
Abstract
Objective
To measure the tooth lengths of fully developed permanent upper incisors and to qualitatively evaluate the root shapes of the incisors in patients with cleft lip and palate (CLP).
Design
Cross-sectional, noninterventional, case-control imaging study.
Setting
Hospital and Stomatology Unit of Peking University, Beijing, China (institutional tertiary care).
Participants
Sixty consecutive nonsyndromic CLP patients (including 40 unilateral [UCLP] and 20 bilateral [BCLP]), and 53 age- and sex-matched controls were selected for this study.
Main Outcome Measure
Crown heights and root lengths of permanent upper incisors were measured from cone beam computed tomography scans, and the root shapes of upper incisors were evaluated.
Results
Compared with controls, the crown heights of upper incisors in CLP patients were reduced by 9.7% to 22.5% (p < .05), and the root lengths were reduced by 15.8% to 31.7% (p < .05). BCLP patients had greater reductions than the UCLP cases (p < .05). There were no significant differences between incisors and their antimeres in controls and BCLP patients. However, measurements on the cleft side in UCLP patients were lower than those of the noncleft side (p < .05). The prevalence of atypical root shape was higher in CLP than in the control group (p = .002); of these, 83.3% (30/36) occurred in central incisors near the cleft.
Conclusion
The permanent upper incisors in nonsyndromic CLP patients are underdeveloped. Incisor developmental deficiency was greater in teeth adjacent to the cleft.
Keywords
Cleft lip and palate (CLP) is one of the most common congenital malformations and involves the lip, palate, jaws, and alveolar process. Some dental anomalies, such as peg-shaped teeth, malformations of crown and root, and delay in tooth development may occur with a higher frequency than normal in patients with CLP (Ranta, 1986; Brouwers and Kuijpers-Jagtman, 1991; Solis et al., 1998; Eerens et al., 2001; Pioto et al, 2005). The early diagnosis of malformations in root shape and deficient root length in CLP patients may influence their orthodontic treatment strategy.
Many studies of the development of teeth in CLP patients have found that the formation of permanent teeth in children with CLP was delayed by between 4 months and 1.6 years (Ranta, 1986; Solis et al., 1998; Lai et al., 2009). However, none of these studies related the delay of tooth development to deficient crown and root development in the permanent upper incisors once fully developed.
There are several reports concerning tooth length in CLP patients. Bonn (1963) reported that the root of the permanent central incisor on the cleft side was shorter than that of the corresponding tooth on the noncleft side. Other researchers reported that 5.1% to 44.1% of unilateral (U)CLP patients had abnormal upper incisors with root malformations, as determined by panoramic radiographs (Hellquist et al., 1979; Dewinter et al., 2003; Tortora et al., 2008). However, these three studies were qualitative descriptions. Aljamal et al. (2010) measured the root lengths and crown-root (C/R) ratios of permanent teeth of CLP patients, also using panoramic radiography. Panoramic radiography has limitations as an observational method because images of teeth on panoramic radiographs may appear distorted and blurred (Friedland, 1998). This can cause inaccuracies in the measurement of tooth length.
The root shape in CLP patients may also complicate their orthodontic treatment plan. A 10.6% prevalence of root malformations of the anterior teeth in the cleft area in UCLP patients was previously reported (Dewinter et al., 2003), but another study found no root malformations in bilateral (B)CLP patients (Tortora et al., 2008). However, neither study defined their criteria for “root malformation.” Stahl et al. (2006) reported 7.6% (20/263) atypical root shapes in patients with cleft lip and/or cleft palate (CL/P) from panoramic radiographs. However, root curvature can occur in the labial or palatal directions, and this may cause underestimation of the root curvature with conventional periapical and panoramic radiographs.
Cone beam computed tomography (CBCT) is a new radiographic method that has been applied in orthodontics and oral surgeries for CLP patients (Hamada et al., 2005; Lund et al., 2010). CBCT provides highly detailed three-dimensional (3D) imaging that can be obtained at any angle. This makes linear measurement more accurate and reproducible (Sakabe et al., 2007; Sherrard et al., 2010). In our hospital, CLP patients routinely receive CBCT scans to evaluate the quality of alveolar bone grafts and the development of teeth near the cleft.
