
Abstract
Cleft lip and palate is one of the most common congenital abnormalities affecting the craniofacial region. Cleft defect results in a broad nostril base and deviated lateral nasal cartilage causing a sunken dome and severe esthetic defect. This case represents an infant with unilateral cleft lip and palate reported at 4 months with an established feeding pattern negating the necessity for an obturator or Nasoalveolar molding. The lip-taping procedure was performed along with a nasal elevator of stainless steel wire framework with a hook-shaped unit padded with self-polymerizing acrylic resin. Prior to surgical repair nasal symmetry improved markedly, and the lip segments demonstrated favorable approximation.
Introduction
Oral cleft, a common congenital abnormality, can occur independently or as part of a syndrome due to the improper fusion of tissues during early development. Its etiology is multifactorial, involving genetic predisposition and external factors such as inadequate nutrition, hormonal imbalances, medication use, toxin exposure, and biological influences. A meta-analysis indicated a global prevalence of 0.3 and 0.45 per 1000 live births for cleft lip and cleft lip with palate, respectively. 1 Asian populations exhibit the highest prevalence, ranging from 0.82 to 4.04 per 1000 live births.2,3 In India, the incidence exceeds the global average, with approximately 35,000 infants born annually with cleft lip and palate. The national prevalence is 0.97 per 1000 live births, an 0.7 per 1000 live births in Gujarat. Unilateral clefts predominantly affect the left side. Gender differences demonstrate that cleft lip is more prevalent in males (male/female ratio of 1.81), while cleft palate is slightly more prevalent in females (female/male ratio of 0.93).2,3 A unilateral cleft defect is characterized by a broad nostril base and divided lip segments on the affected side, with the impacted lower lateral nasal cartilage causing a sunken dome, enlarged alar rim, slanted columella, and protruding nostril tip. In cleft palate cases, the nasal septum deviates toward the unaffected side, and the nasal base shifts, resulting in severe esthetic defect. 4 Matsuo et al. (1989) introduced a nonsurgical technique utilizing silicone tubes to shape the nostril, which Dogliotti et al. (1991) and Grayson et al. expanded upon, employing an intraoral molding plate with nasal stents (NAM) to align alveolar ridges and mold nasal cartilage. Berggren (2001) and Berggren et al. (2005) proposed an alternative method utilizing adhesive paper tape and a nasal elevator to improve nasal morphology prior to surgery.5–9 In some regions, a commercially available nasal elevator based on this design is now being manufactured. Treating clefts with severe nasolabial deformities presents a significant surgical challenge in achieving functional and esthetic outcomes. Recent advancements in CLP treatment have adopted a multidisciplinary approach, facilitated by improved surgical techniques and presurgical infant orthopedics (PSIO) (Esenlik and Aydin, 2015; Gandedkar et al., 2018).10–12 However, many of these methods are complex, costly, and demonstrate maximum benefits only when the patient is presented very early after birth.13,14 This case report highlights an affordable and practical nasal elevator designed to mitigate cleft deformities, in a 4-month-old male infant with unilateral cleft lip and palate presenting late.
Case Report
A 4-month-old male infant was referred to the Pediatric Dentistry Unit, Oral Health Science Centre, Postgraduate Institute of Medical Education and Research, Chandigarh, India for treatment of a cleft deformity. Diagnosed by the Department of Plastic Surgery at the same Institute, with a left-sided group 3 cleft lip palate, as per Balakrishnan classification, the child was born to a healthy mother and was her second offspring (Figure 1A and B). He had attained developmental milestones appropriate for his age and had no systemic illnesses except for the oral cleft. By the time of the clinical visit, his feeding pattern was well-established, negating the necessity for an obturator. Informed consent was obtained from the mother, and a treatment plan was formulated.

(A) and (B) Preoperative Photographs at Age 4 Month; (C) and (D) Iinitiation of Lip Taping Procedure was Done on the Day of Reporting.
A standard lip taping procedure was performed utilizing surgical adhesive tape and a thin dermal dressing to approximate the cleft segments as per the protocol followed at our Centre. (Figure 1C and D). Parents were instructed on lip tape application. Extraoral photographs and manual measurements of the cleft gap were obtained.
To address the nasolabial deformity and depressed left nasal dome, a nasal elevator was designed using a 0.036” stainless steel wire framework with a hook-shaped unit padded with self-polymerizing acrylic resin (Figure 2A and B). The appliance was refined and fitted, with the acrylic padding positioned inside the left nostril to provide pulling action. The frame was secured to the forehead using adhesive tape and activated by bending the wire at the acrylic padding.
