
Abstract
Objective
Evaluate periodontal bone support of maxillary central incisors (MCI) in patients with bilateral complete cleft lip and palate (BCCLP). Determine if syndromic diagnosis, age at time of alveolar bone graft (ABG), presence of maxillary lateral incisor (MLI), history of dentofacial orthopedics, maxillary expansion, and pre-maxillary osteotomy are associated with the periodontal bone support of MCI.
Design
Retrospective radiographic study.
Setting
Tertiary care children's hospital
Patients
One hundred seventy-nine patients with BCCLP (22 syndromic) who had post-operative ABG cone beam computed tomography (CBCT) scans taken between 2002-2018.
Main Outcome Measures:
Crown to root
Results
The C/R ratio in 65% of MCI indicated periodontally compromised teeth. Presence of a MLI improved bone support on adjacent MCI when compared to those missing a MLI (51.4% vs 28.4%, P = .010). There was no significant difference in C/R ratios for syndromic diagnosis, age at ABG, history of dentofacial orthopedics, maxillary expansion, and pre-maxillary osteotomy.
Conclusions
The majority of MCI in patients with BCCLP are periodontally compromised but bone support is improved when cleft adjacent lateral incisors are present.
Introduction
Cleft adjacent teeth in patients with bilateral complete cleft lip and palate (BCCLP) have dental anomalies including gingival recession, altered crown morphology, rotation, and agenesis.1–5 The maxillary central incisors (MCI) can have shortened roots, bone dehiscence and reduced alveolar bone levels compromising their stability and long term prognosis.6,7,8 Repair of BCCLP often involves the use of dentofacial orthopedic appliances, maxillary expansion, orthodontic appliances, pre-maxillary osteotomy, and alveolar bone grafting (ABG). The influence of these interventions on prognosis of MCI in patients with BCCLP is unclear.
The purpose of this study was to assess the periodontal bone support of MCI in patients with BCCLP. The specific aims were to: 1) measure the radiographic crown to root (C/R) ratio of MCI in patients with BCCLP, and 2) determine if predictor variables of syndromic diagnosis, age at time of ABG, presence of maxillary lateral incisor (MLI), history of dentofacial orthopedics, maxillary expansion, and premaxillary osteotomy are associated with the C/R ratio of MCI.
Materials and Methods
Study Design and Sample
The investigators designed and implemented a retrospective radiographic study of patients with BCCLP who had post-operative ABG Cone Beam Computed Tomographic (CBCT) scans between January 1, 2002 and September 30, 2018. Subjects were excluded if medical records were incomplete, CBCT landmarks could not be identified or root development was not complete. This study was approved with a waiver of written informed consent by the institutional review board at Boston Children's Hospital (IRB- P00030161).
Variables
The primary outcome variable was crown-to-root ratios (C/R) of MCI measured radiographically. Predictor variables included syndromic diagnosis, age at ABG, presence of maxillary lateral incisor (MLI), history of dentofacial orthopedics, maxillary expansion, and premaxillary osteotomy.