The objectives of the current study were (1) to determine whether there were deficiencies in the fully developed permanent upper incisors of CLP patients, and (2) to evaluate the root shapes of the incisors of CLP patients.
Materials and Methods
Patient Selection
Information for the present investigation was obtained from the registration of Department of Oral Radiology, from October 2007 to March 2009. Inclusion criteria for CLP patients were as follows: (1) diagnosed with UCLP or BCLP without other recognizable syndromes; (2) was 11 years of age or above; (3) had clear cone beam computed images; and (4) received no previous fixed orthodontic treatment. The sample size was calculated using the formula n1 = n2 = 2[(t2α + t2β)s/δ]2, where s is the estimate of the standard deviation on the basis of results of preliminary study, and 8 is the minimal clinically relevant difference between the two means. In our study, α = 0.05, β = 0.10, t0.10 = 1.645, t0.20 = 1.282, α = 0.05, β = 0.10, s = 3 mm, and δ = 2 mm; therefore, a total of 80 subjects should be enrolled. Sixty consecutive nonsyndromic patients with CLP (comprising 40 UCLP and 20 BCLP) aged from 11 to 27 years (mean, 18.8 ± 4.3 years) were included in this study. The control group consisted of 53 age- and sex-matched non-CLP orthodontic patients who were selected randomly from skeletal Class I orthodontic patients. None of them had received previous fixed orthodontic treatment. Ages of controls ranged from 11 to 26 years (mean, 18.9 ± 4.7 years). Patient age and sex characteristics are described in Table 1.
Age and Sex of CLP Patients and Controls
CBCT Imaging Parameters and Reconstruction
All CBCT images of the upper incisors were obtained with the 3D Accuitomo (J. Morita, Kyoto, Japan) by the same radiologist using the same standardized method, with a pixel size of 0.125 mm and a field of view of 4 cm. The tube voltage was 80 kV and the tube current was 6 mA, with a scanning time of 18 seconds. The volumetric data generated by the CBCT system were reconstructed, and all images were assessed on the same monitor. Primary data reconstructions were made by acquisition software (i-Dixel-3DX, 3D, Version 1.68, J Morita Mfg. Corp.) with an Accuitomo workstation providing axial, coronal, and sagittal views. Secondary reconstruction was then made so that the long axis of the tooth became parallel to the axes of two perpendicular, vertical image planes. This provided optimal visualization of the tooth/root in the axial, coronal, and median sagittal planes (Fig. 1).
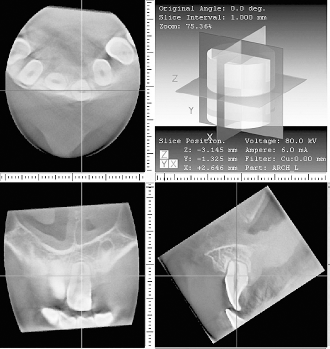
The axial, coronal, and median sagittal views of the right upper central incisor in a 14-year-old boy with BCLP, showing a short root.
Tooth Length Measurements
Crown heights and root lengths of the median sagittal image were measured using the method described by Delivanis and Kuftinec (1980). Four reference points including the apex point (A), incision superius (IS), and the labial and palatal cementoenamel junctions (CEJ) were marked (Fig. 2). The tooth was divided into two parts, the crown portion and the root portion, by the cervical reference line, which joined the labial and palatal CEJ. Crown height was defined from the midpoint of the cervical reference line to the incision superius. Root length was defined from the midpoint of the cervical reference line to the apical point. If the teeth severely bended mesially or distally, the crown portion and the root portion were reconstructed and measured separately along a longitudinal axis paralleling to the crown or root individual axis. The tooth was divided into two parts by using the cervical reference line. The cervical reference line joined the labial and palatal CEJ which are closest to the apical point. Teeth were excluded if (1) the apex was not closed, (2) restoration involving the IS had occurred, and (3) a marked attrition facet of the crown involving the IS was present.
