
Abstract
Objective
To review the available evidence on the use of the Buccal Fat Pad in primary and secondary Cleft Palate repair.
Methods
This is a narrative review. A computerized literature search was conducted for articles published till February 2022 using the Mesh phrases buccal fat pad AND cleft palate, Bichat's Fat pad AND cleft palate, buccal fat pad OR Bichats Fat pad AND cleft palate.
Results
A total of 35 articles were included in this review based on the set eligibility criteria. Most of the studies were retrospective case reviews (n = 16, 45.7%), and the aggregate number of patients from all included studies was 666. Reported uses of the buccal fat pad (BFP) in association with cleft palate repair include the closure of central cleft palate defect and nasal floor in primary cleft palate repair, oronasal fistula repair following primary repair of cleft palate, and closure of relieving incision defect in primary repair of cleft palate. Complications reported were 24 cases of Oronasal Fistula (ONF), 2 dehiscences, and 4 transient mucosal defects.
Conclusion
The high success rate, vascularity, ease of tissue harvest, and low donor site morbidity all support its use as an adjunct flap in cleft palate repair, especially in the closure of wide palatal clefts, to prevent post-palatal repair fistula, wound contracture, and subsequently velopharyngeal insufficiency and possibly midface hypoplasia.
Introduction
The occurrence of oronasal communication/fistula following initial surgical repair of the cleft palate remains a significant problem in cleft palate repair. 1 Identified risk factors include the wide cleft palate, technique of repair, skill of the surgeon among others. 2 Incidence of oronasal fistula has been reported to range from 5% to 60%.2–5 Modifications to techniques of repair and use of adjunctive flaps have been proposed to prevent and repair this relatively common complication of cleft palate repair.
The buccal fat pad (BFP) flap has been a useful adjunct in palatal defect closure, gaining popularity in recent years. 6 Its use was first documented by Egyedi for the closure of oro-antral and oro-nasal communications. 7 It has since been used in various oral reconstruction procedures including cleft palate repair. The BFP was first described by Heister in 1732, since then, extensive data has been gathered about its anatomy, embryology, and function.8,9 The BFP is composed of a central body and 4 diverging extensions: the buccal, pterygoid, superficial, and deep temporal processes. The largest and most superficial part, the buccal process, represents 30% to 40% of the BFP's weight. The blood supply is constituted of an abundant capillary network derived from branches of the maxillary artery. 8 Its rich vascularity, superficial location, proximity to the recipient site, and relatively low donor-site morbidity are the basis of reports of high success rates in BFP flap procedures. 10
Levi et al., 1 described a technique in which bilateral pedicled BFP is used in the closure of the exposed lateral palatal bone arising from the closure of the central hard palate defect. In addition, for palatal fistula repair, the buccal fat pad flap was placed as an added layer under the mucoperiosteal flaps. 1 Their report had 14 cases in all, 10 being primary repairs of cleft palate, and 4 palatal fistula repairs. No patients had complications related to the buccal fat pad flap or donor site perioperatively or postoperatively.
There are multiple published case reports and case series on the use of the BFP for cleft palate closure and this narrative review aims to highlight the outcomes of these reports and identified complications. This is aimed to provide some evidence for the cleft surgeon on this subject, on which decisions on its use for repair of the cleft palate or oronasal fistula closure can be based.
Methods
Eligibility Criteria
Only published articles such as case reports, case series, cohort studies, or randomized studies in which buccal pad of fat was used in the primary or secondary repair of cleft palate or used in the treatment of oronasal fistula occurring after primary repair of cleft palate were included in the review. The technique of repair of the cleft palate was not regarded.
Participants were individuals of all ages managed for cleft palate or oronasal fistula secondary to cleft palate. Also included were studies reporting the use of buccal fat pad for the repair of other intraoral defects in which data could be extracted on patients for whom buccal fat pad was used for cleft palate or oronasal fistula repair.
