
Abstract
Objective
To discuss advantages, disadvantages and strategical application of anatomical subunit approximation technique in complete unilateral cleft lip repair.
Design
Analysis of consecutive 28 cases.
Setting
A single surgeon experience at a university hospital.
Patients
Among 77 patients who underwent cleft lip repair between May 5, 2019 and June 30, 2021, 28 patients with complete unilateral cleft lip who received cheiloplasty by author's technique.
Main Outcome Measures
Surgical outcomes were assessed by frontal view medical photographs obtained postoperatively at follow-up visits.
Results
The average length difference between cleft and noncleft sides was <10% for transverse lip length and philtral height. Nostril sill height demonstrated about twenty percent of difference with much variable results. Although the one sample t-test revealed that differences exist between the cleft and noncleft side, they were within an acceptable range.
Conclusions
Understanding the strengths and limitations of anatomical subunit approximation technique enabled strategic application in complete unilateral cleft lip repair. Satisfactory outcomes were achieved not only regarding the scar placement but also regarding the symmetry of the lips and augmentation of nasal sill.
Introduction
Principles and techniques of cleft lip repair have evolved and developed with history of plastic surgery. LeMesurier devised to lengthen the lip with Z-plasty. 1 Randall's technique allows downward rotation of cleft side with a backcut filled with a large triangular flap of lateral lip. 2 Although this technique is suitable for wide clefts and can be easily followed, esthetic outcomes such as scar position are considered unsatisfactory. In 1955, Millard introduced the rotation-advancement technique which has became the most widely performed method to date.3,4 Since Milard's introduction, surgeons such as Mohler and Cutting have made numerous modifications.
In 2005 Fisher described anatomical subunit approximation technique for cleft lip repair. 5 He managed to place the scar to mimic the normal philtrum by extending it toward the nostril floor. To balance the philtral columns, instead of rotating the noncleft side downwards with a backcut incision below the philtrum, small triangular flaps are transferred. Several studies have confirmed that the surgical outcomes of Fisher's technique are comparable with those of conventional techniques such as Millard's or Mohler's modifications.6,7,8 Previous researches focused on competence of Fisher's technique. However, detailed analysis concerning limitations of this technique has not been addressed. Despite that it is necessary to thoroughly understand its advantages and disadvantages for strategical application in patients.
