
Abstract
Objective
To compare the soft tissue measurements of the upper lip and the nose on the cleft side and the noncleft side before surgery, immediately after cheiloplasty and two months after surgery.
Design
Descriptive clinical study with one group, prospective.
Setting
Department of Odonto-Stomatology, Children's Hospital 1, at Ho Chi Minh City - Vietnam.
Patients
31 patients with a unilateral complete cleft lip participated in this study, 30 patients were evaluated at the time two months after surgery.
Interventions
Interventions include PNAM and cheiloplasty by modified Millard technique.
Main Outcome Measures
Patients proceed to acquire 3D images of lips and nose, define landmarks and measure dimensions. There are 11 evaluators to be compared, p < 0.05 was considered statictical significance.
Results
After two months of surgery, on cleft side and noncleft side, the lengths of the upper lip were 10.87 ± 0.80 and 11.92 ± 0.78 (mm), the widths of the upper lip were 16.06 ± 1.10 and 16.40 ± 1.02 (mm), the heights of the nostril were 4.85 ± 0.44 and 5.93 ± 0.43 (mm), the lengths of columella were 4.08 ± 0.37 and 4.93 ± 0.38 (mm), and the widths of the nostril were 9.07 ± 0.37 and 8.37 ± 0.40 (mm).
Conclusion
Cheiloplasty by modified Millard technique on the patients who used PNAM showed that after two months of surgery, the morphology of the upper lip and nose has a slight disproportion with the nasolabial measurements of the cleft side being smaller than on the noncleft side.
Introduction
Cleft lip and palate is a common congenital anomaly in the craniofacial region, greatly affecting the function, aesthetics and psychology of patients. The treatment of cleft lip and palate is a comprehensive long-term process that requires multidisciplinary coordination. Nowadays, for a unilateral complete cleft lip/palate, in the neonatal period, the newborn was wearing presurgical nasoalveolar molding (PNAM) to reduce the severity of the cleft, and to increase the symmetry of the nose before surgery.1‐5 The following cheiloplasty to close the cleft, shape the upper lip and nose, improve the function and aesthetics of the patient.6‐8 In which, the morphology of the upper lip and nose is one of the most important measures to evaluate the results of cheiloplasty. There have been many studies to evaluate the morphology of the upper lip and nose after cheiloplasty, among which showed that the nasal morphology after surgery is more symmetrical in the group of patients who wear PNAM before surgery. 9 However, there have not been many studies evaluating changes in size of upper lip and nose on three-dimensional images before and after cheiloplasty in this group of patients. Therefore, we conduct this study with the desire to contribute the data of nasolabial measurements on three-dimensional images in children with unilateral complete cleft lip/palate, with the aim of comparing the soft tissue measurements of the upper lip and the nose on the cleft side and the noncleft side at the time before surgery, immediately after cheiloplasty and two months after surgery.
Materials and Methods
Patients
31 patients with a unilateral complete cleft lip participated in this study at Department of Odonto-Stomatology, Children's Hospital 1, at Ho Chi Minh City - Vietnam from March to September 2022.
Selection Criteria
- Children with a unilateral complete cleft lip (with or without cleft palate) ≥ 3 months old.
- Not associated with any craniofacial syndrome.
- Have been treated with PNAM (according to Grayson et al.) 1 for >2 months.
- The child's parents consented to participate in the study.
Exclusion Criteria
- Not healthy enough for surgical anesthesia.
Methods
Design: Prospective, descriptive clinical study with one group.
Materials
- Creality handheld 3D scanner.
- Computer with Geomagic Design X software.
Collecting Data
Obtain medical record information of patients after obtaining written consent from the patient's parent/guardian.
When the patients are under general anesthesia, proceed to acquire 3D images of the patient's lips and nose before surgery (T0), immediately after surgery (T1) using a Creality handheld 3D scanner.10,11
The patients underwent cheiloplasty using the modified Millard technique by two experienced surgeons.
2 months after surgery (T2) when the patient is sleeping in the dental chair: continue to acquire 3D images of the patient's lips and nose using Creality handheld 3D scanner.
