
Abstract
Background
Progressive hemifacial atrophy often causes lip vermilion defects in patients. In this study, we described a one-stage repair method for lip defects in progressive hemifacial atrophy using a lip vermilion mucosal flap or combined dermal fat flap graft.
Patients and Methods
Patients diagnosed with progressive hemifacial atrophy with lip vermilion defects from 2010 to 2022 were included in this study. Based on the severity and location of the patient's lip defect, a lip vermilion mucosal flap was designed and transferred to the lip defect or combined with a hip dermal fat flap for one-stage repair of the lip morphology. Lip morphology and function of patients were followed up after surgery.
Results
A total of 22 patients were enrolled in this study, including 15 patients with lip defects on the upper lip alone and 7 patients with both upper and lower lip defects. Follow-up six months to two years postoperatively, all patients recovered uneventfully without complications. The repaired lips of the patient had a full and symmetrical morphology with no visible scarring. Two patients experienced transient dysesthesia of the lips postoperatively and both returned to normal after three months. All patients had good lip closure with normal dietary and speech function.
Conclusions
The method we described for repairing lip defects in progressive hemifacial atrophy can achieve satisfactory aesthetic and functional lip results. The distinct advantage of this approach is that the patients undergo only one-stage operation and it can be used to repair both upper and lower lip defects.
Introduction
Progressive hemifacial atrophy (PHA) is a rare acquired disease characterized by unilateral progressive atrophy of the facial skin, subcutaneous tissue, muscles, and even bones. PHA has a wide range of lesions and can involve ocular, periocular tissues, nasal ala, lip vermilion, and oral tissues. 1 PHA can cause facial deformities in patients, which seriously affects their mental health and quality of life. Autologous fat grafting, 2 various tissue flap transplantation, 3 bone grafting, 4 or orthognathic surgery 5 are commonly used to reconstruct atrophied facial soft tissues or bones to improve facial deformities. The lip is a commonly involved tissue in patients with PHA, presenting as thinning and defects in the involved lip vermilion with exposed teeth. Both the upper and lower lip of the affected side can be involved. Therefore, the repair of lip vermilion defects is an important part of comprehensive PHA treatment. In this study, we applied a new method of lip vermilion mucosal flap or combined dermal fat flap for one-stage repair of lip defects in patients with PHA.
Patients and Methods
This study enrolled patients diagnosed with PHA combined with lip vermilion defects who visited the Craniomaxillofacial Centre of the Plastic Surgery Hospital, Chinese Academy of Medical Sciences from January 2010 to December 2022. The study was approved by the Ethics Review Committee of Plastic Surgery Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College (Beijing, China). Written informed consent was obtained from all participants.
The operations were performed under local or general anesthesia. The surgical incision was first designed. At the junction of the wet and dry lip vermilion, a transverse incision was designed from the lateral side towards the center of the lip vermilion defect. Then, longitudinal incisions were designed towards the oral side of the lip and a mucosal flap was created based on the extent of the lip vermilion defect. The mucosa was incised along the designed transverse incision to the submucosa and sufficiently released as a recipient bed for the mucosal flap transfer. Along the longitudinal incision lines, the mucosa was incised to the orbicularis oris, and then the mucosal flap was lifted along the orbicularis oris muscle. The prepared mucosal flap was then transferred to the area of the lip vermilion defect. The mucosal flap was properly trimmed, and the incision was closed in one stage after the lip vermilion shape was repaired satisfactorily.
In patients with severe lip vermilion defects, a dermal fat flap was harvested from the patient's hip. The skin was incised to the subcutaneous fat along the preoperative design line in the upper end of the natal cleft, and the composite tissue mass was completely excised. Then the epidermal layer of the composite tissue block was removed and trimmed into a composite dermal fat flap. The dermal fat flap was filled into the lip vermilion defect area to increase the volume of tissue, and then the mucosal flap was covered over it. The surgical procedures are shown in Figure 1.

The surgical procedure for repair of upper lip defects. A: Pre-operative frontal view of a patient with PHA combined with defective deformity of the right upper lip. B: The design of the incision intraoperatively. C: A dermal fat flap was harvested from the hip. D: The hip dermal fat flap (marked with asterisks) was filled into the lip defect area, and then covered with the prepared lip mucosa flap (marked with a black arrowhead). E: The lip mucosal flap was transferred to the defect site and the incisions were closed. F: Post-operative 2-day frontal view. G: Post-operative one-year frontal view.
