
Abstract
Objective
To determine associations of demographic, morphologic, and treatment protocol parameters with quality of life (QoL), appearance/speech satisfaction, and psychological adjustment.
Design
Observational study utilizing retrospective report of protocol variables and current outcome variables.
Setting
Six North American cleft treatment clinics.
Participants
Children, ages 8.0–10.99 years, with Cleft Lip ± Alveolus, Cleft Palate, Cleft Lip and Palate, and parents (N = 284).
Outcome Measures
Pediatric QoL Inventory (PedsQL): Parent, Child, Family Impact Module (FIM); Patient Reported Outcome Measurement Information System (PROMIS); Child Behavior Checklist (CBCL); CLEFT-Q.
Results
Outcome scores were average with few differences by cleft type. Multiple regression analyses yielded significant associations (Ps < .05) between socioeconomic status, race, and age at assessment and parent- and self-reported measures. Females had higher PROMIS Depression (β=.20) but lower CBCL Affective (β = −.16) and PROMIS Stigma scores (β= −.24). Incomplete cleft lip was associated with lower PROMIS Depression, and more positive ratings of CLEFT-Q: Nose, Nostril, Lip Scar; CBCL Competence scores, (βs = −.17 to .17). Younger Age at Lip Closure was associated with higher CBCL School Competence (β= −.18). Younger Age at Palate Closure was associated with higher Child PedsQL Total, Physical, Psychosocial QoL, and better CLEFT-Q Speech Function (βs = −.18 to −.15). Furlow Palatoplasty was associated with more CBCL Externalizing Problems (β = .17) higher CBCL Activities (β = .16). For all diagnoses, fewer Total Cleft-Related Surgeries was associated with lower PROMIS Stigma and higher CBCL Total Competence and Activities (βs = −.16 to .15).
Conclusions
Demographic characteristics, lip morphology, and treatment variables are related to later psychological functioning.
Introduction
Children born with cleft lip and/or palate (CL/P) undergo multiple surgical procedures during infancy and early childhood to improve facial appearance/function and related psychosocial well-being. Published treatment guidelines for CL/P provide wide latitude for the types and timing of treatments. 1 While the exact number of protocols utilized in North America is unknown, clinical experience suggests that there is considerable treatment protocol variation within and across teams. Thus, the number and type of treatments provided to children with CL/P differ widely and can impact care-related burdens for children and families. 2
While there is a relatively large literature regarding psychosocial functioning and quality of life in youth with CL/P,3–5 few studies link psychosocial outcomes to treatment protocol variations. For example, Eurocleft 6 did not formally assess psychosocial outcomes following cleft treatment protocols, although patient satisfaction with treatment was generally high. Using data from Scandcleft, Feragen et al., 7 observed that while the majority of parents were satisfied with their child's appearance at 5 years of age regardless of treatment protocol, one surgical protocol was associated with greater post-operative anxiety and coping difficulties. Notably, Hentges et al. 8 found that younger age at lip repair (neonatal vs 3–4 months) was associated with better cognitive development and school achievement at age 7 in a UK-based sample of children with CL/P. Another recent study observed that greater numbers of CL/P surgeries performed during childhood, specifically between the ages of 8–10 years, were related to increased anxiety and depressive symptoms during adolescence. 9 To date, there has not been a systematic, multi-site study in North America that has investigated treatment protocol outcomes for CL/P as they affect the children's quality of life (QoL), psychosocial adjustment, appearance and speech self-perceptions, and academic functioning. To address this gap, the Americleft Psychosocial Group, an arm of the larger Americleft Project, was initiated to evaluate treatment-related psychosocial outcomes among patients with CL/P in North America. 10 This group developed a protocol for psychosocial outcomes assessment and designed a multi-site project to evaluate psychological outcomes related to the treatment protocol implemented for children ages 8–10 with CL/P. 11 The primary aim of the Americleft Psychosocial Outcomes study was to determine if child- and parent-rated psychosocial outcomes (eg, health-related quality of life (HRQoL), adjustment, speech, and appearance satisfaction) differ based on the treatment protocol implemented for an individual child (eg, age at lip and palate repair; total number of surgeries).
Using data from the Americleft Psychosocial Outcomes Study, this paper addresses the following questions: 1) Do psychological adjustment and QoL differ by cleft type? and 2) Which demographic, morphologic, and treatment protocol parameters relate to child- and/or parent-reported ratings of QoL, appearance and speech satisfaction, and adjustment by cleft type?
Materials and Methods
Human Subjects Protection
Procedures were approved by each site's Institutional Review Board. All parents provided written informed consent, and all minors provided assent.
Participants
Children, ages 8–10 years old (N = 358), with a confirmed diagnosis of CL/P were consecutively recruited between 2016 and 2019 across six sites. To be eligible, the child had to be willing and able to provide assent prior to participation in the study, be willing to comply with all study procedures, and be able to read or understand English or Spanish. Children diagnosed with craniofacial syndromes not believed to have a greater impact beyond that of the cleft (eg, Pierre Robin Sequence without tracheostomy and Van der Woude Syndrome) were eligible to participate. Child exclusion criteria were as follows: 1) Child has a significant medical condition that might have a greater impact on psychological adjustment, appearance, or learning than the cleft diagnosis [e.g., cardiac problems, multiple congenital problems, head injury, prematurity (< 34 weeks gestational age)]; 2) Child has a craniofacial syndrome that would be anticipated to have a greater potential impact on psychological adjustment, appearance, or learning than CL/P (eg, Apert syndrome, craniofacial microsomia, Treacher Collins syndrome, craniosynostosis, 22q11.2 deletion syndrome, Fetal Alcohol Syndrome); 3) Child is unwilling to provide assent; and 4) Child has significant cognitive impairment that affects his/her ability to reliably respond to questionnaires.
Parents/legal guardians of children with CL/P (N = 391) also took part. Parents/legal guardians were eligible to participate if they were at least 18 years old, were willing to provide written informed consent, and able to read English or Spanish. Parents/legal guardians of a child with cognitive impairment or who did not provide assent were eligible to complete parent questionnaires. Parent/legal guardian exclusion criteria included: 1) Factors that would preclude the participant's full compliance with or completion of the study (eg, visual impairment, significant cognitive or psychiatric problems); and 2) Parent was unwilling to provide consent for self or child participation in the study. Both parents could participate so long as eligibility criteria were met. Data from the parent/legal guardian who identified as the child's primary caregiver were used in analyses.
Children enrolled in the Americleft study who had a history of adoption (N = 113) were excluded from the present analyses because of limited treatment records. Thus, the current study included data reported by 284 participants (258 children and their caregivers; 26 caregivers only).
Sites
The six participating cleft teams included: Shriners Hospitals for Children, Chicago, IL; The University of Iowa, Iowa City, IA; Nationwide Children's Hospital, Columbus, OH; The Hospital for Sick Children in Toronto, Canada; The Lancaster Cleft Palate Clinic, Lancaster, PA, and Children's Medical Center (Dallas, TX). Nationwide Children's Hospital served as data coordination site (Table 1). Sites were selected to ensure representation of large and small cleft teams, variation in treatment protocols, and geographic diversity. 11
Participant Characteristics.