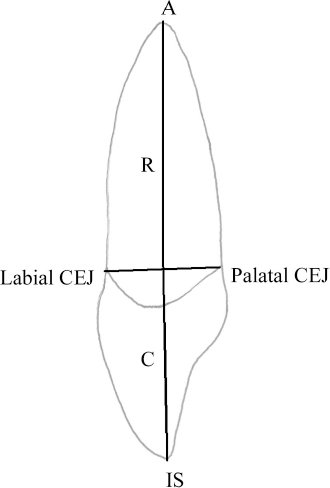
Schematic illustration of the method of measuring of crown height and root length on a median sagittal CBCT image. The line connecting the labial and palatal cementoenamel junction (CEJ) intersects the long axis of the tooth, thereby defining the root length (R) and the crown height (C).
All measurements were made by the same person and were remeasured at an interval of 2 weeks, after which the mean of the two measurements was adopted. Data are expressed as mean (SD) with 95% confidence intervals. To assess intra-examiner reproducibility and the reliability of measurements, 20 randomly selected individuals were remeasured at a minimum interval of one month. The method error (ME) was calculated using the formula ME2 = ∑d2/2n, where d is the difference between double assessments and n is the number of double determinations (Houston, 1983). The method error of the measurement was less than 2%.
Assessment of Root Shape
The coronal and sagittal images of the incisor were constructed to assess the root shapes of the incisors. An atypical root shape was recorded when teeth had root dilaceration or significant root curvature beginning from the cervix of the tooth (Stahl et al., 2006), and/or a twisted root (Fig. 3). Dilaceration is defined as a severe bend or distortion of a tooth, often approximating an angle from 45° to more than 90° (Scheid, 2007). The images were studied by three examiners. The first and second examiner performed two readings of the images independently, and the time interval between the readings was 1 week. The third reading was carried out by all three examiners together 1 month later. Discrepancies in interpretation were resolved by discussion during simultaneous examination. To assess the reliability of the assessment, 20 randomly selected individuals were re-assessed 2 weeks later. The measure of agreement showed no difference between the two assessments (k = 0.95).
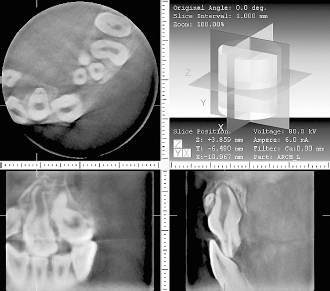
The views of the upper central incisors near the cleft, showing a twisted root.
Data Analysis
In order to exclude the influence of the position of cleft, the upper incisors of the CLP patients were classified into the noncleft and cleft sides, such that all incisors of the BCLP patients were classified as the cleft side. The Statistical Package for the Social Sciences (SPSS), version 13.0 (SPSS Inc., Chicago, Ill), was used for statistical analysis. The tooth lengths of the incisors of males and females in all groups were compared by independent sample Student's t tests. Differences in root lengths, crown heights, and R/C ratios between CLP subjects and controls were studied using two-way analysis of variance (ANOVA) to determine whether sex and/or cleft type was significant, and multiple comparisons was carried out by using the Bonferroni method. Differences in measurements between the incisors and their antimeres were studied using the paired Student's t tests. Differences in the prevalence of atypical root shapes among the groups were analyzed by the chi-square test. For all tests, a p value of <.05 was considered statistically significant. The study was approved by the ethics review committee of the Peking University Health Science Center.
Results
Patient Measurements
Measurements were conducted for a total of 373 upper permanent incisors (177 for CLP, 196 for controls), including 217 central incisors (118 for CLP, 99 for controls) and 156 lateral incisors (59 for CLP, 97 for controls). Seventy-nine potential tooth measurements were not taken, 63 from the CLP sample, mainly because teeth were missing. Only one upper central incisor in a patient with BCLP was not measured because it was severely bended. According to Ribeiro et al. (2003), the lateral incisor is considered a single tooth in the vicinity of the cleft, on the mesial or distal side. When a tooth on the mesial side was found with another one on the distal side, the latter was considered a supernumerary tooth. In the present study, there was one supernumerary tooth in a patient with UCLP, and this was not measured.
