
Abstract
Goldenhar syndrome (GS) is a rare congenital disorder characterized by multiple facial anomalies. This case report describes a GS presenting with bilateral cleft lip and palate and bilateral transverse facial cleft. We performed a single-stage surgery to repair the bilateral cleft lip and bilateral transverse facial cleft when the patient was 4-months-old. Bilateral cleft lip repair using the Mulliken method was performed first, and then the bilateral transverse facial cleft was corrected. Orbicularis oris muscle repair was done at each clefts. Anatomical approximation technique was used and the final oral commissure was determined considering symmetry. Satisfactory outcomes were achieved without complications.
Goldenhar syndrome is a rare congenital disorder first described by Goldenhar in the 1950s and may involve multiple facial deformities in the eyes, ears, mandible, facial nerves, lips, and palate. Previous studies have reported the occurrence of this syndrome in 1:45,000 to 1:3500 live births. 1 It is clinically diagnosed based on the characteristic phenotypes, and various phenotypes with a wide range of severities can be observed.2,3 Orofacial clefts have been reported to account for 40% of the cases of Goldenhar syndrome.4,5
The occurrence of both of the cleft lip and transverse facial cleft in a patient is very rare, and only a few cases have been reported in the literature.6–8 Moreover, most clefts are unilateral, and double-bilateral forms have not been reported yet. Herein, we describe a case of a double-bilateral facial cleft in Goldenhar syndrome, which represents both bilateral cleft lip and bilateral transverse facial cleft.
For a synchronous occurrence of two different types of clefts, a staged surgery might be more advantageous than a single-stage surgery restoring the normal anatomy. For example, if the cleft lip is repaired in the first stage, the restored anatomical landmark can provide a reference for determining the position of the new oral commissure in the next stage. However, when both clefts are bilateral, the partially restored anatomy may not significantly contribute to the second-stage surgery. Moreover, a single-stage surgery would be beneficial to the patient because it could reduce anesthesia-related complication risks by avoiding general anesthesia. In this case, we successfully repaired the bilateral cleft lip and bilateral transverse facial cleft by performing a single-stage surgery with good outcomes.
Clinical Report
A female newborn was referred to the Department of Plastic Surgery because of a bilateral cleft lip and palate and bilateral transverse facial cleft. The patient was delivered via normal spontaneous delivery at 40 weeks of gestational age with a birth weight of 3.050 g (25−50th percentile) and length 49 cm (25−50th percentile). There were no untoward events during delivery. The patient was delivered following the first pregnancy, and prenatal history revealed no maternal risk factors. The parents were not related by blood and no family history of congenital malformations.
During the initial physical examination, bilateral complete cleft lip and palate, bilateral transverse facial cleft, multiple pre-auricular skin tags, epibulbar dermoids in both eyes, and mandibular hypoplasia were identified. The patient required full gavage feeding due to poor sucking and persistent oropharyngeal regurgitation. No respiratory difficulty was noted. The transverse facial clefts on both lateral sides were symmetric and mild in form, and did not involve the masseter muscles. 9 Because of the clefts, disruption of the orbicularis oris muscle was observed at four points around the mouth as follows: the bilateral philtral ridges and bilateral oral angles (Figure 1).

Preoperative photograph of 4 months after birth.
When the patient was 4-months-old, repair of the bilateral cleft lip and bilateral transverse facial cleft and excision of the facial skin tags were performed in a single-stage surgery. Bilateral cleft lip repair was first performed using the Mulliken method. 10 Subsequently, an incision line for bilateral transverse facial cleft repair was designed. Two distinct points of the upper and lower lips were identified on each lateral side and tattooed. These points indicated a distinctive border between the normal lip and its abnormal lateral extension lining the cleft. Several authors have previously described this point. 11–13 We created these points for the new oral commissure and linearly transected them by full-thickness, including the pars marginalis. An incision was made along the vermilion border around the cleft to manage the abnormal linin of clefts. Laterally, the upper and lower incision lines finally converged into a sharp angle minimizing the dog-ear (Figure 2). The vermilion turnover flap was elevated and flipped intraorally. The upper and lower flaps were sutured together and made into the oral mucosa. The disoriented orbicular oris muscles were then identified and dissected. Muscle reorientation was performed only in the cleft area to ensure the continuity of the circular shape, and no additional muscle dissection was performed. At the newly confirmed oral angle, the vermilion was sutured to align it with the vermilion borders after approximating the pars marginalis. 13 The skin was closed in a straight line. Finally, the seven skin tags were excised. Both the bilateral cleft lip and bilateral transverse facial cleft were successfully repaired in a single-stage surgery, resulting in satisfactory outcomes. Follow-up examination 2 months postoperatively demonstrated a symmetric oral commissure, and the shape was naturally maintained (Figure 3). The patient had no additional sucking problems.