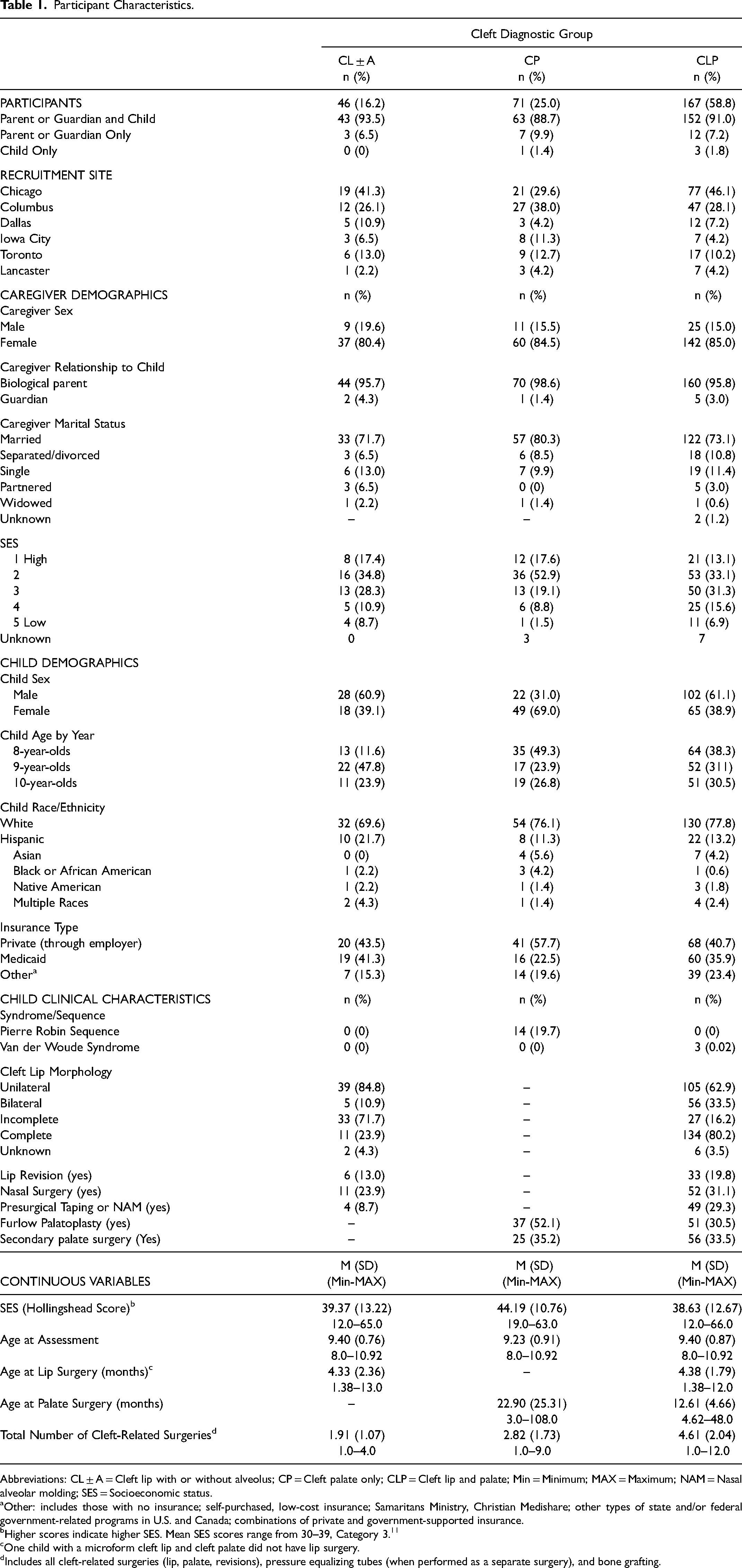
Abbreviations: CL ± A = Cleft lip with or without alveolus; CP = Cleft palate only; CLP = Cleft lip and palate; Min = Minimum; MAX = Maximum; NAM = Nasal alveolar molding; SES = Socioeconomic status.
Other: includes those with no insurance; self-purchased, low-cost insurance; Samaritans Ministry, Christian Medishare; other types of state and/or federal government-related programs in U.S. and Canada; combinations of private and government-supported insurance.
Higher scores indicate higher SES. Mean SES scores range from 30–39, Category 3. 11
One child with a microform cleft lip and cleft palate did not have lip surgery.
Includes all cleft-related surgeries (lip, palate, revisions), pressure equalizing tubes (when performed as a separate surgery), and bone grafting.
Procedures
Following site specific IRB parameters, potential participants were identified from medical chart reviews or were approached by site research team members at the time of a routine clinic appointment. Potential participants identified prior to their upcoming clinic visits received letters, emails, or phone calls of invitation to participate in the study. For families who expressed interest, informed consent forms were reviewed, questions were answered, and written parental consent was obtained, along with verbal or written assent from children.
Parents and children completed questionnaires via paper/pencil or online via REDCap. Parents were interviewed about their child's treatment history. A chart review was conducted by research team members to confirm treatment history.
Measures
Demographic, Morphologic, and Treatment Protocol Predictors
Family Medical History Interview and Chart Review Form. A combination of parent/legal guardian semi-structured interview and medical chart review were used to collect information about the child's cleft and treatments received since birth, including ICD-9 or corresponding ICD-10 diagnostic codes, dates and types of surgeries performed, speech therapy, other developmental therapies and educational interventions. Researchers have identified as many as 190 different protocols in use for the treatment of CL/P. 12 For the purposes of this study, it was necessary to consolidate treatment approaches into broader protocols that reflect major differences in treatment approaches. Treatment elements of interest included: 1) Age at first lip repair; 2) Age at first palate repair and type of palate closure; 3) Velopharyngeal incompetency (operationalized by documented receipt of secondary palate repair); 4) Cleft morphology (unilateral vs. bilateral and incomplete vs. complete); and 5) Total number of cleft-related surgeries including primary cleft lip and palate along with all revisions, alveolar bone grafting and revisions, nasal surgery and revisions, and pressure equalization (PE) tubes. Many children had not yet reached the stage of dental maturity that allowed for secondary bone grafting to be performed. Therefore, we did not examine the impact of bone grafting as a separate treatment but did include it in the total cleft-related surgery count, if performed. When two procedures were performed within the same operating room visit (eg, PE tubes with palate closure), it was counted as one cleft-related surgery. Caregivers were also asked to provide demographic information (eg, race, ethnicity, type of insurance, marital status). Information provided from parents was verified via medical chart review. Questions about parental education level and occupation were embedded within the interview so that Hollingshead Four Factor Index 13 scores could be calculated as a measure of socioeconomic status (SES). Two scores are generated by the Hollingshead Four Factor Index: a continuous score, which ranges from 8–66 (higher continuous scores indicated higher SES) and a categorical score, which ranges from 1 (high SES) to 5 (low SES). Average SES scores (Category 3) range from 30–39.
Health-Related Quality of Life Outcomes
Pediatric Quality of LifeTM (PedsQL). 14 The PedsQL is a widely used, 23-item, reliable and valid measure of health-related quality of life with parallel parent proxy and child versions. The Total score, Physical, and Psychosocial (composite of Emotional, Social, and School Functioning) were used in this study.
Pediatric Quality of LifeTM Family Impact Module (PedsQL FIM). 15 This reliable and valid parent-report measure consists of 36 Likert-scale items that assess how pediatric chronic health conditions impact parental health-related quality of life and family functioning. The Total score (average of 36 items), Parent health-related QoL (Parent HRQoL) Summary Score (the average of the physical, emotional, social, and cognitive scales), and Family Functioning Summary Score (the average of the daily activities and family relationship scales) were used in this study.
PedsQL and PedsQL FIM items are rated using a 5-point scale ranging from 0- never to 4 – almost always. Scores are then transformed and averaged across domains with total score ranges from 0 to 100 and higher scores reflecting better quality of life and lower treatment burden.
Appearance and Speech Function
CLEFT-Q.16,17 The CLEFT-Q is a self-report measure developed for persons with CL/P ages 8 to 29 years. The CLEFT-Q Face (9 items), Lip (9 items), Lip Scar (7 items), Nose (12 items), Nostril (6 items), Speech Distress (10 items) and Speech Function (12 items) scales were used in this study. Each appearance-related item measures how much satisfaction individuals report for a particular feature (eg, how their lip scar looks); items are rated using a scale ranging from ‘not at all’ to ‘very much.’ Speech-related scales are rated about how often (‘never,’ ‘sometimes,’ ‘always’) individuals have speech-related difficulties or negative feelings about their speech. CLEFT-Q scores for each participant were calculated by converting raw scores to scores on a 0 to 100 scale, where higher values indicate better functioning. The CLEFT-Q has acceptable reliability and validity with good ability to discriminate by cleft type. 18
Psychosocial Adjustment Outcomes
Patient Reported Outcomes Measurement Information System (PROMIS). 19 Three pediatric self-report measures from the National Institutes of Health Patient Reported Outcomes Measurements Information System (https://www.healthmeasures.net/) were used to assess self-reported anxiety, depression, and experiences of stigma. Measures include Pediatric Anxiety–Short Form v.1.1, Pediatric Depression Symptoms–Short Form v1.1 and Pediatric Stigma–Short Form 1.0. Each measure includes 8–10 items on a five-point Likert scale ranging from never to almost always. Norms are available as T-scores with a mean of 50 and standard deviation of 10. Higher scores indicate more symptoms reported. Adequate reliability was reported with good precision for the short form measures.19–21
Child Behavior Checklist (CBCL). 22 The CBCL is a reliable and valid, 113-item parent-report measure rating children's externalizing behavior problems (eg, noncompliant, disruptive), internalizing problems (eg, shy, withdrawn, anxious or despondent), and total problems. 22 Items are rated using a scale ranging from ‘not true’ (score of 0); ‘somewhat or sometimes true’ (score of 1); or ‘very true or often true’ (score of 2). Higher scores indicate higher frequencies of observed problems. Scores are converted to T-scores with a mean of 50. The CBCL DSM-related subscales of Anxiety, Affective, and Attention Deficit-Hyperactivity (ADHD) were included to enable comparison of parent-reported symptoms relative to child ratings of anxiety and depressive symptoms and to assess ADHD symptoms. For correlations and linear regressions, raw scores were used for these three DSM-related subscales as recommended by the measure authors given that subscale scores are truncated at T = 50. 22
The CBCL School (eg, academic performance, problems at school), Activities (eg, engagement in hobbies, extracurricular activities), and Social (eg, how many friends a child has, how often they socialize with peers) subscales were also calculated, along with the Total Competence scale. Higher scores reflect better functioning.
