
Abstract
Objective
To examine the current trends and practices across disciplines for feeding infants with cleft palate with or without cleft lip and to describe provider training within this area
Design
Prospective survey
Setting
ACPA approved cleft palate teams and healthcare providers in the United States and Canada
Participants
Interdisciplinary providers that regularly provide feeding services to infants with cleft palate
Intervention
50-item survey designed and distributed electronically via the ACPA
Main Outcome Measures
Information on provider demographics and practice patterns
Results
76 respondents included providers in North America that have either currently or previously served on a cleft palate team. The majority of respondents were in speech-language pathology (49%) or nursing (38%) disciplines, worked in an outpatient setting (70%), and received no information (68%) regarding cleft palate feeding in their academic training. While specific practice patterns were relatively consistent across the respondent cohort, provider characteristics were significantly associated with squeezing the Haberman (p = .013) and likelihood of collaboration with other providers when counseling parents/caregivers (p = .039).
Conclusions
While provider characteristics varied, there were similar practice patterns observed across disciplines. Future research is needed explore training related to feeding knowledge as well as practice patterns in locations with a lower patient volume.
Keywords
Introduction
Orofacial clefting, including cleft palate with or without cleft lip, is one of the most common congenital birth defects in the United States. 1 A cleft palate prevents the infant from creating negative intraoral pressure to extract milk from the breast or a traditional nipple. A majority of infants with cleft palate are reported to have moderate to severe feeding difficulties 2 and differ from their non-cleft peers in their feeding proficiency, rate of milk transfer, and feeding duration.3,4 Other feeding problems may include excessive air intake, nasal regurgitation, inadequate milk intake, and difficulty establishing an adequate suck-swallow-breathe sequence.5,6 Secondary to feeding difficulties, infants with cleft palate frequently exhibit problems with early weight gain and growth. This is particularly concerning for this clinical population due to the importance of weight gain in preparing infants for timely surgical repairs. 7 Reduced human milk feeding has also been reported for infants with cleft palate compared to those without cleft palate.8–10 Difficulty with feeding can lead to maternal stress and anxiety, adversely affecting mother and infant bonding 11 and possible severe life consequences (such as failure to thrive) if adaptive feeding mechanisms are not utilized. 12
Using a cleft-adapted bottle is one strategy to aid in improving feeding difficulties in this population. A variety of cleft-adapted bottle systems are available and include both infant-driven and assisted delivery systems. Infant-driven systems allow the infant to independently compress the nipple to extract milk, while assisted delivery systems require a feeder to compress the nipple or bottle. There has been an increase in the use of infant-driven bottles 13 with the Dr. Brown's Medical Specialty Feeding System (Dr. Brown's) being one of the first bottles offered to infants with cleft palate. 9 Other specialty feeders include the Medela Special Needs Feeder (Haberman), Enfamil Cleft Lip/Palate Nurser (Mead Johnson), and the Pigeon baby bottle by Respironics (Pigeon). Less common primary feeding techniques include feeding tubes, syringes, spoons, and droppers. 14 The severity of feeding difficulty and the selection of cleft-adapted systems is reported to be dependent on the type, size, and severity of the infant's cleft.15,16 Other interventions utilized to improve infant outcomes include increasing the infants’ milk volume intake, concentrating the caloric density of the milk, using an appropriate nipple flow rate, 17 care coordination, and provider training. 12
The scope of cleft palate feeding spans across disciplines. However, few studies to date have described the current feeding practices followed by healthcare professionals directly involved in the care of infants with cleft palate. In addition, there is evidence that information given to parents regarding feeding instruction is lacking due to hospital personnel having limited or no experience in the area of cleft palate feeding management. 18 Snyder and colleagues (2019) surveyed parents of infants with cleft lip and palate regarding perceptions of feeding experiences during the initial evaluation and found that 69% of parents received feeding information at the birth hospital, 4% received information prior to the birth of their child, and 15% received no information at all. 18 Additionally, course-based instruction for low-incidence disorders, such as cleft palate, receives less focus within training programs. 19 While 73% of speech-language pathology programs offer craniofacial course content, only 27% provided a designated and required graduate-level course. Given that speech-language pathologists (SLPs) provide feeding services for infants with cleft palate, training may be lacking in this area and contributing to the varying practices and outcomes reported for feeding infants with cleft palate.
Due to the lack of information about current training and feeding practices followed by healthcare providers, Kotlarek, Zarzycka, and Bush (2022) employed a qualitative multiple case study approach to interview four expert craniofacial feeding providers in the United States. 20 Emergent themes included informal training mechanisms as the dominant form of education, similarities in the components of a feeding consultation, variations of practice in the multidisciplinary aspects of feeding, clinical decision-making and expertise, and clinical and educational dilemmas. 20 Based on these findings, a survey was designed to examine current training and feeding practices among a larger population of providers across disciplines. The purpose of this study was to (1) describe the current trends in feeding practices by providers in cleft care, and (2) define the training received regarding feeding of infants with cleft palate.
