
Abstract
Background
Children born with Trisomy 13 or 18 (T13/18) often have multiple congenital anomalies, many of which drastically shorten their lifespan. Among these defects are cleft lip and palate, the repair of which presents an ethical dilemma to the surgeon given the underlying comorbidities associated with T13/18. The authors present an ethical discussion and institutional experience in navigating this dilemma.
Methods
The authors analyzed existing literature on T13 and T18 surgery and mortality. A retrospective study over ten years was also conducted to identify pediatric patients who underwent surgical correction of cleft lip and/or palate secondary to a confirmed diagnosis of T13/18. The authors identified two patients and examined their treatment course.
Results
The authors’ review of literature coupled with their institution's experience builds on the published successes of correcting cleft lip and palate in the setting of T13/18. It was found that both patients identified in the case series underwent successful correction with no surgical complications.
Conclusion
A careful balance must be struck between improved quality of life, benefits of treatment, and risks of surgery in children with T13/T18. Careful consideration should be given to the medical status of these complex patients. If the remaining medical comorbidities are well managed and under control, there is an ethical precedent for performing cleft lip and palate surgeries on these children. A diagnosis of T13/T18 alone is not enough to disqualify patients from cleft lip/palate surgery.
Introduction
Trisomy 13 (T13) and Trisomy 18 (T18) are chromosomal aneuploidies that present with mental disability and multiple congenital anomalies. Both syndromes are associated with cardiac defects and cleft lip and palate. Further, both T13 and T18 have a low survival rate: children with either syndrome have a one-year survival rate of 5-12%.1–4 However, with an ongoing shift away from the perspective that T13/T18 is incompatible with life, 5 caregivers of patients with T13 or T18 sometimes wish to explore reconstructive surgery options for their children with cleft lip and/or palate. This situation presents an ethical dilemma for the surgeon. Is such a surgery justified given the increased risk of surgical mortality from cardiac and other comorbidities? Further, is the considerable trouble that the surgery puts the patient and family through justified given the short lifespan of T13 and T18 patients? 6 What factors should be considered when weighing this decision? The authors analyze these questions by presenting and discussing ethical appeals for both sides of the argument. Our institution's own experience with this issue is also discussed.
Presentation of Ethical Appeals
Arguments Against Surgery
The primary concern associated with performing surgery on patients with T13 and T18 is that the surgery may be dangerous given their comorbidities. Cardiac comorbidities, in particular, are concerning given that these patients are at particular risk of cardiovascular compromise from intravenous and inhalational anesthetics. 7 The principle of nonmaleficence requires physicians to avoid harming the patient and, by extension, to avoid procedures that are inappropriately burdensome. 8 As such, this principle supports avoiding elective surgery in patients with T13 and T18.
Further, a medical procedure is considered “futile” if a desired outcome is overwhelmingly improbable.9,10 The limited lifespan for infants with Trisomy 13 and Trisomy 18 has historically been used as justification for limiting lifesaving treatments, including surgery. 11 This concept may also apply to cleft lip/palate repair since these patients may not live long enough past the postoperative period to benefit.
Arguments in Favor of Surgery
The principles of beneficence, justice, and autonomy support the choice of performing reconstructive surgery. Beneficence requires physicians to act in the benefit of the patient and promote their welfare. 8 Although patients with T13 and T18 often have limited oral feeding ability, over half of these patients are able to take some amount of food orally.12,13 Cleft lip and palate repair therefore provides functional improvement to T13 and T18 patients. Furthermore, early intervention for cleft lip and palate has been shown to positively influence the caregiver-child relationship in children without T13/T18. 14 Justice demands that children with T13/T18 deserve the allocation of resources to receive these same benefits.
Additionally, the ethical principle of autonomy demands that the wishes of patients and their caregivers be respected. While the safety of the procedure with all risks and benefits must be carefully weighed for each case, this principle reminds that the wishes of caregivers of children with T13 and T18 requesting surgery be weighed very seriously.
Discussion
The central issue in this discussion is therefore whether the benefits of surgery (principles of beneficence and autonomy) are outweighed by risk of harm (principle of nonmaleficence) or possible futility. It is the position of the authors that patients with T13 and T18 should not be denied surgery due to their diagnosis alone.
