
Abstract
Objectives
Few evidence-based psychosocial programs exist within craniofacial care. This study (a) assessed feasibility and acceptability of the Promoting Resilience in Stress Management-Parent (PRISM-P) intervention among caregivers of children with craniofacial conditions and (b) described barriers and facilitators of caregiver resilience to inform program adaptation.
Design
In this single-arm cohort study, participants completed a baseline demographic questionnaire, the PRISM-P program, and an exit interview.
Participants
Eligible individuals were English-speaking legal guardians of a child <12-years-old with a craniofacial condition.
Intervention
PRISM-P included 4 modules (stress-management, goal-setting, cognitive-restructuring, meaning-making) delivered in 2 one-on-one phone or videoconference sessions 1–2 weeks apart.
Main Outcome Measures
Feasibility was defined as >70% program completion among enrolled participants; acceptability was defined as >70% willingness to recommend PRISM-P. Intervention feedback and caregiver-perceived barriers and facilitators of resilience were summarized qualitatively.
Results
Twenty caregivers were approached and 12 (60%) enrolled. The majority were mothers (67%) of a child <1-year-old diagnosed with a cleft lip and/or palate (83%) or craniofacial microsomia (17%). Of these, 8 (67%) completed PRISM-P and 7 (58%) completed interviews; 4 (33%) were lost-to-follow-up before PRISM-P and 1 (8%) before the interview. Feedback was highly positive, with 100% willing to recommend PRISM-P. Perceived barriers to resilience included uncertainty about their child's health; facilitators included social support, parental identity, knowledge, and control.
Conclusions
PRISM-P was acceptable among caregivers of children with craniofacial conditions but not feasible based on program completion rates. Barriers and facilitators of resilience support the appropriateness of PRISM-P for this population and inform adaptation.
Introduction
Caregivers of children with congenital craniofacial conditions are at risk for psychological distress.1–3 Following their child's diagnosis, caregivers must take on a wealth of new information regarding their child's diagnosis, treatment, and long-term medical needs, as well as cope with their own complex emotions which may include grief, guilt, and anxiety about their child's future. 1 Thereafter, their child will follow a multidisciplinary treatment pathway throughout childhood and into adulthood. This represents an ongoing and chronic stressor for caregivers, as they must cope with novel challenges related to treatment, medical outcomes, and psychosocial adjustment at each phase of their child's life.1,4 These stressors may impact caregiver mental health, family functioning, and marital relationships and have negative downstream effects on children's own wellbeing.2,5–7 Despite these challenges, few evidence-based psychosocial interventions exist for caregivers of children with craniofacial conditions. 8
One intervention that offers potential for this population is the Promoting Resilience in Stress Management (PRISM) intervention.9,10 PRISM is a brief, skills-based program designed to enhance perceived resilience and mitigate psychological distress in adolescents and young adults (AYAs) with serious illness and their families.9,10 Within this program, resilience is operationalized as a process of identifying and harnessing new and existing resources to maintain wellbeing during and after any stressor.
11
The manualized PRISM program aims to bolster resilience by targeting four ‘resilience resources’: Stress Management, Goal-Setting, Cognitive Restructuring, and Meaning-Making
PRISM-P Intervention Sessions.