Defining landmarks and measuring upper lip and nose dimensions (according to Mishra et al., 2010 and Ezzat et al., 2007)12,13 by computer with Geomagic Design X software14,15 (as shown in Figure 1a & 1b) by an assessor with Intra-class Correlation Coefficient of all variables are above 0.8. These landmarks and measurements are as follows:
A/A’: The peak of Cupid's bow on the noncleft side/cleft side B/B’: The corner of the mouth on the noncleft side/cleft side C/C’: The alar base on the noncleft side/cleft side D: Midpoint at the base of columella E/E’: The columella base on the noncleft side/cleft side F/F’: The highest point of columella on the noncleft side/cleft side G: The tip of the nose H/H’: Midpoint of CD/C’D I/I’: The highest point of the alar rim on the noncleft side/cleft side AC/A’C’: The length of the upper lip on the noncleft side/cleft side AB/A’B’: The width of the upper lip on the noncleft side/cleft side CD/C’D: The width of the nostril on the noncleft side/cleft side EF/E’F’: The length of the columella on the noncleft side/cleft side HI/H’I’: The height of the nostril on the noncleft side/cleft side Angle X: The deviation of the columella (angle formed by the line through DG and the vertical line, in which the vertical line had been defined as the plane perpendicular to the line connecting the bilateral madial canthus, which contains the line through the point D)
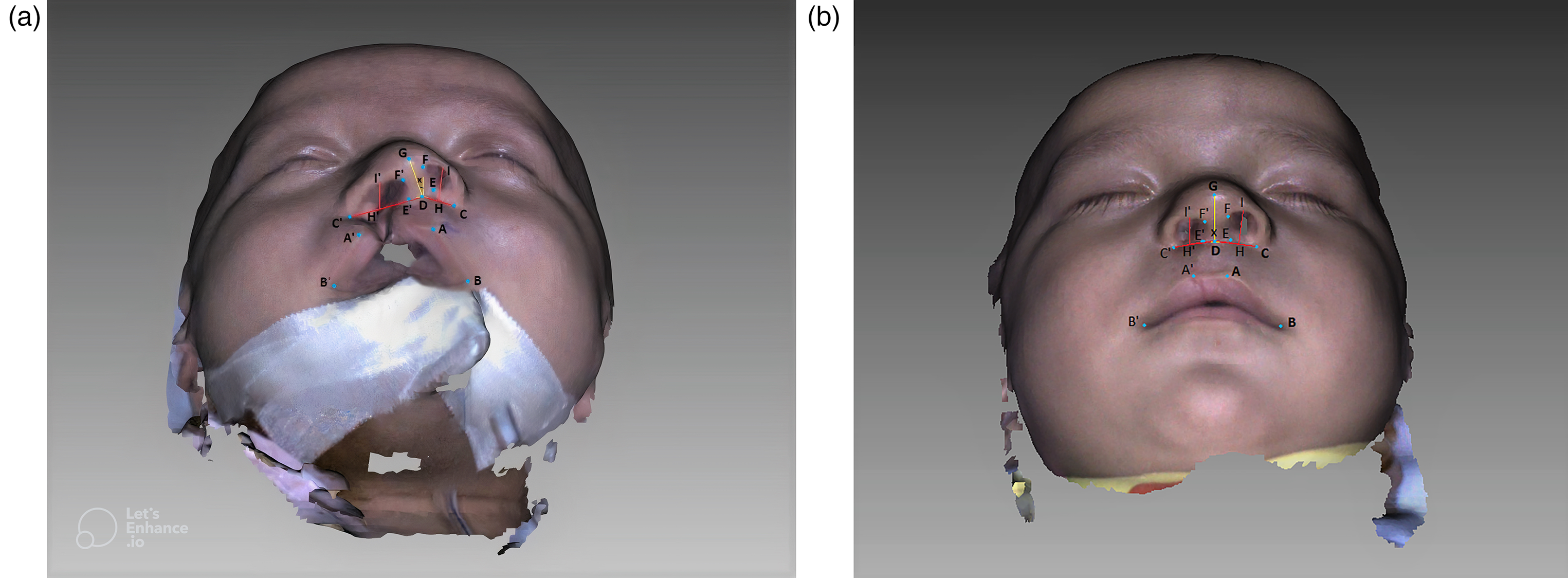
Landmark and measurements of the upper lip and nose on three-dimensional images: (a) Before surgery; (b) After surgery.