The morphology and function of the lip were assessed postoperatively, including fullness, symmetry, scarring, lip sensation, mouth opening, etc.
Results
A total of 22 patients with PHA were included in this study, including 7 males and 15 females. The age of the patients was 17–24 years, with a mean age of 21 years. There were 15 patients with obvious defects on the upper-lip vermilion only, and 7 patients with defects on both the upper and lower red lips. Sixteen patients underwent lip vermilion mucosal flap grafting and six patients received combined dermal fat flap and mucosal flap grafting. The follow-up period of patients postoperatively ranged from 6 months to 2 years, with a mean follow-up time of 13 months.
There were no postoperative complications such as hematoma, infection, or necrosis of the mucosal flap in any of the patients. In terms of lip morphology, lip vermilion defects were significantly improved in all patients, with full lip shape and good symmetry. No significant scarring was seen on any of the patient's lips. In terms of function, two patients experienced postoperative hypoesthesia in the lips, but both returned to normal three months after surgery. All patients had good lip closure with normal dietary and language function postoperatively. There was no limited mouth opening or salivation in all patients.
Clinical Report
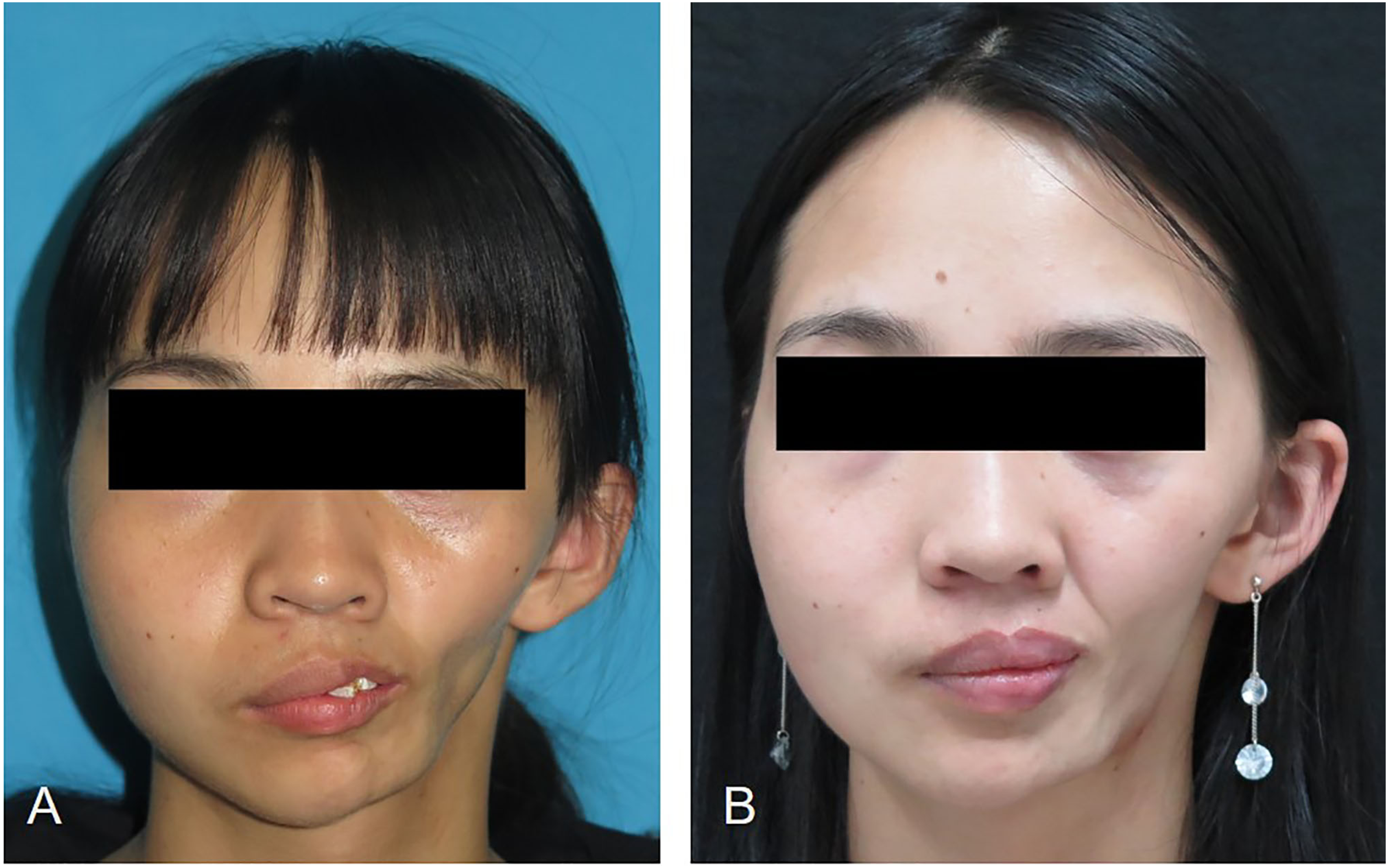
Pre-operative (A) and post-operative one-year (B) frontal view photograph.