In the patients with CLP, the difference in the tooth lengths between male and female patients was not statistically significant. However, in the control group, the tooth lengths of male patients were approximately 1 mm (5%) longer than those of female patients for all the upper incisors (p < .05; Table 2).
Differences in Tooth Lengths of Incisors According to Sex in CLP Patients and Controls
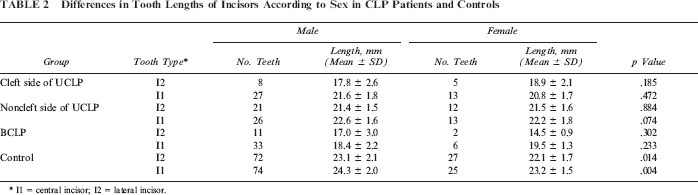
I1 = central incisor; I2 = lateral incisor.
Tooth Length, Root Length, and Crown Height: Upper Central Incisor
For the upper central incisor (I1) two-way ANOVA between the groups revealed that patient sex had a significant effect on the root length and R/C ratio, but the cleft factor did have a significant effect on all the measurements.
The mean tooth lengths and root lengths of the BCLP patients, and the cleft and noncleft sides of UCLP patients are shown in Table 3. Compared with the control group, the mean tooth lengths were reduced by 5.8%, 9.6%, and 21.2% in the noncleft and cleft sides of UCLP patients, and BCLP patients, respectively. The Bonferroni test showed that the differences between all the groups were statistically significant, except for the difference between the cleft side and noncleft side of UCLP. The mean root lengths were reduced by 7.5%, 15.8%, and 31.7% in noncleft and cleft sides of UCLP patients, and BCLP patients, respectively. The Bonferroni test showed that the differences between all the groups were statistically significant. By examining crown height, BCLP I1 teeth were reduced by 9.7% compared with controls (p < .01); however, crown heights on both the cleft and noncleft side in UCLP were only reduced by 3% (p > .05). With regards to the R/C ratio, teeth were reduced by 25.0% in a comparison of the BCLP samples to controls (p < .01), while the cleft side of the UCLP patients were reduced by 13.4% (p < .01); however, the difference between the control group and the noncleft side of UCLP was not statistically significant (Table 3).
Differences in the Tooth Lengths, Root Lengths, Crown Heights, and R/C Ratios Between UCLP, BCLP, and Controls
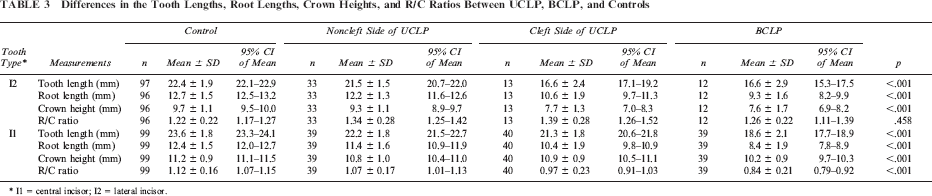
I1 = central incisor; I2 = lateral incisor.
Tooth Length, Root Length, and Crown Height of the Lateral Incisor
Regarding the lateral incisor (I2), two-way ANOVA between the groups revealed that patient sex only had a significant effect on the root length, whereas cleft had a significant effect on all measurements except the R/C ratio.
The differences in the tooth lengths, root lengths, and crown heights between UCLP, BCLP, and controls were statistically significant (Table 3). The Bonferroni test showed that the differences between controls and the noncleft side of UCLP, and between the cleft side of UCLP and the BCLP group, were not statistically significant. However, the differences between controls and the cleft side of CLP were significant for all three measurements (p < .01). R/C ratios between UCLP, BCLP, and controls were not significantly different (Table 3).