Methods
Survey Development
This survey was created based on themes arising from semi-structured interviews regarding feeding practices and training. These interviews were conducted with a small group of expert providers engaging in feeding services for infants with cleft palate. 20 The survey comprised a total of 50 items and was divided into three sections: (1) respondent information regarding residence, age, and occupation, (2) provider practice pertaining to feeding infants with cleft palate, and (3) training and education within this area. The survey was developed using binary and multiple-choice questions, Likert-scale items, and open-ended responses.
The Wyoming Survey and Analysis Center reviewed survey questions to resolve any potential bias. An expert researcher and provider of cleft palate care piloted the survey for face and content validity and provided feedback. Skip logic was used throughout the survey to ensure that all questions were applicable and appropriate for each respondent. For example, when respondents indicated that their feeding recommendations change for a cleft of the lip only when compared to an overt cleft, they were provided follow-up questions to explore their reasoning. All questions required a response with a forced-choice feature with the exception of open-ended response questions, which explored additional, less-prevalent feeding topics and allowed respondents to provide relevant information that could direct future recommendations.
Survey Dissemination
The survey was assembled and disseminated through Qualtrics XM Software, an online survey tool (Qualtrics XM, 2021, Provo, UT). Members of the American Cleft Palate-Craniofacial Association (ACPA) received information about the study electronically via a link to the consent form and survey. Similarly, cleft care teams from the ACPA list were emailed directly with the link to further response rates and to offer additional providers the chance to respond. The targeted population for respondents included interdisciplinary healthcare professionals who were regularly involved in feeding consultations for infants with cleft lip and/or palate, as defined by service (past or current) on a cleft palate team. Potential respondents were informed that the survey would require approximately 10-min to complete. Participation was voluntary with no more than minimal risk and no direct benefits to completion. Approval to conduct the research was granted by the University of Wyoming Institutional Review Board.
Statistical Analysis
The data were imported from Qualtrics into SPPS Version 28.0 for data analysis. Descriptive statistics were used to identify the frequency of response to each relevant question. Chi-square tests of association were used to determine the relationship between provider information and specific practice patterns. Relevant provider information included: age, discipline, practice setting, experience in the discipline, and experience in craniofacial care. Practice patterns of interest included: first bottle selection, use of the Haberman, bottle inventory, and collaboration. Categories were collapsed to meet assumptions for conducting these analyses. Collapsed categories for provider information included: Provider age (20–49 years or 50+ years), discipline (SLP or other), experience in discipline (≤20 years or 21+ years), experience in craniofacial care (≤10 years or 11+ years), setting (outpatient or other). Collapsed categories for practice patterns included: Squeezing the Haberman (yes or no/dependent on patient), first bottle selection (Dr. Brown's or other), and likelihood of collaboration with other professionals (almost never/not very often or often/almost always). If assumptions were still not met (expected cell counts were less than 5), results from the Fisher's exact test were reported; these analyses are denoted with * in the results section.
Results
Respondent Characteristics
Qualtrics identified 87 respondents that consented to take the survey, 79 of which indicated they provided feeding services to infants with craniofacial differences. Respondents were further limited to providers in North America to control for practice differences based on availability of resources. Thus, 76 healthcare providers (United States: 96%, n=73; Canada: 4%, n=3) were included in the analysis. Twelve respondents (16%) did not finish the entire survey but were included in the analysis for earlier survey items.
Regarding discipline, respondents identified as either a speech-language pathologist (49%, n=36), nurse/nurse practitioner (38%, n=28), physician assistant (5%, n=4), occupational therapist (3%, n=2), dietitian (3%, n=2), or dual certified lactation consultant/nurse (1%, n=1). Ages of respondents were reported in ranges: 20–29 years (10%, n=7), 30–39 years (26%, n=19), 40–49 years (25%, n=18), 50–59 years (18%, n=13), 60–69 years (21%, n=15), and 70–79 years (1%, n=1). Discipline-specific experience varied, including respondents who had been practicing in their discipline for: <1 year (3%, n=2), 1–5 years (15%, n=11), 6–10 years (15%, n=11), 11–15 years (12%, n=9), 16–20 years (12%, n=9), and 21+ years (42%, n=31). The vast majority of respondents reported working in an outpatient (70%, n=51) or inpatient hospital setting (18%, n=13), with some (5%, n=4) covering multiple medical settings. Provider setting by discipline is listed in Table 1.
Setting of Feeding Providers and Average Percentage of Time Dedicated to Craniofacial Care Based on Discipline. All Values Listed in %.