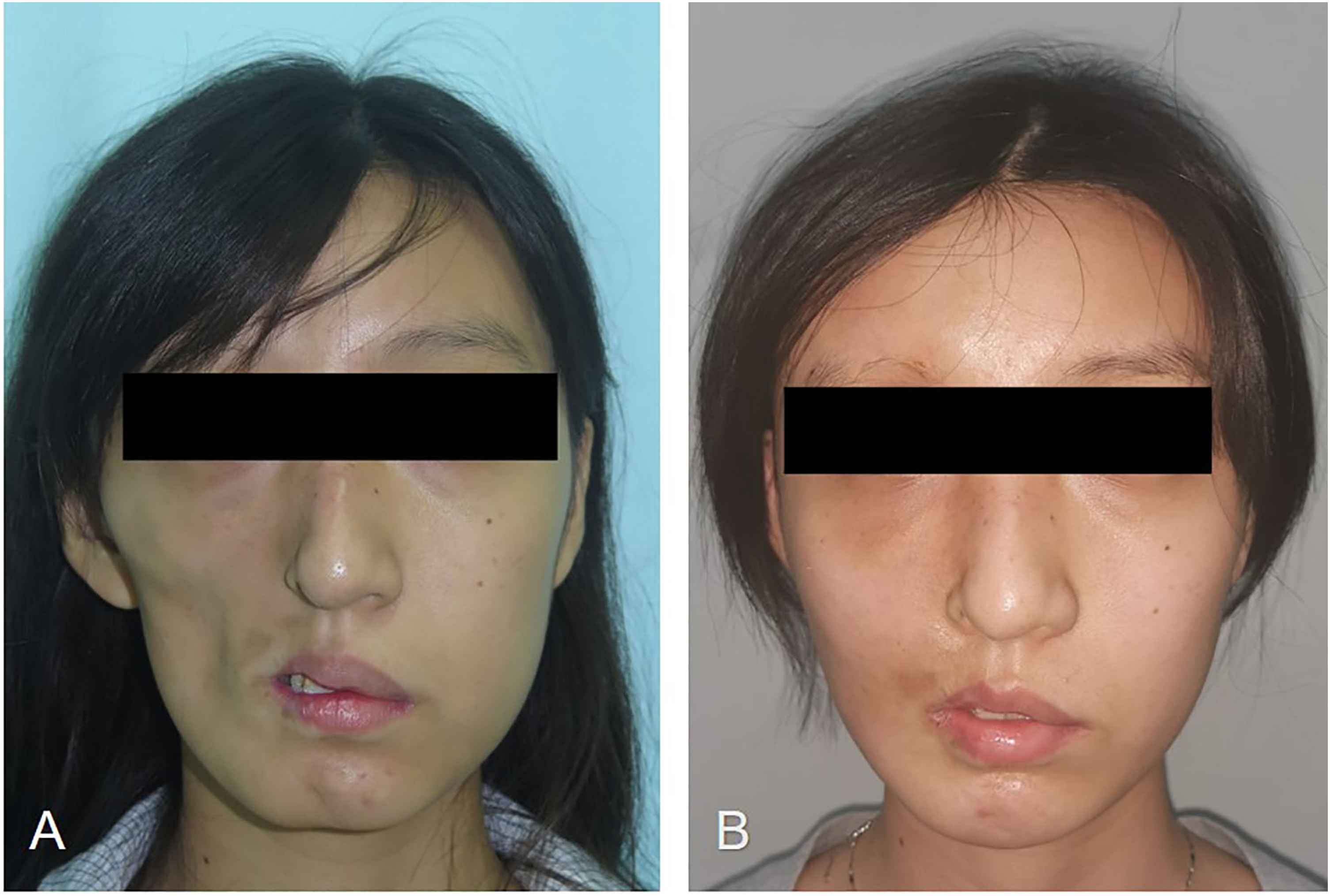
Pre-operative (A) and post-operative 8-month (B) frontal view photograph.