Nonmaleficence
The major concern in patients with T13/T18 is that they have elevated surgical risk due to their comorbidities, and that nonmaleficence requires not exposing these children to that risk. However, there is a growing body of evidence that T13 and T18 patients can often tolerate surgery and that intensive medical management with surgery may actually extend life. 15 In a retrospective review, Kosho et al. assessed outcomes in Japanese patients with T18. While T18 is classified in Japan as a condition for which only ongoing life-supporting treatments are considered, many hospitals have decided to perform more intensive procedures. The authors noted that patients with T18 who received intensive surgical treatment for comorbidities, such as esophageal repair and gastrostomy, generally demonstrated improved survival. 11 Similar findings were published more recently by Nishi et al. who found no intraoperative death or anesthetic complications in 24 patients with T18 receiving either palliative or radical surgery. Follow-up analysis found a higher survival rate in those receiving radical surgery. 16 It is important to note that many of the surgical patients described in these papers had various congenital cardiovascular defects including ventricular septal defect, coarctation of the aorta, mitral valve stenosis, and double outlet right ventricle.
There have also been papers specifically describing cleft lip and palate surgeries in this patient population. In 2015, Akamatsu et al. published a report of a 31-month-old girl with T13 who presented for cleft lip and palate repair. This patient had complete bilateral cleft lip and palate, hypoplasia of the nose, aplasia of the columella, a short prolabium, and a small floating premaxilla. The operation was completed successfully without large fluctuations in the patient's vital signs; her postoperative course was uncomplicated. 17 The authors note that they made efforts to reduce the length of the operation as per the request of their pediatrician colleagues. The surgery was completed in one hour and twenty-one minutes by omitting precision gauge measurements for intraoperative design, performing the surgery with intradermal suture and minimal skin sutures, and omitting the prolabium skin flap when circulation of the prolabium was insufficient.
Similarly, Pollard and Beasley reported two cases of children with T13 who received cleft lip and palate surgery. In the first case of an 8-month-old boy, the procedure was abandoned when oxygen saturations dropped to 75% during inhalation induction. His recovery from anesthesia was slow, and he experienced a few episodes of respiratory obstruction in the recovery room. Sadly, he died at 12 months of age, likely from a combination of cardiomyopathy and pneumonia. In contrast, the second patient was a 9-month-old girl whose procedure proceeded successfully with an uneventful postoperative course. 18 Finally, in 2017 Kamal et al. reported a further case of a successful cleft lip and palate repair in a 10-month-old child with T13. The authors noted that anesthesia induction was difficult in this case due to neck stiffness of the child; however, the procedure was completed in a timely manner due to careful preoperative planning. 7
Our hospital has similarly had experience with cleft lip and palate surgery in patients with T13. After obtaining Institutional Review Board approval, we performed a retrospective chart review of all patients at our institution who underwent surgical correction of cleft lip and/or palate secondary to T13 or T18 from 2012 to 2022. Of the six patients diagnosed with T13 or T18 in our database, only two patients with T13 had received surgical intervention. In the cases of the patients who did not receive surgery, justification was that the patient could not open their mouth wide enough for surgery or that patients were nonverbal and did not eat by mouth. The institutional ethics committee was not consulted as these justifications were deemed sufficient to decline surgery and because there was no disagreement between providers and caregivers.
The first patient was a seven-year-old male who presented to our clinic for repair of a bilateral cleft lip and palate. The patient's medical history was significant for T13, an atrial septal defect, and restrictive airway disease. Given the patient's comorbidities, he was seen in our pediatric anesthesia screening service (PASS) clinic where he received operative clearance. Cardiology requested he be kept in a euvolemic state to avoid any fluid overload. Primary repair of the lip was performed in the standard fashion. The operation was unremarkable: the patient remained hemodynamically and respiratorily stable, with a total operative time of 4 h and 33 min and a total anesthesia time of 5 h and 18 min. Postoperatively, a nasopharyngeal airway device was inserted into the right nostril in place of a stent to ensure unobstructed flow through the nasal cannula. The patient's postoperative course was uncomplicated, and he was discharged home on postoperative day (POD) 3. Additionally, the 90-day postoperative period was unremarkable for any complications including intolerance of anesthesia, scarring, or wound dehiscence.