This article described the author's design and technique for complete unilateral cleft lip repair. It is based on Fisher's method with modifications to overcome it shortcomings and maximize satisfactory results for both patients and surgeons.
Patients and Methods
Surgical Technique
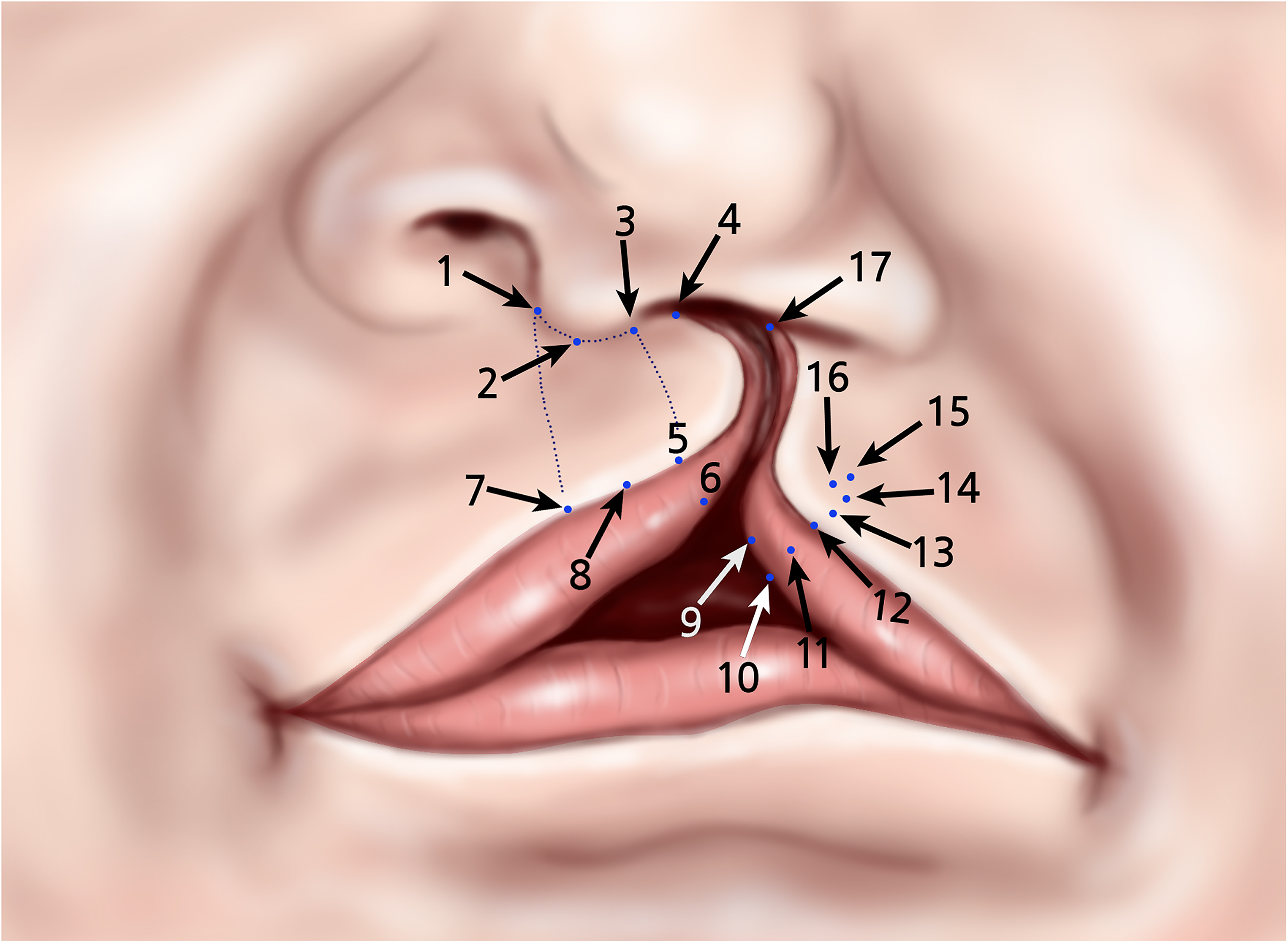
Key markings for surgical design.
Markings
Point 1 was marked at the border of the noncleft side lip-collumela crease, which corresponds to the height of the non-cleft side phitral column. Point 3 was marked to mirror point 1 to mark the height of the cleft side phitral column. Cupid's bow peaks and midpoint of lip were marked (point 57,8). On the lateral lip, the Noordhoff's point (point 12) was identified where the vermilion height is at its greatest to determine the vertical and horizontal lengths of the cleft side lip. Point 13 was placed on a perpendicular line from point 12 to the white roll. Triangular flap, which will be transferred to the medial segment, was marked by point 14,15,16.in larger size than expected.
On the lateral dry vermilion Noordhoff's flap was marked with sufficient size (point 9,10,11). Point 3 and 5 formed a line which mirrored the non-cleft side philtral column. Point 4 was an estimated point of closure of the cleft side's nasal sill. Incision line started from the lateral base of columella (point 3), running down the slope 3–5 and 6 to reconstruct the philtral column. At this point, marking of perpendicular opening incision from point 6 that received the Noordhoff's vermilion flap from the lateral side was unnecessary because the red line could be easily defined during the procedure. Superiorly, the incision will be made toward the nasal sill (point 3–4) and continue along the nostril sidewall during the execution, following Fisher's anatomic subunit approximation design.
Fisher's design was based on precise measurements and calculation for the lateral lip. Contrarily, we limited the markings to the vermilion and small triangular flap. No markings were made on the medial margin of skin to clearly visualize the border of the skin and mucosa. Incision was made from the point 15 along the skin edge toward the nasal vestibular web on the cleft side, passing point 17. As measurements of lateral lip are susceptible to change with dissection, appropriate size of triangular flap and estimated point of closure can only be determined after releasing the orbicularis oris muscle and partial skin closure with dermal suture of the Cupid's bow peak.