This study was approved by the Ethics Committee in Biomedical Research of University of Medicine and Pharmacy at Ho Chi Minh City on November 30, 2021, No. 713/HDDD-DHYD.
Results
There were 31 patients treated with PNAM and underwent cheiloplasty by the modified Millard technique; in which, there was 1 patient who did not re-examine at the time 2 months after surgery.
The study sample had 21 boys and 10 girls, the left-sided clefts accounted for 67.7% (21 patients), and cleft lip with cleft palate accounted for 77.4% (24 patients). The average age at surgery was 18.7 weeks of age (from 12.7 to 35) and the average duration of wearing PNAM is 14.3 weeks (from 8.3 to 24.3).
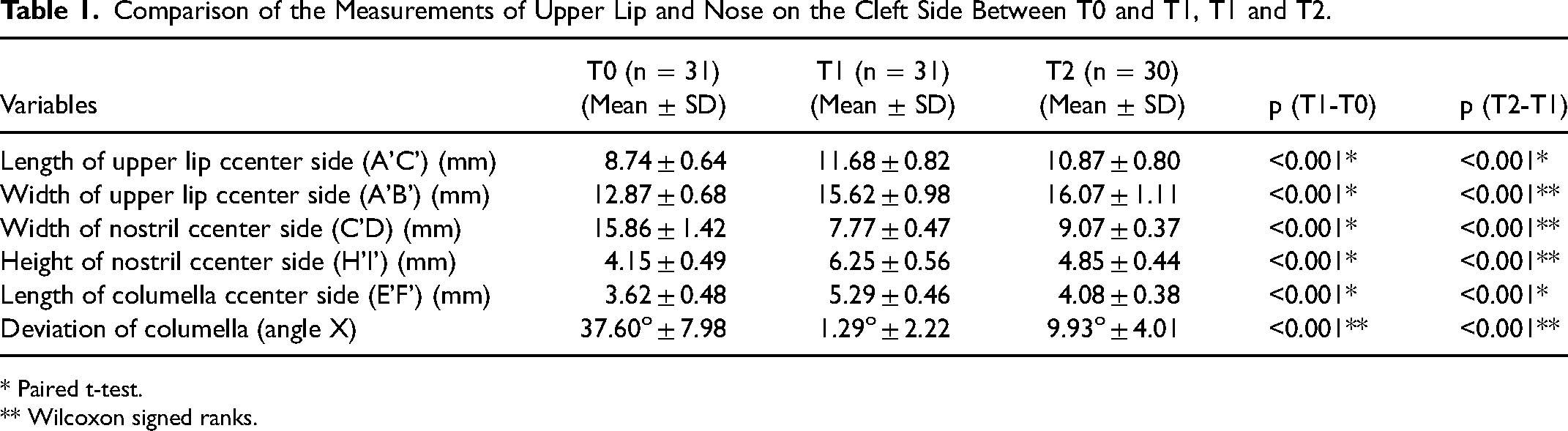
Comparison of the measurements of the upper lip and nose on the cleft side between T0 and T1, T1 and T2 are presented in Table 1. After two months of surgery, on the cleft side there are a decrease in the length of the upper lip, the height of the nostril and the length of the columella accompanying an increase in the deviation of the columella, the width of the nostril and the width of the upper lip compared to immediately after surgery (as shown in Table 1).
Comparison of the Measurements of Upper Lip and Nose on the Cleft Side Between T0 and T1, T1 and T2.
* Paired t-test.