Statistical Methods
All predictor variables (demographic, morphologic, and treatment variables) included in the individual models were chosen a priori. Due to small n's, race/ethnicity was collapsed such that children identified as White formed one group and children identified as Hispanic, Black or African American, Native American, or Multiple races formed a second group. Pearson correlations were calculated to ensure that no predictor variables correlated at greater than .80 to minimize risk of multicollinearity. Analyses were conducted using SPSS 28.0.1. 23
Descriptive Statistics
Descriptive statistics (frequencies, percentages, means, standard deviations, correlations) were calculated, and continuous variables were examined for normality and equality of group variances. Differences for predictor variables by cleft type [cleft lip with or without cleft alveolus (CL ± A), cleft palate only (CP), and cleft lip and palate (CLP)] were determined by Chi Square (X2) or linear regression. Differences on outcome measures by cleft type and differences in child perceptions of appearance and speech outcomes (CLEFT-Q scores) by site (to determine if children's perceptions of outcomes varied by treatment team) were analyzed via linear regression. Robust standard errors based on 1000 bootstrap samples were used to determine P values and confidence intervals (CI; 95% CI reported in brackets [ ] below) for linear regression analyses. Effect sizes are reported as partial eta squared (ηp2) (ηp2 = .01 corresponds to a small effect size, ηp 2 = .06 to a medium effect size, and ηp 2 = .14 to a large effect size). 24
Preliminary Analyses: Pearson Correlations Between Predictor Variables and Outcomes
Separate Pearson correlations were calculated between predictor variables and outcomes by cleft type [cleft lip with or without cleft alveolus (CL ± A), cleft palate only (CP), cleft lip and palate (CLP)]. A minimum of five subjects in a group was required to be included in the correlation analyses. 25 Correlations with P values ≤ .10 were retained for inclusion in multiple regression analyses.
Supplemental Table 1 provides the plan for the preliminary Pearson correlations. Outcome variables were the same for all cleft types with the exception that CLEFT-Q Face, Lips, Lip Scar, Nose, and Nostril were only analyzed for children with visible clefts (CL ± A and CLP) while CLEFT-Q Speech Distress and Speech Function were only evaluated for children with who had a cleft palate (CP and CLP). Demographic predictor variables were the same for all cleft types and included child age, child sex, child race (White, not White), and SES (Hollingshead continuous score; higher scores indicate higher SES). Treatment and morphological variables differed by cleft type such that correlations for CL ± A did not include the three variables specific to palate surgery (Age at Palate Surgery; Furlow Palatoplasty, yes/no; and Secondary Palate Surgery, yes/no) while correlations for children with CP did not include variables specific to cleft lip [Cleft Morphology (incomplete/complete and unilateral/bilateral); Presurgical lip taping or NAM, yes/no; Age at lip surgery; Lip Revision, yes/no; Nasal Surgery yes/no]. Analyses for children with CLP included all treatment and morphological variables. Total Cleft-Related Surgeries was included in all analyses, regardless of cleft type.
Associations of Demographic, Morphologic, and Treatment Variables with Outcomes
Multiple regression analyses (MRA) by cleft type were used to determine if demographic, morphologic, or treatment variables that met preliminary correlation criteria for inclusion predicted variability in parent- and child-rated psychosocial adjustment and outcome measures. MRA were conducted if there was more than one predictor variable that met criterion for inclusion (P values ≤ .10). Durbin-Watson statistic was determined for each MRA with values between 1.5 and 2.5 indicating lack of autocorrelation. Predictor variables were considered meaningful if P values ≤ .10 due to the exploratory nature of this study.
Results
Demographics and Clinical Characteristics
Table 1 presents demographic and clinical characteristics for the sample by cleft type. Enrollment data for the study have been previously published. 26 A total of 284 participants were enrolled (58.8% CLP). Both caregiver and child participated for 96% (n = 258) of enrolled participants; only caregivers participated for 7.7% (n = 22); and only the child participated for 1.4% (n = 4). Across the entire sample, the mean age was 9.35 (SD = 0.87) years at the time of participation with no significant differences observed by cleft type. Over half were male (53.5%); however, there was a significant sex by diagnosis interaction, X2(2) = 19.33, P < .001: 60% of children with CP were female while 61% of children with both CL ± A and CLP were male. The sample primarily identified as White (76.1%), with 14.1% identifying as Hispanic; race/ethnicity did not differ by cleft type. Among parents/guardians, 82% were mothers, the majority (77.4%) were married or partnered, and half reported at least some college or vocational school, college, and/or graduate degrees. Mean SES was slightly above average (M = 40.13; SD = 12.49), and families of children with CP were of significantly higher SES than families of children in other diagnostic groups, F(2, 273) = 4.98, P = .008, ηp2 = .035, Mean Difference (MD) for SES between CP and CL ± A was 4.82, [-0.12, 9.45], P = .048 and MD between CP and CLP was 5.57, [2.04, 8.48], P=<.001.
On average, children with CL ± A or CLP were 4.37 months of age at time of lip repair (range 1.38 to 13.0 months) with no differences by cleft type. Lip was incomplete for 60 (29.3%) and unilateral for 144 (70.2%) of the children. Fifty-three (24.9%) of the children with a cleft lip received presurgical taping and/or NAM. Of those, 46 (88.5%) had a complete cleft lip, and 20 (38.5%) were bilateral.
Children with CP were significantly older at time of palate closure than children with CLP, MD = 10.29 months, [6.21,14.38]; F(1, 229)= 4.67, P < .001, ηp2 = .10. Thirty-seven (52.1%) children with CP and 51 (31.5%) with CLP had received a Furlow palatoplasty. Type of palate surgery was unknown for 46 participants. Twenty-five children (35.2%) with CP and 56 (33.5%) children with CLP required secondary palate surgery. Secondary palate surgery was required less frequently for children who had a documented Furlow palatoplasty (21.6%) than children who did not (40.4%) or had an unknown (47.8%) type of palate surgery, X2(2) = 11.58, P = .003. For regression analyses, unknown palate repair and non-Furlow repairs were combined.
Across diagnostic groups, children underwent an average of 3.73 (SD = 2.14) cleft-related surgical procedures (range 1–12). Number of surgeries differed significantly by cleft type, F(2281) = 50.28, P < .001, ηp2 = .26. Children with CLP had more procedures than children with both CL ± A (MD = 2.70, [1.96, 3.45], P < .001) and CP (MD = 1.79, [1.67, 2.42], P < .001). Additionally, children with CP had significantly more procedures than children with CL ± A (MD = 0.90, [0.38, 1.28], P < .001).
Pearson correlations among predictor variables are provided in Supplemental Table 2. Correlations ranged from −.26 to .45 with no correlation greater than .80; therefore, all predictor variables were retained for preliminary Pearson correlation analyses. Of note, there were no significant correlations between SES, Child Race, or Insurance Status and Age at Lip Closure, use of Presurgical Taping/NAM, Lip Revision, Nasal Surgery, Age at Palate Closure, Furlow (yes, no, unknown), Secondary Palate Closure, or Total Cleft-Related Surgeries (R's ranged from -.03 to .10, P's ranged from .170 to .978).