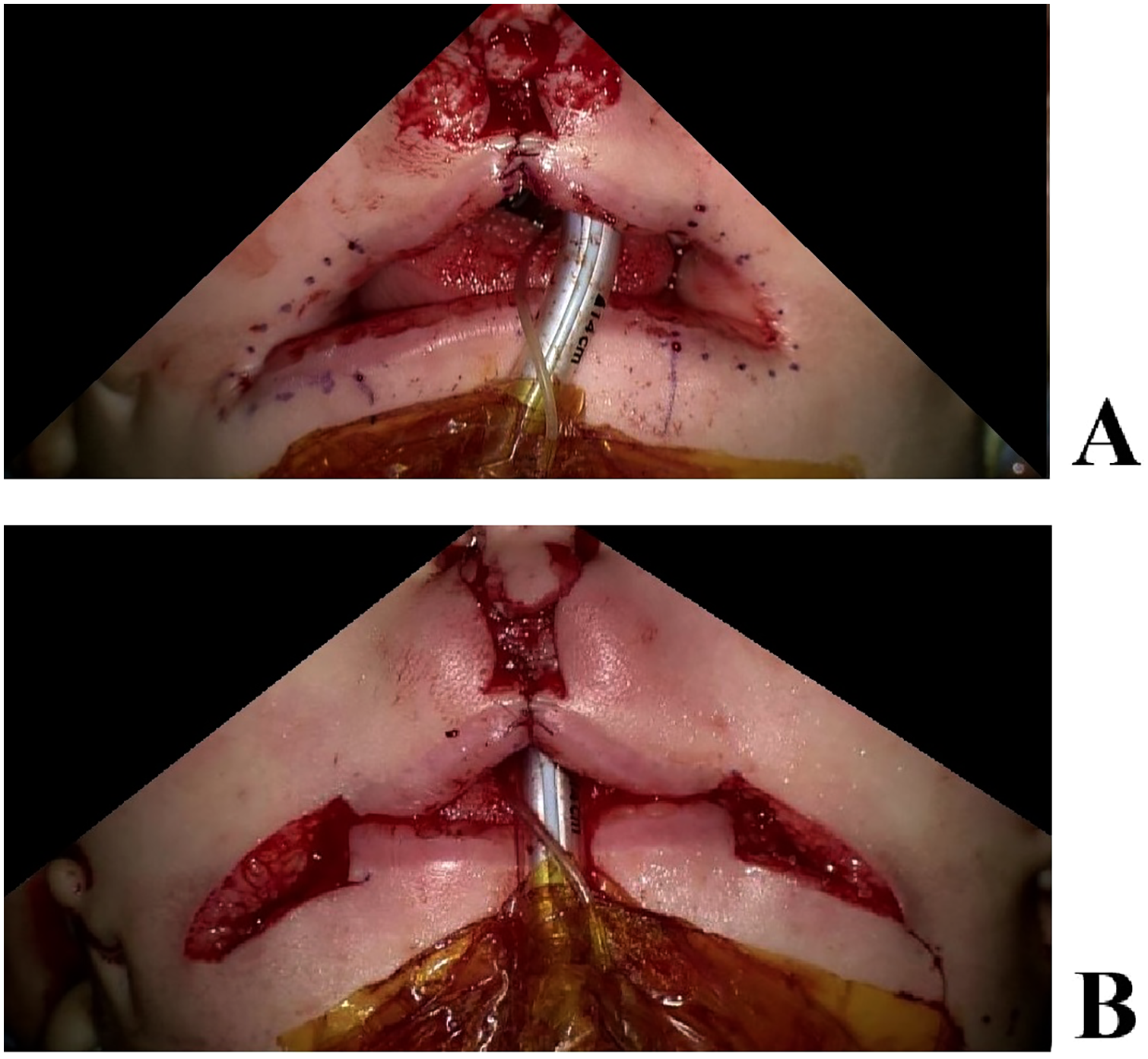
Intraoperative markings for lateral clefts. (A) After lateral cleft excision. (B).

Postoperative photograph of 2 months after repairing bilateral cleft lip and bilateral facial cleft. (A) Frontal view. (B) Worm's eye view.
