
Abstract
Objective::
The current study examined stop consonant production in children with cleft lip and/or palate (CP ± L) 2-6 months following palatal surgery.
Design::
Prospective comparative study.
Setting::
Multisite institutional.
Participants::
Participants included 113 children with repaired CP ± L (mean age = 16 months) who were participating in the multicenter CORNET study.
Procedures:
Parents of participants were asked to record approximately two hours of their child's vocalizations/words at home using a Language ENvironmental Analysis (LENATM) recorder. Four ten-minute audio-recorded samples of vocalizations were extracted from the original recording for each participant and analyzed for presence of oral stop consonants. A minimum of 100 vocalizations were required for analysis.
Results::
Preliminary findings indicate that at least one oral stop was evident in the consonant inventory for 95 of the 113 children (84%) at the time of their post-surgery 16-month recording, and 80 of these children (71%) were producing two or more different stops. Approximately 50% of the children (57/113) produced the three voiced stops, and eight of the children (7%) were producing all six stop consonants.
Conclusions::
The findings of this study suggest that the majority of children with repaired CP ± L from English-speaking homes are producing oral stops within six months following palatal surgery. Similar to same-age children without CL ± P, voiced stops were more frequently evident in the children's inventories than voiceless stops. In contrast to findings of previous reports suggesting place of articulation differences, a somewhat comparable percentage of children in this study produced voiced bilabial, alveolar, and velar stops.
Introduction
The influence of an unrepaired palatal cleft on early vocal development has been well documented over the last 20 years. When vocalizations of children with an unrepaired cleft palate are compared to those of their noncleft peers, differences are evident between the groups in type of consonants produced. Whereas stops, nasals, and glides are typically seen in the early phonetic inventories of noncleft children, numerous reports indicate that as a group, children with unrepaired cleft palate produce fewer oral stops than noncleft children1–7 and their vocalizations include more labial sounds than those with an alveolar, palatal, or velar placement.1,6,8,9
The absence of stops in the vocalizations/early speech of children with cleft palate prior to palatal surgery has been associated with an inability to achieve the oral pressure necessary for stop production.1,6,10–13 In their series of investigations, however, Chapman and colleagues reported that while children in the cleft group produced significantly fewer oral stops than their noncleft peers prior to palatal surgery, 1 more than 60% of these children had one or more obstruents in their phonetic inventory. 14 In their 2018 report, Hardin-Jones and Chapman 14 acknowledged that while some toddlers produce oral stops prior to palatal surgery, the relatively low frequency of these consonants could explain the preference that these children show for words beginning with sonorants. “The preference for words beginning with sonorants in their early lexicon was probably related to the practice and refinement of these types of consonants in babble—and not necessarily to the presence or absence of oral stops per se” (p. 7). This is not a new idea as other investigators have also linked the absence of oral stops in the babbling inventory of these children to an early preference for words beginning with sonorants.15–17
Lack of emergence of stop consonants following palatal surgery has long been considered an important indicator of the need for early intervention and/or additional surgical management for velopharyngeal dysfunction (VPD). Recently, Hardin-Jones and Chapman 14 examined the relationship between nasal substitutions in early words (identified in language samples obtained at 13, 17, 21, and 27 months of age) and hypernasality at 39 months of age for 34 children with repaired cleft palate. In their retrospective study, they identified the earliest age at which each child produced at least 10 words and then examined words in that sample for the presence of nasal substitutions. When present, nasal substitutions were tracked in each subsequent language sample to identify the age at which they were no longer present. The authors reported that while 76% (26/34) of the children produced nasal substitutions on one or more early words, only 38% of them (10/26) demonstrated moderate-severe hypernasality and suspected VPD at 39 months of age. In addition, they noted that while nasal substitutions typically replaced stop consonants, they were also substituted for liquids, glides, and fricatives. Of particular interest in this study was the finding that 16 of the 26 (62%) children who produced nasal substitutions also produced oral stops prior to palatal surgery. The authors argued that “nasal substitutions that are evident in the early lexicon of young toddlers without clefts are transient productions that resolve as the child's inventory of practiced consonants expands and their phonology becomes increasingly systematic” (p. 7). This is likely also the case for many children with cleft palate. As noted by Hardin-Jones and Chapman, 14 “these productions may simply reflect the normal variability found in the early linguistic stage of phonological development, as well as the child's use of sounds that have been “practiced” in babble and early words and are thus more easily produced” (p. 1259).
While oral stops may be present in the inventories of some children with cleft palate prior to palatal surgery,1,18 there is a growing body of evidence suggesting that it can take up to 6 months or more for oral stops to emerge following palatal surgery for others.14,19–21 Salas-Provance et al 20 reported that oral stops were evident in three of the four fifteen-month-old children they studied who had undergone palatal repair at 13 months of age, just two months post palatoplasty. Jones et al 19 studied a larger cohort of 14 children with repaired cleft palate and reported that 11 (79%) produced at least one oral stop at approximately 17 months of age (six months post-surgery), with 64% producing two or more stops. Overall, they noted a 50% increase in oral stop production from the presurgery to the postsurgery session.