Child and Parent Outcome Measures by Cleft Type
Health-Related Quality of Life and Psychosocial Adjustment. Overall, scores were within the average range for each of the outcome variables. 27 There were no significant differences by cleft type for Child-rated health-reported Quality of Life (QoL); however, Parent proxy-reported QoL was higher (fewer concerns) for children with CL ± A on PedsQL Psychosocial, F(2272) = 3.28, P = .039, ηp2 = .024 than children with CPO, MD = 6.70 [1.81, 11.51], P = .011; and children with CLP, MD = 4.44 [0.56, 8.26], P = .027 (Table 2). Scores also differed significantly on PedsQL Family Impact Module (FIM Total), F(2275) = 3.04, P = .049, ηp2 = .022. This appeared to be driven by a significant difference on the PedsQL FIM Family Functioning scale, F(2275) = 3.71, P = .026, ηp2 = .026. Parents of children with CL ± A reported higher scores (fewer concerns) than parents of children with CP (FIM Total: MD = 4.83 [0.78, 8.90], P = .026; FIM Family: MD = 4.41 [0.08, 8.78], P = .048) and CLP (FIM Total: MD = 5.53 [2.81, 8.71], P = .002; and FIM Family: MD = 6.70 [3.23, 10.19], P = .001). In each analysis, scores for children with CP did not differ significantly from scores for children with CLP.
Outcome Means and Group Differences by Cleft Type.
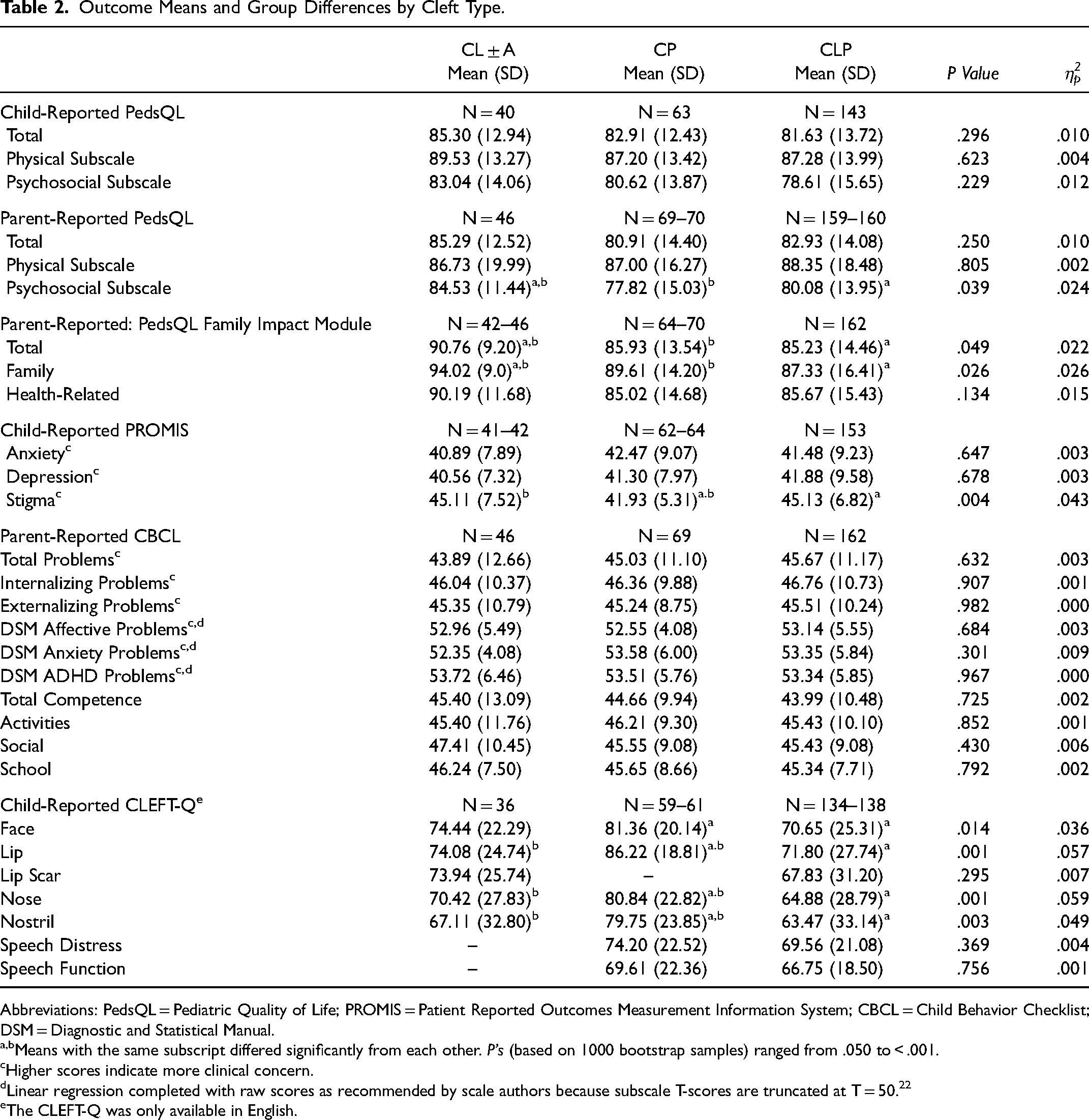
Abbreviations: PedsQL = Pediatric Quality of Life; PROMIS = Patient Reported Outcomes Measurement Information System; CBCL = Child Behavior Checklist; DSM = Diagnostic and Statistical Manual.
Means with the same subscript differed significantly from each other. P's (based on 1000 bootstrap samples) ranged from .050 to < .001.
Higher scores indicate more clinical concern.
Linear regression completed with raw scores as recommended by scale authors because subscale T-scores are truncated at T = 50. 22
The CLEFT-Q was only available in English.
Mean T-scores ranged from 40 to 42 for the PROMIS Anxiety and Depression, and from 41 to 45 for the PROMIS Stigma scale, indicative of fewer concerns relative to normative samples on these scales. There were no differences in scores by cleft type for child-reported PROMIS Anxiety or Depression; however, children with CP reported significantly lower scores (fewer concerns) on the PROMIS Stigma scale, F(2255) = 5.66, p = .004, ηp2 = .043, than children with CL ± A, MD = −3.18, [-5.83, −0.46] P = .022, and CLP, MD = −3.21, [−4.91, −1.31] P = .001. Parent-reported CBCL Problem and Competence scores did not differ by cleft type.
Speech and Appearance Outcomes
Children with CL ± A and CLP completed the CLEFT-Q Lip Scar and children with CP and CLP completed the CLEFT-Q Speech Distress or Speech Function with no significant differences observed by cleft type on any of these CLEFT-Q subscales. There were no significant differences in child-reported CLEFT-Q appearance or speech outcome scores based on treatment site (data not shown).
Preliminary Analyses: Pearson Correlations Between Predictor Variables and Outcomes
All correlations for each of the outcome variables with demographic, morphologic, and treatment variables by cleft type and by visible, palatal, and all diagnoses are provided in Supplemental Tables 3–6. There were only four children with CL ± A who underwent presurgical taping/NAM; therefore, Presurgical taping/NAM is not included in the correlation table for CL ± A. Table 3 provides a summary of correlations between predictor and outcome variables by cleft type and by visible, palatal, and all diagnoses that met the criteria of P value ≤ .10.
Correlations Considered for Regression Analyses by Cleft Type.