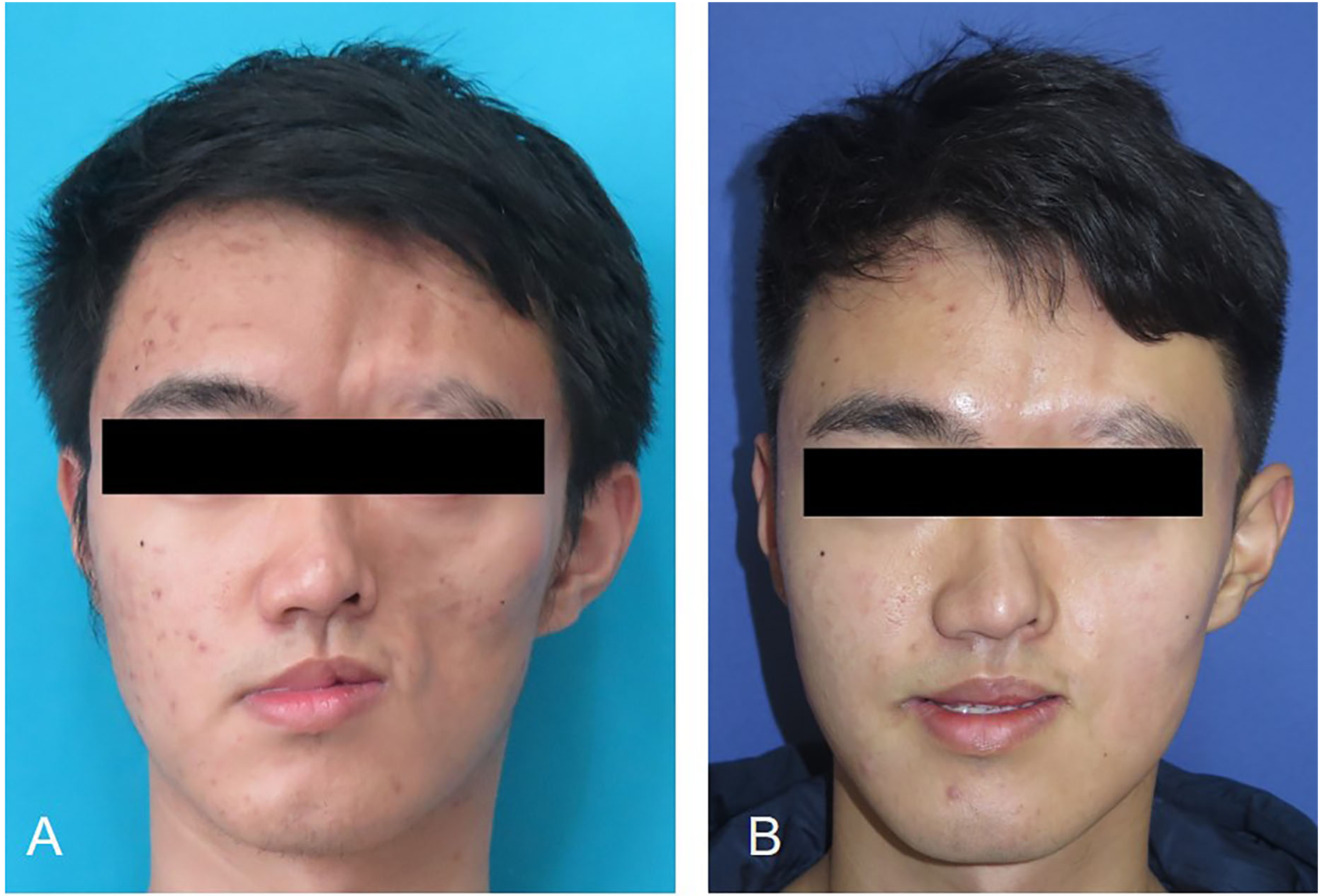
Pre-operative (A) and post-operative 14-month (B) frontal view photograph.