** Wilcoxon signed ranks.
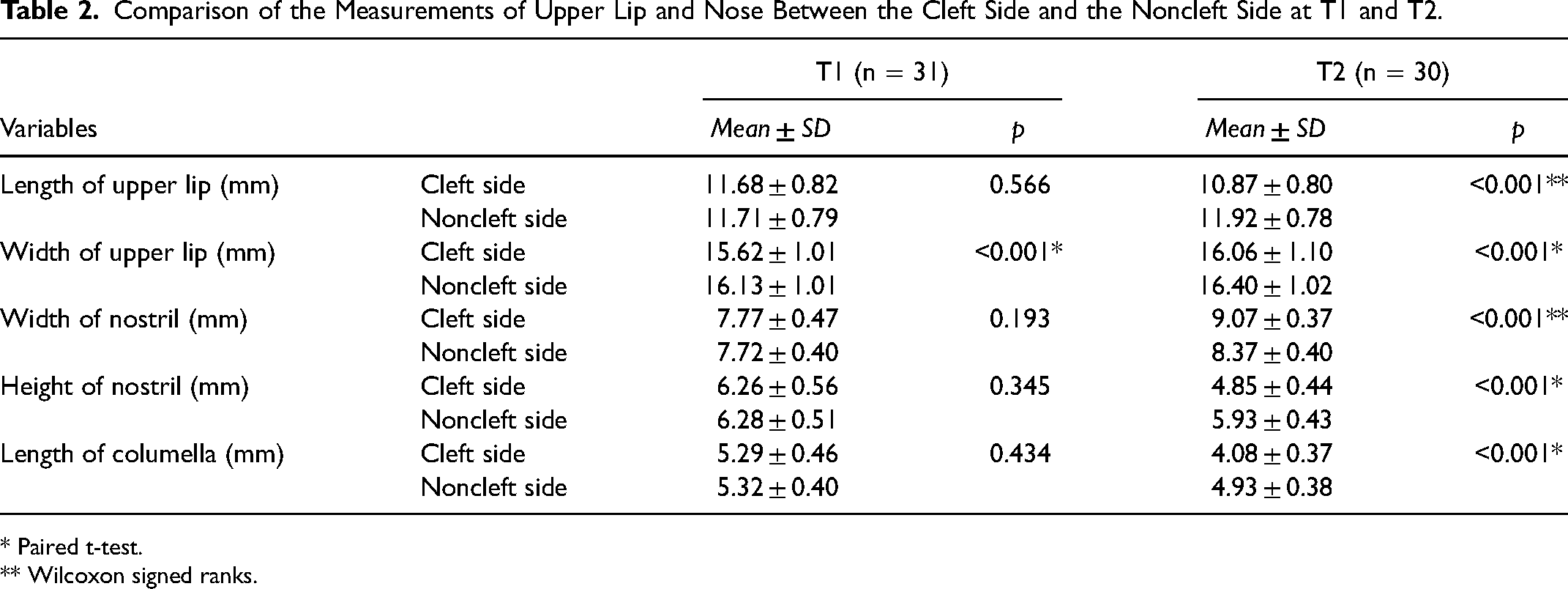
Comparison of the measurements of the upper lip and nose between the cleft side and the noncleft side at T1 and T2 are presented in Table 2. Immediately after surgery, the measurements of the upper lip and nose between the cleft side and the noncleft side were almost similar. However, after 2 months of surgery, on the cleft side, there were shorter upper lip, lower and wider nostril, and shorter columella compared to the noncleft side, the difference was statistically significant (as shown in Table 2).
Comparison of the Measurements of Upper Lip and Nose Between the Cleft Side and the Noncleft Side at T1 and T2.
* Paired t-test.