The second patient was a 2-year-old female with confirmed diagnoses of T13, holoprosencephaly, diabetes insipidus, and a ventral septal defect who presented to our clinic for primary repair of a partial midline cleft lip and palate. Intraoperatively it was determined that the premaxilla was untethered to any vomerine stem and was not large enough to support any bone grafting. For this reason, it was subsequently excised and the premaxilla and prolabium were released to facilitate the lip repair. The patient remained hemodynamically and respiratorily stable with a total operative time of 2 h and 51 min and with a total anesthesia time of 4 h and 2 min. Due to the patient's high risk for perioperative respiratory distress, she was sent to the progressive care unit (PRCU) for a higher level of monitoring. On POD 1 the patient developed hypernatremia due to an electrolyte/fluid disorder which was corrected by the endocrine care team, likely related to the patient's diabetes insipidus. Of note, on POD 1, the prolabium was noted to have a congested appearance, which was resolved after the removal of several surrounding sutures and the nasal stent. On POD 2 the patient became febrile with a maximum temperature of 101.5 F which was resolved with Tylenol per os (PO). On the morning of POD 3 the patient became acutely febrile again, without a source of surgical infection, with a maximum temperature of 104 F which was resolved with Tylenol PO. The patient was discharged home on POD 4. The remaining 90-day postoperative period was unremarkable for complications such as poor scarring or wound dehiscence. Eight months later, the patient underwent palatoplasty without complication. The total operative time was 1 h and 12 min with an anesthesia time of 1 h and 31 min. The patient was discharged from the hospital on POD 4 and the ninety-day postoperative period was unremarkable for any complications. This patient has been seen at nine-year follow up and is doing well. She is feeding orally, pulling up to stand and walking with support. She receives speech therapy, occupational therapy, physical therapy, and vision therapy twice a week and is home-schooled. Our institution's experience thus builds on these published successes, with both patients identified in our case series receiving successful surgeries with no complications.
These case reports so far have discussed cleft palate and lip repairs on patients with T13. There is also a precedent for performing these surgeries on patients with T18. In 2015 Karimnejad et al. published a retrospective cohort analysis that provides further context to cleft lip/palate surgeries for both trisomies 18 and 13. The authors reviewed the databank of the Support Organization for Trisomy 18, 13, and related disorders (SOFT). SOFT maintains a surgery registry with information on surgical procedures performed on this population. Records were specifically reviewed for otolaryngologic cases, in which the authors included cleft lip/palate repair. The authors found that, of 1380 procedures performed on children with T13 or 18, 231 (16.7%) were otolaryngologic. 19 Indeed, cleft lip repair was the second most common otolaryngologic procedure performed, with 40 cleft lip and 30 cleft palate repairs being performed that year. Of note, cleft lip and palate repair was more commonly performed in patients with T13, which is consistent with these defects being more common in T13 than T18. 19 Our own review of the SOFT database further revealed that other plastic surgery procedures such as mandibular distraction and entropion repair have also been performed for these patients.
One feature frequently seen in these reported cases of successful reconstructive surgery is the lack of significant cardiac defects in any of these patients. Identification of a relatively healthy heart may thus be a soft prerequisite for cleft lip and palate repair in T13/T18 patients, especially given the risk of cardiovascular compromise from anesthetics. 15 Nevertheless, the presence of cardiac defects is not necessarily an absolute contraindication to surgery in this patient population. Of note, one of the patients reported in our case series received successful and complication-free reconstructive surgery in the setting of an atrial septal defect. Further, as described previously, many of the intensive surgeries performed on this patient population were successfully carried out on patients with such congenital cardiovascular abnormalities. At the same time, the lack of cardiac abnormalities does not preclude poor outcomes and a difficult postoperative course, as evidenced by the first patient in Pollard and Beasley's case report.