Execution
After the skin marking, the procedure started from point 13 to the lateral nasal vestibular web area elevating the lateral flap(L flap), a superiorly based flap composed of skin and mucosa. Upper limit of this incision ends at the nasal vestibule and lower limit passes the points 11-9-10. An opening incision on the nasal vestibule was made running cephalad to receive 180° superiorly rotated L flap. To avoid a narrow nostril, rotated L flap was inserted and sutured to the nasal vestibular opening incision. The oral lining of the lateral portion of nasal floor was also reconstructed using this procedure.
Subsequently, lateral orbicularis oris muscle(OOM) was dissected in a conventional manner. It is important to release the abnormal attachment of the OOM to correct the appearance and restore its function. On the medial lip, incision line was made from point 6-5 to 3 and extended along the lateral lip-columella junction towards the lateral base of the columella and continued into the nostril passing the point 4 along the way. The opening incision above the white roll of medial lip is not made at this point. A posteriorly based mucosal flap was elevated(M flap) lateral to this incision. Fisher's technique does not create the Millard's C flap. Thus, M flap can be elevated with a broad base, guaranteeing a robust, reliable flap large enough to reconstruct the inner lining of the medial portion of nasal floor. Dissection was continued from point 4 to reach the caudal septum to allow repositioning it to the midline. M flap is turned down laterally to the nasal floor and sutured to the previously interpositioned L flap. All tissues of M and L flaps were recruited to reconstruct the inner lining of the nasal floor as much as possible without discarding. Thus, upper part of the L and M flaps were used to create the oral lining of the nasal floor. The lower part of these two flaps formed the oral lining that corresponds to anterior gingivobuccal sulcus.
Before suturing the OOM, innermost nostril skin flap from the lateral side and columella base flap from the medial side were partly sutured to reconstruct the nasal lining of nasal floor, since it is difficult to place the sutures after OOM approximation. Vermilion free border was closed temporarily. Then mucosal closure of the inner sulcus was cautiously executed with proper spacing to approximate both sides equally by trimming tissue and adjusting the location of sutures. L and M flaps can be trimmed if surplus tissue exists. Subsequently, OOM muscle was approximated.
Next, dry vermilion closure was performed where the opening incision was made on the red line(from point 6) of the medial lip. It receives the Nordhoff vermilion flap, which is formed by connecting points 10-9-11-12. The lateral vermilion flap was trimmed, if needed, to appropriate size and inserted to the opening incision of the medial lip vermilion. To evaluate shape and symmetry of vermilion, Cupid's bow peak was formed by applying a dermal suture, approximating point 5 and 12. To gain symmetry with lengthening of the medial side, especially in complete cleft lip, skin opening incision was made above the white roll of the medial lip perpendicular to line 3–5. Only after completion of this maneuver, we could decide the proper size of the required inferior triangular flap to level the peak of the Cupid's bow of both sides. Following transposition of properly sized triangular flap, dermal sutures placed in caudal to cephalad direction. At this point, generous amount of skin of lateral lip segment might remain below the alar base. This redundant soft tissue was not discarded and sutured in situ, in order to overcorrect the height of the nostril sill.
Study Population and Outcome Measures
Patients with complete unilateral cleft lip who underwent cleft lip repair in our institution during the study period were included in this study. Patients with incomplete unilateral clefts were excluded because severity of the cleft would likely affect the surgical results. Lastly, cases without proper pre- or postoperative medical photographs or those lost to follow-up visits were excluded. Retrospective review of medical records and photographs was conducted. Baseline patient demographics including sex, laterality of the cleft, age at the time of surgery and date on which photograph was taken, were collected. This study was approved by the Institutional Review Board of Samsung Medical Center (IRB file no.: 2022-05-035). All patients provided informed consent for the operative procedures and postoperative managements.
