
Abstract
Objective
To evaluate a method of measuring the change in palatal length and shape following maxillary advancement using synchronous lateral videofluoroscopy and voice recording in order to understand how movement of the maxilla may affect VPI risk in patients with cleft lip and/or palate (CL/P).
Design
Retrospective cohort study of children with cleft lip and/or palate.
Setting
Single center, tertiary children's hospital.
Participants
Patients with cleft lip and/or palate who underwent maxillary advancement between 2016–21 inclusive.
Interventions
Maxillary advancement surgery, including those who underwent concurrent mandibular procedures.
Main outcome measures
The length of the soft palate and the genu angle were measured throughout palatal dynamic range. Pre- and post-operative measurements were compared using a one sided T-test, with subgroup analysis for patients with clinical VPI.
Results
Ten patients were examined. The mean distance of maxillary advancement was 10.5 mm. The average increase in pre-genu soft palate length was 2.8 mm in the resting position and 2.9 mm in the closed position. The genu angle decreased in the closed position by 16.3 degrees.
Conclusions
The soft palate showed limited ability to lengthen following maxillary advancement and this may explain the risk of VPI. There was partial compensation by the muscle sling of the palate as demonstrated by a more acute post-operative genu angle and this suggests one reason for the variability of VPI reported. Future research is required to investigate how length and shape changes measured using this method can predict VPI risk.
Introduction
Cleft lip and/or palate (CL/P) are commonly occurring congenital anomalies with an incidence of approximately 1 in 700 live births. 1 Patients with cleft lip and palate have impaired maxillary growth that affects expansion in both the transverse and sagittal plane of the midface. 2 This could be contributed to by both the cleft itself and also from growth restriction due to scarring as a result of surgical repair in infancy. As the craniofacial skeleton develops throughout childhood, the maxilla grows disproportionately to the mandible, resulting in a 21% chance of developing maxillary retrusion for patients with CL/P.2,3 This adversely affects dental occlusion and esthetic profile of the face.
Le Fort I maxillary advancement is commonly performed to correct the resulting class III skeletal malocclusion. It has been reported that between 25–47% of patients with CL/P undergo maxillary advancement with the intention to normalize dental occlusion, improve facial esthetics and restore lip and tongue position for the generation of intelligible speech.2–5 Advancing the maxilla can adversely alter velopharyngeal sphincter function. The actual effect of this procedure on the velopharyngeal closing mechanism remains controversial, however, as published research shows conflicting estimates of velopharyngeal insufficiency (VPI) following maxillary advancement and reported incidence covers a wide range from 0–84% of cases affected.5–11 A recent meta-analysis suggested that the risk of bias and inconsistency in the literature precluded definitive risk prediction. 12 Harjunpää et al. found that the amount of horizontal or vertical movement of the maxilla during advancement did not predict the presence of VPI post-operatively. 13 Speech consequences of VPI include hypernasality and excessive nasal air emission, while nasal regurgitation of oral diet can also be a significant symptom. 14 This additional risk from surgery is important in patients with CL/P as they are a group that is already at increased baseline risk of VPI due to the N abnormal musculature of the soft palate.15,16
The soft palate is a complex structure. Anatomically, it has both a proximal and distal segment separated by the palatal genu. The genu approximates the border between the muscular and aponeurotic segments of the palate.17,18 In non-cleft patients, the position of the genu is strongly correlated to the length of levator veli palatini. 19 Velopharyngeal valve closure requires that the soft palate contacts the lateral and posterior pharyngeal walls to separate the nasopharynx from the oropharynx, an action that is essential for intelligible speech and oronasal competence. 2 Adequate velopharyngeal function is therefore dependent on the length, structure and activity of the velum as well as the opposing pharynx. By advancing the maxilla anteriorly during surgery, the attached soft palate is also advanced and this may be the mechanism by which VPI occurs in patients undergoing this procedure. The velopharyngeal gap has previously been measured in patients undergoing maxillary advancement, 20 however the actual change in palatal length and shape has never before been investigated. McComb et al. found that a shorter overall length of the soft palate and the postoperative pharyngeal depth were both risk factors for VPI, 2 a finding supported more recently in a similar study by Impieri et al. 21 These studies were performed, however, with the palate in the static, resting position only. The soft palate is a dynamic structure and there have been no studies examining structure and function throughout its range of motion.