More recently, Zajac and his colleagues 21 followed 120 children from 12 to 24 months and estimated the age of stop emergence using parametric survival models. Four groups of children were studied, including a group with repaired cleft lip and palate (CLP), repaired cleft palate only (CPO), noncleft children with a history of frequent otitis media (OM), and a group of typically developing noncleft children without a history of otitis media (TD). In their study, stop emergence was defined as the production of three or more stops over two consecutive visits (either the same stop or a combination of different ones). According to the survival model used, the estimated age at which 80% of the children in each group would achieve stop emergence was 18.9 months for the CPO group and 21.8 months for the CLP group. In contrast, emergence of stops was estimated at 15 months for children in the TD group and 15.3 months in the OM group. Interestingly, when comparisons of the children with clefts assumed an age of palatal surgery of 10.5 months, the authors noted that the estimated time for emergence of stops was “1.36 times longer for an increase of 1 month in age at time of surgery” (p.35). The authors concluded that lack of stop development prior to 16 months of age is not a red flag for VPD, but noted that lack of stops by 20 months of age is reason for concern and recommended that clinicians be proactive and refer the child for early intervention. They also reported that later age at time of palatal surgery was associated with an increase in age at time of stop emergence.
The collective findings reported in the studies cited above suggest that oral stops will emerge spontaneously for the majority of children with repaired cleft palate anywhere from 2 months to 8-11 months post-palatoplasty depending on cleft type. The investigations reported to date have provided limited information about specific stop production and many reports suffer from small sample sizes. The current study was conducted to expand our knowledge of stop production following palatal surgery in a large cohort of children. We were interested in examining both the patterns and timing of stop development to facilitate decisions regarding the type and timing of clinical care. If the majority of children with repaired cleft lip and palate simply acquire oral stops slower than their noncleft peers, then their absence immediately following surgery may not always indicate a need for direct intervention. However, evidence-based decision making regarding the need for intervention requires data to determine what is typical for children with cleft palate post palatoplasty. Specifically, we asked the following questions:
What percentage of children with repaired cleft palate +/− cleft lip produce stops at approximately 16-months? What percentage of children with repaired cleft palate (+/− cleft lip) produce labial stops, alveolar stops, velar stops, or some combination within 6 months following palatal surgery? What is the relationship between oral stop production and age at time of surgery and/or time between surgery and assessment?
Methods
This study was reviewed and approved using a Single Institutional Review Board model with the University of Utah as the Institutional Review Board of record (IRB#00105205). Written informed consent was obtained at the sites for each child participant following federal law, regulation, and policy, including the policies set forth by the National Institutes of Health.
Participants
The speech samples used in this study were obtained from 113 children (76 males and 37 females) with repaired cleft palate ranging in age from 14-18 months (mean age = 16 months) who were participating in the multi-site CORNET study. The cohort included 15 children with bilateral cleft lip and palate (BCLP), 49 with unilateral cleft lip and palate (UCLP), 27 with isolated clefts of the hard and soft palate (HSP), and 22 with isolated clefts of the soft palate only (SPO). All participants were from homes in which English was reported to be the primary spoken language.
All participants had undergone palatoplasty prior to the time of the study. Age at time of palatal surgery ranged from 9-16 months (mean = 11.88 months). Time between palatal surgery and speech assessment ranged from 1-9 months (mean = 4 months).
Information regarding middle ear status and hearing was obtained through hospital records and parental report. Of the 113 children, 81% (92/113) had received pressure equalizing tubes. Parents of 105 participants (93%) completed the Ages and Stages Questionnaire (ASQ-3) 22 and the problem-solving score was used as a proxy for cognitive development. Cut-off scores were used to estimate whether a child's development was on schedule, borderline, or in need of additional assessment. Seventy-eight of the 105 participants (74%) demonstrated problem solving skills that were considered to be on schedule while 14 (13%) were in the borderline range. Scores suggesting the need for additional assessment were reported for 13 (12%) children.
Procedures
Each participant's parents were asked to record approximately two-to-four hours of their child's vocalizations/words at home using a Language ENvironmental Analysis (LENA) -digital language processor (DLP). The LENA DLP is a small audiorecorder that can be placed in a vest that the child wears throughout the recording period and holds the microphone-to-mouth distance relatively constant. When the audiorecording is subsequently uploaded and processed, the LENA software automatically identifies the number of vocalizations a child produces throughout the recording and displays this information in hourly and five-minute intervals.