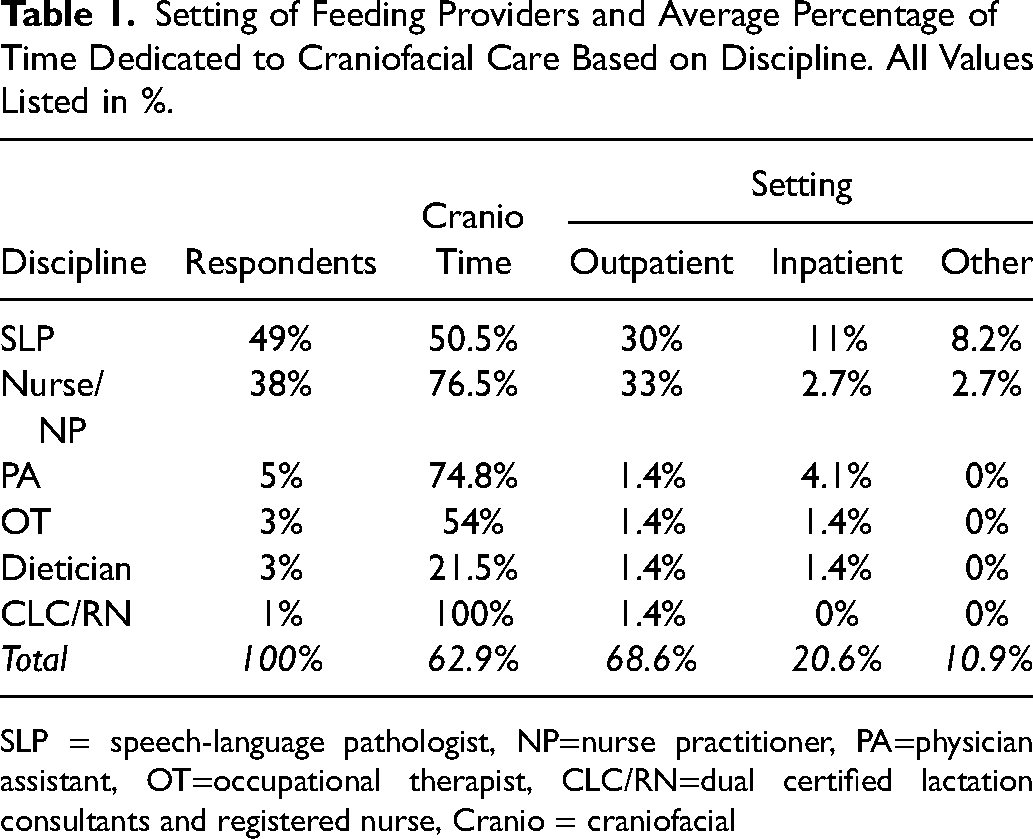
SLP = speech-language pathologist, NP=nurse practitioner, PA=physician assistant, OT=occupational therapist, CLC/RN=dual certified lactation consultants and registered nurse, Cranio = craniofacial
All respondents were familiar with cleft and craniofacial care. All respondents reported either currently serving on a cleft or craniofacial team (97%, n=74) or had done so in the past (3%, n=2). Years of experience in craniofacial care ranged widely, including respondents with <1 year (5%, n=4), 1–5 years (29%, n=21), 6–10 years (18%, n=13), 11–15 years (11%, n=8), 16–20 years (15%, n=11), and 21+ years (22%, n=16) experience. Most respondents reported being involved in feeding consultations for infants with orofacial clefting very frequently (56%, n=41) or somewhat frequently (29%, n=21). When asked to estimate the percentage of their workweek devoted to the assessment and/or treatment of patients with craniofacial differences, responses ranged from 10–100% with an average of 61.78% of the typical workweek. Most providers reported receiving information on feeding infants with cleft palate through on-the-job training (97%, n=61), continuing education opportunities (84%, n=53), or shadowing other providers (76%, n=48). Forty-three providers (68%) reported receiving no information on feeding infants with cleft palate in their degree program, thus the majority felt a lack of confidence (63%, n=40) in this area upon graduating with their terminal degree.
Practice Patterns and Assessment
Variations in practice patterns were observed across respondents. When a cleft has been diagnosed prenatally, the majority (86%, n=60) of providers indicated first discussing potential feeding options with the parent/caregiver prior to the birth of the child with some providers opting to discuss feeding at the hospital prior to discharge (1%, n=1), after the hospital discharge but within the first week of life (11%, n=8), or only if there are feeding issues (1%, n=1). Most providers indicated that they almost always (45%) or often (38%) work collaboratively with another discipline when counseling parents/caregivers; the top three disciplines for collaboration include speech-language pathology (69%), nursing (58%), and surgery (48%). Most providers reported relying on their clinical expertise all of the time (74%, n=43) while using external evidence/research (43%), internal evidence (48%), and parent/caregiver perspectives (59%) quite often (Figure 1). Providers consult current research relative to feeding infants with cleft palate with the following frequency: Almost always (9%, n=5), often (64%, n=34), not very often (30%, n=16), and almost never (5%, n=3).
Common cleft-adapted bottles are available at respondents’ facilities with the following prevalence: Dr. Brown's Medical Specialty Feeding System (Dr. Brown's; 99%), Medela Special Needs Feeder (Haberman; 84%), Pigeon Baby Bottle by Respironics (Pigeon; 53%), and Enfamil Cleft Lip/Palate Nurser (Mead Johnson; 41%). Of those providers that recommend the Dr. Brown's System, 86% determine flow rate/nipple size by observing the infant's suck-swallow-breathe sequence, and 64% base the decision on feeding duration; infant weight (30%) and age (47%) were less common indications for determining flow rate. Of those providers that use the Haberman, 37% recommend parents squeeze the nipple, 7% recommend parents do not squeeze the nipple, and 56% vary their recommendations based on the patient.