Measurements
Patients had CBCT images acquired with a standard protocol on either an i-CAT 3D (Imaging Sciences International Inc, Harfield, PA) or a Planmeca ProMax 3D Max (Planmeca Oy, Helsinki, Finland) imaging system. Measurements were performed on CBCT scans obtained greater than 4 months after ABG using Dolphin 3D software (Dolphin Imaging & Management Solutions, Version 11.95 Premium. Chatsworth CA, USA). Images with 1-mm cuts were oriented along the long axis of the tooth and the most apical margin of alveolar bone identified. Radiographic crown height of the MCIs was measured linearly from the incisal edge to the most apical border of the alveolar bone along the long axis of the tooth. Axial, sagittal and coronal views were all used to identify the most apical point of the alveolar bone. From this same point, the root length was measured linearly from the most apical border of the alveolar bone to the root apex (Figure 1). The length of the crown to the length of the root was used to calculate MCI radiographic crown to root ratio (C/R ratio). A C/R ratio of 1/1.5 was considered a normal MCI C/R ratio based on accepted anatomic norms and radiographic studies.9–14 The McGuire and Nunn prognosis classification system denotes that teeth with 50% or less bone support have a poor prognosis. 15 Therefore, a MCI with 50% bone loss has an adjusted C/R ratio of 1.75/0.75 or 2.33. All MCI with C/R ratio >2.33 were classified as periodontally compromised. Calculation of intra-class correlation coefficients (ICC) allowed for determination of interrater reliability for continuous variables by a second measurer. ICC was calculated using a 2-way mixed model and interpreted following the guidelines presented by Koo and Li. 16
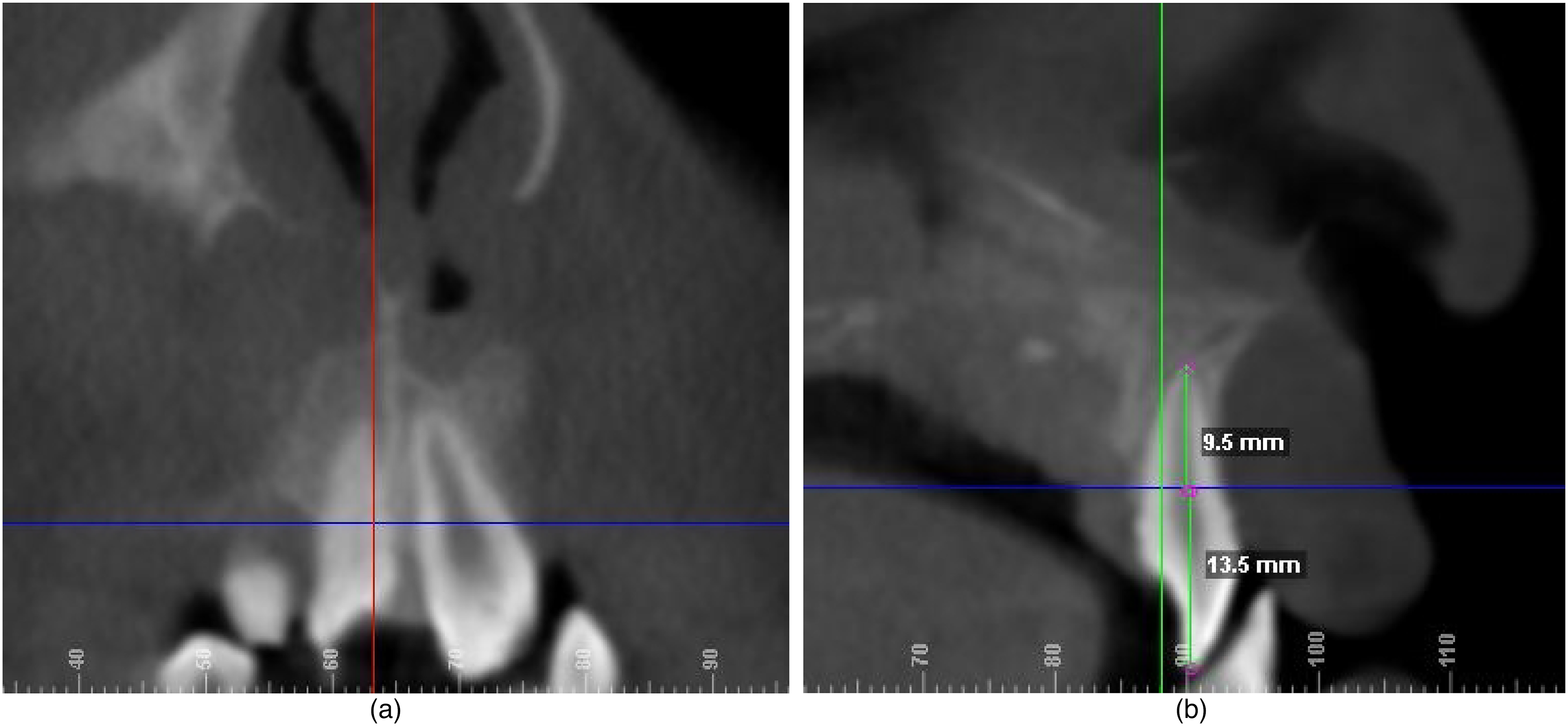
A. Coronal view with right maxillary central incisor oriented along its long axis. Margin of alveolar bone marked by blue line. B. Sagittal view of right maxillary central incisor in cross section. Crown measurement made using measuring tool along the long axis of the tooth from incisal edge to most apical border of alveolar bone denoted by blue line. Root measurements made linearly from this point to root apex.