The LENA software was used to identify each child's hourly Child Vocalization Count (CVC) during the recording. Eight consecutive five-minute audio-recorded segments were extracted from the child's most vocal hour. Those segments were imported in pairs and aligned using Audacity audio editor software to create four ten-minute audio-recorded samples of vocalizations for each participant. A minimum of 100 vocalizations were required across the four ten-minute segments to ensure an adequate sample size for analysis. In cases where the minimum number of vocalizations was not evident across consecutive segments, eight segments with the most vocalizations were identified for inclusion to ensure that at least 100 vocalizations were available for analysis. Coders listened to the audiorecordings on a computer using Sennheiser (Model eH 1430) headphones.
Modified Naturalistic Listening in Real Times (NLRT) Analysis
The modified NLRT analysis used in this study was described previously 23 and was performed using TimeStamper software. 24 This software identifies annotations of two different keystrokes: one for canonical syllables and one for noncanonical syllables. Each ten-minute recording was loaded into the TimeStamper program and assessed once in real time without pause. A cumulative count of syllables was recorded by the TimeStamper program. Each coder also recorded the consonants they heard the child produce on a coding form. To be considered in a child's inventory, each consonant had to be produced a minimum of two times across the entire sample.
The audiorecordings were coded by two transcribers: one certified SLP and one graduate student in speech-language pathology. Prior to initiating data analysis, the certified SLP participated in a training session on the NLRT approach and the TimeStamper software with Dr. Elisabeth Willadsen who was experienced in using the software. The certified SLP replicated the training protocol with the student author several months later. The major types of vocalizations (ie, canonical syllables, marginal syllables, fully resonant nuclei, and quasi-resonant nuclei) were reviewed. Reflexive vocalizations (ie, cry, laughter, laughed syllables without a consonant, hiccups, burps, sneezes, sounds of effort/grunts) and babbling sequences that did not contain a vowel (eg, st) were excluded as were vocalizations produced when the child had something in his/her mouth (ex. pacifier; food). Prolonged consonants that conveyed a specific message (eg, “shhh” to indicate “be quiet”; “mmm” to indicate “yummy”) and consonants heard during whispered words and singing were included.
Data Analysis
Descriptive analyses were performed to characterize stop usage across the participants including frequency of individual stops as well as place and voicing characteristics of the stop productions. Regression analyses were performed to examine the association between number of oral stops and (1) age at time of surgery and (2) the number of months between surgery and the 16- month assessment. All models controlled for cleft type, biological sex, and the ASQ problem solving score. Models were compared using adjusted R-squared and Akaike's Information Criterion to determine which best fit the data and explained the variability in stop inventory.
Reliability
Both transcribers independently coded the number of syllables from 53 of the total 113 recordings (47%) using the modified NLRT. Interjudge reliability for total number of consonants in inventory and number of stops, calculated using Pearson's product moment correlational analysis, was 0.94 and 0.94, respectively.
Results
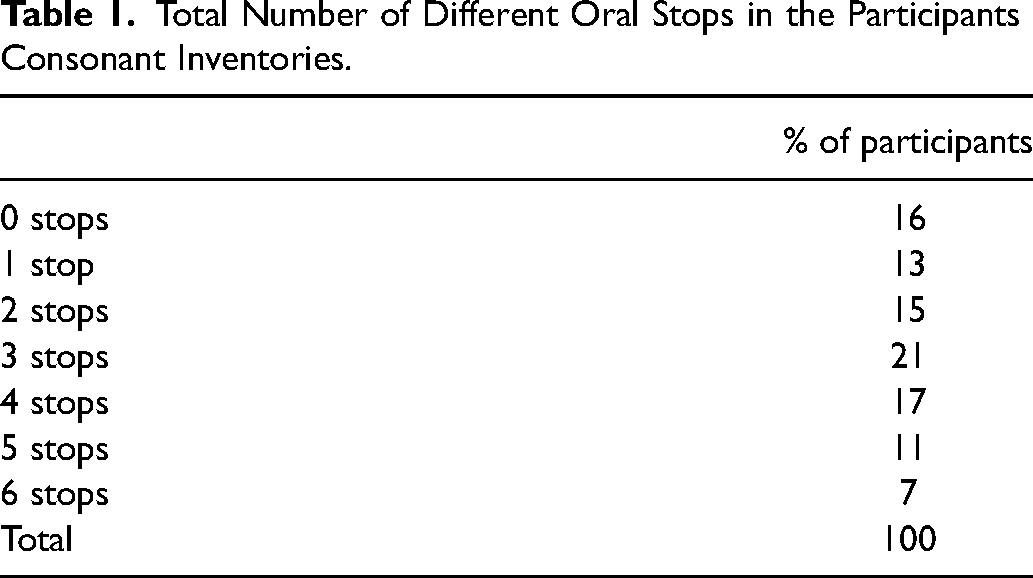
Sixteen percent (n = 18) of the participants were not producing any oral stops at the time of their assessment (see Table 1). At least one oral stop was evident in the consonant inventory for 95 of the 113 children (84%) at the time of their post-surgery recording, and 80 of these children (71%) were producing two or more different stops. Approximately 50% (n = 57) of the children produced the three voiced stops and eight of the children (7%) were producing all 6 stop consonants.