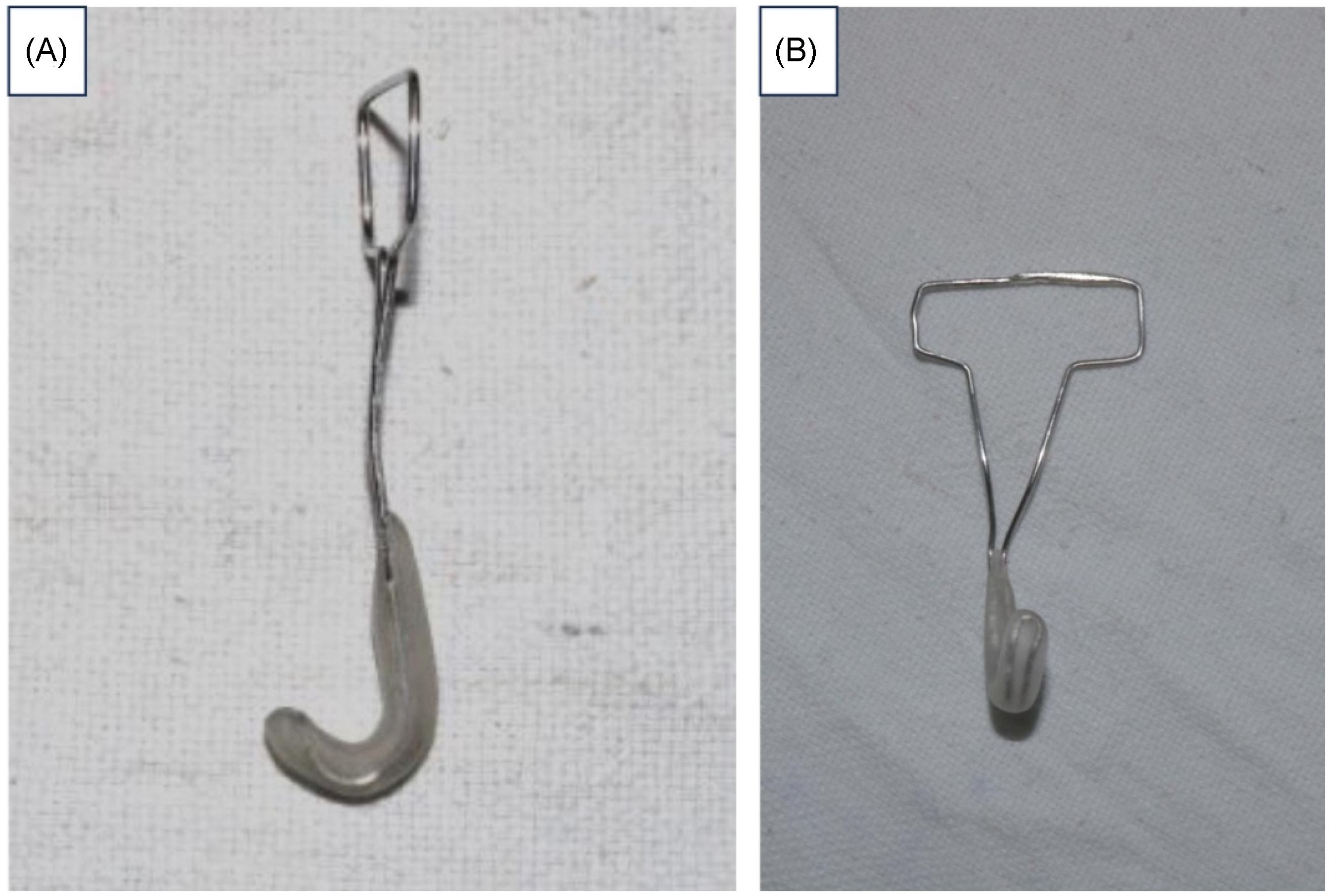
(A) and (B) Nasal Elevator Fabricated Using 0.036 Stainless Steel Wire Extending into a U-shaped Unit Covered With Clear Acrylic.
The patient was monitored for 24 h without allergic reactions or cutaneous eruptions. Monthly follow ups were conducted (Figure 3A and B). After 7 months, the gap between the cleft segments was reassessed, revealing a significant reduction in nasal segment separation from 9.5 to 4.5 mm. The nasal tip had shifted to a central position, the cleft side's dome had elevated, the medial and lateral crura angle had decreased, and the Alar facial groove on the cleft side became more pronounced. Overall, nasal symmetry improved markedly, and the lip segments demonstrated favorable approximation (Figure 3C and D).