Surgical outcomes were evaluated based on medical photographs obtained at the last visit. Frontal view photographs were assessed with the ImageJ software program (National Institute of Health, Bethesda, Md). To evaluate symmetry, transverse lip length(LL), length of philtral columns and height of nostril sill (NSH) were measured. Transverse LL was defined as the distance from crista phitra to cheilion. Philtral height (PH) was the vertical distance from the crista phitra to alar base line. Alar base line was defined as a straight line connecting the lowest point of both alar crease. NSH was the vertical length from alar base line to the lowest point of nostril (Figure 2). As the measurements were conducted in pixel units, ratios between the cleft and noncleft sides were obtained and analyzed. All statistical analyses were performed using SPSS version 20.0 (IBM Corporation, Armonk, NY, USA).
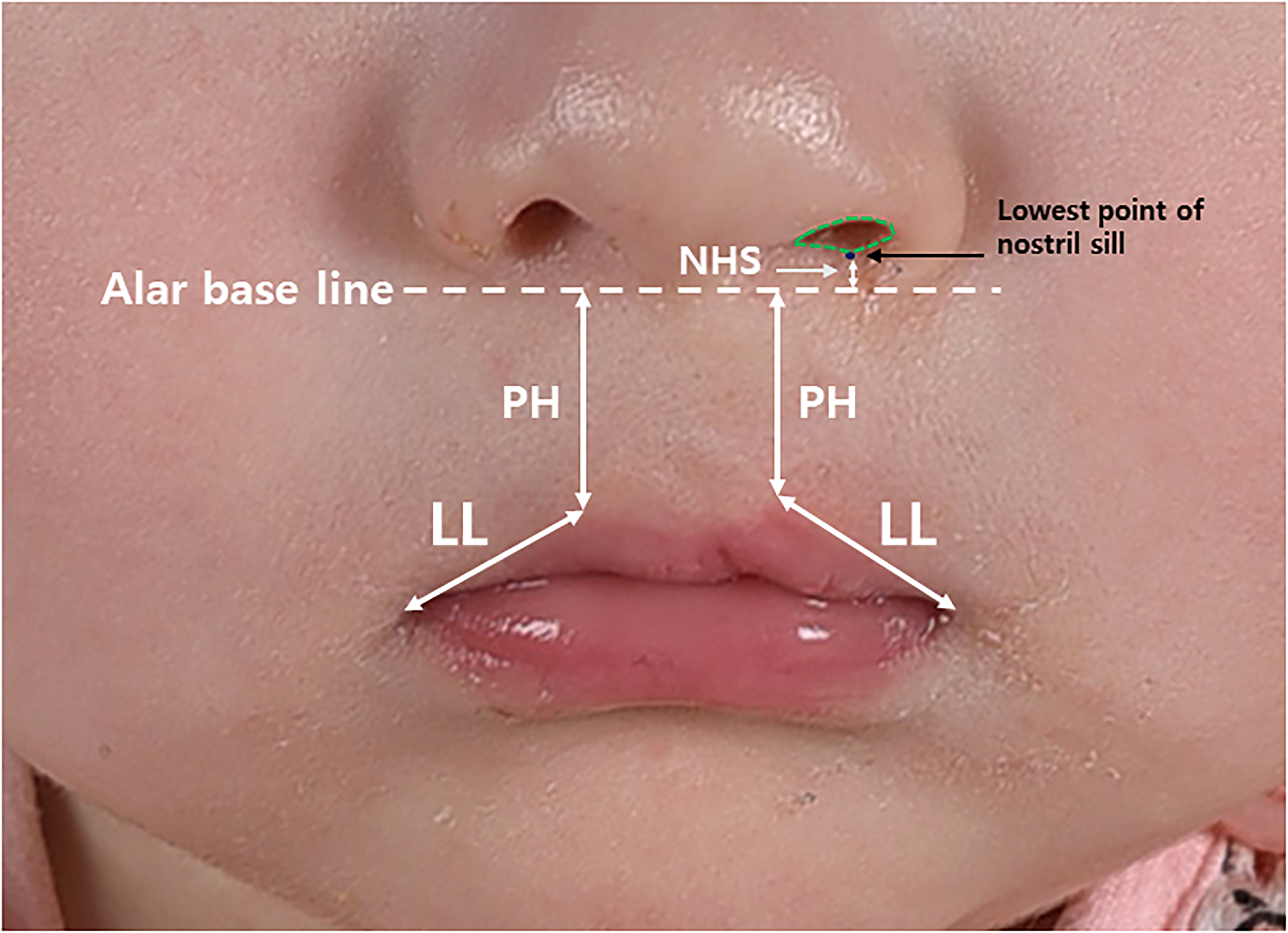
Measurements to evaluate symmetry of cleft and noncleft side. LL; Lateral lip length, PH; Philtral height, NSH; Nostril sill height.