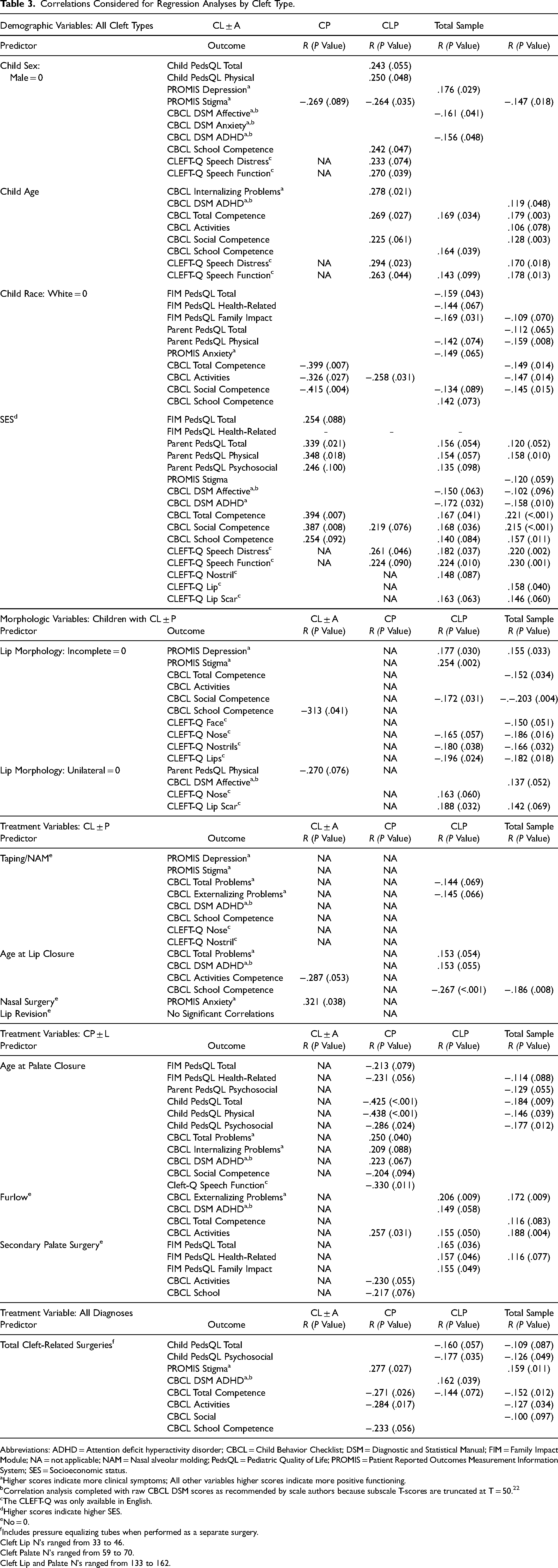
Abbreviations: ADHD = Attention deficit hyperactivity disorder; CBCL = Child Behavior Checklist; DSM = Diagnostic and Statistical Manual; FIM = Family Impact Module; NA = not applicable; NAM = Nasal alveolar molding; PedsQL = Pediatric Quality of Life; PROMIS = Patient Reported Outcomes Measurement Information System; SES = Socioeconomic status.
Higher scores indicate more clinical symptoms; All other variables higher scores indicate more positive functioning.
Correlation analysis completed with raw CBCL DSM scores as recommended by scale authors because subscale T-scores are truncated at T = 50. 22
The CLEFT-Q was only available in English.
Higher scores indicate higher SES.
No = 0.
Includes pressure equalizing tubes when performed as a separate surgery.
Cleft Lip N's ranged from 33 to 46.
Cleft Palate N's ranged from 59 to 70.
Cleft Lip and Palate N's ranged from 133 to 162.
Associations of Demographic, Morphologic, and Treatment Variables with Outcomes
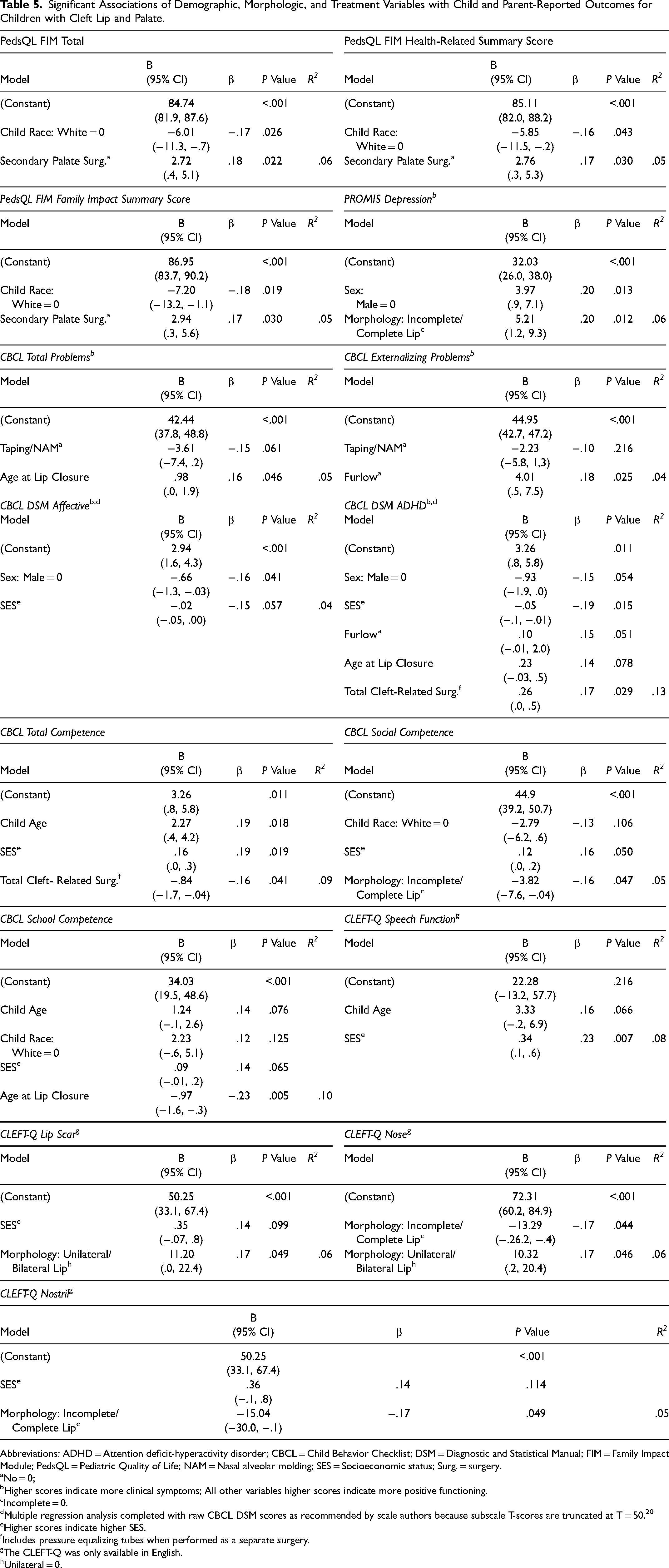
MRA were conducted for outcomes that had more than one predictor variable that met criterion for inclusion. Complete results of the MRA including B with 95% Confidence Intervals and exact P values for all variables entered into the MRA are found in Table 4 for children with CL ± A and CPO, and Table 5 for children with CLP. MRA analyses that did not result in any significant associations are not included in the tables.
Significant Associations of Demographic, Morphologic, and Treatment Variables with Child- and Parent-Reported Outcomes for Children with Cleft Lip ± Alveolus a and Children with Cleft Palate.b
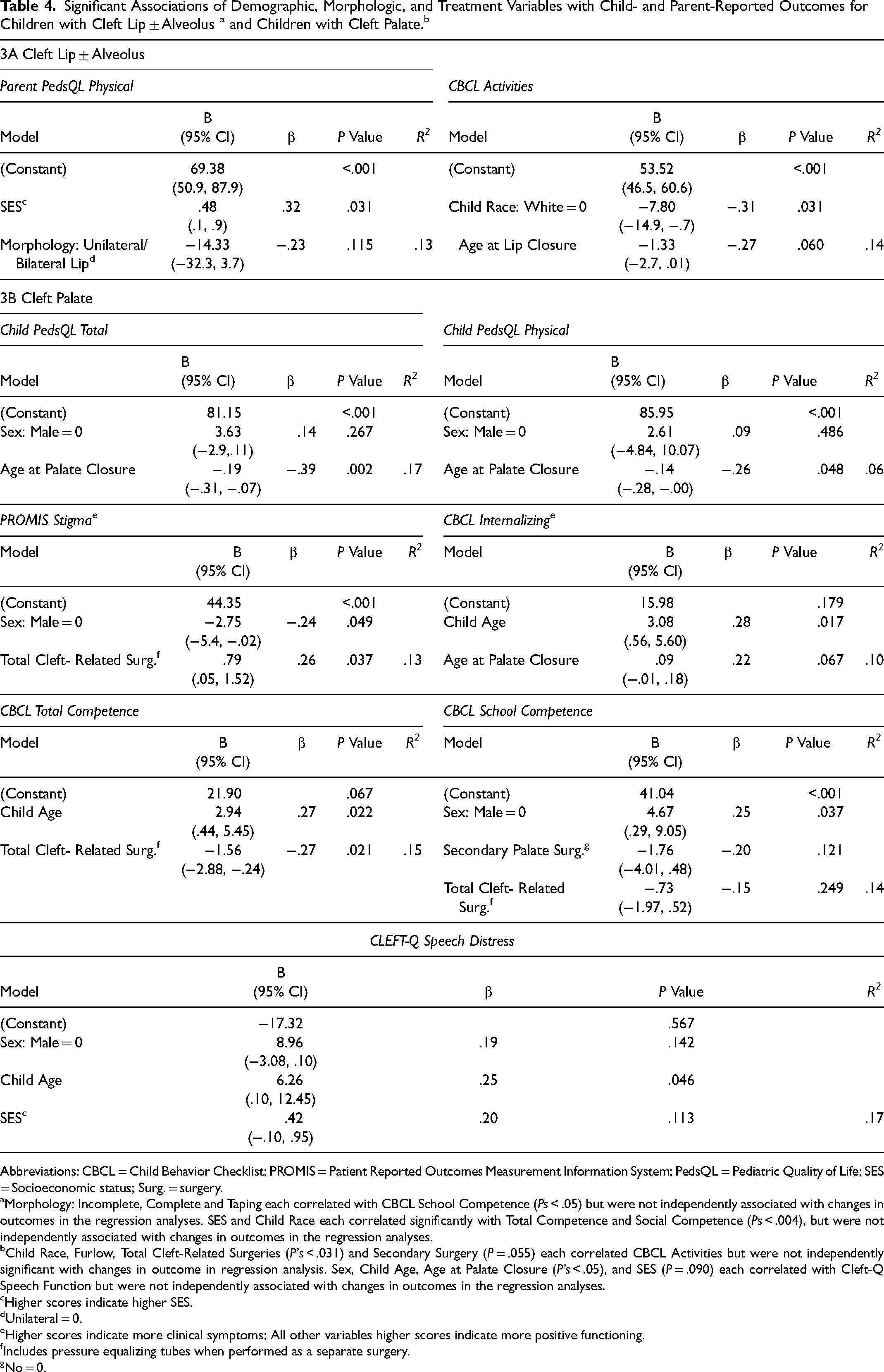
Abbreviations: CBCL = Child Behavior Checklist; PROMIS = Patient Reported Outcomes Measurement Information System; PedsQL = Pediatric Quality of Life; SES = Socioeconomic status; Surg. = surgery.