The intervention was cleft palate repair (unilateral, bilateral, or soft palate only) or oronasal fistula repair secondary to cleft palate using any cleft palate repair technique in combination with a buccal fat pad (unilateral or bilateral, pedicled or free graft) as an adjunct. The outcomes assessed were successful closure of the cleft palate/ oronasal fistula and report of any associated complications relating to the use of buccal fat pad post-surgery
Search Strategy and Selection of Studies
We conducted systematic searches for published articles in PubMed (NLM), Cochrane, Ovid Medline, and OpenGrey databases. The US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov) and the World Health Organization International Clinical Trials Registry (WHO clinical trials registry) were also searched for ongoing and past studies. Additional searches for relevant studies were done through the following methods: hand-search of the reference section of eligible studies and purposeful Google scholar searches. Only articles written in English or with English language translations were considered for the review. All databases were searched until February 2022.
The Mesh phrases used were buccal fat pad AND cleft palate, Bichat's Fat pad AND cleft palate, buccal fat pad OR Bichats Fat pad AND cleft palate.
Two of the authors (AAA and OAO) independently screened the titles and abstracts (when available) of all reports identified through electronic searches. The search was designed to be sensitive to include all available studies. For studies appearing to meet the inclusion criteria, or for which there was insufficient data in the title and abstract to make a clear decision, we obtained the full report. The full reports were also independently assessed by the first 2 authors to establish whether the publication met the inclusion criteria or not. Disagreements were resolved by the last author (WLA).
Data Extraction and Management
The first 2 authors (AAA and JO) independently extracted data from the included studies. There were no disagreements in data extraction. For each study, the following data were recorded (where available): Authors’ name and year of publication, study design, socio-demographic characteristics of participants, indications for use of the buccal fat pad, duration of the follow-up, and complications recorded. Extracted data were transferred to a Microsoft Excel data sheet for data clean up and analysis.
Results
A total of 40 full text of identified articles were retrieved, and 3 articles were excluded due to insufficient data while 2 articles were excluded as they were published in Chinese language and full text in English could not be retrieved. Hence, 35 articles made the final examination and analysis.
Most of the publications were published within the last decade (n = 21, 58.3%). Majority of the studies were retrospective case reviews (n = 16, 45.7%), followed by case reports (n = 9, 25.7%), case series (n = 4, 11.4%), prospective studies (n = 4, 11.4%), and randomized studies (n = 2, 5.7%). The reports consisted of a total of 666 patients, with an age range of 0.33–51 years. The sex of patients could only be retrieved from 17 articles, resulting in 238 males and 179 females. The reported follow-up period ranged from 3 weeks to 5 years. Reported uses of the BFP in association with cleft palate repair include the closure of central cleft palate defect and nasal floor in primary cleft palate repair, Oronasal Fistula (ONF) repair following primary cleft palate repair, and closure of relieving incision defect in primary cleft palate repair. Complications reported were 24 cases of ONF, 2 dehiscences, and 4 transient mucosal defects (Table 1).
Studies Included in the Review.