Total Number of Different Oral Stops in the Participants Consonant Inventories.
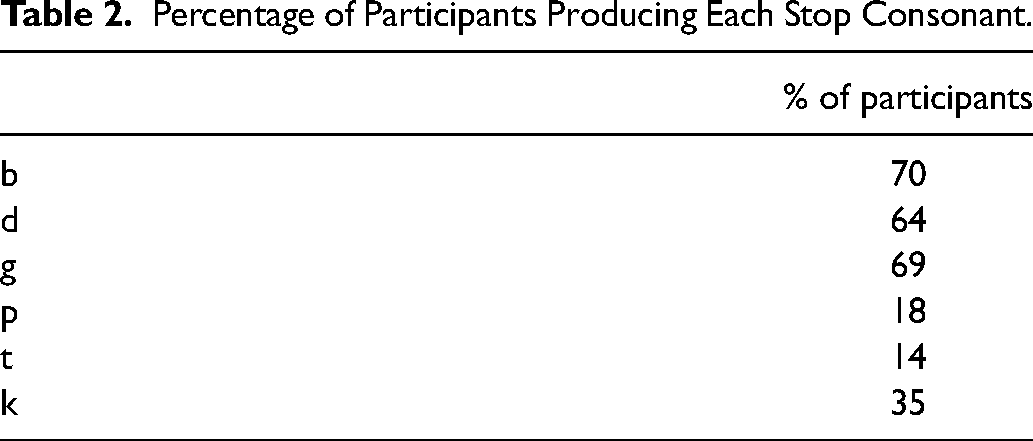
As evident in Table 2, the voiced stops /b/, /d/, and /g/ were present in 70%, 64%, and 69% of participant's consonant inventories while the voiceless stops of /p/, /t/, and /k/ were present in only 18%, 14% and 35% of the children's inventories, respectively. When the data were collapsed by place of production, labial, alveolar, and velar stops were produced by 70%, 64%, and 70% of the children, respectively.
Percentage of Participants Producing Each Stop Consonant.
Differences were apparent in stop production across different cleft type groups. At least one oral stop was evident in the consonant inventory for 77% of children with SPO clefts, 96% of children with clefts of the HSP, 76% of children with UCLP, and 100% of children with BCLP (See Table 3). A much larger percentage of children in the SPO and HSP groups produced 3 or more stops (55% and 75%, respectively) compared to children in the UCLP and BCLP groups (42% and 67%, respectively).
Percentage of Children in Each Cleft Type Subgroup Producing Stops.
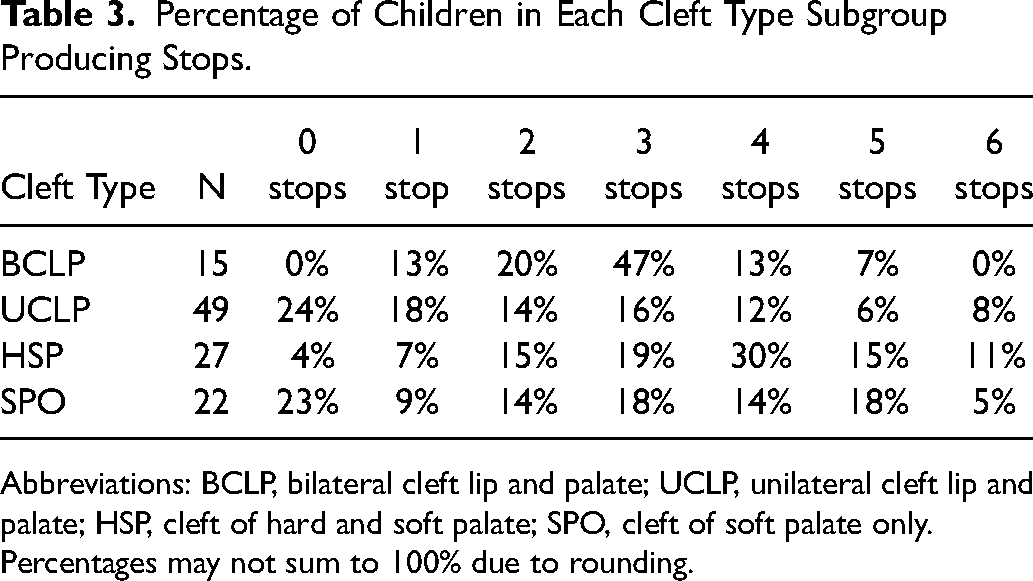
Abbreviations: BCLP, bilateral cleft lip and palate; UCLP, unilateral cleft lip and palate; HSP, cleft of hard and soft palate; SPO, cleft of soft palate only.
Percentages may not sum to 100% due to rounding.