Discussion
Progressive hemifacial atrophy, also known as Parry-Romberg syndrome (PRS), was first reported by Parry in 1825 and described in detail by Romberg in 1846. 6 PHA tends to develop before the age of 20 years in patients and progresses slowly for 2–10 years before entering a stable phase, with a high prevalence in females.7,8 PHA usually involves the facial skin to the bones accompanied by deformities of the ocular, nasal, and oral lips. Lip deformity in patients with PHA has unique clinical features, characterized by atrophy and thinning of the affected side of the oral lips, with localized defects of the lip vermilion. The localized defect in the lip vermilion prevents the lips from closing completely, leaving a hole between the upper and lower lip with exposed teeth. This can seriously affect the patient's facial form and cause drooling. Therefore, reconstruction of lip vermilion defects is essential but a great challenge in patients with PHA combined with lip defect deformity.
In the past few decades, scholars have explored methods of repairing lip defects in patients with PHA. Rees et al. 9 used the tongue flap to reconstruct lip vermilion defects in eleven patients with PHA. This method achieved good postoperative results with adequate correction of the patient's lip contour and few complications. However, the tongue of the patient needed to be immobilization for 10 days to two weeks and the pedicle was cut off two weeks in a second stage of surgery two weeks later. The immobilization of the tongue can cause discomfort for the patient as well as eating and speech disorders. In addition, there was a color difference between the transplanted tongue tissue and the normal lip vermilion, which could be camouflaged by lipstick in female patients, but was noticeable in male patients. In the comprehensive reconstruction of bone and soft tissues in patients with severe PHA, Hu et al. used a lower lip cross-lip flap to repair red lip defects in patients. 10 The lower lip cross-lip vermilion flap was first described by Kawamoto et al. in 1979. 11 This lip flap filled the upper lip defect while reducing the thickness of the lower lip for a better balance between the upper and lower lips. The pedicle of the flap was located in the center of the lower lip and required oro-labial immobilization before performing a second-stage surgical cutting of the pedicle, which would affect the daily diet and speech functions of the patients.
Jin et al. 12 repaired upper lip vermilion defects of patients with PHA using a modified crossed-lip vermilion flap of the lower lip with the pedicle located at the affected side of the oral corner. This method required no oro-labial immobilization and could effectively preserve the eating and speech function of the patients. However, this reconstruction procedure still needed a second stage of operation to devide the pedicle and did not apply to patients with both upper and lower lip defects. Yang et al. 13 reported a technique for one-stage repair of upper-lip defects in PHA by use of a lower-lip axial composite tissue flap. No second-stage surgical procedure was required to cut off the pedicle, but this method also cannot reconstruct the upper and lower lip defects simultaneously.
Various current methods for the reconstruction of lip vermilion defects in patients with PHA have their advantages and disadvantages. The primary shortcomings of the above-mentioned repair modalities are that most of them need two-stage surgery and cannot repair both upper and lower lip defects simultaneously. In this study, we described a procedure that enabled the one-stage repair of lip vermilion defects in PHA and was applicable to patients with simultaneous upper and lower lip defects. We repaired lip vermilion defects by transferring a lip mucosa flap on the affected oral side. It is worth noting that in patients with severe lip involvement, lip mucosal flap transfer alone cannot obtain good lip morphology due to significant lip atrophy and thinning. For such patients, we increased the amount of lip tissue with a hip dermal fat flap graft. The incision of the dermal fat flap was small and hidden which was not easy to be detected. In the present study, all patients showed remarkable improvement in lip vermilion defects without complications. In addition, the patients had normal oro-labial functions such as eating and speech postoperatively. This suggested that this method could be effective in repairing lip vermilion defect deformities in patients with PHA.
Conclusion
In conclusion, the lip vermilion mucosal flap graft or combined dermal fat flap graft that we used for one-stage repair of lip defect deformity in patients with PHA is an effective technique. This reconstruction method can achieve a satisfactory lip morphology and is easy to perform with few postoperative complications. The obvious strength of this method is that it does not need lower lip tissue to repair upper lip defects, and therefore can be applied to patients with both upper and lower lip defects. Furthermore, the patients underwent only one stage of surgery and without oro-labial immobilization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Special Research Fund for Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, CAMS Innovation Fund for Medical Sciences, (grant number YS202033, 2021-I2M-1-068).