Assessment practices, although variable, demonstrated more consistent patterns compared to bottle usage. Sixty-three respondents (98%) indicated the parent(s)/caregiver(s) feed the infant during a feeding consultation; 41 providers (64%) also indicated they (or another provider) feeds the infant. The vast majority of providers (77%, n=40) typically recommend the Dr. Brown's System first during the initial feeding consult. The top three components routinely assessed/considered as part of a typical feeding consultation included coordination (eg, suck-swallow-breathe) (98%, n=63), cleft type/severity (97%, n=62), and duration of feeds (97%, n=62). The most inconsistently assessed areas included bolus intake (52%, n=33), muscle tone (67%, n=43), and nasal regurgitation (70%, n=45). The top three feeding topics routinely discussed with parents included feeding within 30 min (100%, n=64), flow rate/nipple size (92%, n=59), and parent/caregiver counseling (91%, n=58). The most inconsistent topics discussed with parents included directing the nipple to the non-cleft side (53%, n=34), external pacing (58%, n=37), and breastfeeding (61%, n=39). Over half of all providers surveyed indicated that the infant's ability to feed with the system (98%), infant health issues (94%), and availability of specific feeding systems at their facility (64%) were all very important factors in selecting a feeding system. On the contrary, 73% and 39% of providers indicated the strength of product marketing and surgeon preference, respectively, were not important at all in choosing a feeding system (Figure 2). Approximately half of providers (53%, n=34) reported that babies with overt cleft palate often feed without concern after the first feeding consult; other responses included almost always (11%, n=7), not very often (33%, n=21), or almost never (n=2).
Association between Provider and Practice Patterns
The data revealed significant associations between some combinations of provider demographics and practice patterns. There were no statistically significant associations between first bottle selection and age of provider (χ2(1) = .145, p = .703), discipline of provider (χ2(1) = 1.135, p = .287), years of experience in the field (χ2(1) = .003, p = .955), years of experience in craniofacial care (χ2(1) = 1.049, p = .306), or practice setting* (p = .522). There was a statistically significant association between years of experience in craniofacial care and recommending that parents squeeze the Haberman to assist in milk delivery (χ2(1) = 6.234, p = .013); this association was moderately strong, Cramer's V = .381 (Table 2). The odds ratio of recommending to squeeze the Haberman in providers with ≤ 10 years versus 11+ years’ experience was 5.225 (95% CI, 1.366–19.986). Thus, providers who more recently began working in craniofacial care are 5.225 times more likely to recommend squeezing the Haberman than providers with more craniofacial-specific experience. However, there were no significant associations between squeezing the Haberman and age of provider (χ2(1) = 1.626, p = .202), discipline of provider (χ2(1) = 2.618, p = .106), years of experience in the field (χ2(1) = .199, p = .655), or practice setting (χ2(1) = 1.867, p = .172). There were also no significant associations between practice setting and bottle inventory.