Morphology: Incomplete, Complete and Taping each correlated with CBCL School Competence (Ps < .05) but were not independently associated with changes in outcomes in the regression analyses. SES and Child Race each correlated significantly with Total Competence and Social Competence (Ps < .004), but were not independently associated with changes in outcomes in the regression analyses.
Child Race, Furlow, Total Cleft-Related Surgeries (P's < .031) and Secondary Surgery (P = .055) each correlated CBCL Activities but were not independently significant with changes in outcome in regression analysis. Sex, Child Age, Age at Palate Closure (P's < .05), and SES (P = .090) each correlated with Cleft-Q Speech Function but were not independently associated with changes in outcomes in the regression analyses.
Higher scores indicate higher SES.
Unilateral = 0.
Higher scores indicate more clinical symptoms; All other variables higher scores indicate more positive functioning.
Includes pressure equalizing tubes when performed as a separate surgery.
No = 0.
Significant Associations of Demographic, Morphologic, and Treatment Variables with Child and Parent-Reported Outcomes for Children with Cleft Lip and Palate.
Abbreviations: ADHD = Attention deficit-hyperactivity disorder; CBCL = Child Behavior Checklist; DSM = Diagnostic and Statistical Manual; FIM = Family Impact Module; PedsQL = Pediatric Quality of Life; NAM = Nasal alveolar molding; SES = Socioeconomic status; Surg. = surgery.
No = 0;
Higher scores indicate more clinical symptoms; All other variables higher scores indicate more positive functioning.
Incomplete = 0.
Multiple regression analysis completed with raw CBCL DSM scores as recommended by scale authors because subscale T-scores are truncated at T = 50. 20
Higher scores indicate higher SES.
Includes pressure equalizing tubes when performed as a separate surgery.
The CLEFT-Q was only available in English.
Unilateral = 0.
Cleft Lip with or without Alveolus. Predictor variables that met criteria for inclusion in MRA analysis for CL ± A included SES, Child Race, Lip Morphology: Unilateral-Bilateral, Pre-surgical Taping or NAM, Age at Lip Surgery, and Nasal Surgery (Table 3 and Supplemental Table 3).
Higher values for SES were significantly associated with higher scores (fewer concerns) on the Parent proxy PedsQL Physical (β = .32). Child Race (White) was significantly associated with higher scores (fewer concerns) on CBCL Activities (β = −.31). MRA did not yield any significant results for PROMIS Stigma, CBCL Total Competence, CBCL Social Competence, or CBCL School Competence (Table 4).
Cleft Palate Only. Predictor variables that met criteria for inclusion in MRA analysis for CP included Sex, Child Age at assessment, Child Race, SES, Age at Palate Closure, Furlow, Secondary Palate Surgery, and Total Cleft-Related Surgeries (Table 3 and Supplemental Table 4).
Younger Age at Palate Closure was significantly associated with higher scores (fewer concerns) on the Child PedsQL Total and Physical scales (β = −.39 and β = −.26, respectively). More Total Cleft-Related Surgeries and Male Child Sex were significantly associated with higher scores (more concerns) on PROMIS Stigma (β = .26. and β = −.24, respectively). Older Child Age at assessment was significantly associated with more CBCL Internalizing problems (β = .28). Older Child Age at Assessment and fewer Total Cleft-Related Surgeries were both associated with higher CBCL Total Competence (β = .27 and β = −.27, respectively). Child Sex (Female) contributed significantly to higher CBCL School Competence (β = .25). Finally, Child Age was the only variable that remained significant as a predictor of CLEFT-Q Speech Distress (β = .25) with older Child Age at assessment related to less distress.
Cleft Lip and Palate. Predictor variables that met criteria for inclusion in MRA analysis for CLP included Child Age at assessment, Child Race, SES, Secondary Palate Surgery, Lip Morphology: Incomplete-Complete and Unilateral-Bilateral, Presurgical Lip Taping or NAM, Age at Lip Closure, Furlow, and Total Cleft-Related Surgeries.
Child Race (White) and Secondary Palate Surgery (Yes) were both significantly associated with higher scores (fewer concerns) on the PedsQL FIM Total (β = −.17 and β = .18, respectively); PedsQL FIM Health Related (β = −.16 andβ = .17, respectively); and PedsQL FIM Family Impact (β = −.18 and β = .17, respectively) scales. Child Sex (Female) and Morphology: Incomplete/Complete (Complete) were associated with higher concerns on PROMIS Depression (β = .20 and β = .20, respectively).
Older Age at Lip Closure was associated with more CBCL Total Problems (β = .16). Furlow Palatoplasty was associated with more CBCL Externalizing Problems (β = .18). Child Sex (Male) was associated with more CBCL Affective Problems (β = −.16). Lower SES and more Total Cleft-Related Surgeries were associated with higher scores (more concerns) on the CBCL DSM ADHD scale (β = −.19 and β = .17, respectively).
Older Child Age at Assessment, higher SES, and fewer Total Cleft-Related Surgeries were associated with higher CBCL Total Competence (β = .18, β = .19, and β = −.16, respectively). Higher SES and Morphology: Incomplete were associated with higher CBCL Social Competence (β = .16, β = −.16, respectively). Younger Age at Lip Closure was associated with CBCL School Competence (β = −.23).
Higher SES was associated with higher ratings on CLEFT-Q Speech Function. Morphology: Incomplete and Bilateral were both associated with better child ratings on CLEFT-Q Nose (β= -.17 and β= .17, respectively). Morphology: Incomplete was associated with higher ratings on CLEFT-Q Nostril (β = −.17), and Morphology: Bilateral was associated with higher ratings on CLEFT-Q Lip Scar (β = .17).
Discussion
This study addresses a major gap in the literature by examining the relationships of demographic, morphologic, and treatment variables from infancy and early childhood to psychological outcomes at school age, including child- and parent proxy-reported QoL, child ratings of appearance and speech function, and psychological adjustment in large sample of children, ages 8–10, who had a diagnosis of CL/P and were born and treated in North America. Children were recruited from six sites representing both large medical centers and small, rural, cleft clinics.