Comparison of Antimeres
The results of the paired Student's t tests indicated that there were no significant differences between the incisors and their antimeres in controls and BCLP (p > .05). However, measurements obtained on the cleft side were significantly lower than those of the noncleft side in UCLP (p < .05), except for the R/C ratios of the lateral incisor and the crown height of the central incisor (Table 4).
Differences in the Tooth Lengths, Root Lengths, Crown Heights, and R/C Ratios Between the Cleft Side Incisors and Their Antimeres in UCLP
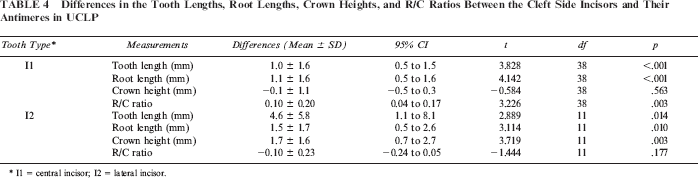
central incisor; I2 = lateral incisor.
Atypical Root Shape
The prevalence of atypical root shapes was higher in CLP patients than in the control group (ρ2 = 12.92, p = .002) (Table 5). There were 36 teeth with atypical root shape in the CLP patients; 83.3% (30/36) of these were central incisors near the cleft, several of which had twisted roots.
The Number and Percentage of Teeth With Atypical Root Shape in all Samples
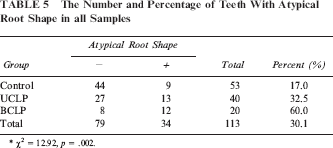
* χ2 = 12.92, p = .002.
Discussion
In previous studies, periapical radiographs (Brezniak et al., 2004), parallel apical film (Larheim and Eggen, 1979), and panoramic radiographs (Hölttä et al., 2004) were used to evaluate root length quantitatively and qualitatively. However, radiographs can appear distorted and blurred, which may cause inaccuracy in marking and measurements. To reduce the influence of distortion, some researchers have used the mesial and distal CEJs to divide the tooth into crown and root portions and calculate the C/R ratio (Sameshima and Asgarifar, 2001; Hölttä et al., 2004). However, the accuracy and reliability of this method are affected by the position, angulation, and rotation of the tooth (Friedland, 1998; Sameshima and Asgarifar, 2001; Stramotas et al., 2002; Sherrard et al., 2010). According to one study, rotation and malposition occur in 78.1% of permanent central incisors adjacent to the cleft in children with UCLP and 95.9% in BCLP (Lai et al., 2009) owing to the lack of space at the end of the alveolar segment (Smahel et al., 1996). Therefore, it is difficult to estimate the upper incisors accurately with the use of conventional radiographs. CBCT provides highly detailed 3D imaging, which can be obtained at any angle, offers optimum viewing, and eliminates superposition. This makes linear measurements more accurate and reproducible (Sakabe et al., 2007; Sherrard et al., 2010).
The results of the current study indicate that the permanent upper incisors in nonsyndromic CLP patients are developmentally deficient, with the root affected most severely. Incisors adjacent to the cleft show more developmental deficiency than those further away. We found that the crown heights of the central and lateral incisors in CLP patients are reduced by 9.7% to 22.5%, and the root lengths are reduced by 15.8% to 31.7%. The root portion was affected more severely than the crown portion in our CLP patients, which was in accordance with previous results (Bonn, 1963; Hellquist et al., 1979; Dewinter et al., 2003; Tortora et al., 2008; Aljamal et al., 2010). We also found that most measurements on the cleft side in UCLP were lower than those of the noncleft side, except for R/C ratios of lateral incisors and the crown heights of central incisors. This result contradicts a previous study showing that BCLP and UCLP subjects had comparable C/R ratios for the maxillary anterior teeth, and that UCLP cleft and noncleft side teeth C/R ratios were also comparable (Aljamal et al., 2010). Moreover, our study also shows that the developmental deficiency increases with the severity of the cleft. Compared with the controls, the root lengths of BCLP patients were reduced to a greater extent than those of UCLP cases (31.7% versus 15.8% for central incisors; 27.0% versus 17.1% for lateral incisors). The crown heights of BCLP patients were also reduced compared to those of UCLP subjects (9.7% versus 2.8% for central incisors; 22.5% versus 21.0% for lateral incisors), as were the R/C ratios (13.4% versus 25.0% for central incisors). These results also contradict Aljamal et al. (2010). The findings of the two studies are not entirely consistent, and this might have resulted from different measurement methods and racial differences of the studied populations.