Discussion
Orofacial clefts are common in patients with Goldenhar syndrome, although cleft lip and transverse facial cleft occurring synchronously are rare. Moreover, these clefts are commonly unilateral, and bilateral involvement is uncommon. Goldenhar syndrome presenting with both unilateral cleft lip and unilateral transverse cleft has been reported by Park et al. and Lee et al.6,7
Herein, we describe a rare case of Goldenhar syndrome presenting with double-bilateral clefts; bilateral complete cleft lip and bilateral transverse facial cleft. The transverse facial cleft, also called Tessier number 7 cleft or macrostomia, presents with a wide range of severity from a simple commissural defect to a complete cleft involving the masseter muscle and facial bone. In the present case, the transverse cleft was mild, did not reach the medial border of the masseteric muscle, and symmetrically affected the right and left oral commissure. 9 In addition to the double-bilateral orofacial clefts, the patient also presented with multiple facial skin tags, epibulbar dermoids on both eyes, and mandibular hypoplasia, which all fulfill the criteria of the Goldenhar syndrome. Upon general examination, hearing loss was detected and no other abnormalities were identified.
Because the patient suffered from feeding problem due to the orofacial clefts, the goal of the first surgery was cleft repair. However, the timing of repairing the two different types of clefts is debatable. If the cleft lip is unilateral, a staged surgery might be advantageous because the preceding cleft lip repair restores the normal anatomy, which could be a reference for the second surgery, especially when determining the new oral commissure. For example, the reconstructed philtrum is an important anatomical landmark permitting the measurement of the philtrum-commissure distance on the noncleft side. However, in the double-bilateral case presented here, a staged surgery might not be advantageous because such an anthropometric method is not feasible for bilateral transverse facial clefts.
Because positioning the new oral commissure is critical and challenging, several methods have been developed. Measuring the distances between landmarks in the noncleft site is applicable when the cleft is unilateral. Using non-lip structures, such as nasal alars or pupils as anthropometric landmarks has been proposed.14–16 Referring to the average lip length of the same age could be considered, although individual differences could not be ignored. 17 A distinctive border between the normal lip and abnormal lining of the cleft can be observed at the lateral cleft site, and several authors have described the characteristic appearance. Tse et al. created this point with the new oral commissure and introduced an anatomical approximation technique. 13 Ueno et al. applied the same technique on patients with bilateral transverse facial cleft. 18
In lateral cleft correction, some authors have advocated using Z-plasty for cheek skin closure for several reasons. Z-plasty might minimize lateral migration of neocommissure by distributing scar contractile force. Central limb of the Z on melolabial fold could be camouflaged to look like nature skin fold.11,19 In senior author's experience, however, lateral migration was nearly undetectable after straight-line closure in long-term follow-up more than 2 years. Since the most of the patients who undergo cleft surgery are very young, melolabial fold is often hard to be found. This makes it difficult to position the central limb of Z precisely on the natural skin fold. Z out of the natural fold may produce aesthetically inferior outcome than linear scar. Even if the Z is well-positioned, two separated scars still remain. Some authors have assisted the utility of Z-plasty in reducing scar length. 20 It was not applicable to this patient because there was no skin redundancy or length mismatch. For the above mentioned reasons, we used straight-line technique for cheek skin closure.
We repaired both types of clefts in a single-stage surgery. In our surgical procedure, the cleft lip was first repaired, followed by transverse facial cleft correction as bilateral cleft lip repair is a more complex procedure than lateral facial cleft repair. The anatomy of the nose, philtrum, and peak of the Cupid's bow was restored through delicate manipulation using the Mulliken method. 10 The next step was positioning the new oral commissure in both lateral sides. Since the midline of the upper lip was defined through the preceding cleft lip repair, the symmetry of the new oral commissure could be easily achieved. We marked the abovementioned border between the normal lip and the lateral clefts, and the final oral commissure was determined considering symmetry.
Especially in patients with a syndromic case, minimizing the number of general anesthesia sessions would be necessary because associated anomalies such as mandibular hypoplasia or other conditions may increase the risks of anesthesia-related complications. In the present case, double-bilateral clefts were successfully repaired in a single-stage surgery, and the outcomes were satisfactory. The patient benefited from a reduced risk of anesthesia-related complications by avoiding general anesthesia. The wounds healed well without any complications, and the 2-month follow-up examination revealed symmetric oral commissure. The patient became possible to suck on a pacifier, but still was difficult to bottle feed due to remaining cleft palate.
Conclusion
In this report, we describe a rare case of a double-bilateral orofacial cleft, that presented with bilateral cleft lip, bilateral transverse facial cleft, and surgical repair. Some surgeons may prefer a staged reconstruction for several reasons. 21 However, in this single-stage procedure, symmetry was achieved without any complications. Thus, the repair of a double-bilateral orofacial cleft can be reliably performed in a single-stage surgery, with reduced anesthesia-related risks. Constant follow-up is needed to assess long-term outcomes.
Footnotes
Acknowledgement:
No acknowledgement
Ethics
This study was performed after approval from the Institutional Review Board (IRB) at Samsung Medical Center. (Approval No. SMC 2022-07-107-001)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.