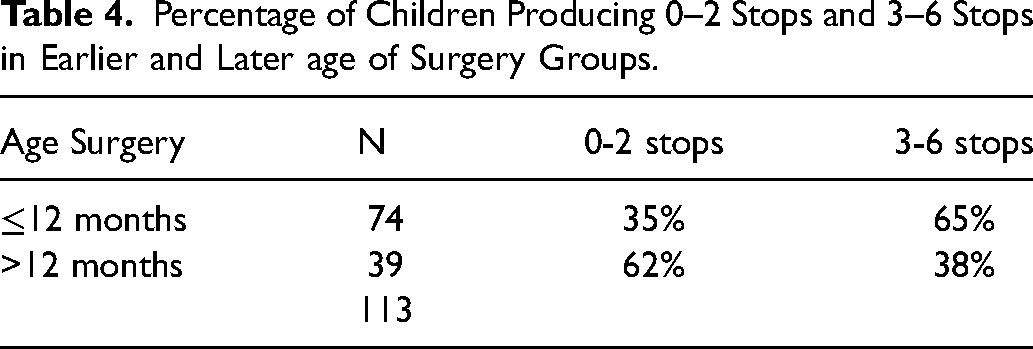
The impact of age at time of surgery on oral stop production was examined for children who received palatal surgery at or prior to 12 months of age and those who received surgery at 13 months and beyond. Oral stops were absent in a much smaller percentage of children in the early surgery group (12%) than the later surgery group (23%). A larger percentage of children in the early surgery group produced 3-6 stops (65%) compared to children in the later surgery group (38%) (see Table 4).
Percentage of Children Producing 0–2 Stops and 3–6 Stops in Earlier and Later age of Surgery Groups.
Linear regression revealed that each month increase in age at palate repair was associated with 0.36 fewer total stops (P < .007), and each additional month between surgery and the 16-month assessment was associated with 0.45 additional stops (P < .000). Because these two time measurements are highly correlated, they were examined in separate regression models, each adjusting for cleft type, biological sex, and the ASQ problem solving score. Comparison of model diagnostics revealed that the model assessing the impact of months between surgery and the assessment fit the data best and more completely explained the variability in the outcome variable (see Table 5).
Regression Analysis Results.
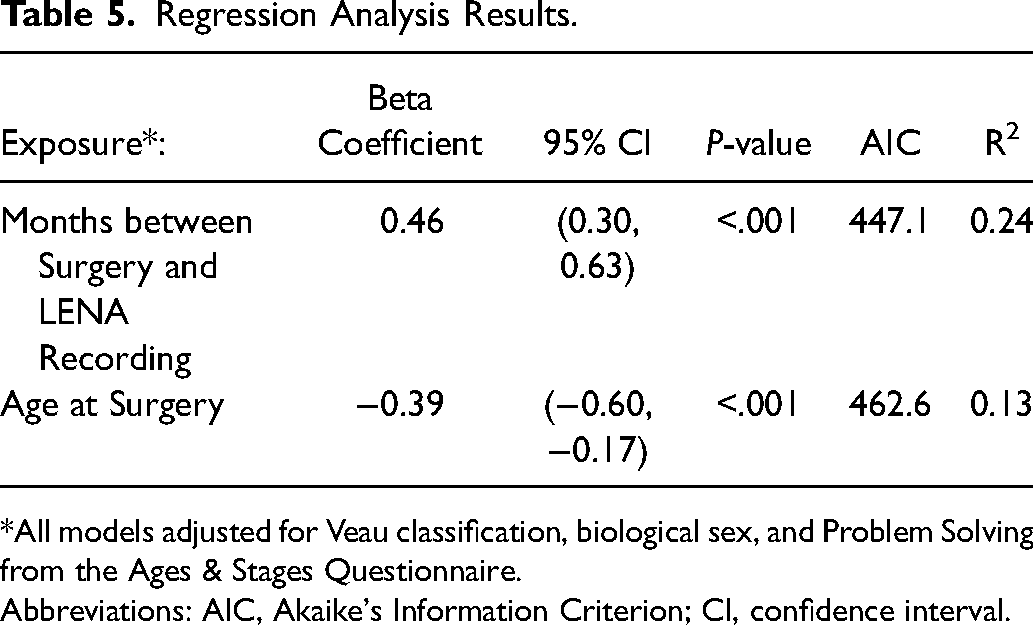
*All models adjusted for Veau classification, biological sex, and Problem Solving from the Ages & Stages Questionnaire.
Abbreviations: AIC, Akaike's Information Criterion; CI, confidence interval.
Discussion
The current investigation studied oral stop production in young children with repaired cleft palate following palatal surgery and examined the relationship between stop production and age at time of palatal surgery. Eighty-four percent of the children produced at least one oral stop during their post-operative assessment, 71% were producing two or more different stops, and 7% produced all 6 oral stops. Both cleft type and age at time of surgery appeared to influence stop production in this cohort.