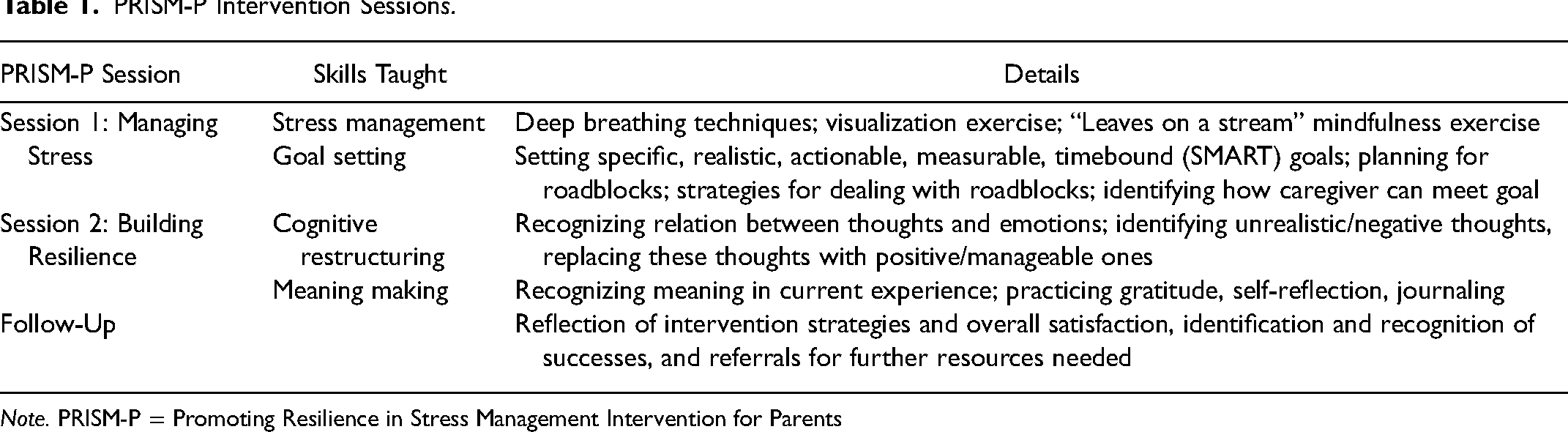
Note. PRISM-P = Promoting Resilience in Stress Management Intervention for Parents
Given its success in other populations, PRISM-P shows promise for caregivers of children with craniofacial conditions. First, specialist clinicians have highlighted the need to prevent as well as treat psychological distress in this population. 19 PRISM has been shown to have both a preventative and interventional effect on psychological wellbeing and thus has potential to meet this need.14,15,18 Second, extant studies have demonstrated that skills similar to those taught within PRISM (eg, active coping strategies, optimism) are associated with improved psychosocial health among caregivers of children with craniofacial conditions.6,20,21 Finally, PRISM can be successfully delivered by bachelor's- or master's-level staff 9 and thus has potential to be disseminated in a cost effective manner. 22 Though PRISM is designed to be applicable across different populations of individuals dealing with serious illness, it may be tailored based on the unique needs of the population to maximize success. Identifying factors that help or hinder caregivers’ ability to feel resilient (ie, facilitators or barriers of resilience) in the context of craniofacial conditions may critically inform future tailoring of PRISM and/or similar psychosocial interventions for this population.
The goals of the current study were to: (1) conduct a single-arm cohort study to assess whether the standard PRISM-P intervention is feasible and acceptable among caregivers of children diagnosed with craniofacial conditions; and (2) qualitatively describe caregiver-perceived barriers and facilitators of resilience in the context of their child's craniofacial condition to inform future adaptation of psychosocial interventions for this population.
Method
Participants
Ethical approval for this study was granted by the Institutional Review Board at Seattle Children's Hospital. Caregivers were eligible to participate in the intervention if they were the legal guardian of a child aged 12 years or under who had been diagnosed with a craniofacial condition and was receiving medical care at Seattle Children's Hospital; able to speak and read in English; and cognitively able to participate in interactive sessions. Though PRISM-P is designed for caregivers of children at any age, caregivers of children >12 years-old were not eligible to avoid potential contamination with a concurrent psychosocial intervention study for adolescents with craniofacial conditions. Multiple caregivers from the same family (ie, spouses, co-parents) were each eligible to enroll though were treated as separate/individual study participants.
Procedure
Recruitment was conducted from June 2019 through April 2020. Following a convenience sampling approach, the research team screened caregivers for eligibility via electronic health records. Eligible caregivers were introduced to the study via an emailed flyer or during their scheduled clinic visit by a known craniofacial provider. Consent conferences took place via phone or in-person during a subsequent clinic visit. Study staff reviewed the consent forms with potential participants including study activities, potential risks and benefits, and procedures to protect confidentiality and privacy, and provided opportunity for questions. All participants provided informed consent prior to starting the intervention. Enrolled participants were invited to complete a brief demographic survey for which they received a $10 gift card. Surveys were completed via paper-and-pencil or online via Research Electronic Data Capture (REDCap), a secure HIPAA-compliant web application for data collection, based on participant preference. Participants who completed the demographic survey then completed the PRISM-P program.
Following the PRISM-P program, participants completed a follow-up interview for which they received an additional $10 gift card. Follow-up interviews were conducted one-on-one via telephone by one of five trained research assistants who had not had prior contact with the participant. First, a series of structured questions were used to solicit intervention feedback, including willingness to recommend PRISM to other caregivers; general feedback regarding intervention content, timing, and delivery; and suggestions for improvement. Second, a series of semi-structured questions assessed caregivers’ definitions of resilience and their perceived barriers and facilitators of resilience in the context of their child's craniofacial condition and care. See Supplementary Table 1 for full interview guide. Interviews lasted approximately 10–15 min and were audio-recorded. Recordings were transcribed verbatim by trained research assistants.