** Wilcoxon signed ranks.
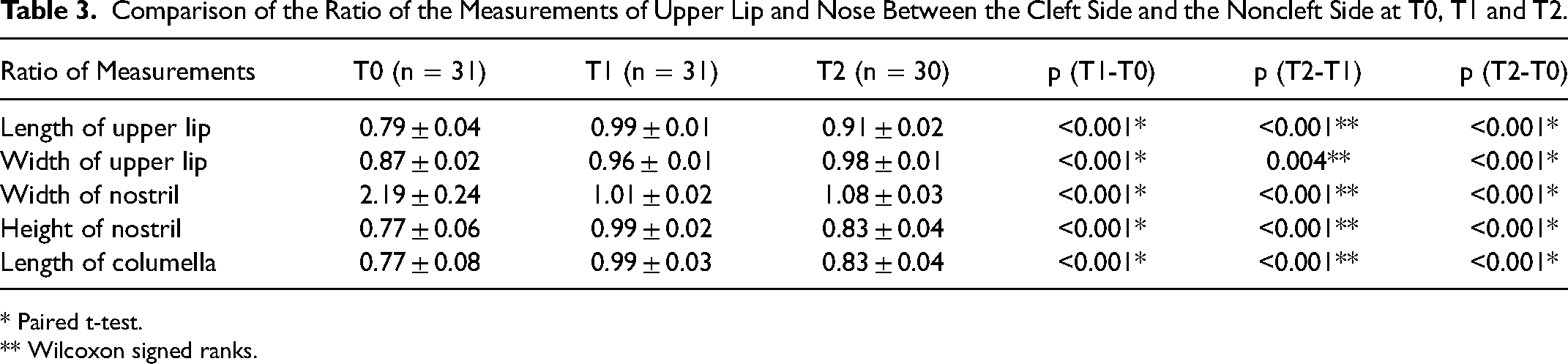
Comparison of the ratio of the measurements of the upper lip and nose between the cleft side and the noncleft side at T0, T1 and T2 are presented in Table 3. The ratio of the length of the upper lip, the height of the nostril and the length of the columella increased from time T0 to T1 and decreased from time T1 to T2. The ratio of the width of the upper lip gradually increased from the time T0 to T2. The ratio of the width of the nostril decreased from the time T0 to T1 and increased from the time T1 to T2. All of the above changes were statistically significant (as shown in Table 3).
Comparison of the Ratio of the Measurements of Upper Lip and Nose Between the Cleft Side and the Noncleft Side at T0, T1 and T2.
* Paired t-test.
** Wilcoxon signed ranks.
Discussion
Comparison of the Measurements of the Upper lip and Nose on the Cleft side Between T0 and T1
Table 1 shows that immediately after surgery (T1), there was an increase in the length and width of the upper lip, the height of the nostril and the length of the columella on the cleft side, while the width of the nostril on the cleft side decreased significantly compared to before surgery. The deviation of the columella is significantly improved, the columella is almost vertical. Obviously, surgery is not only closing the cleft but also helping to restore the anatomical shape of the lips and nose to the appropriate size, reconstruct the alar base and correct the deformities of the nose.
Comparison of the Measurements of the Upper lip and Nose on the Cleft side Between T1 and T2
After two months of surgery, there was a decrease in the length of the upper lip, the height of the nostril and the length of the columella on the cleft side; and an increase in the width of the nostril on the cleft side and the deviation of the columella compared to the time immediately after surgery (p < 0.05) (as shown in Table 1). The main factor affecting the results of cheiloplasty in the early period after surgery is common scar shrinkage, in which the straight scar of the Millard technique will often shrink and pull the top of the peak of Cupid's bow up, causing the length of the upper lip on the cleft side to be shortened. 16 There is also a recurrence of nasal cartilage deformity, combined with asymmetric growth direction of the alveolar on both sides of the cleft leading to the above situation, although the patients in our study had been using PNAM. The study of Cutting et al. (2003) after performing an extended Mohler variant of the Millard unilateral cleft lip repair also showed a decrease in the length of the upper lip and an increase in the width of the upper lip on the cleft side at 6 weeks after surgery. 17 Mulliken et al. (2012) also presented that after cheiloplasty using modified Millard technique, the width of the upper lip on the cleft side tends to increase by the time after surgery, similar to the results of our study. 18
For the nose, some previous similar studies in patients who had worn PNAM as the study of Nayak et al. (2020) also recorded a gradual decrease in the height of the nostril, a gradual increase in the width of the nostril on the cleft side, and an increase in the deviation of the columella by the time after surgery. 19 This recurrent problem has also been concerned by the authors and proposed solutions to help increase the symmetry of the nose. Chang et al. (2010) performed a retrospective study to compare the nasal morphology after cheiloplasty between 4 groups. Group 4 is the group that applies the most solutions including PNAM, primary rhinoplasty, overcorrection and silicone nasal conformer to retain the nostrils for 6 months after surgery; and the result showed that group 4 was fewest recurrences and achieved the best proportion of the groups. 20
Comparison of the Measurements of the Upper lip and Nose Between the Cleft side and the Noncleft side at T1