This study was designed with the aim of defining and measuring the change in the length and shape of the soft palate throughout its dynamic range during speech for patients with CL/P who underwent maxillary advancement.
Methods
This was a retrospective cohort study including patients with CL/P who underwent Le Fort I maxillary advancement between 2016 to 2021. This research was approved by the local ethics committee (approval #2021/SSA00646). Participants were identified through unit records of maxillary advancement procedures. Patient demographics such as age and sex were recorded as well as underlying syndromes or conditions, the cleft subtype, and surgical procedure details. Patients in the unit who were under consideration for maxillary advancement underwent pre- and post-operative synchronous nasendoscopy, lateral video fluoroscopy and speech recording as part of the routine unit protocol workup.
The primary outcomes were the quantitative change in palatal dimensions and shape. The methodology for measurements was adapted from the work of Pet et al., who investigated soft palate dimensions and shape following Furlow Z-Plasty in cleft patients from lateral videofluoroscopy footage. 22 The palatal length in our study was estimated in two segments as presented in figure 1. Lateral videofluoroscopy footage was paused and measurements taken at the resting palatal position and also at maximum closure for comparison. The anterior velum (pre-genu) was measured from the posterior margin of the maxillary alveolar process to the genu. This is represented in the resting and closed palatal position by AB and AC respectively in figure 1. The posterior velum (post-genu) was measured from the genu to the palatal tip and is represented in the resting and closed palatal position by BD and CE respectively in figure 1. Measurements were taken in millimeters and adjusted for scale using the Storz rigid nasendoscope, which was of known diameter. The genu angle was estimated using trigonometric calculation from the other measurements. Measurements were taken by two independent investigators in duplicate and averaged to reduce bias.
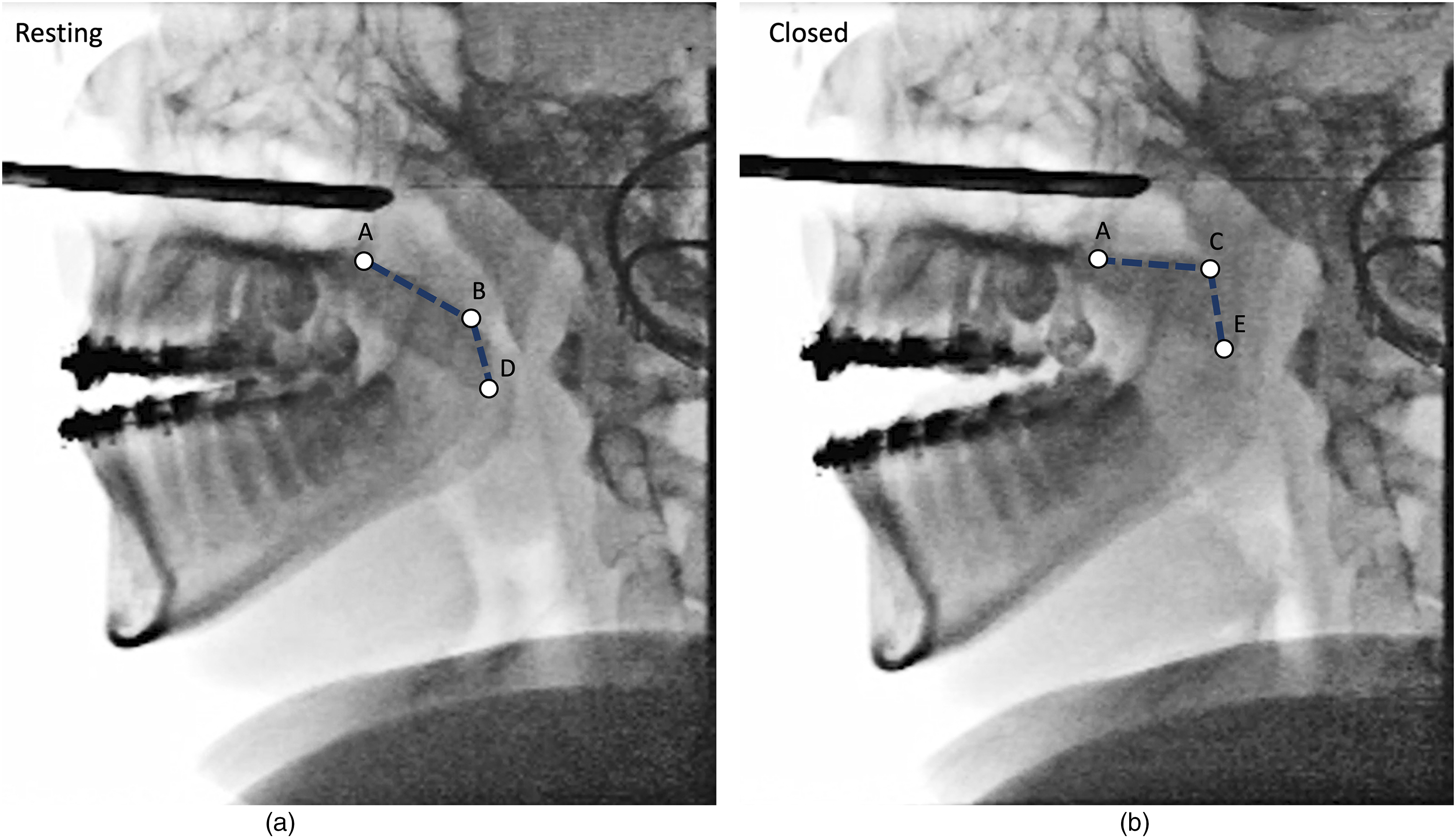