Postoperative Stop Consonant Production
The majority of children with repaired cleft palate in this study produced one or more oral stops within 6 months following palatoplasty. Voiced stops were more commonly present than voiceless stops and a comparable percentage of children in this study produced bilabial stops, alveolar stops, and velar stops. These latter findings stand in contrast to those previously reported by Vallino and her colleagues 25 and Jones, Chapman, and Hardin-Jones. 19 In their investigation of stop consonants, Vallino and colleagues reported that a larger percentage of 18-month-old children with repaired cleft palate (n = 53) produced alveolar stops (68%) than bilabial (55%) and velar stops (51%). They noted that, in contrast to previous reports, their children appeared to be “most delayed relative to the production of bilabial stop consonants” (p. 94). The participants in the Vallino et al, study 25 were a subset of children followed in the Zajac et al 21 study. Although they did not report phonetic inventories in the Zajac et al study, the authors did state that “voiced stops, particularly /b/ and /d/, were the stops that emerged for most children regardless of cohort” (p.37). Jones and colleagues 19 also found that bilabial and velar stops occurred more frequently in the post-operative inventories of their 17-month old children with repaired cleft palate (71% and 79%, respectively) (n = 14) while only 36% of children produced an alveolar stop. The differences observed between these investigations can probably be attributed to differences in sample size and methodology. The participants in the current investigation and the Jones et al study were recorded as they vocalized in their natural environment, whereas participants in the Vallino et al study 25 were recorded as they responded to prompts during administration of the Communication and Symbolic Behavior Scales Developmental Profile. 26
Voiced stops usually emerge before voiceless stops in typically developing, noncleft children 27 and that same trend was noted for participants in the current study as well. In an early investigation of phonetic inventories in typically developing children ages 15-24 months, Stoel-Gammon 27 reported that “initial inventories contained voiced stops prior to voiceless ones, with the reverse situation (ie, voiceless preceding voiced) holding in final position” (p. 510). Using implicational statements, she noted that (1) the presence of a velar phone in the word initial position implied the presence of both labial and alveolar phones and (2) the presence of a velar phone in the final position implied the presence of an alveolar phone. Although syllable position was not recorded in the present study, seven children produced velars but no labials or alveolars. Five of the seven children produced only /g/ while the remaining two children produced both /g/ and /k/. This observation was consistent with previous reports documenting the presence of velar stops in the early sound systems of children with and without cleft palate.5,28,29
While participants in this study showed trends similar to that reported for noncleft children in the emergence of voiced consonants, differences were evident when place of articulation was considered. Stoel-Gammon 27 and Robb and Bleile 28 found differences in place of articulation during emergence of stop consonants in their typically developing cohorts, with anterior phones (labial and alveolar) tending to emerge prior to posterior ones. Labial and velar consonants were produced by more children in the current study, than alveolar consonants.
Impact of Age at Time of Surgery and Cleft Type on Stop Production
The findings of this study are consistent with previous investigations reporting an association between age at time of palatal surgery and stop emergence in children with cleft palate.8,9,21 In this study, children who received early surgery at or before 12 months produced a greater number of different stops than children who received surgery after 12 months of age. Authors have previously suggested that it can take 3-6 months for some children to begin producing stops following palatal surgery.12,30,31 We found that only 21% of the children in this study were producing oral stops three months following surgery, 70% were producing stops 6 months out, and 95% were producing stops nine months following surgery. Similar findings were reported by Zajac and his associates 7 with approximately 80% of their cohort achieving stop emergence 7-8 months following surgery. In terms of age at time of stop emergence, Zajac and colleagues reported that 58% and 83% of their cohort of 52 children with cleft palate achieved emergence of stops at 16 months and 18 months, respectively. In our cohort of 113 children, 78% were producing stops by 16 months and 84% were producing stops by 18 months of age.
Differences in oral stop production were also evident across cleft type groups. While 75% or more of the children in each group were producing at least one oral stop, a much larger percentage of children with isolated cleft palate (CPO) produced multiple stops compared to children in the CLP group. Of particular interest in this study was the finding that a much larger percentage of children with BLP (100%) produced at least one stop when compared to children in the other cleft type groups (76%-96%). Although a relatively small sample size in this group (n = 15) could have contributed to this finding, previous reports of cleft type differences in older children have suggested that young children with CLP tend to demonstrate poorer articulation than children with CPO (see Peterson-Falzone et al 11 for a review). The participant's articulatory performance will be reassessed at three years of age to determine if children in the BLP group demonstrate comparable if not better findings than children in the other cleft type groups.