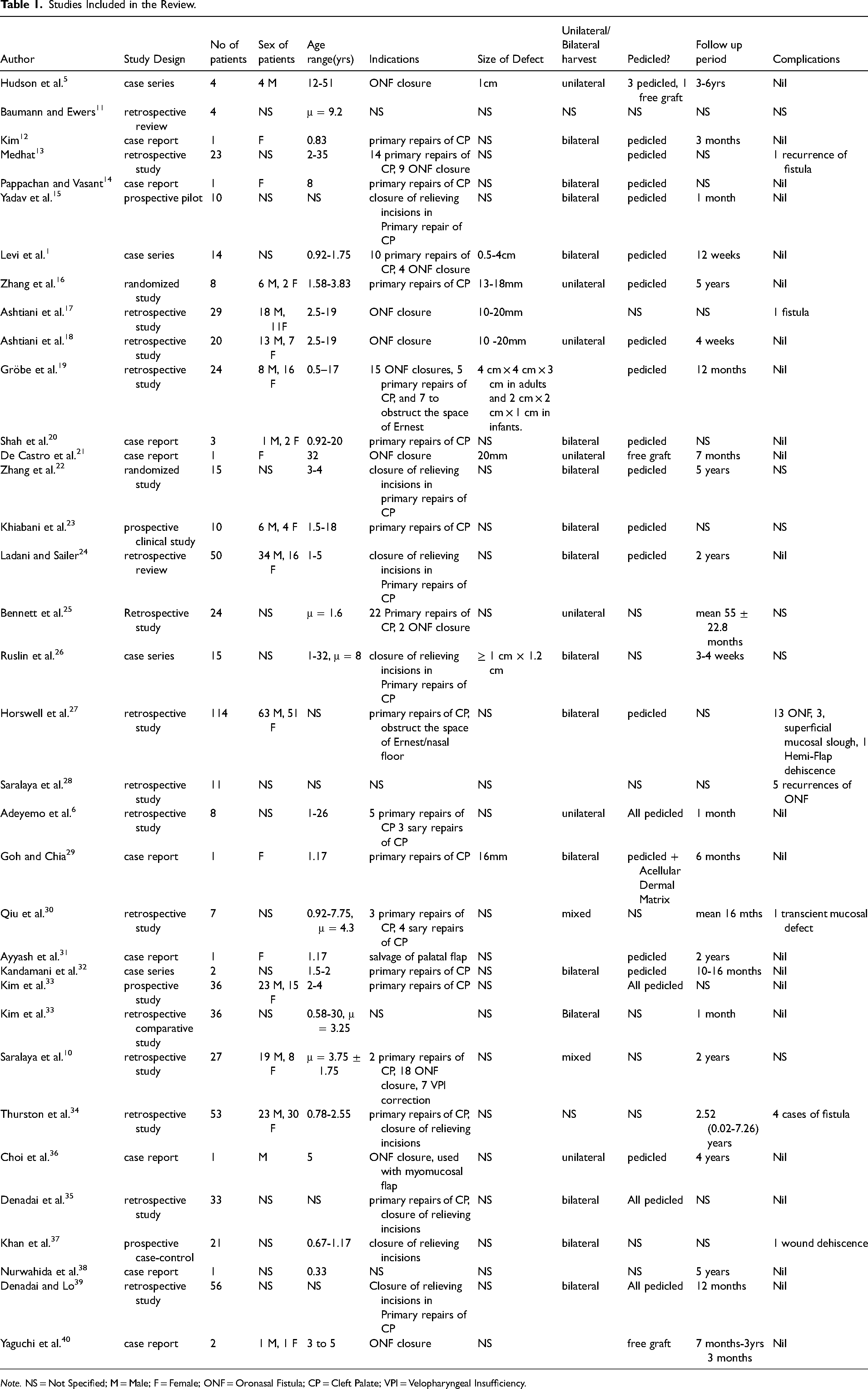
Note. NS = Not Specified; M = Male; F = Female; ONF = Oronasal Fistula; CP = Cleft Palate; VPI = Velopharyngeal Insufficiency.
Discussion
In the repair of the cleft palate, the junction of the hard and soft palate is the area associated with maximum tension, hence this region is most associated with the occurrence of complications such as wound dehiscence and oronasal fistula formation, and this remains a significant problem in cleft palate repair.19,26 Results from this study have shown that the BFP is a useful and reliable adjunct in the repair of the cleft palate, either in primary repair to reduce the likelihood of wound dehiscence and oronasal fistula formation, by providing an additional protective layer between the oral and nasal mucosa, or in secondary repair to manage oronasal fistula. In addition, there are a substantial number of reports on the use of the BFP in the obliteration of the lateral defect resulting from the bipedicled flap elevation, hence preventing exposure of bare palatal bone, and reducing contracture, which has been postulated to reduce transverse maxillary growth. A randomized study to assess the effect on maxillary growth when the lateral relieving incisions are filled with BFP or iodoform gauze found the difference in maxillary growth was statistically significant in favor of the BFP group. 22 However, further studies are still required to establish this finding.