(A) mean palatal measurements taken from lateral video fluoroscopy footage with the palate in the resting position. (B) palatal measurements taken throughout dynamic range with the palate in the closed position.
Secondary outcomes examined the qualitative function of the soft palate. The presence of VPI post-operatively was recorded as diagnosed by expert cleft speech pathology review of the synchronous footage, which is part of unit protocol and the current gold standard for VPI assessment. 23 The need for further surgical procedures for VPI, such as Furlow Z-Plasty, posterior pharyngeal wall implant, or pharyngeal flap, were recorded.
Patient demographics and the secondary outcomes were presented as descriptive statistics. Pre- and post-operative soft palate measurements were compared using a one sided T-test performed with the software SPSS v28.0. Changes were considered statistically significant if p < .05. Subgroup analysis was performed between patients who were diagnosed with VPI post-operatively and those who had no features of VPI. Inter rater reliability was assessed by calculating the intraclass correlation coefficient (ICC) using a two way random effects model. The ICC and was considered to be good if greater than 0.75. 24
Results
Ten patients were identified, all of whom had pre- and post-operative synchronous imaging. Five patients were male and five were female. All patients had a diagnosis of non-syndromic cleft lip and palate. The mean age at the time of maxillary advancement was 18 years (range 16 to 20 years). All patients had documented, routine speech therapy and craniofacial unit assessments throughout growth and none were noted to have clinical VPI. Maxillary advancement was performed by Le Fort I osteotomy with rigid plate fixation, using orthodontic wafers as guidance for the correction. The mean maxillary advancement was 10.5 mm (range 9 to 12 mm). Quantitative data regarding changes in pitch or yaw was not available, as orthodontic preparation was performed off site. Three patients underwent concurrent mandibular setback procedures. Lateral video fluoroscopy was performed pre-operatively with comparison at a mean time of six months (range three to 16 months) post-operatively.