Results of the Crosstabulation, Risk Estimate, and Chi-Square Test Between Years of Experience in Craniofacial Care and Squeezing the Haberman.
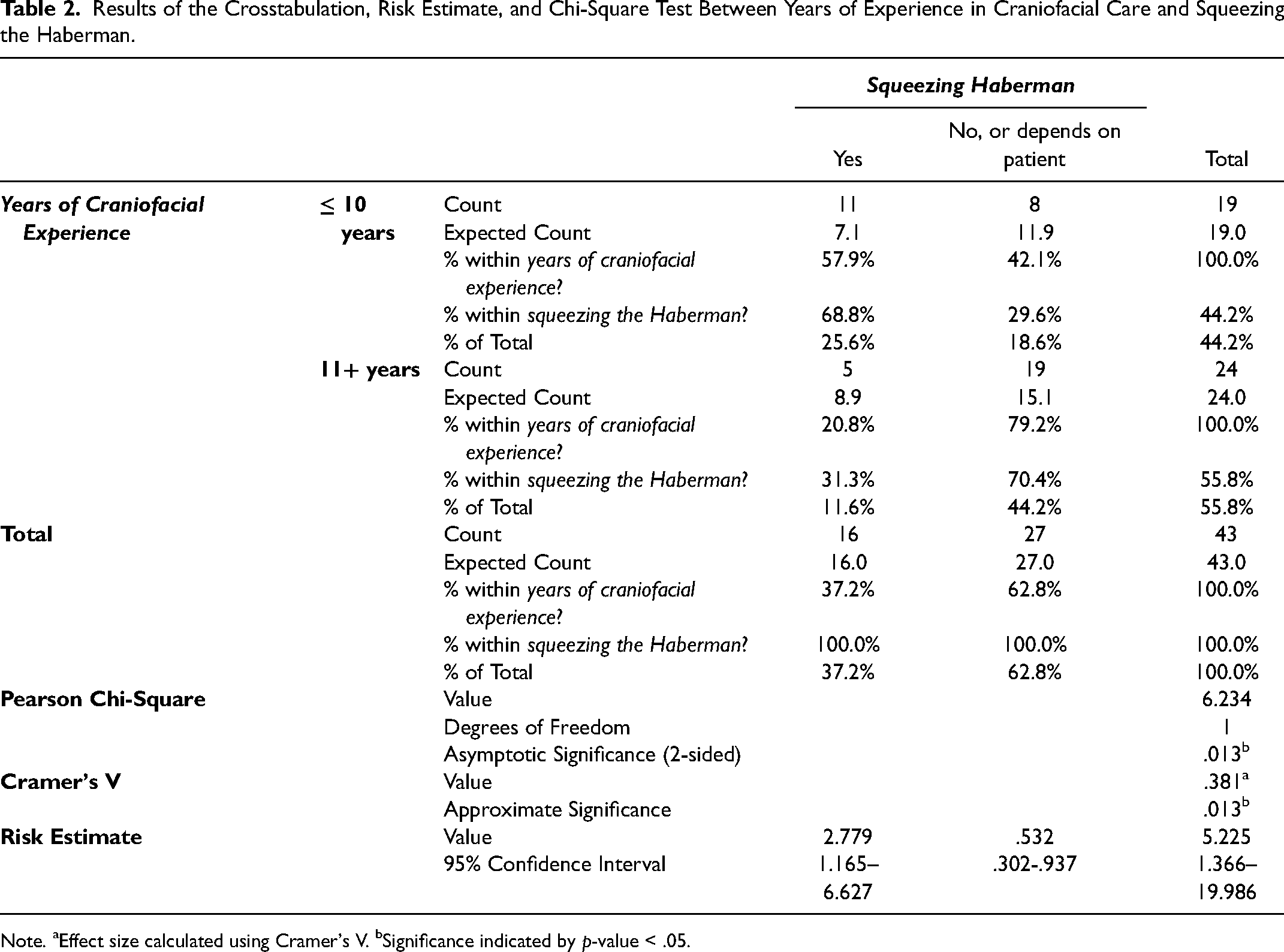
Note. aEffect size calculated using Cramer's V. bSignificance indicated by p-value < .05.
There was a statistically significant association between years of experience in the field* and likelihood of collaboration (p = .039; Table 3). This association was moderately strong, Cramer's V = -.268. The odds ratio of working collaboratively with another discipline while counseling parents/caregivers about feeding in providers with ≤ 20 years versus 21+ years’ experience was 5.185 (95% CI, 11.224–21.963). As such, providers with less experience practicing in their discipline are 5.185 times more likely to collaborate with other providers while counseling parents/caregivers than providers with more experience practicing in their discipline. There were no statistically significant associations between likelihood of collaboration and age of provider* (p = .084), discipline of provider* (p = 1.000), years of experience in craniofacial care (χ2(1) = 1.229, p = .268), or practice setting* (p = .721).
Results of the Crosstabulation, Risk Estimate, and Fisher's Exact Test Between Years of Experience in the Field and Working Collaboratively with Another Discipline While Counseling Parents/Caregivers About Feeding Infants with Cleft Palate.
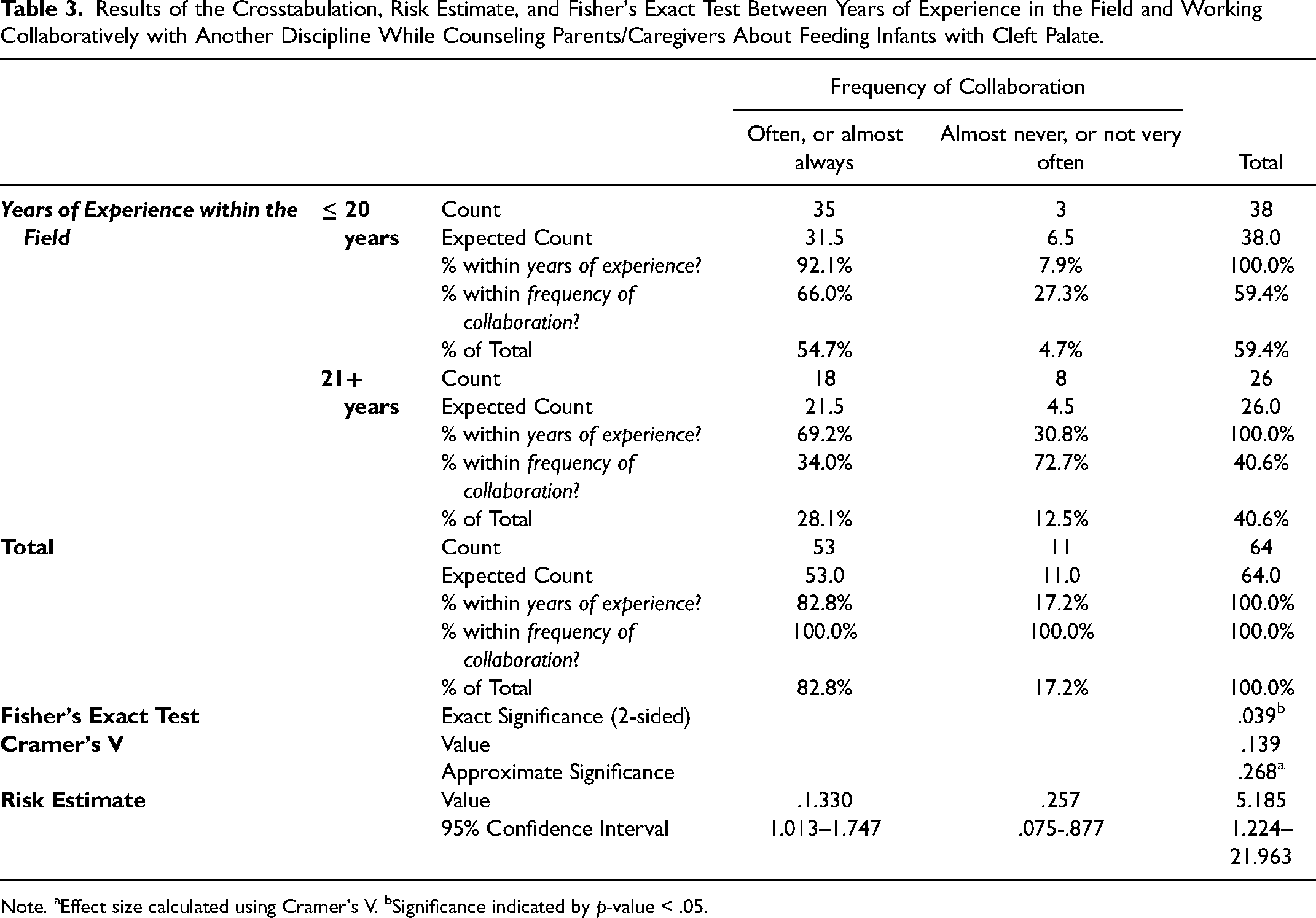
Note. aEffect size calculated using Cramer's V. bSignificance indicated by p-value < .05.
Discussion
Providing feeding services to infants with cleft palate spans across multiple disciplines, leading to the potential for variations in treatment patterns, training, and experience. Of the respondents in this survey, speech-language pathology was the most common discipline (followed by nursing), and the vast majority practiced in an outpatient setting. Variations were present across age and experience level. Experience level, both within discipline as well as craniofacial care specifically, were associated with variations in practice patterns. Despite these differences, similar assessment practices existed among respondents. The following will highlight specific findings of the present study in light of the previous literature.
Although a majority of respondents reported that coursework specific to feeding infants with cleft palate was not provided during their degree program, results indicate that assessment and intervention patterns within craniofacial care are overall consistent. Consistency may be secondary to training being provided on-the-job by practitioners with experience in craniofacial care and through continuing education opportunities provided by the same organization (American Cleft Palate-Craniofacial Association). On-the-job training may also explain why the majority of respondents indicated relying on their clinical expertise most when providing feeding services to this population.