Results
Total 77 patients underwent cleft lip repair surgery at our institution during the study period. Twenty-eight patients were included in the study. Number of patients with a right cleft and left cleft were 7 and 21, respectively. 10 girls and 18 boys were included. Mean age at the time of surgery was 114 days. Analyzed photographs were obtained at an average of 296 days postoperatively.
Frontal view of postoperative photographs were analyzed. Table 1 lists the mean and standard deviation of the calculated values. Ratio of LL and PH showed similar values demonstrating that the length was shorter on the cleft side within average difference of 10%. NB was lower on the cleft side. All the three obtained values were found to be normally distributed. One sample t-test was conducted for normally distributed parameters with the test value of one. The 95% confidence intervals are listed in Table 1. Transverse LL had the most narrow interval, because of relatively consistent results. NSH varied the most, with the widest interval showing lower bound up to 33% of difference.
Analysis of Parameters of Symmetry in Ratio.
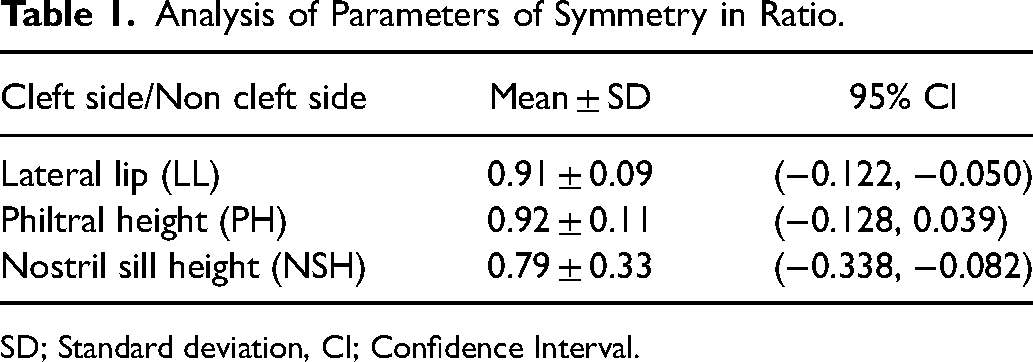
SD; Standard deviation, CI; Confidence Interval.
Discussion
Anatomical subunit approximation technique has gained worldwide popularity. Its strengths have been discussed in numerous studies. However, the limitations and strategical application in patients have not been investigated in detail. We suggest a surgical technique based on Fisher's technique with strategic application for satisfactory outcomes.
Photographic assessment and statistical analysis showed length of cleft and noncleft side to achieve 1:1 for LL and PH. Sufficient lengthening, within 10% of difference in length, of cleft side was achieved without critical sacrifice of lateral lip's transverse length nor a backcut violating the columellar base.
NHS was corrected but not as much as PH and LL, and the results were more variable. This is related to the difference in the soft tissue of each patient. If a patient has a surplus of soft tissue to build the nasal base, overcorrection of the nostril sill can be performed to achieve symmetric appearance in the long term. Recent studies suggest that primary rhinoplasty can be safely performed without facial growth restraint. In this sense, we focused on correcting the skewed axis of growth rather than the nostril shape itself. In the long run, setting the growth axis upright would result in balanced nasal appearance than manipulating nasal cartilage by direct intervention. In addition, alar cartilage of 3 month old Asian children is fragile and prone to damage during surgical manipulation. Sutures or grafting techniques applied to an injured cartilage do not show a good long-term results. For this reason, direct manipulation of alar cartilage was not performed at this stage.