The buccal pad of fat lies within the buccal space in the cheek, this space lies between the buccinator muscle medially, the deep cervical fascia, and muscles of facial expression anterolaterally, and the masticator space and parotid gland posteriorly. 8 It consists of a body and four processes. It is estimated to be about 10ml in volume and can be used to cover an area of about 10cm3. It is supplied by the buccal and deep temporal branches of the maxillary artery and the transverse facial branch of the superficial temporal artery and drained by the facial vein. 40 The volume of the transposable fat pad can vary considerably, and it must be handled very carefully at all times. 40 A detailed description of the anatomy and physiology of the buccal fat pad can be found in the literature.8,9
There has been an increase in interest in the use of the buccal fat pad in oral reconstruction as evidenced by many case reports and case series available on the subject. Following the first report of Egyedi in 1977, 7 many reports have followed, with clear evidence of its versatility and reliability in reconstruction within the oral cavity. Various reports have shown its use in the closure of oroantral communications/oronasal communication,41,42 primary and secondary cleft palate repair, 31 closure of soft tissue and bony defects in the oral cavity,43–45 closure of skull base defects, 46 interposition material in TMJ surgery, 47 sinus grafting, 48 facial sculpting and malar augmentation,49–51 periodontal surgery,52–54 dental pulp revascularization 55 and stem cell research. 56 This current study is focused on a narrative review of its use in cleft palate repair only.
Hudson et al., 5 were the first to publish a case series in the English language literature on the use of the pedicled buccal fat pad in the management of cleft palate. This was followed in 1998 by another article published in the Chinese language literature by Zhao et al. 57 Hudson et al., 5 detailed the use of the BFP in the closure of the alveolar cleft in 4 patients managed for cleft palate defect. The age of the patients in their series ranged from 12 to 51 years old, and the fat pad was used to close the dentoalveolar cleft following the placement of an iliac crest bone graft. No complications were recorded, and all cases were assessed to have healed satisfactorily. Zhao et al., 57 applied the BFP in primary cleft palate repair in a series of six patients in which it was used to cover the raw surface of the hard palate cleft and/or fill the dead space between the oral and nasal tissue layers, specifically at the junction of the hard and soft palate. They also reported uneventful recovery in all cases.
Hudson et al., 5 enumerated the advantages of the use of a buccal fat pad in the alveolar cleft closure to include the provision of vascular support to both the alveolar bone graft and the palatal soft tissues, promotion of secondary granulation thereby minimizing the chances of soft tissue wound dehiscence, obliteration of dead space between the oral and nasal cavities. The fat pad, by virtue of its physiologic composition, also provides a hydrophobic middle layer between the palatal mucosal flap and the bone graft. 40
The considerable number of reports on the use of buccal fat pad in oral reconstruction attest to its usefulness and increased acceptance by clinicians.20,58 The results of this study show that in the repair of the cleft palate, the BFP has found usefulness in areas such as primary and secondary repair of the cleft palate, obturation of lateral palatal mucoperiosteal defect in the bipedicled flap technique, adjunct for soft tissue coverage in alveolar cleft repair among others. In addition, it has been used in patients of a wide age range, from as young as 0.3 years to as old as 51 years.
The critical size of the cleft palate defect that can be repaired with the BFP is yet to be established, however, from our result, the largest size of the cleft palate defect in which the BFP was used was 2cm × 2cm × 1cm in infants and 4cm × 4cm × 3cm in adults. 19 Ashtiani et al., 18 recommended the use of the BFP in the closure of post cleft palate repair fistula of 1-2 cm in size. For other intraoral sites, the use of the BFP in the repair of defect sizes of up to 7cm × 4cm × 3cm has been reported. 44 In a prospective study by Kim et al., 32 in which the BFP was used as an adjunct in primary repair of the cleft palate in 36 patients specifically for prevention of ONF, compared to 29 patients in which it was not used, reported that no fistula was formed in the group with BFP closure, while 4(13.8%) of those who did not have their cleft repaired with BFP had a fistula. They found the use of BFP graft and the ratio of cleft width were significant factors in palatal fistula formation (P = .035, .003).