Consistencies are present in overall assessment practices. Caregivers are feeding their infants during evaluation and treatment sessions while being given feedback by the provider. This practice is consistent with current early intervention practices. 21 Additionally, a majority of our survey respondents (86%) reported determining the appropriate flow rate when feeding infants with cleft palate by observing the infant's suck-swallow-breathe sequence, which takes into consideration the patient's ability to maintain physiologic stability including a safe swallow and appropriate respiration. Prior research on nipple flow rate indicates that flow rate varies widely 22 and can be impacted by several different factors, including the amount of compression applied, number of sucks an infant attempts, thickness of the milk, and swallow timing. 23 Evidence suggests that infants should use a flow rate that allows them to feed both safely and efficiently, not necessarily based the marketed flow rate related to infant age. 24 The results of the present study are consistent with those by Madhoun and colleagues, which reported that flow rate in the population of infants with cleft palate was not determined by age and that infants with cleft palate may benefit from moving to a faster flow rate earlier than their peers to improve feeding efficiency. 9
An overwhelming majority of providers in North America have access to and regularly utilize the Dr. Brown's System. In the present study, 99% of providers indicated having access to the Dr. Brown's bottle at their facility. Madhoun and colleagues reported that a majority (59%) of infants using a cleft-adapted bottle were using the Dr. Brown's at the time of their study. 9 The present study extends upon this finding, with 77% of respondents indicating that the Dr. Brown's bottle is typically the first bottle trialed when feeding an infant with cleft palate. This high prevalence of use across disciplines and provider settings may be related to several factors, including the movement toward more infant-directed versus caregiver-assisted feedings. 13 Other considerations in bottle selection may include cost, appearance, and functionality. At the time this survey was deployed, the average cost per bottle from common retailers was $30 (USD) for the Haberman, $26 for the Pigeon, $13 for the Dr. Brown's, and $4 for the Mead Johnson. With a cost variation of $26, caregivers may choose bottles that are toward the cheaper end of this range. Additionally, the visual difference between a Dr. Brown's cleft-adapted bottle and a standard bottle is nonexistent, which may be appealing to both providers and caregivers. 20 Further research is needed into caregiver perspectives surrounding feeding their infants with cleft palate.