Limitations of Anatomical Subunit Approximation Technique
When performing the Fisher's repair according to the original description, 25 landmarks are defined and the surgical design is completed before the initial incision. This procedure is time consuming and less efficient regarding the distorted anatomy of cleft lip. 9 Landmark markings and measurements, especially on the lateral lip, are prone to change when underlying OOM muscle is freed from its attachment.
Millard performed “cut as you go” technique with the backcut of the medial lip. Similarly, the senior author applied the principle to the lateral lip since anatomic landmarks change as dissection continues. Adjustments including the lower triangular flaps and opening incisions to receive those flaps were made during the final step of skin closure, only after releasing OOM and suturing Cupid's bow peaks. Intraoperative design can reflect even small changes of landmarks during the operation following this procedure.
Fisher's design of the lateral lip segment is completed before the incision. 1 In cases with long lateral lip segment, even wedge resection of skin was performed. However, as mentioned beforehand, markings are prone to change and even small amount of soft tissue can be utilized to augment the nostril sill height. Therefore, no skin excision was made on the lateral lip before closure. This gives a great flexibility to the reconstruction of nostril sill.
The advantage of Fisher's technique for cleft lip repair is that tissue is realigned in anatomic subunits without incision crossing the columellar base and results in less scar formation. However, the lengthening of medial segment depends only on Rose-Thompson effect and small triangular flaps, without any backcut incision. It provides insufficient lip length especially for severe complete clefts. Particularly, in children who did not undergo preoperative nasoalveolar molding.