Intervention Content & Delivery
PRISM-P is comprised of four skills-based components delivered 1:1.9,10 For this study, PRISM-P was offered as two 45–60-min sessions, each of which included two components (Table 1). Sessions were delivered 1–2 weeks apart via phone or videoconference. This format has been shown to be feasible and acceptable among caregivers of children with other chronic conditions primarily treated in an outpatient setting. 10 The first session (‘Managing Stress’) occurred within 2-weeks following completion of the baseline demographic survey and the second session (‘Building Resilience’) occurred 1–2 weeks later. To practice skills between sessions, participants received paper-pencil worksheets reviewing each PRISM skill and were invited to download the PRISM mobile app to practice the skills on their smartphone (Supplemental Figure 2). Sessions were delivered by trained bachelor- or masters-level professionals (‘coaches’) with oversight from licensed clinical psychologists, as indicated by previous models.9,10,15 Four coaches were trained based on established protocols involving eight hours of group-based in-person training, practice sessions, and role plays. All sessions were audio-recorded and monitored for fidelity by the lead coach (a licensed clinical psychologist) using a standardized tool. Specifically, the lead coach monitored fidelity of the first 2 sessions delivered by each coach and thereafter randomly selected 1 in every 3 sessions. This resulted in approximately 10 total hours of fidelity monitoring. Coaches received 30-min biweekly 1:1 supervision sessions which included directed feedback and re-training if necessary.
Data Analysis
Demographic and clinical variables were summarized descriptively. Feasibility of PRISM-P was assessed based on the percentage of enrolled participants who completed the two-session program, defined a priori as >70%. This was defined based on rates observed in prior studies examining feasibility of the PRISM program.9,10,12 Acceptability was assessed based on qualitative interview feedback, defined a priori as >70% of interviewed caregivers responding positively to the question, “Are you willing to recommend PRISM to other caregivers?”. All remaining follow-up interview data, including both program feedback and caregiver resilience experiences, were analyzed using directed content analysis 23 and following the Standards for Reporting Qualitative Research (SRQR) 24 guidelines. Coding was conducted by co-first authors (a developmental and research psychologist, respectively) using a combination of inductive and deductive approaches. For the first section of the follow-up interviews (intervention feedback), the coding team constructed an a priori codebook comprised of structural codes based on interview questions. Then, each coder independently coded the corresponding section of each transcript and met to resolve any discrepancies. For the second section of the follow-up interviews (resilience experiences), each coder first open-coded the corresponding section of each transcript to identify emergent codes. Coders then met to compare results and create a final codebook. Each coder independently re-coded each transcript with the final code book and met to resolve any coding discrepancies. Finally, codes were organized into broader categories.
Results
Sample Characteristics
Twenty eligible caregivers were approached over a 10-month recruitment period. Of these, 12 (60%) agreed to participate and provided informed consent, 8 (67%) of whom were co-enrolled with their spouse or partner (spouse/partners were treated as separate, independent study participants). Enrolled caregivers included 8 mothers (67%) and 4 fathers (33%) of children (Mage = 10 mos., SD = 3 mos., range = 1–17 mos.) diagnosed with cleft lip and/or palate (CL/P; 83%) or craniofacial microsomia (CFM; 17%). There were no consistent differences between caregivers who enrolled vs. did not enroll based on child age or diagnosis; the most common reason for not enrolling in the study was a lack of perceived time.
Four caregivers were lost-to-follow-up before completing any study components. Thus, the final sample included 8 caregivers (Table 2): 6 mothers (75%) and 2 fathers (25%) among whom 4 (50%) were co-enrolled with their spouse or partner (ie, 2 mother/father couples). Sample characteristics are shown in Table 2. Caregivers were 32 years-old on average (SD = 7 years). The majority self-identified their race as White (75%), followed by Asian (13%), or more than one race (13%). All self-identified their ethnicity as non-Hispanic (100%).
Demographic Information for Study Participants (N = 8).