Table 2 shows that immediately after surgery, the measurements of the upper lip and the nose between the cleft side and the noncleft side is almost proportional. It can be seen that the modified Millard technique with the advancement and rotation flaps can help compensate for the missing length of the upper lip on the cleft side. In addition to the incisions available in thí technique, the surgeons have skillfully approached with alar cartilage to correct the deformities of the nose. And with the design of the L-flap on the lateral side, the surgeons can easily narrow the nostril on the cleft side. In addition, stitching to create continuity of the orbicularis oris muscle and closing the base of the nostril on the cleft side also help to create symmetry for the nostrils. Cutting et al. (2003) also showed that immediately after surgery, there was no difference in the lengths of the upper lip between the cleft side and the noncleft side, the width of the upper lip on the the cleft side was shorter than the noncleft side, similar to our results. 17 Some studies used the ratio between the measurements of the cleft side and the noncleft side to evaluate the symmetry of the upper lip and the nose, in which the closer this ratio is to 1, the more proportional it is. 20 Table 3 shows that immediately after surgery, most of the ratios between the cleft side and the noncleft side are approximately equal to 1, showing that the upper lip and the nose is almost proportional right after cheiloplasty. Study by Nayak et al. (2020) on patients wearing PNAM, the results also show that the nose is almost symmetrical at the time immediately after surgery. 19
Comparison of the Measurements of the Upper lip and Nose Between the Cleft side and the Noncleft side at T2
After two months of surgery, the length and the width of the upper lip, the height of the nostril, the length of the columella on the cleft side is smaller than the noncleft side, the width of the nostril on the cleft side is larger than the noncleft side (p < 0.05) (as shown in Table 2). As mentioned above, in the first few months after surgery, there is shrinkage of the straight scar, as well as the recurrence of nasal cartilage deformity and the difference in growth rate between the cleft side and the noncleft side leading to asymmetry. 21 In literature, some studies with a longer evaluation time after surgery and with the surgical methods according to Millard or Tennison- Randall or Mohler, the results after surgery were recorded with asymmetry, in which the length and width of the upper lip on the cleft side is smaller than on the noncleft side.22,23 However, most of the studies on measurements are based on two-dimensional images, which are somewhat limited when assessing the stereoscopic images.
For the measurements of the nose, the results of this study are similar to the study of Pai et al. (2005) on patients wearing PNAM, in which the measurements on the cleft side and the noncleft side were equal at the time one month after surgery and then the width of the nostril tended to be larger and the height of the nostril on the cleft side was smaller than on the noncleft side at one year after surgery. 3 In another study, Mahmoun et al. (2021) compared a group of patients wearing PNAM with the group that did not wear PNAM. The results show that the difference in the length of the columella between the cleft side and the noncleft side after surgery of the patients wearing PNAM lower than in patients not wearing PNAM, but still maintained a tendency to have the cleft side lower than the noncleft side in the postoperative period. 24 Therefore, in order to ensure stable surgical results, in addition to using PNAM, solutions can be implemented to compensate for the recurrence of deformities such as simultaneous primary rhinoplasty, cheiloplasty with modified techniques, overcorrection, maintenance of long-lasting silicone nasal conformer after surgery.
Conclusion
Cheiloplasty by modified Millard technique on the patients who used PNAM showed that immediately after surgery, the morphology of the upper lip and nose is quite proportionate to the measurements between the cleft side and the noncleft side with no statistical significant difference, except that the width of the upper lip on the cleft side is smaller than on the non cleft side. After two months of surgery, the morphology of the upper lip and nose has a slight disproportion with the nasolabial measurements of the cleft side being smaller than on the noncleft side, except that the width of the nostril on the cleft side is larger.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.