Figure 3 demonstrates the calculation devised by Fisher to determine the base of the inferior triangle flap. The base width (c) equals the difference between two lip heights with 1 mm reduction gained from Rose-Thompson effect (ab1 = c, a = b + c + 1). Fisher explained that the length c is kept ≤ 2 mm. 1 According to his formula, difference between two lip heights (ab) should not exceed 3 mm. Thus, method to deal with a severe cleft with a length difference ≥ 3 mm is unclear. When the difference exceeds 3 mm, relatively large sized triangular flap or multiple triangular flaps should be transferred. However, a large triangular flap leaves a scar similar to Randall's technique (Figure 4). In this situation, it is questionable whether applying Fisher's method can truly reduce the scar burden.
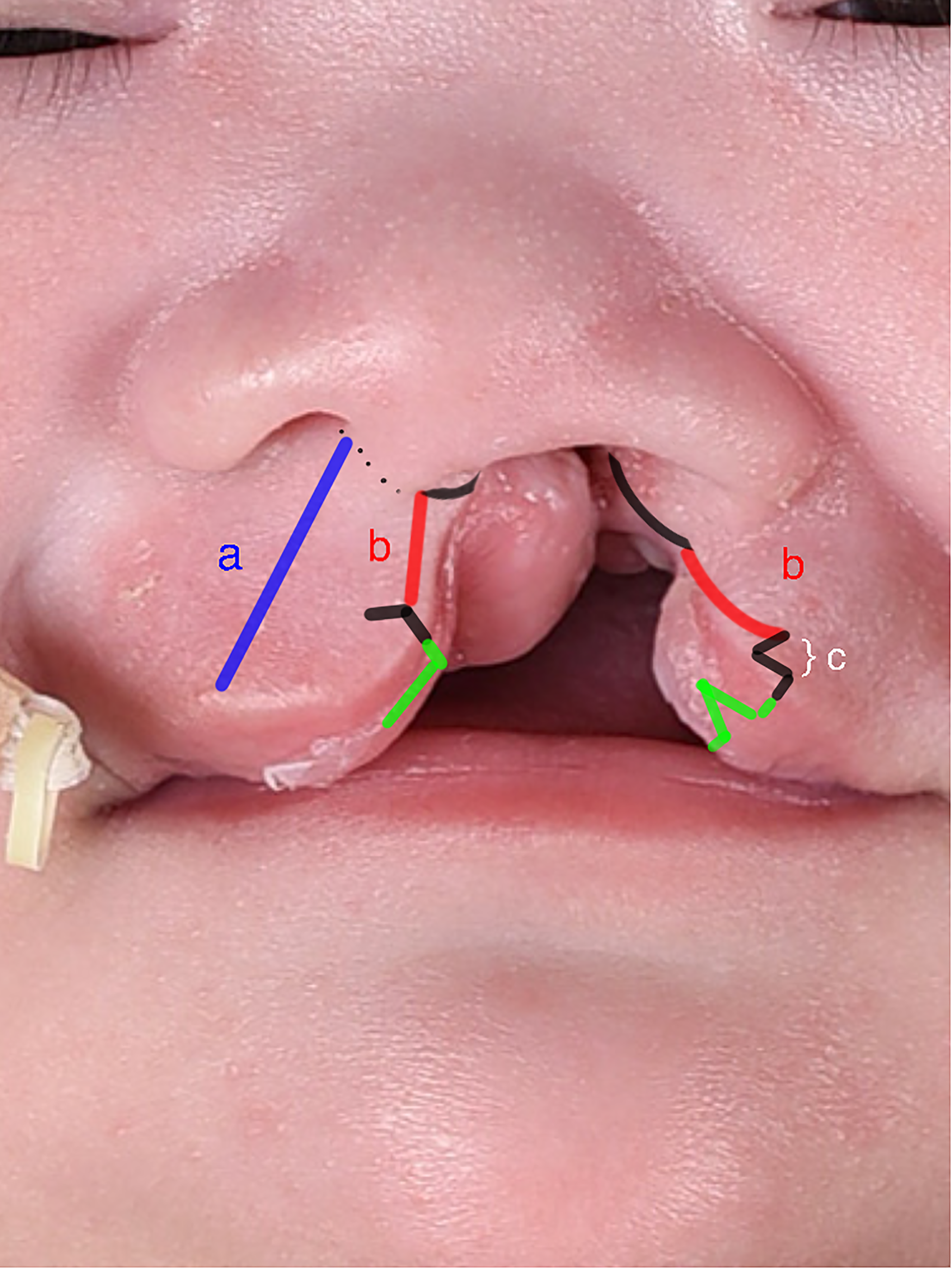
Authors’ surgical design with description of Fisher's formula for determining the size of inferior triangle. a = b + c + 1.

Postoperative photo of a patient who had a large sized inferior triangle transferred. Note the scar violating the philtral column.
When determining the size of the lower triangle, Fisher's formula is used if ab is ≤ 3 mm. However, if it exceeds 3 mm, transferring relatively large amount of tissue from lateral lip is unavoidable. No consensus is yet made regarding the number and size of triangular flaps in severe complete clefts. In this case, one large triangular flap should be divided into two or three small ones to avoid a scar violating the philtrum.
Correcting the Nasal Base
Performing primary rhinoplasty to correct the displaced septum and low lateral cartilage at the time of cheiloplasty is generally an accepted idea. Despite primary rhinoplasty done at its best, height of the nostril sill of the cleft side tends to collapse with time.
Millard advanced the lateral lip medially to fill the defect produced by elevation of the C flap. Contrarily, Fisher did not create the C flap; therefore, the tissue from the lateral lip can be turned up or down as desired. When lateral lip tissue under the nostril sill was concluded to be excessive by Fisher's calculation, he resected it in a wedge shape in advance. However, we did not resect them until closure of the OOM, after which redundant soft tissue could be pushed up to overcorrect the nostril sill height. The height of the nostril sill could be effectively augmented by transferring the lateral lip skin flap upward. This also results in higher alar base, which improves alar base symmetry (Figure 5a, 5b-2).