Child- and Parent-Rated Outcomes by Cleft Type
On the PedsQL, child- and parent proxy-reported Total scores ranged from 80 to 85. This is consistent with responses from a healthy normative sample 14 and with those reported in the cleft literature.28,29 Child-reported PedsQL scores in our sample did not differ significantly by cleft type, but there was a significant difference for parent-reported scores. Children with CP received lower parent proxy-reported psychosocial QoL scores relative to children with CL ± A and CLP, though the difference was only statistically significant for the CL ± A group. Other studies have also observed lower QoL scores in children with CP.29–31 CP is associated with greater risks for cognitive problems and these problems could also impact psychosocial functioning.32–34 Collectively, these findings highlight the need for psychosocial support for children with cleft palate (with or without cleft lip) and the potentially detrimental effects of speech differences on psychosocial functioning. 29
To date, few studies have utilized the PedsQL Family Impact Module in a cleft population. Compared to a community sample, 35 scores from our sample were higher, suggesting that parents of children with CL/P in this specific age range are reporting little impact of the condition on parental health-related quality of life or family functioning. Our PedsQL FIM Total scores were comparable to those reported in other studies for children ages 8–12 years 29 with similar differences observed by cleft type, notably that the highest ratings (indicative of better functioning/low impact on family and parent functioning) were observed for children with CL ± A. Data from the United Kingdom Cleft Collective Birth Cohort Study reported that total PedsQL FIM scores were approximately 10 points lower prior to infant's primary cleft surgery indicating greater impact on caregiver and family functioning during the initial months of the child's life. 5 This suggests that the impact of the cleft condition on the parents’ well-being and family functioning may change and potentially lessen with time. Future longitudinal studies are needed to better understand changes in family impact over time.
CLEFT-Q differences observed by cleft type were consistent with findings from field test data. 18 Children with CP reported more satisfaction with appearance while scores for children with CL ± A did not differ significantly from those with CLP. Similarly, CLEFT-Q Speech Distress and Speech Functioning scale scores were comparable for children with CLP and CPO. Children with CLP and CL ± A reported more concerns with stigma than children with CP, but did not differ from each other. Overall, children with visible clefts had more negative perceptions of their appearance and reported greater feelings of stigma. Other measures of child- and/or parent-reported anxiety, depression, behavior problems, and competence scores (PROMIS and CBCL) did not differ significantly by cleft type. Child-report on the PROMIS scales yielded mean scores within the lower average range compared to clinical data, 36 reflecting fewer issues. Parent-report on the CBCL also yielded mean scores within the average range compared to normative data 22 and similar to other reports of children with CL/P. 37
Associations of Demographic, Morphologic, and Treatment Variables with Outcomes
Figure 1 provides a visual summary of the associations between demographic, morphologic, and treatment variables with QoL, psychosocial adjustment, and appearance and/or speech function for children with CL ± A, CP, and CLP.
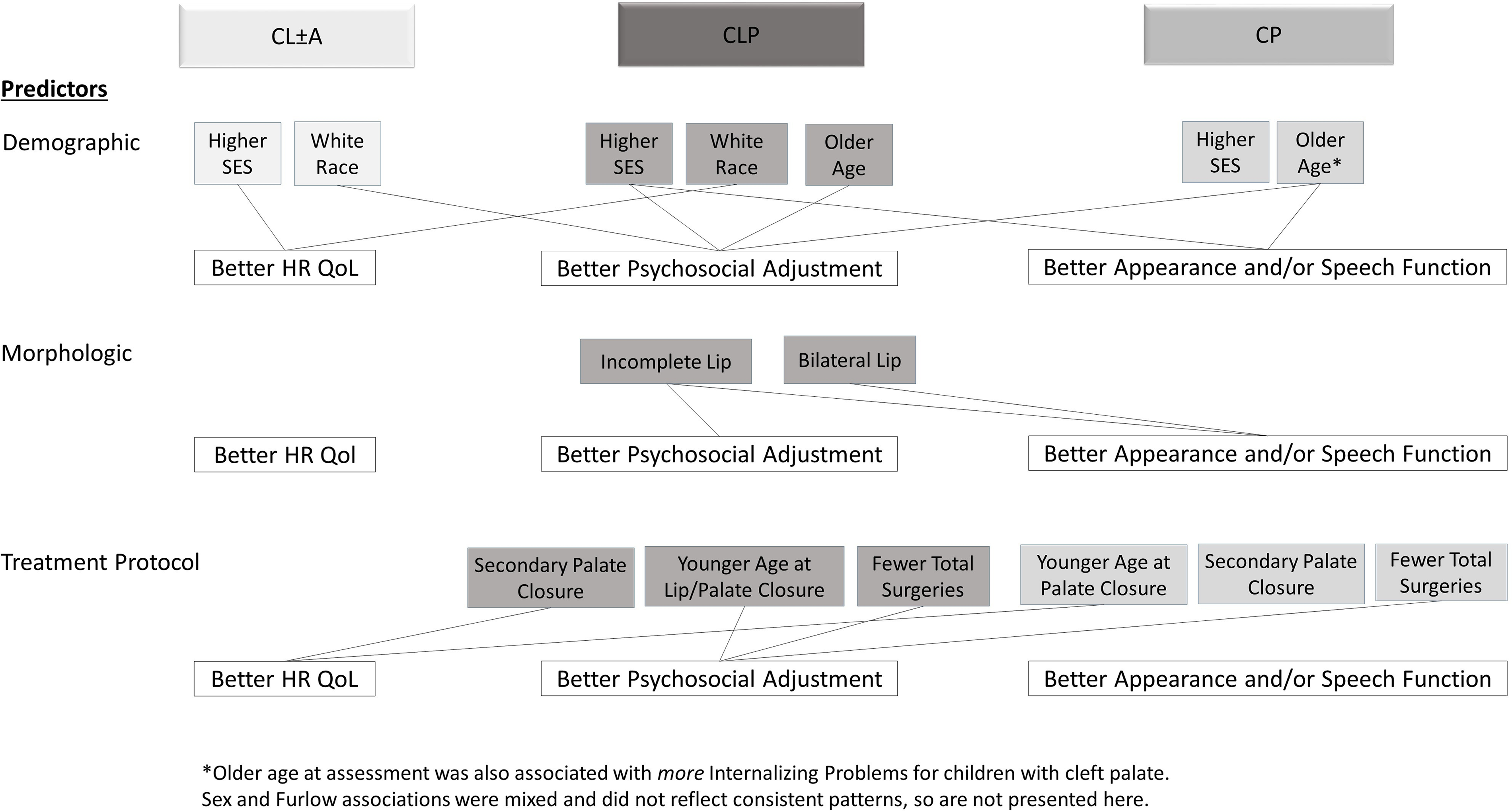
Associations of Demographic, Morphologic, and Treatment Variables with Outcomes.
Demographic Characteristics. Family SES, Insurance Status, and Child Race were not significantly correlated with any of the treatment variables (ie, Age at Lip Surgery, Presurgical Taping/NAM, Nasal surgery, Age at Palate Surgery, Furlow palatoplasty, secondary lip or palate surgeries, or Total Cleft-Related Surgeries) for this sample, but they were salient in relationships to child- and parent-rated outcomes (particularly when looking at correlations at the total sample). Children residing in higher SES homes reported less stigma and reported feeling better about appearance and speech functioning. Parents of children from higher SES homes reported better overall QoL for children, particularly when clefts were visible. The potential negative impact of the cleft on family QoL was lower for children identified as White. Higher SES and/or White race were also associated with parent perceptions of child competence, including greater participation in activities, more interactions with friends, and better school achievement. There was a low but significant correlation between SES and Race such that children identified as White tended to reside in higher SES homes.
A similar association between family factors (eg, race and lower income and education) and behavioral and emotional problems was observed for children with CL/P in the Cleft Collective Study. 35 Family SES and race have a strong influence on adjustment outcomes including satisfaction with appearance and speech as well as perceptions of stigma and child competence. It is important to note that in the present study these findings are not better explained by possible center differences, as there were no significant differences in these outcome variables across centers. Together, these findings suggest that children with CL/P who identified as non-White and children from lower SES homes require more vigilance by cleft teams because they may be at higher relative risk for psychosocial concerns.
Impact of Cleft Lip Morphology and Treatment on Outcomes for Children with Cleft Lip with or without Cleft Palate (CL ± P). In the present study, cleft lip morphology was associated with outcomes reported by both children and parents. Diagnosis of complete cleft lip was correlated with more child-reported depressive symptoms, greater stigma, poorer feelings about lip and nose appearance, and poorer parent-reported social competence, particularly for children with CLP. Bilateral cleft lip was associated with better child-reported appearance of lip scar and nose.
