown in Supplementary Figure S1. The prevalence of recessed margin significantly increased from 10 years of age to the end of growth.
The portion that was recessed at 1 year of age and the end of growth is shown in Figure 4. In patients with complete cleft, almost all patients had the recessed part on the cleft side at 1 year of age (100%, n = 13/13) and at the end of growth (94%, n = 17/18). Conversely, in patients with incomplete cleft, approximately 40% (n = 7/18) and 60% (n = 11/18) had the recessed parts in the center and cleft side at the end of growth, respectively (P = .02).
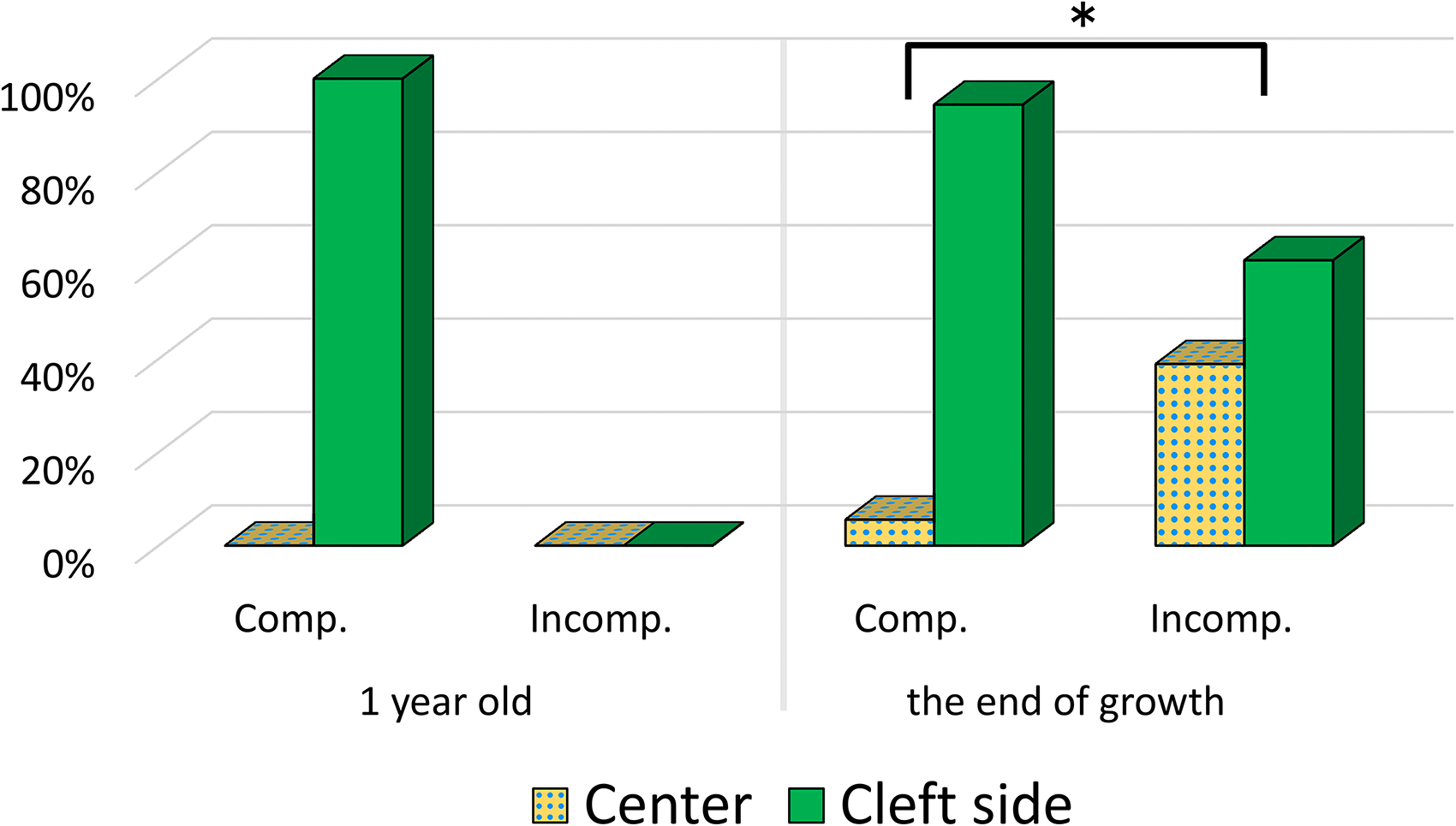
The subdivision, wherein the recessed part exists at 1 year and at the end of growth: center or cleft side. (*P < .05, chi-square test).
Two representative cases are shown in Figures 5 and 6.
A male patient with left incomplete cleft lip and cleft alveolus. The photographs “a” to “f” refer to the same patient. (A) Photograph before primary surgery (B) Nodular type at 1 year of age. (C) Nodular type at 5 years of age before revision surgery. (D) Z-plasty in the vermilion border and reduction of the vestibule mucosa are performed in revision surgery at 5 years of age. (E) Smooth type at 10 years of age. (F) Recessed type on the cleft side at 18 years of age before the revision surgery.

A female patient with left incomplete cleft lip and cleft alveolus. The photographs “a” to “f” refer to the same patient. (A) Photograph before primary surgery. (B) Smooth type at 1 year of age. (C) Smooth type at 5 years of age before revision surgery. (D) Z-plasty in the vermilion border and reduction of the mucosa was performed in revision surgery at 5 years of age. (E) Recessed type at 10 years of age. (F) Recessed type in the center at 18 years of age before the revision surgery.