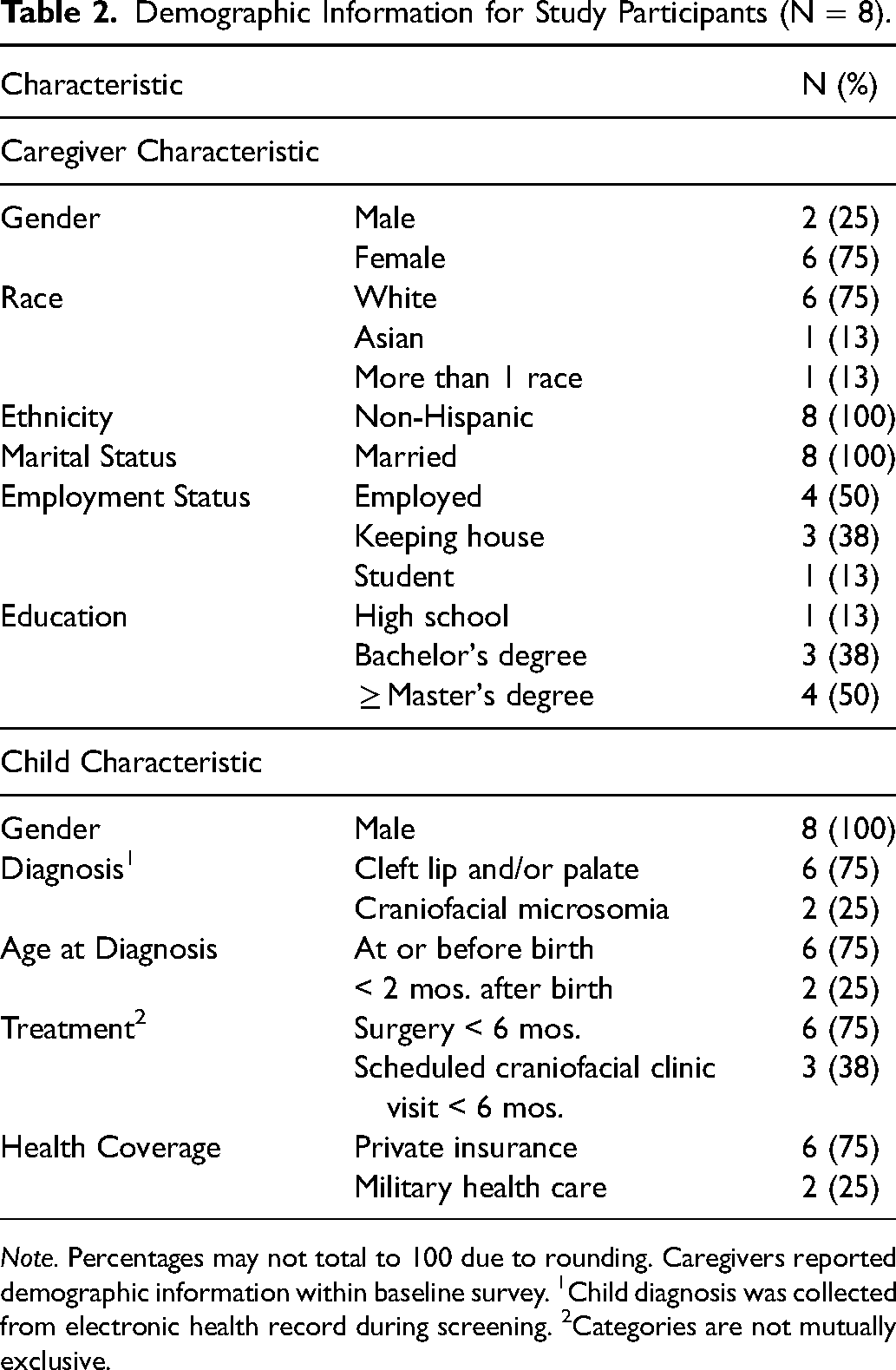
Note. Percentages may not total to 100 due to rounding. Caregivers reported demographic information within baseline survey. 1Child diagnosis was collected from electronic health record during screening. 2Categories are not mutually exclusive.
Feasibility of PRISM-P
Feasibility was determined based on the proportion of enrolled caregivers who completed the PRISM-P intervention. Of the 12 caregivers who enrolled in the study, 8 (67%) began and completed the two-session program. The median number of days between sessions was 11 and all sessions were delivered with 100% fidelity.