Futility
Surgical repair of cleft lip and palate in patients with T13 and T18 could be considered futile since these patients historically have barely lived long enough past the postoperative period to benefit from the procedure. However, while many children may live very short lives, there is a range of phenotypes, and some children become long-term survivors who demonstrate physical and psychosocial maturation. Kosho et al. note several cases of patients who were able to survive past the age of ten years, some of whom were able to walk independently, recognize language, feed fully orally, and, in one case, take care of another child. 12 While the ethical principle of justice asks us to assess relative benefit that various patients can receive from a treatment, these examples clearly demonstrate that a diagnosis of T13/T18 alone does not disqualify a child from benefitting from reconstructive surgery over many years.
Much of this paper has so far focused on the surgeon's point of view in assessing surgical risk when making such ethical decisions. While this is a critical component of the decision-making process, the decision must ultimately be made following the principles of shared decision making with patient caregivers. There are many opportunities for misunderstanding and conflict in these scenarios because they inherently involve value judgments. Caregivers often request maximal treatment even though traditional management recommendations have been focused on palliative care. 20 This discrepancy among parents and providers was further demonstrated by Kosho et al., who found that parents often report that healthcare providers do not see their child as having value despite physical and mental limitations. 12 Most parents have very meaningful interactions with their children with T13/T18 and were positive about caring for their children: Janvier et al. reported that 97% of parents described their children as happy and reported that the children enriched their family life regardless of the length of the child's life. 20 This concept has been echoed by families writing about their experiences with T13/T18. 21 Shared decision making between providers and caregivers is the gold standard of clinical care 22 and is therefore critical in these cases. This decision making process should respect patient autonomy and should follow the “Relational Potential standard” as modified by Wightman et al. 23 While the “best interest standard” is the gold standard for surrogate decision making, a lack of definitive criteria to determine a best interest can lead to a discrepancy between the medical team's perception of the infant's best interest and the rationale underlying the caregiver's request for medical interventions. 23 In such cases, the Relational Potential standard as modified by Wightman et.al. should be used because it assigns moral value to the caring relationship between a caregiver and a child. 23
Moreover, it is important to avoid succumbing to the “disability paradox,” wherein disabled patients receive lesser care due to their disability. Socially, the general public believes that persons with disabilities do not have a high quality of life compared to abled persons. 24 However, Albrecht et.al., note that quality of life is broader than just health-related issues. It goes beyond activities of daily living and disease, involving a more complete social, psychological, and spiritual being. In fact, some persons with disabilities report experiencing a good quality of life seemingly against all odds. 24 This thought process was first addressed in the context of a paradigm shift to life-prolonging treatment for infants with Trisomy 21, wherein the Baby Doe regulations were established to prevent medical neglect following the Hopkins Mongol Case. 25 This concept was later extended in the literature to T13 and T18 with the conclusion that patients with these conditions “are the next Baby Doe(s).” 26
Synthesis
The key questions asked in this article are whether cleft lip and palate surgery is justified in patients with T13/T18 given the increased risk of surgical mortality and, further, whether the considerable trouble that the surgery puts the patient and family through is justified given the historically short lifespan of T13 and T18 patients. We have demonstrated through a review of the literature and representative cases at our institution that surgery can be performed safely in these patients with added precautions such as limiting operative time and maintaining euvolemia.
Further, having provided life-sustaining interventions (e.g., cardiac surgery) to this specific population of infants with Trisomy 13 and Trisomy 18, the issue becomes identifying ethical support for providing life-altering interventions (e.g., cleft palate repair, orthopedic surgeries). The principle of justice provides such ethical justification. An accepted formulation for the principle of justice is that similarly situated individuals are to be treated similarly unless there is a morally compelling reason for dissimilar treatment. We have demonstrated that T13 and T18 alone are not enough of a safety concern to offer dissimilar treatment. Thus, given that infants with other syndromes involving both cardiac anomalies and cleft palate are sequentially offered both the life-sustaining and life-altering interventions, infants with Trisomy 13 and Trisomy 18 are to be similarly treated by offering these surgeries. Put plainly, the diagnosis of Trisomy 13/Trisomy 18 alone is not sufficient to exclude patients from reconstructive surgery. Doing so avoids the disability paradox and respects the relational potential standard.