Modified Naturalistic Listening in Real Time (NLRT)
The modified naturalistic listening in real time (NLRT) approach used in this study was found to be an efficient and reliable method for documenting emergence of consonants for research purposes. 23 Unlike phonetic transcription, which is more labor intensive and may be more likely to overestimate a child's speech production capabilities, NLRT is thought to mimic what parents’ perceive when listening to their child. Ramsdell et al 32 argued that parents attend to global sound patterns and attend less to phonetic detail. They recommended that “the functional repertoire of infant syllables is best seen as that repertoire recognized by caregivers” (p. 1627). In the current study, parents were also asked to indicate sounds their children produced; thus, parent reports of phonetic inventory size were available for 64 of the participants in this study. In all but 18 cases, the inventory size reported by the coder was larger than that of the parents. Parents and coders agreed on inventory size for eight participants while parents reported a larger inventory than was transcribed for 10 children. These findings contrasted with those of Ramsdell and her colleagues 32 who compared the syllable inventories obtained using parent report, phonetic transcription, and naturalistic listening. During their naturalistic listening task, however, raters were instructed to listen to samples of recorded speech in real time without pausing the recording or taking notes. The syllable types produced by the child were then recorded from memory. The authors reported that similar syllable inventories were obtained between parent report and naturalistic listening. Larger syllable inventories were obtained using phonetic transcription. Differences between the parent-reported consonant inventories and those coded by the listeners in this study can probably be attributed to the online tallying of consonants used in the modified NLRT. Unlike the NLRT procedure which was designed to identify functional or frequently occurring consonants, the modified NLRT was designed to identify both emerging and frequently produced consonants. Interestingly, although the coders in this study routinely identified a larger phonetic inventory than that reported by the participants’ parents, both groups agreed on presence or absence of stops in each child's inventory 86% of the time. The findings of this study suggest that NLRT is an appropriate method to use when the goal is to identify the consonants that are most likely to be available for word learning; however, we chose a modified NLRT approach in this project because we were interested in identifying the number of children for whom stops had emerged.
Clinical Implications
The findings of this study have implications for the initial sounds to be targeted in therapy as well as the timing of intervention for young children with cleft palate. In the past, clinicians treating children with CLP have expressed concern when oral stops do not begin to emerge in the weeks following palatal surgery and speculated that the absence of stops might be related to post-operative velopharyngeal dysfunction (VPD). The findings of this study and other recent reports14,21,30 suggest that while stop emergence may be delayed for many children with cleft palate, stops will begin to emerge for the majority of these children within 6-8 months following surgery. When stops do not emerge within that timeframe, decisions regarding early intervention must be addressed (if the child is not already receiving it for other reasons). Facilitating the production of stop consonants is an appropriate target for early speech-language intervention since they are early developing consonants but the option of which type of stop to target is often questioned. Voiced stops typically emerge first in children with and without cleft palate and so are often considered appropriate targets to work on first in intervention. But when glottal stops are substituted for oral stops, clinicians have recommended stimulating a voiceless stop with a voiceless (whispered) vowel first to discourage those aberrant productions. Although this may be appropriate for some children (particularly older children) who are producing glottal stop substitutions, it is important to recognize that young children in the single word stage may substitute a nasal or glottal during the transition to oral stop production. 18 Interestingly, although glottal stops were produced occasionally by some of the children in this study, none produced pervasive glottal stops. In addition, at this assessment point, there was little difference in occurrence of stops by place of articulation. Therefore, when choosing which stop to target, consideration should be given to stimulable consonants or place of articulation of other “in-inventory” consonants that could be used to “shape” production of the stop at that same place of articulation. 12
A word of caution seems appropriate here. Historically, clinicians were concerned that absence of oral stops in the months following palatal surgery might be an early indicator of VPD. The evidence suggests, however, that slower emergence of stops is characteristic of most children with repaired cleft palate- even those with adequate velopharyngeal function. Only 14 of the children in this study (12%) were receiving speech-language intervention at the time of their 16-month postoperative evaluation. So while early intervention to expand phonetic and lexical inventories may have facilitated the emergence of stops for some children, emergence occurred spontaneously for the majority of them. Knowing that children with clefts demonstrate slower emergence of stops, however, should not lead clinicians to become complacent in advocating for early speech-language stimulation/intervention. Rather the slower acquisition of stops in this group of children should be interpreted within the context of their broader communicative profile.