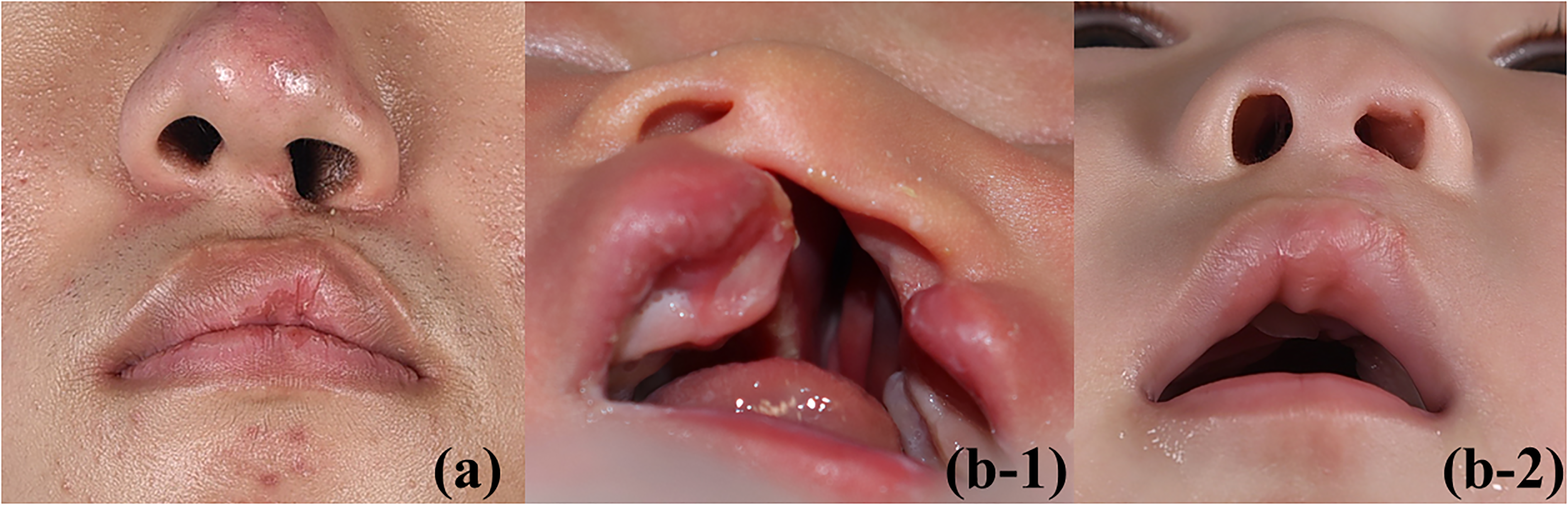
Comparison of the nostril sill height in conventional method (a) and authors’ method (b-1, b-2). The nostril sill of the cleft side has a tendency to collapse over time (a). By recruiting the soft tissue of the lateral segment of the lip upwards, height of the nostril sill(NSH) is well augmented, even overcorrected, to gain sustainability (b-2).
Overcorrection of NSH with soft tissue at the timing of lip repair can minimize structural distortion of nose. Furthermore, the M flap is a large and robust flap, which has a sufficiently broad base and includes the area of C flap in the Millard's technique. Therefore we can reconstruct nasal floor in a more stable manner using this abundant M flap. In terms of functional reconstruction, stable nasal floor prevents narrow nostril and alveolar fistula. 10 While scar placement and aesthetic outcomes are emphasized while discussing Fisher's method, this is an undervalued strength that improves functional outcome.
Conclusion
Repair of complete cleft lip is a procedure of great importance for patient's well-being and positive self-image. As Millard's rotation advancement technique has undergone numerous modifications, Fisher's anatomical subunit approximation technique has much potency to produce better results with refinements.
Strategically applied Fisher's technique demonstrated satisfactory results regarding symmetry of upper lip and philtral length in cleft and non cleft sides.
Limitation of Fisher's technique is observed in case of a severe complete cleft with a difference of philtral height length ≥ 3 mm. Transferring multiple triangular flaps or single large sized triangular flap should be considered to overcome this drawback; when severe cleft is encountered, fabricating multiple flaps or switching the surgical technique can be considered an optimal strategy.
Minimal markings without determining the size of triangular flap or wedge excision of skin on the lateral lip would result in shorter operation time and satisfactory outcomes. In addition to its well-known advantage of favorable scar placement, its potential to enable nostril sill augmentation and ability to provide sufficient tissue by M flap for coverage of inner lining could play a key role in improving surgical results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board of Samsung Medical Center (IRB file no.: 2022-05-035). All patients provided informed consent for the operative procedures and postoperative managements.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.