Although a majority of respondents reported practice patterns were consistent, some differences were also noted. Use of the Haberman bottle varied among respondents, with some providers (37%) using the bottle as a caregiver-assisted system (with the feeder manually compressing the nipple during feedings) and others either never providing squeeze assistance (7%) or varying their recommendation by patient (56%). Specifically, providers who more recently began working in craniofacial care were more likely to squeeze the Haberman. Inconsistency with the Haberman being used as an infant-directed versus a caregiver-assisted system aligns with variations in current published literature. The Haberman manual 25 does not state that the nipple should be squeezed to assist with feedings, while publications by the ACPA Family Services (2009) 26 advise families to squeeze the nipple while the infant is sucking and to pause squeezing when the infant rests. Thus, it is evident that all providers are not using this bottle in the same way, and discrepancies in educational and printed literature may be leading to this variation in practice. Another inconsistency in practice patterns related to completion of feeding. The majority of providers in the present study said it was important to have infants finish feedings in under 30 minutes; however, respondents did not indicate routinely assessing or documenting bolus intake. Knowing the amount of volume needed to ensure appropriate weight gain would aid in determining the number of feedings needed per day and the appropriateness of a given flow rate. Additional variations in practice patterns exist relative to facility-specific guidelines (e.g., surgical post-operative care) as there are no standardized guidelines. 27 Additional research is necessary to assess variations in post-operative feeding guidelines following cleft repairs, specifically after cleft palate repair, and the functional implications.
Collaboration in feeding assessments of infants with cleft palate also varied among providers. Specifically, those providers with less experience in their discipline were more likely to collaborate with other professionals during feeding consultations. This difference may be related to several factors, including the recent shift in educational programs to focus on more interdisciplinary care and translational teams. 28 In such, recent graduates may be more likely to collaborate in healthcare settings. There is a continued need for further education and research regarding feeding infants with cleft palate in discipline-specific degree programs. Providers who see infants with a cleft palate less frequently, such as hospital labor and delivery units, neonatal intensive care units, and home-based early intervention programs, may be less likely to have training in this area based on availability of mentors. In the present study, on-the-job training was reported as a substantial training mechanism for this subspecialty. Lack of formal education in this area may be contributing to misinformation being provided to families, unnecessary nasogastric tube placement, inaccurate expectations for breastfeeding, or weight loss due to lack of availability of a cleft-adapted system at birth.14,29
Future Directions
This study has highlighted several areas for future investigation. While we primarily aimed to capture the practice patterns of feeding providers with experience in craniofacial care, it is also important to investigate the practice patterns of those professionals that may not regularly be involved in craniofacial care. Providers in certain settings (e.g., neonatal intensive care unit) may be the designated providers for feeding services for patients with cleft palate but encounter these individuals less frequently than those surveyed in the current study. Demographic variables, such as hospital size or geographic location, may be beneficial to consider in these future comparisons. Additional research into common training vessels and trends for this group of providers is also warranted. Lastly, to the best of our knowledge, there is no literature that links certain practice patterns (e.g., squeezing the Haberman) with a difference to intake or infant weight gain. It is likely that clinicians are relying on their clinical judgement for certain practice patterns when ample research does not exist.
Conclusion
Providers in North America who are regularly involved in feeding consultations for infants with cleft palate differ with respect to demographic characteristics despite quite similar practice patterns. While provider age and experience vary, the majority of providers are speech-language pathologists and work in an outpatient setting. Despite similar practice patterns and assessment characteristics, significant associations between provider demographics and practice patterns were observed. Across disciplines, practice knowledge surrounding feeding infants with cleft palate is typically gained through mentorship or on-the-job training.
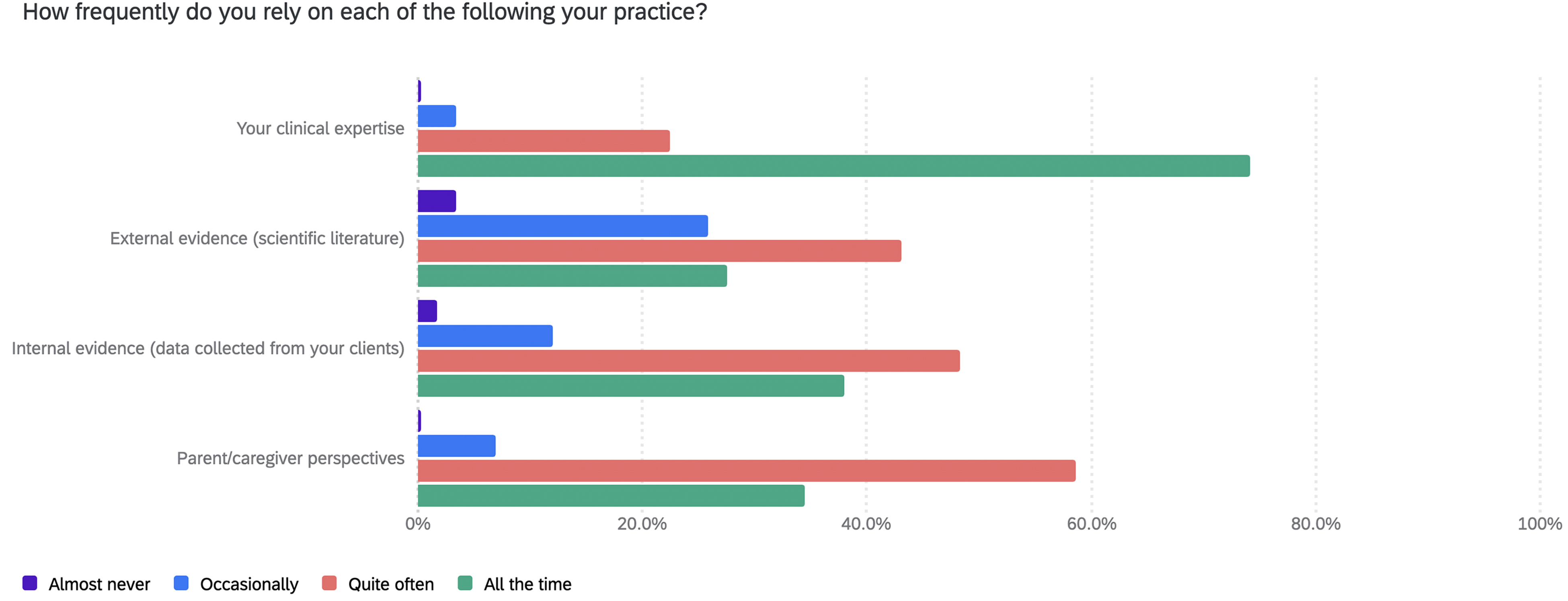
Participant responses to the question: How frequently do you rely on each of the following [components of evidence-based practice] in your practice?