As highlighted by Gröbe et al. 18 the main objective of utilizing the BFP in palatal fistula repair or prevention is to relieve tension by transferring fatty tissue into an area with a lack of tissue at the closure site, resulting in tension at the junction of the hard and soft palate. The BFP is placed between the nasal layer and the oral mucosa and secured with sutures to the nasal mucosa.32,59 In wide palatal clefts in which approximation of the nasal layer is difficult or iatrogenic tears of the nasal layer is experienced during repair, the BFP can be mobilized and used in augmentation of the nasal layer repair as a prophylactic measure to prevent fistula formation. The use of the BFP in conjunction with Furlow's double opposing Z-plasty and its modifications have been found to be of clinical usefulness10,59 as it increases the volume of the soft palate while allowing maximum palate lengthening and at the same time fills the dead space underneath the oral mucosa. This may be for the purpose of Velopharyngeal Insufficiency (VPI) correction 10 or primary repair of cleft palate. 59
On complications of using the BFP in cleft palate repair, the result of this study shows that the associated complications are minimal. Of the combined 666 patients in the studies included in this review, only 30(4.5%) cases of complications were recorded. Most of the reported complications were recurrence of ONF. This low incidence of complications has been attributed to the good vascularity of the flap,8,10 hence guaranteeing its fidelity. In most of the series reviewed, epithelization of the flap occurred within 4-6 weeks,18,31,60 epithelization as early as 2 weeks post-surgery has also been documented. 1 Swelling of the cheeks is noted as sequelae from the harvest of the BFP and is expected to resolve in about 5 days post-op.10,17
Donor site morbidity is mild, usually restricted to postoperative edema and pain that resolves within the range of 2 to 5 days.28,60 To address the concern of possible facial asymmetry occurring following the harvest of BFP for cleft palate repair, Bennett et al., 24 analyzed retrospectively the cheek volume of 24 patients using 3D photogrammetry, the patients were their controls as only those with the unilateral harvest of the BFP were included in the study. They found the difference in volume between the flap and non-flap sides was not statistically significant (P = .81). In addition, an expert review of the patient photographs could not reliably identify the side from which the BFP was harvested. Similarly, Echlin et al., 61 in a cadaveric study, reported that the volume of the BFP used in cleft palate fistula repair constitutes just about one-third (36%) of the total volume of the fat pad, hence, two-thirds of the fat pad is still within the cheek, suggesting that any resulting change in cheek volume will be negligible. In addition, they also reported on the reach of the flap, in their study, approximately three-fourths of flaps would cover the mid-hard palate, and adequate closure of the soft palate and posterior hard palate could be achieved in all cases.
Using magnetic resonance imaging to study the surgical impact of the pedicled BFP flap on the levator veli palatini (LVP) muscle and surrounding velopharyngeal (VP) anatomy following primary palatoplasty, Kotlarek et al., 62 reported that the BFP flap creates a longer soft palate, with a greater distance between the posterior hard palate and the levator veli palatini, and a larger effective velopharyngeal ratio compared to conventional surgical techniques. Although the result of this study is preliminary, nonetheless, it provides an insight into the additional benefits of the BFP flap.
Conclusion
The role of the BFP in oral reconstruction is no more in doubt, and this review has highlighted its specific use in cleft palate surgery. The high success rate, vascularity, ease of tissue harvest, and low donor site morbidity all support its use as an adjunct flap in cleft palate repair. It could be a useful adjunct in the closure of wide palatal clefts, to prevent post palatal repair fistula, wound contracture, and subsequently velopharyngeal insufficiency, and possibly midface hypoplasia.
Footnotes
Authors’ Note
Ethics approval was not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.