Compared to their noncleft peers, young children with cleft palate frequently demonstrate smaller phonetic and lexical inventories17,33,34 that warrant speech-language intervention. While inventory sizes of 3-6 word-initial consonants (including 2-3 oral stops) have been reported in the early words produced by typically developing children at 15-18 months, 27 larger inventory sizes of 6-9 consonants (including 2-5 oral stops) have been reported in children ages 15-18 months when all non-reflexive productions are transcribed. 28 Because a young child's phonetic inventory tends to expand to accommodate growth in vocabulary, lack of sound contrasts in words can result in poor intelligibility. While no studies have directly addressed the impact of a limited consonant inventory on speech intelligibility that we are aware of, studies have examined the relationship between size of consonant inventory and vocabulary skills.35–39 We know from studies of late talkers35,36 that in addition to lexical delays, these children also exhibit smaller consonant inventories; thus, deficits in consonant production and vocabulary development go “hand-in-hand”. As noted by Stoel-Gammon, 38 a limited number of sounds in the child's production repertoire limits the number of words that can be produced. The implications for delays in consonant development on vocabulary growth may be even more impactful for children with cleft palate.16,17,34 Hardin-Jones and Chapman 17 and Lu and colleagues 34 both found that children with cleft palate were similar to noncleft peers for size of expressive vocabulary until approximately 13-14 months, after which age their acquisition of new words slowed and the gap between the cleft and noncleft groups widened. Post hoc analyses by Hardin-Jones and Chapman 17 suggested that it was not just the number of sounds available to children with cleft palate but the type of sounds (predominance of sonorants over obstruents) and the sounds that are more common in the early words of children learning English (a predominance of stops/obstruents). Further, early deficits in consonant inventory may impact other speech and language skills at later ages for children with cleft palate.18,40
It is likely that many young children with delays in speech sound development will benefit from stimulation activities designed to enhance not only their consonant inventory but their expressive lexicon as well. While activities to stimulate a child's consonant and word development can be provided through direct speech-language intervention, they can also be provided through a home stimulation program. The option most appropriate for an individual child will depend on a number of factors including the child's ability to benefit from more direct intervention, whether other sound classes are missing from the child's consonant inventory, and the extent of the language delays. Clinicians can facilitate a parent's efforts to stimulate their child's phonetic and lexical development by educating them regarding age-appropriate expectations for consonant and early word development, demonstrating appropriate modeling strategies, and assisting them in identifying consonants that are easily stimulable. A key take-a-way from this investigation that should be reinforced with parents is that absence or slow development of stops in the months immediately following palatal surgery is not unusual for many children with repaired cleft palate and should not be construed as evidence of VPD. While many children are producing oral stops within the first several months postsurgery, it can take up to 6 months (and sometimes longer) for others. In addition, parents should be advised that aggressive monitoring and treatment of hearing and middle ear status is always indicated for these children to mitigate the influence of fluctuating hearing levels associated with middle ear fluid on early speech sound development.
Limitations
The current study examined the presence of stop production at a single age for toddlers who had undergone palatal surgery. In the absence of preoperative recordings, it was not possible to directly attribute onset of stop production to the repaired cleft palate nor could we determine the exact age at which stops emerged since we did not assess the children at frequent, repeated intervals. It is likely that differences in the emergence of stops by place of articulation may have been observed if the children had been evaluated at younger ages.
Although hearing data were available for 68 children in this study, hearing levels were not included as a co-variate in the statistical analysis because of differences in assessment protocols across sites and absence of any data for a substantial number of children. Normal hearing was reported for 60 children while a mild-to-moderate hearing loss was reported for 8 others. While we suspect that the conductive hearing loss documented in these children is related to ear disease and is fluctuating in nature, we did not assess hearing on the day that recordings were obtained and thus cannot isolate the impact of hearing on the children's phonological performance. It seems likely, though, that the reduction in hearing levels associated with middle ear disease contribute to the overall phonological delay demonstrated by many children with cleft lip and palate.
Conclusions
The findings of this study indicate that the majority of children with repaired cleft palate are producing one or more stop consonants within six months of palatal surgery. In our cohort of 113 children, 84% were producing stops by 18 months of age and the majority of these children had not received early intervention. These findings in conjunction with those reported by Zajac et al7,21 and Hardin-Jones and Chapman 14 suggest that early speech-language intervention may not always be indicated immediately following palatal surgery to facilitate production of these consonants. In the absence of concerns regarding size of consonant and lexical inventories, SLPs may opt to work with parents on development of a home stimulation program. Absence of stops in the months following palatal surgery should not be considered early evidence of VPD. Evidence of VPD, when present, will unfold over time as the child's speech sound system matures.
Footnotes
Acknowledgements
The authors would like to acknowledge the University of Liverpool CTRC for development of the TimeStamper software. They would also like to thank the children and their families who provided the data for analysis in this study. Finally, the authors would like to acknowledge the clinical sites participating in the Cleft Outcomes Research NETwork (CORNET) Consortium that contributed recordings for this project, listed below in alphabetical order: Ann & Robert H. Lurie Children's Hospital; Barrow Cleft and Craniofacial Center Dignity Health – St. Joseph's Hospital & Medical Center; Boston Children's Hospital; Cardon Children's Medical Center/Banner Children's Specialists; Children's Hospital of Alabama; Children's Hospital Colorado; Children's Hospital Los Angeles; Children's Hospital of Philadelphia; Lancaster Cleft Palate Clinic-Penn State/Milton S. Hershey Medical Center; Nationwide Children's Hospital; Phoenix Children's Hospital; Seattle Children's Hospital; Shriners Hospital for Children – Chicago; University of Iowa; University of Wisconsin – Madison.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Dental and Craniofacial Research, (grant number 1R01DE027493-01).