Most treatment variables including taping/NAM and lip or nose revisions were not associated with parent- or child-reported psychosocial outcome variables for children with CL ± P. Rather, factors outside of the child's control, including demographic characteristics and severity of the cleft, showed the highest associations with psychosocial outcomes. The one exception to this was age at lip surgery. For children with CL ± P in our study, earlier age at lip surgery was associated with higher school competence. In our study, the mean age at lip closure was 4.37 months with a range of 1.38 to 13.00 months. We did not have information about why lip surgery may have been completed at older vs. younger ages. Age at lip surgery was not significantly correlated with use of pre-surgical taping or NAM, but more than 50% of the infants underwent lip surgery at four months of age or later. Grollemund et al. 38 reported that neither timing of surgery, when performed under 4 months of age, nor severity of the cleft was associated with infant withdrawal; however, maternal stress was related to infant withdrawal. The current study design did not permit measuring parental stress during infancy; however, there is considerable evidence linking parental stress to negative outcomes for families whose children are born with CL/P. 5
Neither lip revision nor nasal surgery were associated with higher child-reported lip or nose appearance scores on the CLEFT-Q. Similarly, these procedures were not associated with child-reported QoL, depression, or feelings of stigma; nor parent perception of family QoL, child QoL, or child competence. The only significant correlation was between nasal surgery and an increase in self-reported anxiety for children with CL ± A who underwent nasal surgery.
Impact of Treatment on Outcomes for Children with Cleft Palate with or without Cleft Lip (CP ± L). Particularly for children with CP, age at palate repair was a salient variable. Children with CP who underwent palate repair at a younger age reported higher QoL scores and better speech function, although this relationship decreased in strength after age, sex, and SES were accounted for in analyses. Parents also associated younger age at palate closure with better Family QoL, fewer behavior problems, and better social competence, suggesting that earlier palate repair is associated with better outcomes. Nonetheless, for children with CP in our sample, the standard deviation for mean age at palate repair was wide, and children were older at time of repair relative to children with CLP, highlighting the need for further examination of the relationship between age at palate repair and outcomes in future studies.
There is some limited evidence from our data that type of palate repair impacts psychosocial outcomes. Children with CP and CLP who received a Furlow palatoplasty as their primary surgery participated in more activities outside the home; however, children with CLP who received a Furlow palatoplasty were also rated by their parents as having more externalizing problems. In general, children who received a Furlow palatoplasty were less likely to require a secondary surgery which could reduce total number of surgeries and relatedly, stress and burdens on children and their families. Secondary palate surgery was associated with better family QoL, even though it was not significantly correlated with child perceptions of improved speech functioning or less speech distress.
Total Cleft-Related Surgeries and Outcomes for All Participants. Psychological outcomes were better in many areas when children had fewer total cleft-related surgeries. Child-reported QoL was higher when children had fewer surgeries. Across the total sample, children reported less stigma with fewer surgeries. When children were reported to have fewer surgeries, there were also fewer parent-reported behavior problems, particularly ADHD problems, better school performance, more participation in outside activities, and better overall competence. These findings are consistent with other studies which found that greater numbers of medical interventions performed during childhood is associated with poorer outcomes.9,39 In our sample, we did not account for factors such as surgical complications which may contribute to greater number of surgeries and relatedly, poorer psychosocial outcomes.
Limitations
This study has several limitations including retrospective assessment of treatment history, which may have introduced inaccuracies due to problems with parent recall and incomplete medical records. Given the vast number of CL/P treatment protocols, we evaluated major differences in treatment approaches (eg, type of palate repair) and were not able to evaluate subtler protocol differences (eg, surgeon-specific modifications of surgical techniques) or other treatment-related variables such as the timing and type of speech therapy, psychological, or hearing-related services, which may have affected outcomes. 38
While we approached consecutive families at all six sites, differences between participating and non-participating families could also potentially influence our findings. Additionally, we excluded children who had other comorbid medical conditions or cognitive disabilities, thus our findings are not generalizable to these patients, although parents of children with isolated CL/P with cognitive disabilities were eligible to participate. Further, our findings do not reflect outcomes for children who are not receiving interdisciplinary cleft care, a population who may be experiencing disparities due to care costs or limited access to care.40,41 Due to measure and funding limitations, we were not able to include families who spoke languages other than English or Spanish. Another limitation pertains to the age of our child participants, as they are likely to require additional cleft-related surgery and other related interventions as they mature. Thus, it is unknown whether the observed relationships between psychosocial outcomes and early cleft treatment variables will remain stable or change over time and in response to additional procedures. Small numbers of participants necessitated dichotomizing several variables (eg, race) which may obscure important relationships between these variables and our outcome measures.
Future prospective, longitudinal studies are needed to address these limitations and to better understand psychosocial outcome trajectories from infancy through adulthood. Studies are also needed to better understand the role of contextual factors (eg, coping style, resiliency) and psychosocial and treatment outcomes.
Conclusions
Demographic characteristics, cleft severity, and treatment variables, particularly total number of cleft-related surgeries, age at lip and palate repair, and type of palate repair, are related to later psychological functioning from parent and child perspectives. These findings represent a critical step towards advancing our understanding of how demographics and cleft treatments impact children's psychosocial functioning and will aid in the identification of empirically-supported approaches to achieve the best outcomes for all children affected by CL/P.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231181581 - Supplemental material for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables
Supplemental material, sj-docx-1-cpc-10.1177_10556656231181581 for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables by Canice E. Crerand, Amy L. Conrad, Claudia Crilly Bellucci, Meredith Albert, Celia E. Heppner, Farah Sheikh, Suzanne Woodard, Shivika Udaipuria and Kathleen A. Kapp-Simon in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656231181581 - Supplemental material for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables
Supplemental material, sj-docx-2-cpc-10.1177_10556656231181581 for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables by Canice E. Crerand, Amy L. Conrad, Claudia Crilly Bellucci, Meredith Albert, Celia E. Heppner, Farah Sheikh, Suzanne Woodard, Shivika Udaipuria and Kathleen A. Kapp-Simon in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656231181581 - Supplemental material for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables
Supplemental material, sj-docx-3-cpc-10.1177_10556656231181581 for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables by Canice E. Crerand, Amy L. Conrad, Claudia Crilly Bellucci, Meredith Albert, Celia E. Heppner, Farah Sheikh, Suzanne Woodard, Shivika Udaipuria and Kathleen A. Kapp-Simon in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-4-cpc-10.1177_10556656231181581 - Supplemental material for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables
Supplemental material, sj-docx-4-cpc-10.1177_10556656231181581 for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables by Canice E. Crerand, Amy L. Conrad, Claudia Crilly Bellucci, Meredith Albert, Celia E. Heppner, Farah Sheikh, Suzanne Woodard, Shivika Udaipuria and Kathleen A. Kapp-Simon in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-5-cpc-10.1177_10556656231181581 - Supplemental material for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables
Supplemental material, sj-docx-5-cpc-10.1177_10556656231181581 for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables by Canice E. Crerand, Amy L. Conrad, Claudia Crilly Bellucci, Meredith Albert, Celia E. Heppner, Farah Sheikh, Suzanne Woodard, Shivika Udaipuria and Kathleen A. Kapp-Simon in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-6-cpc-10.1177_10556656231181581 - Supplemental material for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables
Supplemental material, sj-docx-6-cpc-10.1177_10556656231181581 for Psychosocial Outcomes in Children with Cleft Lip and/or Palate: Associations of Demographic, Cleft Morphologic, and Treatment-Related Variables by Canice E. Crerand, Amy L. Conrad, Claudia Crilly Bellucci, Meredith Albert, Celia E. Heppner, Farah Sheikh, Suzanne Woodard, Shivika Udaipuria and Kathleen A. Kapp-Simon in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
Funding for this project was provided by a grant from the Cleft Palate Foundation (Kapp-Simon, PI). We thank Mariana Arroyo Flores, B.S., Jennifer Litteral, M.A., Hillary M. Kapa, M.P.H., Hailey Umbaugh, B.S., Emily Kuhlmann, B.A., Kristina Butler, M.S., Alessia Portante, B.S., Ashlyn Parides, B.A., Dennis Burchette, B.A., who helped with data collection and/or manuscript preparation. We extend our appreciation to the children and families who took part in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cleft Palate Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.