Data Analysis
The MCI C/R ratio was compared across all predictor variables using independent-samples median testing and Fisher's exact analyses. All analyses were performed using SPSS software (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp). Significance was set as P < .05.
Results
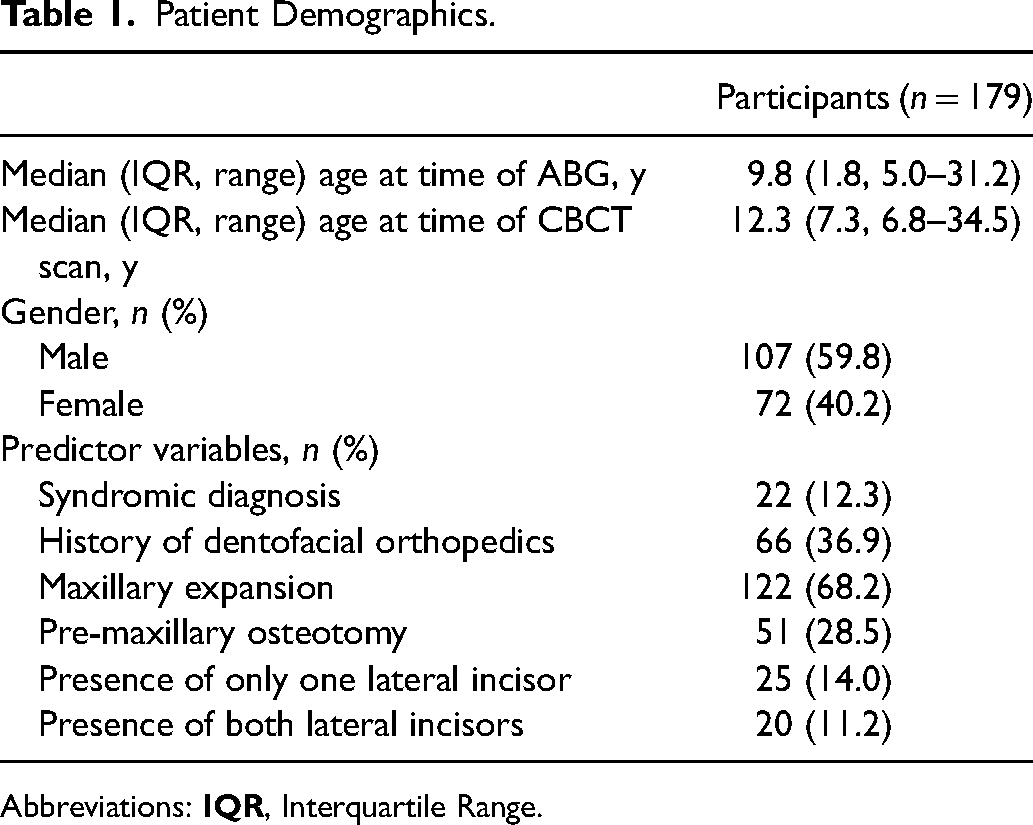
The study sample was comprised of 179 subjects (59.8% male, median age 12.3 years, Interquartile range [IQR] 7.3 years, range 6.8–34.5 years) (Table 1) including 22 with a syndromic diagnosis (40.9% male, median age 10.1 years, IQR 2.0 years, range 7.3-18.6 years. The median age at time of ABG was 9.8 years with an interquartile range of 1.8 years. For 65.0% of MCI, the C/R ratio was >2.33 indicating periodontally compromised teeth. Intra-class correlation coefficients using 2-way mixed modeling for both crown and root measurements at tooth #8 and #9 sites were all greater than 0.90 indicating excellent inter-rater reliability. There was no significant difference in C/R ratios for syndromic diagnosis, age at ABG, history of dentofacial orthopedics, maxillary expansion, and pre-maxillary osteotomy (Table 2). The crown/root ratio for MCI #8 and MCI #9 did not significantly differ between male and female patients (P = .800; P = .532, respectively). MCI with a missing adjacent lateral incisor (MLI) had a significantly poorer prognosis compared to those where the MLI was present (70.3% vs 50.0%, P < .001). A total of 152 (84.9%) patients were missing at least one MLI. There were 43 MCI missing at the time of CBCT measurements. Subjects with a syndromic diagnosis were significantly more likely to be missing a MCI compared to those without a syndromic diagnosis (31.7% vs 9.2%, P < .001). (Table 2). Age at ABG, history of dentofacial orthopedics, maxillary expansion, and pre-maxillary osteotomy, were not associated with a missing MCI.