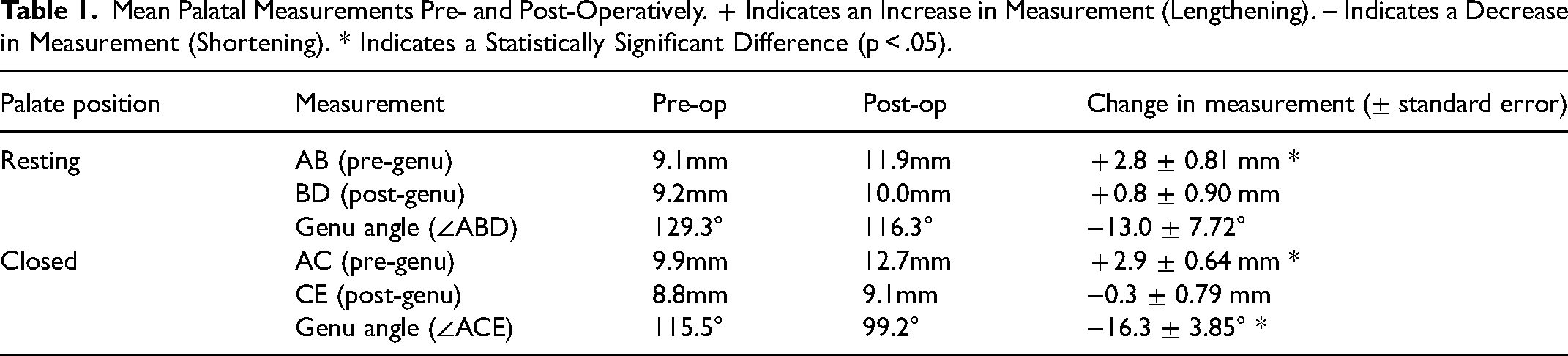
The mean palatal measurements are summarized in table 1. There was a statistically significant increase in length of the anterior (pre-genu) velum post operatively of 2.8 mm in the resting position and 2.9 mm in the closed position. The length of the posterior (post-genu) velum was not significantly changed. There was a statistically significant decrease in the genu angle post-operatively but only in the closed position, where the genu became more acute by an average of 16.3°. There was a trend towards a change in the genu angle in the resting position, which became more acute by an average of 13.0°, however this was not statistically significant.
Mean Palatal Measurements Pre- and Post-Operatively. + Indicates an Increase in Measurement (Lengthening). – Indicates a Decrease in Measurement (Shortening). * Indicates a Statistically Significant Difference (p < .05).
Three patients were diagnosed with VPI post-operatively, one of which underwent follow up palatal lengthening surgery by way of Furlow Z-plasty with good improvement in speech. The remaining two patients did not undergo further procedures; one patient's symptoms resolved over time and one was managed conservatively, having only mild VPI symptoms. Subgroup analysis was performed between the VPI group and the remaining patients, however there were no statistically significant differences between these groups for any measurements.
Discussion
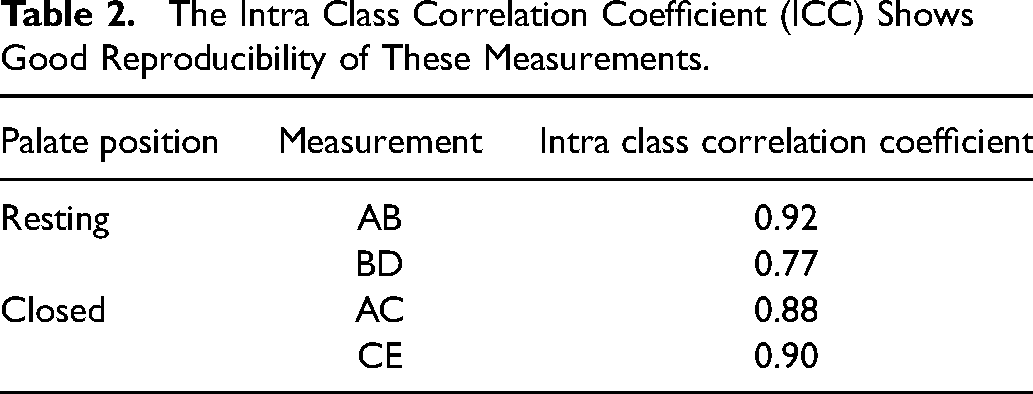
The intra class correlation coefficient was over 0.75 for all measurements (see Table 2), indicating that the imaging modality was clear enough to allow good reproducibility of the measurements between assessors. Considering the small sample size included in this study, advancing the maxilla in patients with cleft palate had noteworthy effects of the measured length and shape of the soft palate.
Length
The anterior portion of the soft palate was significantly lengthened on post-operative assessment by 2.8 mm and 2.9 mm in the resting and closed positions, respectively. This suggests that the velum has some ability to stretch and lengthen despite the underlying congenital abnormality and the additional presence of post-surgical scarring from previous palate repair. There is, however, a mismatch between the degree of maxillary advancement compared with the lengthening of the soft palate. The soft palate only lengthened, on average, by approximately 27% of the overall distance of maxillary advancement. There was, therefore, a resulting relative palatal length deficiency. This indicates that only partial compensation is possible from the velar side of the sphincter mechanism, and may explain why VPI occurs only in some patients and how studies have found it challenging to define risk factors for VPI, as individuals may have varied ability to stretch and compensate. It also highlights the role of the posterior pharyngeal wall in compensation, which may disguise the clinical effect of the palatal length deficit on speech.