Acceptability of the PRISM-P
Seven participants completed feedback interviews (58% of enrolled caregivers, 88% of caregivers who completed the program). One caregiver was lost-to-follow-up after completing PRISM-P but prior to their interview. The median number of days between intervention completion and follow-up interviews was 23. Among those who completed interviews, all 7 (100%) provided positive responses to the question, “Are you willing to recommend PRISM to other caregivers?” Five structural codes described caregivers’ additional feedback regarding the PRISM-P program (Table 3). Overall, feedback was highly positive. Regarding
Acceptability Analysis Codes and Exemplar Quotes
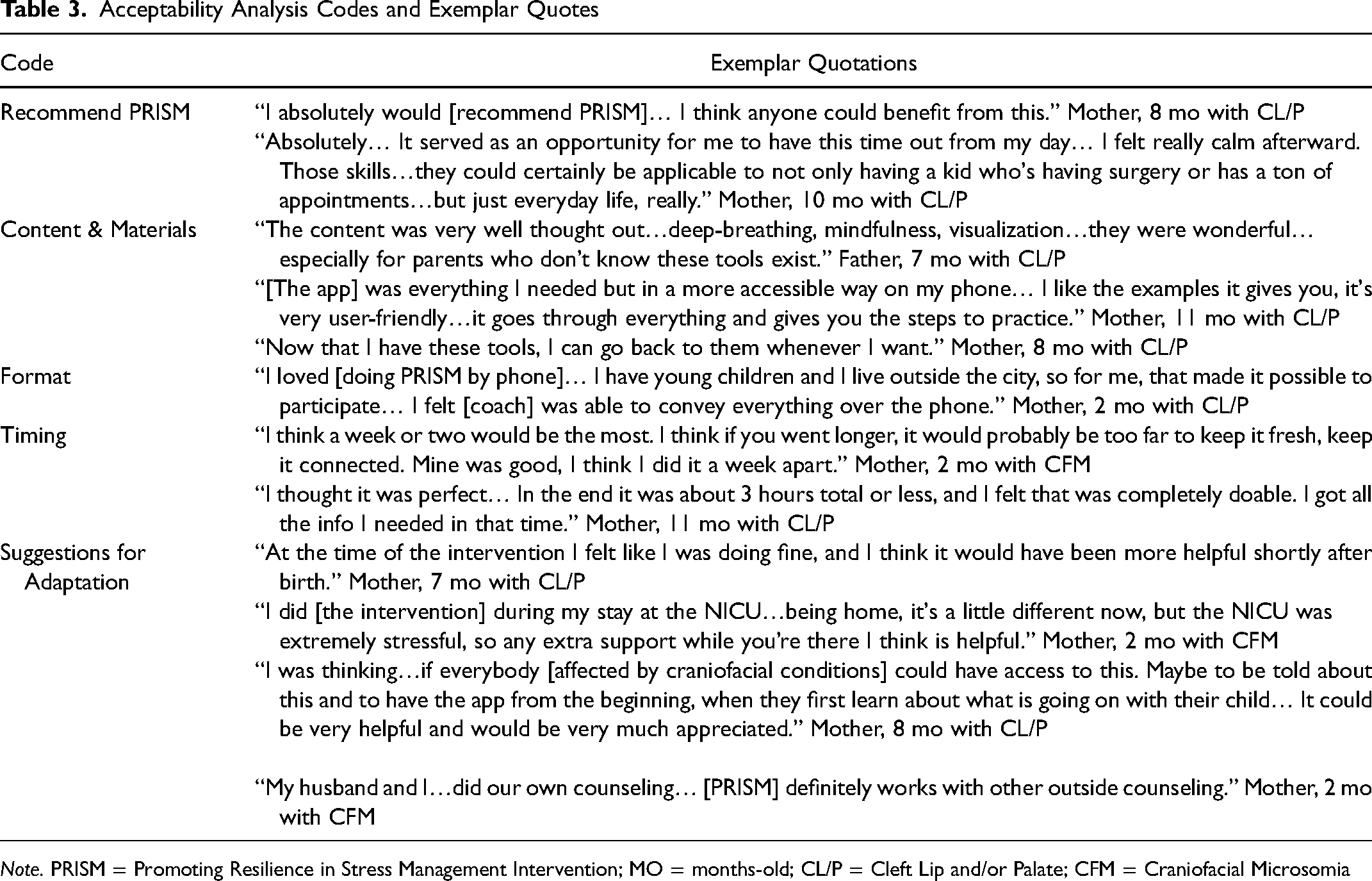
Note. PRISM = Promoting Resilience in Stress Management Intervention; MO = months-old; CL/P = Cleft Lip and/or Palate; CFM = Craniofacial Microsomia
Caregiver Perceptions of Resilience
Caregivers’ perceptions of resilience were organized into three categories: definitions, facilitators, and barriers of resilience (Table 4).
Caregiver Perceptions of Resilience Codes and Exemplar Quotes.