The differences in R/C ratios of the central incisor between all groups were statistically significant (p < .001), but R/C ratios of the lateral incisor did not differ significantly, even though lateral incisor root lengths and crown heights in CLP patients were shorter than those of controls. One possible explanation for this is that the lateral incisor is more proximal to the cleft, so the development of the root and crown may be uniformly affected.
The mechanisms involved in human tooth root formation are not well understood. Some types of environmental insult during tooth development were reported to result in short-rooted teeth, such as chemotherapy (Jaffe et al., 1984) and radiotherapy (Hölttä et al., 2005). Many studies have found that the formation of permanent teeth in children with CLP was delayed, and that the cleft side was delayed compared with the noncleft side (Ranta, 1986; Brouwers and Kuijpers-Jagtman, 1991; Solis et al., 1998; Eerens et al., 2001; Pioto et al., 2005). Some researchers suggest that a deficiency of the blood supply near the cleft, either congenital or as a result of surgery, may negatively affect incisor dental formation in the cleft area (Dixon, 1968; Vichi and Franchi, 1995; Ribeiro et al., 2002). Fayad and Steffensen (1994) also reported that teeth in areas with denser vascularization developed faster and were larger than on the less vascularized side in children with facial hemihypertrophy and hemihypotrophy. The less vascularized effect of the cleft in CLP patients may decrease the proliferation and differentiation activity of cells in the developing apical complex of tooth roots (Xu et al., 2009), which could cause deficiencies in the organization of the root dentine during tooth development.
In this study, males and females in the CLP group exhibited no differences in tooth lengths, but the tooth length was about 5% less in females than in males in the control group, in agreement with the findings of previous studies (Verhoeven et al., 1979; Alvesalo, 2008; Aljamal et al., 2010). Studies suggest that the promoting effect of the Y chromosome on growth of root length is greater than that of the X chromosome (Lähdesmäki and Alvesalo, 2004; Alvesalo, 2008). However, the root-shortening effect of the etiological factor of the cleft in the CLP patients may dominate over the effect of sex chromosomes (Aljamal et al., 2010).
The prevalences of atypical root shape in UCLP and BCLP were 32.5% (13/40) and 60.0% (12/20), respectively, which were higher than the previous studies (Dewinter et al., 2003; Stahl et al., 2006; Tortora et al., 2008). In the current study, CBCT provided highly detailed 3D imaging. Since CBCT images can be obtained at any angle, we could avoid the underestimation of root curvature (labial or palatal) typical of conventional periapical and panoramic radiograph measurements. We also found that 83.3% (30/36) of teeth with atypical root shapes were central incisors near the cleft, several of which had twisted roots. Traumatic injury to the primary predecessors (Smith and Winter, 1981) and ectopic development of the tooth germ (Stewart, 1978) are two commonly causes of atypical root shape. In CLP patients, a cleft of the alveolus, and insufficient alveolar bone support, may cause ectopic development of the central incisor germ and therefore a high incidence of atypical root shape.
One limitation of the present study is that the CLP subjects were not randomly selected, and the male-female sex ratio was approximately 5.7:1 in BCLP patients, although males and females exhibited no differences in the mean tooth length. Another limitation was that teeth other than the upper incisors were not measured due to the limited scan scope.
Conclusion
Upper incisors in nonsyndromic CLP patients are underdeveloped, with the root affected more severely than the crown. This developmental deficiency increases with the severity of the cleft, with BCLP patients showing more severe deficiency than UCLP patients. Incisors that are closer to the cleft show more developmental deficiency. The cleft may play an important role in the developmental deficiency of the tooth in CLP patients.