Patient Demographics.
Abbreviations:
Maxillary Central Incisor Prognosis Using Fisher's Exact Analysis.
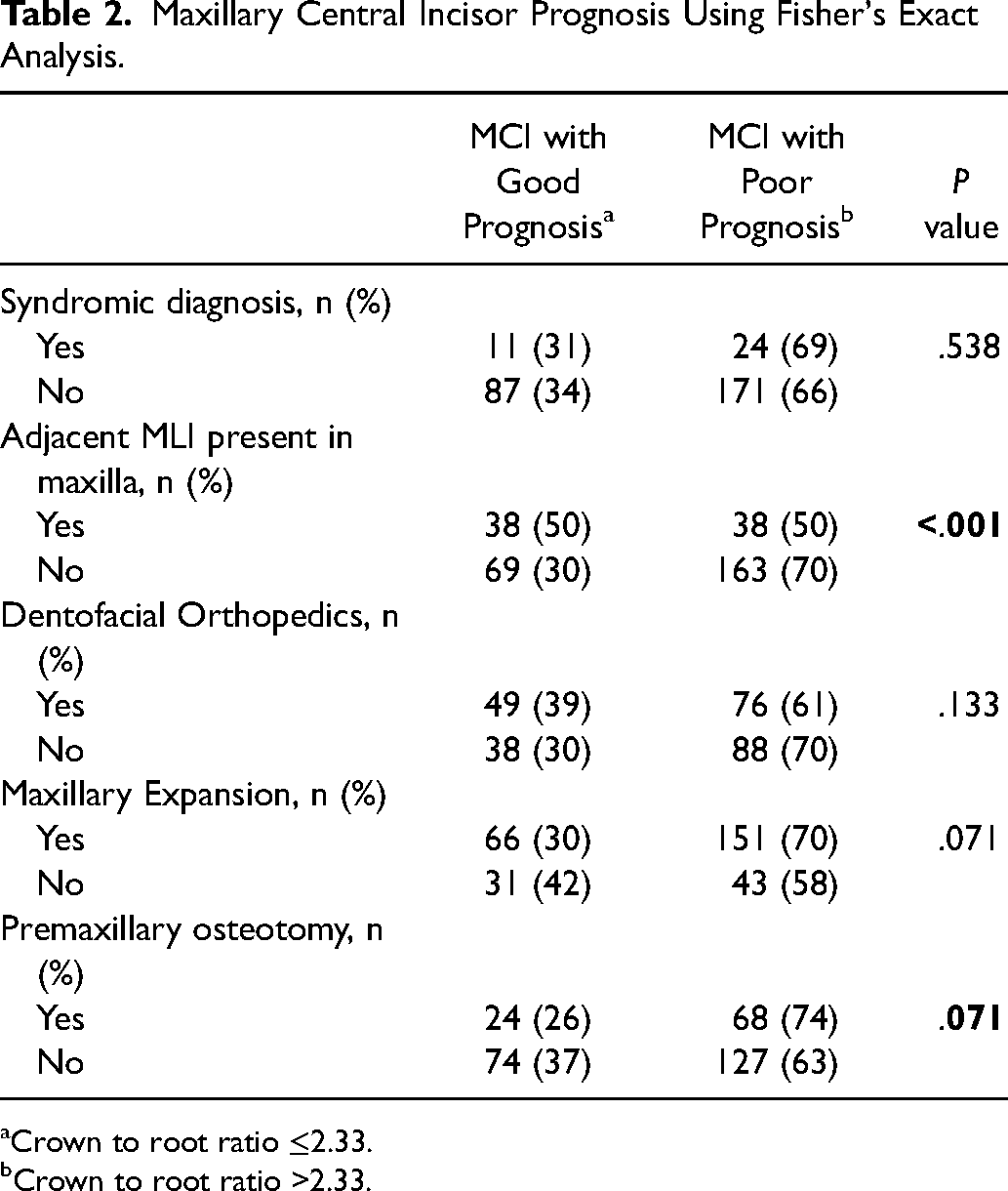
Crown to root ratio ≤2.33.