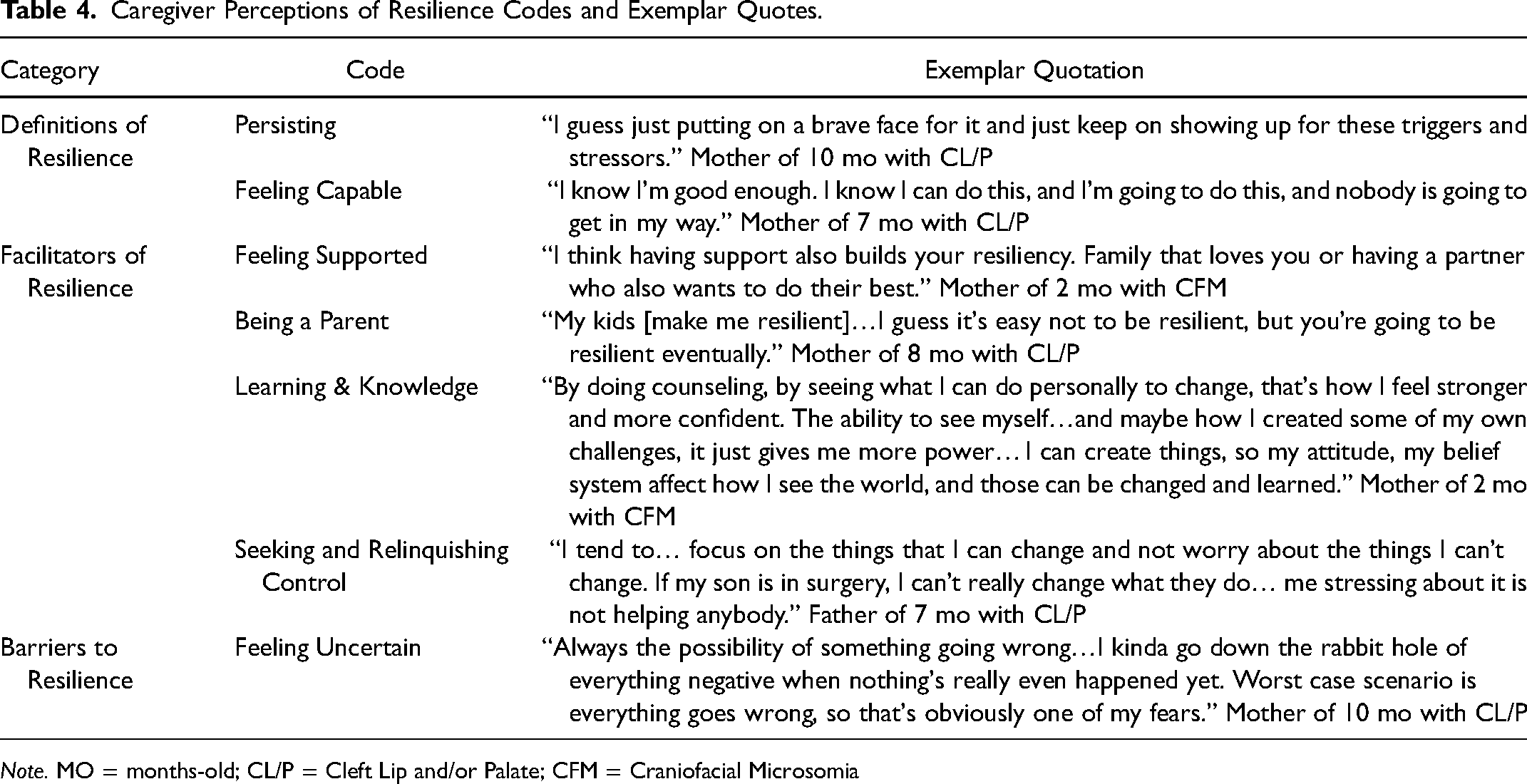
Note. MO = months-old; CL/P = Cleft Lip and/or Palate; CFM = Craniofacial Microsomia
“There's so much that goes into it, and just focusing on one day at a time. One little chunk of progress at a time.”
They also described resilience as “Having been through the NICU, like that's built resiliency because you went through something pretty challenging, and you’re through it, and it builds that strength muscle of knowing that you’re capable of challenges.”
“[My husband] is my closest support system… we’re really close with my parents so that's been helpful too.”
Some caregivers described
“Being a mom, you know, being giving to your kids. There's not really a choice. I mean you just wake up and you gotta take care of them. But it builds resiliency.”
Caregivers also described “I think being informed about everything. Knowing the facts on things instead of being in the dark or not really interested in it. The doctors and the people that help you to understand when you really have no clue about it, I think that helps me to be resilient—learning and understanding.”