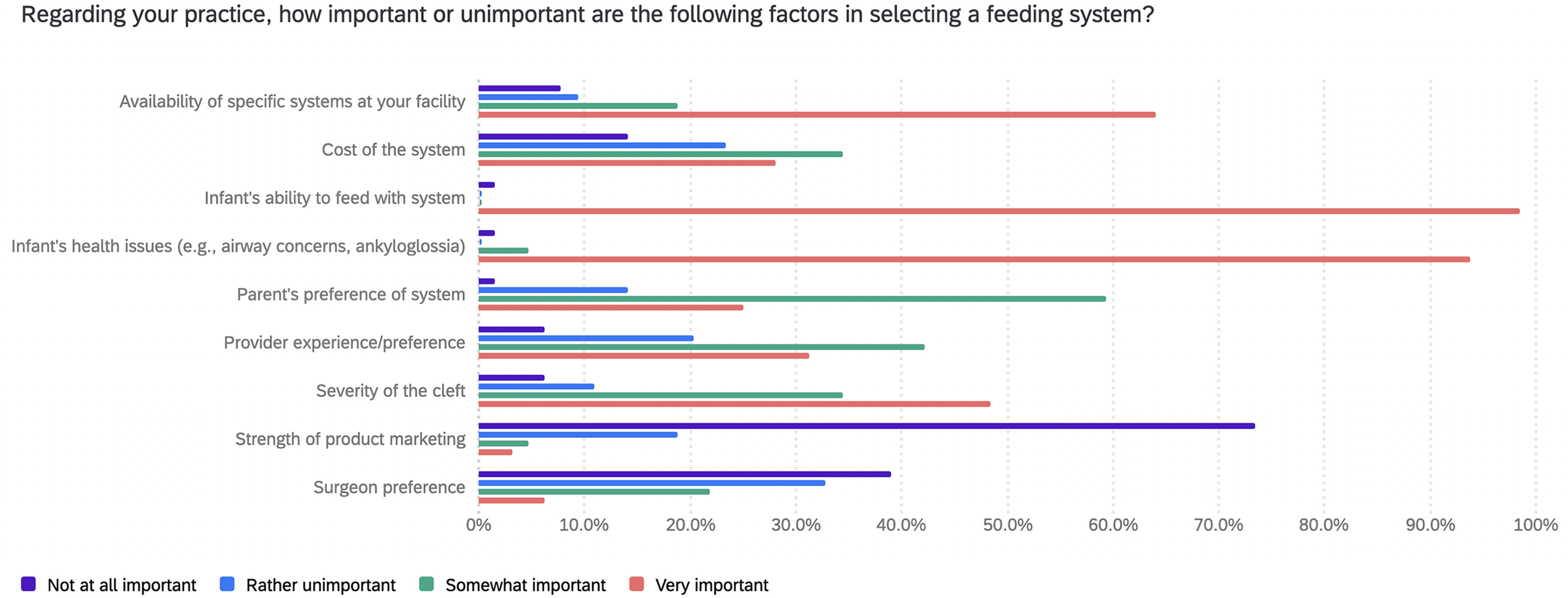
Participant responses to the question: Regarding your practice, how important or unimportant are the following factors in selecting a feeding system?
Footnotes
Acknowledgements
We would like to thank Dr. Mary Hardin-Jones for her contributions to this study and Dr. Bistra Anatchkova (Wyoming Survey and Analysis Center) for reviewing this survey prior to dissemination.
Research Ethics and Patient Consent:
We have no additional conflicts of interest to disclose and have adhered to all ethical guidelines. The University of Wyoming Institutional Review Board reviewed this study, which was considered exempt.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.