Crown to root ratio >2.33.
Discussion
The purpose of this study was to assess the periodontal bone support of MCI in patients with BCCLP. The specific aims were to: 1) measure the radiographic crown to root (C/R) ratio of MCI in patients with BCCLP, and 2) determine if the predictor variables of syndromic diagnosis, age at time of ABG, presence of maxillary lateral incisor (MLI), history of dentofacial orthopedics, maxillary expansion, and premaxillary osteotomy are associated with the C/R ratio of MCI.
The results of this study showed that 65.0% of MCI in patients with BCCLP had an unfavorable crown to root ratio. When an adjacent MLI was present, the MCI had significantly greater periodontal bone support and improved prognosis. Unfortunately, 85% of this cohort were missing at least one MLI. These findings are consistent with other reports documenting congenitally missing MLI in 60-80% of patients with cleft lip and palate.17–20
The unfavorable C/R ratio of the maxillary central incisors in patients with BCCLP may be compromised by the existing anomalies in these teeth.13,18,19,21 Al Jamal et al. found that the root length of MCI in patients with BCCLP were shorter than non-cleft controls while crown height was not-statistically different. 13 This suggests that crown heights are comparable and a shortened MCI root in patients with BCCLP accounts for the higher crown to root ratio. Delayed MCI root development may occur in patients with BCCLP and can result in a larger C/R ratio if measurements are taken prior to the completion of root formation, but MCI with an open root apex were not included in our study.19,22 Most of the published studies evaluating MCI abnormalities are in patients with unilateral clefts and the non-cleft side is used as control. Reduced alveolar bone height, decrease in periodontal bone thickness and increased frequency of boney dehiscence of cleft adjacent MCI have been reported in patients with unilateral clefts.6,23–26 All three contribute to impaired periodontal support around cleft adjacent MCI and influence MCI long term prognosis. Crown to root ratio was chosen in our study because it takes into account both alveolar bone height as well as dental anomalies such as shortened roots to assess overall prognosis of these teeth.
Several variables were evaluated to determine association with MCI C/R ratio. The presence of a lateral incisor was the only predictor associated with a better MCI C/R ratio. This is likely due to the lateral incisors ability to retain more bone in the premaxilla. There is also evidence of a stabilizing effect of normal transseptal fibers between the central and lateral incisors. 27 When the lateral incisor is missing, the MCI is adjacent to the cleft defect and is more susceptible to poor plaque control and gingivitis until the oronasal fistula and alveolar cleft are repaired.27–29 We hypothesized that dentofacial orthopedics, maxillary expansion and pre-maxillary osteotomy would have detrimental effects to the MCI because of the extrinsic forces placed on the MCI with these interventions. We found that none of these variables were associated with an increased MCI C/R ratio. Orthodontic therapy can shorten MCI roots via external apical root resorption leading to worsening C/R ratio and there is evidence that external apical root resorption from orthodontic therapy is greater on cleft adjacent MCI compared to non-cleft MCI.7,8,30 At our institution orthodontic therapy is deferred until after the alveolar cleft is repaired, and therefore we did not include this as a predictor variable. However, since most patients with BCCLP will undergo orthodontic therapy after alveolar bone grafting, we hypothesize the percentage of MCI with poor bone support may increase with time.
This study has several limitations including the retrospective study design and relatively small sample size. Due to the retrospective nature of the study we were not able to obtain all clinical data from the 179 patients included in our sample, thus a subset of data points were not available for analysis. This study only measures C/R ratio at one point and does not document the long term health of these teeth. Future studies investigating periodontal support of MCI after orthodontic/surgical treatment and at the completion of growth may provide more insight into the long term prognosis of MCI in patients with BCCLP. Additionally, our findings may not be generalizable since not all institutions follow the same treatment algorithms.
In conclusion, the majority of MCI in patients with BCCLP have poor C/R ratio suggesting a guarded long term prognosis. The periodontal support of MCI is improved when cleft adjacent lateral incisors are present. Dentofacial orthopedics, maxillary expansion and premaxillary osteotomy did not appear to be associated with the periodontal health of the MCI in patients with BCCLP.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article