Finally, caregivers described a process of
“The patient's perception of control is a large part of resilience. Because if it feels like you don’t have control of the situation, then that tends towards more anxiety and more inaction. If you feel like you have control, then you can take action, which is what resilience is all about.”
Many caregivers also acknowledged the utility of learning to relinquish control, particularly concerning their child's treatment. One mother of a 10-month-old with CL/P described this process, saying, “I feel like I’m at the point where I just kind of roll with it pretty well now. I guess just accepting that it's all part of a bigger plan that [hospital] has for [child] and that I really don’t have much say in it anyways. I just have to show up and be the mom and let the surgeons be the surgeons and let the doctors be the doctors and the nurses be the nurses.”
“Give me confirmation if [child's surgery] is going to happen like it's scheduled or if it's going to get canceled like the last time… we don’t know if it's going to get canceled again or if it's going to happen… they haven’t let us know so now we’re like, ‘uh?’ That would be helpful.”
Caregivers also described uncertainty about how their child's craniofacial condition may affect their future, both in terms of their physical health and psychosocial adjustment. One mother of a 2-month-old with CFM described this experience, saying, “What worries me? How he's going to fit in with his peers. Is he going to be made fun of? Is he going to have friends because he looks differently? Also, I mean, the surgery's coming up, like his breathing, heart, there's the medical side of it, it's scary… but then there's like the social part. How people are going to… mostly, how he's going to feel himself?”
Discussion
Having a child with a craniofacial condition can be highly stressful for caregivers 1 yet evidence-based psychosocial interventions for this population are lacking. 8 In the current study, we aimed to examine feasibility and acceptability of the Promoting Resilience in Stress Management for Parents (PRISM-P) intervention for caregivers of children born with craniofacial conditions and describe caregiver-perceived barriers and facilitators of resilience to inform future program tailoring. Results indicated that (a) PRISM-P was not feasible based on program completion rates due to early passive attrition, though retention was high among those who began the program; (b) PRISM-P was acceptable and program feedback was highly positive; and (c) caregivers’ perceived contributors and inhibitors of resilience were generally well-aligned with skills taught in PRISM-P, though also suggested novel intervention targets for this population.
Enrollment rates were similar to other PRISM studies,9,10,12 suggesting there is general interest in and a need for psychosocial supportive care programs among caregivers of children with craniofacial conditions. Passive attrition between enrollment and the first intervention session was higher than expected, though it is unlikely that session-related burden or content concerns were driving factors as these caregivers were lost to follow up before completing any study components. Rather, some caregivers may have enrolled initially due to social desirability factors or lacked time to continue following enrollment. Indeed, other PRISM studies have identified perceived lack of time and scheduling challenges as key barriers to participation.10,18,25 This suggests that successful delivery of psychosocial programs in this population may require novel strategies to promote retention, such as truncating timelines between enrollment and intervention delivery, combining interventions with in-person clinical care, or strengthening follow-up efforts to promote engagement. Notably, period effects may also have influenced retention in this instance. Most attrition occurred during the early weeks of the COVID-19 pandemic, a time in which caregivers of children with craniofacial conditions experienced elevated stress related to managing their child's medical needs in a rapidly shifting hospital environment 26 and participation in additional research may have been too burdensome.
Despite attrition, PRISM-P was well-received by those who completed the program. All caregivers who completed baseline surveys subsequently completed both PRISM-P sessions, aligning with prior PRISM studies demonstrating high levels of engagement among those who begin the program.12,15,18 PRISM-P was also highly acceptable, with acceptability rates mirroring those observed in other caregiver and patient populations,9,10,12 and program feedback was positive overall. Caregivers found program content helpful; perceived the length and timing between session as appropriate; and appreciated flexible modes of delivery. This suggests that skill-based interventions are appealing to this population and that offering remote options (eg, phone or videoconference) enables participation for busy caregivers. Regarding timing of delivery, caregivers suggested that PRISM would be most useful if delivered during the postnatal period and/or to caregivers whose child had required a stay in the neonatal intensive care unit (NICU). Though this suggestion may be specific to the needs of caregivers of young children with craniofacial conditions, it aligns with extant research describing the stressful nature of the postnatal period 1 and the unique needs of NICU caregivers.27,28 Thus, psychosocial programs such as PRISM-P may be maximally beneficial for parents of young children in these contexts.