Discussion
Deformity of the mucosal free margin is one of the most important characteristics of cleft lip, and correction surgery is the most common repair method.1,3 However, classifying its morphology and incidence rate throughout growth has not been reported. Clarifying this will help surgeons be aware of the deformity and determine the type of intervention required for revision surgery, the proper timing thereof, and the patients’ prospects.
In this study, we evaluated the morphology of the free margin throughout the growth period. Two-thirds of the patients had weakness of the mucosal free margin at the end of growth even if they previously had better-shaped lips or underwent revision surgeries. The revision rate of free margin previously reported ranged from 3.8% to 57% at under 10 years of age, approximately 10 years of age, or was unreported.1,3–6 However, these studies lack precise evaluation of the patients after the end of growth. Thus, the post-growth outcome of revision surgery was unknown. Furthermore, the revision and incident rates are unequal because these depend on the patients’ psychosocial issues and surgeons’ preferences. Surgeons are now more cognizant about the relative weakness of the free margin, as evidenced by the recent rise in revision rates. 3 Therefore, our results are consistent with the recently observed increase in revisions.
In nearly half of the patients with incomplete cleft, weakness of the mucosal free margin was found at the center of the lip, like the whistling deformity in bilateral clefts, at the end of growth. The others had weakness on the cleft side, as with complete clefts. We speculate that this might be due to the variation in tissue volume, growth pattern around the cleft, weakness of the orbicularis oris muscle, scar tethering of the lip from vertical lengthening, and spontaneous thinning of scar tissue over the years. In some patients with incomplete cleft and supple tissue on the lateral lip, the recessed part in the center might eventually become visible if the prolabium has less tissue initially or grows less. Therefore, if the vermilion fullness on the cleft side is excised, it may be preferable that a small amount of vermilion fullness was left intact and subsequently monitored upon follow-up. The excess vermilion fullness can then be used to translocate tissue volume to the center in any flaps3,7 to supply median weakness or create a median tubercle. Considering the changes in the mucosal free margin through the 4 points of growth, the prevalence of recessed margins significantly increased from 10 years of age to the end of growth. We believe that pubertal growth spurt or development of secondary sexual characteristics most likely led to the development of weakness at the mucosal margin after 10 years of age; this result may also represent soft tissue and scar tissue change through the pubertal period.
This study has limitations. The retrospective nature of the research limits our findings. Additionally, the data from the excluded patients could have had a significant impact on our results. Furthermore, intra-rater and inter-rater reliability bias may have affected the results because of the unblinded decision-making process for deformity classification. Short-term postoperative photographic evaluation of the revision surgery was not performed, and our results did not reflect the true natural course as 85% of patients underwent a scheduled revision surgery at 5 years of age. Additionally, we did not use a vermilion flap in this study. A laterally based vermilion triangular flap is widely used to augment deficient prolabial vermilion through the smooth addition of keratinized vermilion to the prolabium and restore the vermilion width at the cleft side philtral column.8,9 Therefore, the results of this study may not be generalizable to patients currently undergoing treatment. The incidence rate may be higher than these patients as they are currently being treated.
Conclusion
Our results depict the morphological changes in the mucosal free margin throughout the growth years (1-18 years of age) of patients with complete and incomplete clefts. The mucosal free margin continued to change even beyond 10 years of age, and the recessed part became more obvious with age. Patients with incomplete clefts showed desired results at early ages but two-thirds of the patients with complete and incomplete clefts showed weakness at the end of growth, although 85% of patients underwent a scheduled revision surgery at 5 years of age. Half of the patients with incomplete cleft had a center weakness at the end of growth. Based on this longitudinal morphological change, primary surgery should be focused on preserving tissue, and revision surgeries should also be performed leaving tissue volume until the final revision surgery after growth.
Supplemental Material
sj-doc-1-cpc-10.1177_10556656221108851 - Supplemental material for Longitudinal Morphological Changes in the Mucosal Free Margin After Unilateral Cleft Lip Repair
Supplemental material, sj-doc-1-cpc-10.1177_10556656221108851 for Longitudinal Morphological Changes in the Mucosal Free Margin After Unilateral Cleft Lip Repair by Yuta Nakajima, Shunsuke Yuzuriha and Fumio Nagai in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-tiff-2-cpc-10.1177_10556656221108851 - Supplemental material for Longitudinal Morphological Changes in the Mucosal Free Margin After Unilateral Cleft Lip Repair
Supplemental material, sj-tiff-2-cpc-10.1177_10556656221108851 for Longitudinal Morphological Changes in the Mucosal Free Margin After Unilateral Cleft Lip Repair by Yuta Nakajima, Shunsuke Yuzuriha and Fumio Nagai in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-tiff-3-cpc-10.1177_10556656221108851 - Supplemental material for Longitudinal Morphological Changes in the Mucosal Free Margin After Unilateral Cleft Lip Repair
Supplemental material, sj-tiff-3-cpc-10.1177_10556656221108851 for Longitudinal Morphological Changes in the Mucosal Free Margin After Unilateral Cleft Lip Repair by Yuta Nakajima, Shunsuke Yuzuriha and Fumio Nagai in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
None.
Author’s Note
This manuscript was presented orally at the 64th annual meeting of the Japan Society of Plastic and Reconstructive Surgery April 14, 2021 in Tokyo, Japan and at the 14th World Congress of The International Cleft Lip and Palate Foundation April 20-22, 2022 in Osaka, Japan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was reviewed and approved by the Committee for Medical Ethics of Shinshu University School of Medicine Institutional Review Board (No. 4803).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JSPS KAKENHI (grant number JP21K09761).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.