Shape
The soft palate shape as measured by the genu angle, was significantly different post-operatively. The soft palate became more acute by 16.3° in the closed palatal position following maxillary advancement. This may represent residual tension and resistance to stretch by the palatal muscle sling. Alternately, the more acute genu may indicate an active compensatory “knee bend” attempt of the levator veli palatini to achieve velopharyngeal closure during speech. By forming a more acute angle the soft palate may be able adjust for the relative length deficiency to still achieve closure, perhaps at a higher level of the nasopharynx than pre-operatively. Again, this compensatory mechanism may be variably present in the individual (and indeed this small study group), leading to a less predictable change of VPI post-operatively.
The study had several limitations. It was not able to identify a significant difference in palatal length or shape for patients with a post-operative diagnosis of VPI compared with those who had no signs of VPI. This was likely due to the small number of participants, including only three patients who had VPI. A larger study would be required to investigate this measurement method as a predictor for VPI. Unit experience with this imaging modality is that it is generally well tolerated, however some key patient groups may not be able to tolerate the rigid nasendoscope, for example patients with intellectual disabilities such as some patients with syndromic clefts. The measurements taken only characterized the anterior structures involved in velopharyngeal closure. Further studies could be undertaken to measure post-operative changes in the other components of anteroposterior velopharyngeal closure, such as Passavant's ridge, posterior pharyngeal wall or superior constrictor mobility. The characterization of palatal length and shape for patients without a cleft undergoing maxillary advancement could be important for comparison, as patients without a cleft may be capable of more significant palatal lengthening due to the absence of post-surgical scarring in the palate. This study did not identify any patients without a cleft for comparison. There is an opportunity for studies with larger patient numbers to use subgroup analysis to compare patients with or without clefts, as well as other factors, such as different cleft subtypes or the original surgical repair technique. The lateral video fluoroscopic images reviewed in this study were clear, however we note that dynamic magnetic resonance imaging has been investigated and may also provide high quality imaging for accurate of measurements. 25
Conclusion
VPI following maxillary advancement surgery is an important issue for patients with CL/P as it can result in significant symptoms of hypernasality and nasal air emission speech characteristics as well as nasal regurgitation. The current literature is unclear regarding the incidence of and risk factors for developing VPI following Le Fort I maxillary advancement for patients with CL/P. This study characterized the change in length and shape of the soft palate following maxillary advancement in this group by using a novel method of measurement, which was shown to be reproducible. The soft palate appears to have the capacity to lengthen, although to a lesser degree compared with the distance of maxillary advancement, resulting in a relative palatal length deficiency. The genu angle became more acute post-operatively, indicating that the muscular palatal sling may exert ongoing passive tension on the soft palate, or that there is an active attempt at a “knee bend” by the palate to improve closure in compensation for the length deficiency. The ability of the soft palate to partially lengthen and achieve velopharyngeal contact by adopting a more acute genu angle may explain why VPI risk is variably reported in the literature, as each individual patient may have varied ability to compensate in these ways. This study provided a preliminary understanding of the change in the length and shape of the soft palate following maxillary advancement throughout its dynamic range, although its small cohort limits generalization to a wider patient group at present. More research is needed to fully understand how this method of measurement can characterize these changes in the context of variation amongst patients with a cleft, different cleft subtypes and the original method of surgical repair. Simultaneous videofluoroscopy, nasendoscopy and voice recording could be used for a larger patient cohort with a post-operative diagnosis of VPI to identify pre-operative length and shape predictors of VPI risk.
The Intra Class Correlation Coefficient (ICC) Shows Good Reproducibility of These Measurements.
Footnotes
Acknowledgements
The corresponding author is not the recipient of any research scholarships. This research was not funded by any organization.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Previous Presentations
The Royal Australian College of Surgeons Annual Scientific Congress 2022, Brisbane Australia.