Caregivers’ perceptions of resilience were generally well-aligned with extant resilience literature and reflected content and skills taught within the PRISM program. This suggests that program content was appropriate for this population and that caregivers identified with and/or adopted concepts learned through the program. Caregivers’ definitions of resilience focused on personal strength and resilience as an evolving process. This is well-aligned with definitions described by other caregiver populations and taught within the PRISM program (ie, resilience defined as a process of harnessing resources to maintain wellbeing).11,29,30 Caregivers also described resilience barriers (ie, worry, uncertainty) and facilitators (ie, learning to seek vs. relinquish control) that are targeted by existing PRISM skills. For example, PRISM's “Catching Negative Self-Talk” skill teaches participants to manage worry by distinguishing what is uncontrollable (ie, situational factors) from what is controllable (ie, one's response to the situation) and to use cognitive reframing to address the latter.9,10 Caregivers also described unique facilitators of resilience that inform novel intervention targets and avenues for program tailoring. Specifically, caregivers described learning, becoming knowledgeable, and drawing on their identity as a parent as facilitators of resilience. Thus, programs like PRISM-P may benefit from extending behavioral skills such as goal setting to focus on caregivers’ knowledge-related goals; adding components focused on medical and/or psychosocial education in the context of craniofacial care; and integrating self-affirmation skills that encourage caregivers to reflect on their parental roles and identities as a source of strength. Future studies should also examine the extent to which these factors are unique to caregivers of infants with craniofacial conditions or extend to caregivers of older children.
Limitations
Findings should be considered in light of methodological limitations. First, we did not collect feedback from those who were lost to follow-up after enrolling, which limited our ability to understand and address reasons for attrition. Second, sample homogeneity limits generalizability of findings. Eligibility criteria were not limited to caregivers of infants or children with specific craniofacial conditions. However, our recruitment approach involved introducing the study during a scheduled craniofacial clinic visit. Thus, most families we approached were those with children <1 year-old with CL/P who tended to have more frequent clinic visits. Thus, it is unclear whether these findings would generalize to caregivers of older children or caregivers of children with other craniofacial conditions. Additionally, most participating caregivers were White, non-Hispanic, married, and highly educated mothers; and, as half of participating caregivers were co-enrolled with their spouse, our sample represented a limited number of families. Thus, an important future direction will be examining the feasibility and acceptability of this program in a larger, more diverse caregiver sample including caregivers from racially minoritized groups; LGBTQ + caregivers; fathers; and single-parent caregivers. Finally, this study overlapped with the onset of the COVID-19 pandemic, which truncated our enrollment window and potentially influenced attrition, data completion, and caregivers’ perspectives on resilience. Future studies should replicate these findings in other temporal contexts.
Conclusion
This small-scale feasibility study demonstrates the potential of the PRISM-P intervention for caregivers of children with craniofacial conditions. Our findings suggest that psychosocial interventions are acceptable and well-received within this population, though participant retention may be a feasibility challenge. Our qualitative findings contribute to an ongoing discussion regarding what constitutes resilience in the context of long-term health conditions. Given the current lack of evidence for psychosocial interventions in this population, this study addresses an important gap by providing preliminary evidence for the potential of psychosocial supportive care and novel insights informing the design and delivery of future trials.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231157449 - Supplemental material for Feasibility and Acceptability of the Promoting Resilience in Stress Management-Parent (PRISM-P) Intervention for Caregivers of Children with Craniofacial Conditions
Supplemental material, sj-docx-1-cpc-10.1177_10556656231157449 for Feasibility and Acceptability of the Promoting Resilience in Stress Management-Parent (PRISM-P) Intervention for Caregivers of Children with Craniofacial Conditions by Kaitlyn M. Fladeboe, Nicola Marie Stock and Carrie L. Heike, Kelly N. Evans, Courtney Junkins, Laura Stueckle, Alison O’Daffer, Abby R. Rosenberg, Joyce P. Yi-Frazier in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656231157449 - Supplemental material for Feasibility and Acceptability of the Promoting Resilience in Stress Management-Parent (PRISM-P) Intervention for Caregivers of Children with Craniofacial Conditions
Supplemental material, sj-docx-2-cpc-10.1177_10556656231157449 for Feasibility and Acceptability of the Promoting Resilience in Stress Management-Parent (PRISM-P) Intervention for Caregivers of Children with Craniofacial Conditions by Kaitlyn M. Fladeboe, Nicola Marie Stock and Carrie L. Heike, Kelly N. Evans, Courtney Junkins, Laura Stueckle, Alison O’Daffer, Abby R. Rosenberg, Joyce P. Yi-Frazier in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.