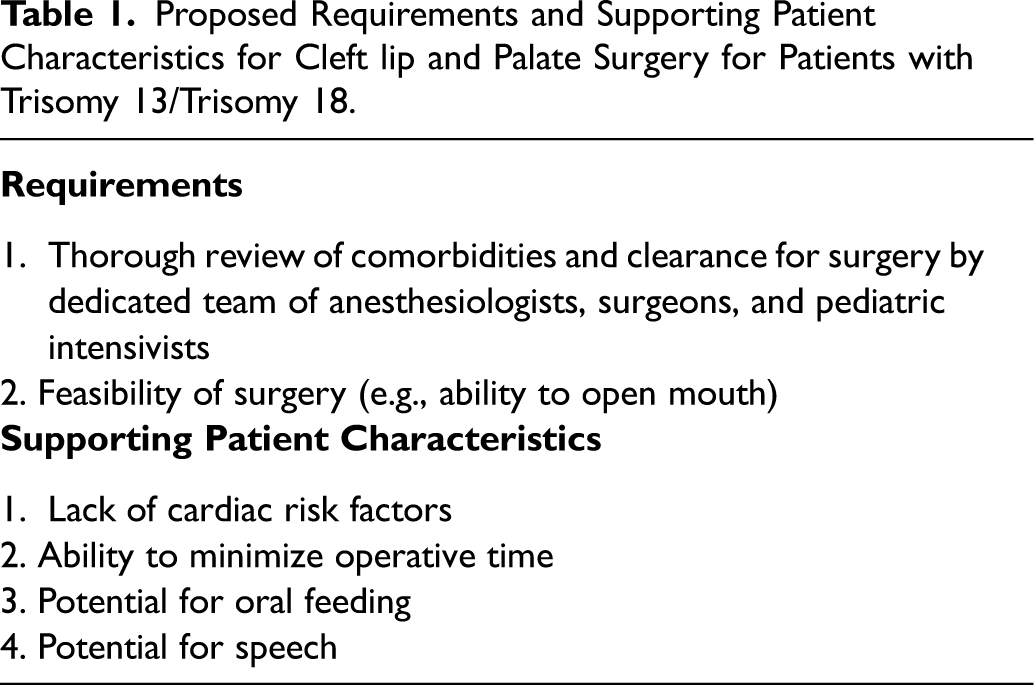
As with all patients, individual risks and benefits of surgery as well as values of the patient's caregivers must be carefully weighed. Shared decision making is to be central in this process, with caregivers working to address their centrally held values. We propose a set of criteria and supporting patient characteristics for justifying cleft lip and palate surgery in these patients. These criteria are detailed in table 1. Our institution has established a Pediatric Anesthesia Screening Service (PASS clinic) to screen patients with health conditions that may increase risk during anesthesia or surgery. We propose that clearance after thorough review of a patient's comorbidities should be a prerequisite for performing surgery in patients with T13/T18. In addition, the procedure must be feasible, with the patient able to open the mouth sufficiently for operative access. Further, while not an absolute contraindication, particular care should be taken when deciding to perform surgery in children with significant cardiac defects. These patients are also likely to benefit from reconstructive plans where operative time can be minimized. Finally, patients who stand to benefit the most from reconstructive surgery are those with the potential for oral feeding and speech.
Proposed Requirements and Supporting Patient Characteristics for Cleft lip and Palate Surgery for Patients with Trisomy 13/Trisomy 18.
Conclusion
A balance must thus be struck between improved quality of life, benefits of treatment, and risks of surgery in children with T13/T18. Careful consideration should be given to the medical status of these complex patients. Level of cardiac function is an important component of this analysis, with published reports of successful cleft lip/palate repairs focusing on children with healthy hearts. Furthermore, careful preoperative planning is instrumental in keeping procedure length short. However, if the remaining medical comorbidities are well managed and under control, there is an ethical precedent for performing cleft lip and palate surgeries on these children. These children may benefit greatly from the surgery, as they already contribute to their family in meaningful ways regardless of their lifespan. The decision to proceed with surgery thus requires careful discussion with caregiver input, but a diagnosis of T13/T18 alone is not sufficient to ethically exclude patients from surgery.