(A) and (B) Appliance Delivered Along With Lip Tape in Place, Appliance Activation Done; (C) and (D) Photographs at 7 Months with Reduced the Cleft Gap and Good Nasal Morphology; (E) and (F) Postsurgical Image Showing Good Lip Esthetics and Satisfactory Elevation of Nasal Dome.
The medical team advised the patient to continue utilizing the assembly until the scheduled lip repair surgery. However, the procedure was delayed due to the patient's low hemoglobin levels of 8 g/dL. The lip repair surgery was performed in the Department of Plastic Surgery, when the patient was 10 months and 7 days old, yielding optimal results. Figure 3E and F depicts postoperative photographs immediately after surgery and at the 1-week follow up, respectively. The asymmetrically elevated nasal dome on the left side was repositioned more accurately, improving the patient's profile. The parents expressed complete satisfaction with the esthetic outcome. The patient is now awaiting palate repair surgery.
Discussion
Repairing cleft lip is both demanding and gratifying, requiring a deep understanding of esthetics and technical skill. 15 Neglecting nasal cartilage deformities often necessitates further surgeries. 15 Matsuo et al. noted that newborns have soft, pliable nasal, and auricular cartilage cells, enabling presurgical esthetic adjustments. This pliability arises from the nasal cartilage's composition, including chondrocytes and an intercellular matrix of collagen, elastin, and proteoglycan aggregates. Postbirth, the intercellular matrix components disconnect due to an influx of hyaluronic acid, enhancing moldability. 16 Elevated hyaluronic acid levels result from increased maternal estrogen in fetal circulation, aiding childbirth and gradually decreasing over the first 3 to 4 months postnatally.17,18 Numerous researchers recommend initiating the process of molding nasal cartilage and elongating the columella shortly after the third day of birth, continuing for up to 3 to 4 months postnatally to achieve optimal outcomes. 18
In this instance, the patient presented for medical intervention at 4 months and 2 days of age due to barriers such as financial limitations and accessibility to tertiary healthcare facilities. By this time, the infant had adapted to bottle feeding with breast milk, demonstrating appropriate weight gain and overall physical and mental development, indicating adequate nutrition. While there were no immediate functional concerns, addressing esthetic needs was essential. Considering the parent’s cosmetic concerns and the multiple benefits of PISO, we implemented our center's standard protocol for cleft lip and palate treatment. Regular follow-up examinations revealed a notable 5 mm reduction in the gap between cleft segments within 3 months and 15 days due to the combined effect of lip taping and nasal stent, indicating significant healing within 4 months. The appliance was fabricated using readily available 0.036 orthodontic stainless steel wire manipulated according to the patient's anatomy. The nasal part of the appliance was coated with acrylic resin to give the desired anatomical shape to the ala of the nose. It is a custom-made cost-effective alternative to the commercially available nasal elevators (Dynacleft). Post-lip repair, the cleft segments were esthetically aligned with minimal scar tissue formation and smooth healing. The appliance's simplicity and cost-effectiveness resulted in high parental satisfaction.
This device employs a straightforward approach to enhance facial esthetics as a whole. By regulating the pressure of the nasal stent, it effectively facilitates the molding and elevation of the nasal cartilages without inducing any adverse effects. Functional force was applied by gently bending the wire at the point where it exits the acrylic, directing it toward the nasal dome to provide a steady lifting force to the alar segments. An orthodontic plier was used to create a mild blanching effect on the soft tissue surface. The appliance was reactivated at each visit, with close monitoring for signs of rashes or ulceration, which remained negligible throughout. A key advantage of the custom-fabricated stent was its precise anatomical adaptation, along with its cost-efficiency. It offers ease of maintenance for caregivers and convenient activation for clinicians. This case report highlights the unique ability of a simple molding device assembly to significantly reduce the separation of cleft segments—even when the age of the patient is well beyond the typical age at which PNAM is undertaken. This depicts meaningful outcomes in late-presenting cases, reaffirming the clinical value of such interventions beyond conventional timelines in developing communities.
Conclusion
In developing countries, referrals to tertiary care centers for cleft lip and palate management are frequently delayed, exacerbating the condition's effects on feeding, weight, and psychological wellbeing due to the infant's appearance. The high cost of treatment further limits accessibility. To address these issues, our cleft team developed a cost-effective and sustainable nasal elevator, efficacious even for late-presenting patients. Strict compliance with the device reduced the cleft gap considerably commencing at 4 months of age, paradoxical to the conventional norms of early initiation of presurgical nasoalveolar molding. The parents have reported the appliance to be user-friendly, well-tolerated by the child, and highly cost-effective. Further prospective studies with larger samples are required to confirm the above findings.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.