
Abstract
Objective
To define “high osteotomy” and determine the feasibility of performing this procedure.
Design
Single institution, retrospective review.
Setting
Academic tertiary referral hospital.
Patients, Participants
34 skeletally mature, nonsyndromic patients with unilateral CLP who underwent Le Fort I osteotomy between 2013 and 2020. Patients with cone-beam computed tomography (CBCT) scans completed both pre- (T1) and post-operatively (T2) were included. Patients with bilateral clefts and rhinoplasty prior to post-operative imaging were excluded.
Interventions
Single jaw one-piece Le Fort I advancement surgery
Main Outcome Measures
Measurements of the superior ala and inferior turbinates were taken from the post-operative CBCT.
Results
The sample included 26 males and 8 females, 12 right- and 22 left-sided clefts. The inferior turbinates are above the superior alar crease at a rate of 73.53% and 76.48% on the cleft and non-cleft sides, respectively. One (2.9%) osteotomy cut was above the level of the cleft superior alar crease, and no cuts were above the level of the non-cleft superior ala. On average, the superior ala was 2.63 mm below the inferior turbinates. The average vertical distances from the superior alar crease and the inferior turbinates to the base of the non-cleft side pyriform aperture were 12.17 mm (95% CI 4.00–20.34) and 14.80 mm (95% CI 4.61–24.98), respectively. To complete a “high osteotomy,” with 95% confidence, the cut should be 20.36 mm from the base of the pyriform aperture.
Conclusions
A “high” osteotomy is not consistently possible due to the relationship between the superior alar crease and the inferior turbinate.
Keywords
Introduction
Orofacial clefts are the most common congenital birth defect of the face and place a substantial burden on patients and their families. 1 Surgical repair of orofacial clefts can result in significant scarring of soft tissues supporting the maxilla, which can restrict maxillary growth as the child develops.2–5 This scarring can contribute to maxillary deficiency and the development of a class III malocclusion, which are commonly observed in patients with orofacial clefts at the time of facial maturity.6,7 In patients with maxillary deficiency, orthognathic surgery is generally recommended with a reported incidence of 22–48% in patients with unilateral cleft lip and palate (UCLP) and 50–76% in patients with bilateral cleft lip and palate (BCLP).8–12
Midface deficiency in patients with a cleft lip and palate is often so severe that a traditional Le Fort I osteotomy of the lower maxilla may not be sufficient to ameliorate the deficiency and augment the paranasal soft tissue, leading to the development of a variety of craniofacial surgical techniques. One of these techniques is a “high” LeFort I osteotomy. This technique has been advocated to include an increased amount of the zygoma and anterior wall of the maxilla for improved midface protrusion. Unlike a traditional LeFort I osteotomy that starts relatively low on the medial buttress of the maxilla, the “high winged” LeFort I osteotomy starts much higher on the pyriform aperture and continues across the anterior maxilla to include a greater area of the face in the inferior osteotomy segment. Proponents of the “high winged” LeFort I osteotomy claim similar advantages to the LeFort III/I combination osteotomy without necessitating exogenous implants or imparting the morbidity associated with a true LeFort III osteotomy. 8
While a “high” osteotomy may address the lack of midface volume, this term is used without a clear definition in the literature. Dabir and Vahanwala define a traditional LeFort I osteotomy as starting approximately 3–4 mm above the nasal floor on the lateral wall of the pyriform aperture. 13 If the anatomy of the bony pyriform is considered, the superior limit of the Le Fort I osteotomy would be defined by the attachment of the inferior turbinate to the medial buttress. Thus, a “high” osteotomy would theoretically lie somewhere between 3–4 mm above the nasal floor and the inferior turbinate along the lateral nasal wall. Surgeons have used various descriptions of a “high” osteotomy, but none provide any specifics about where the osteotomies begin along the lateral nasal wall.8,14,15 Thus, a more specific definition of “high” osteotomy is needed if it is to be widely adopted and advocated.
In this study, we define a “high” LeFort I osteotomy as one that starts at or above the level of the superior nasal alar crease. This reference point was chosen in order to encompass the superior perialar tissue by including at least some of the upper maxilla. Using cone-beam computed tomography (CBCT) data of patients with a cleft lip and palate who have undergone LeFort I osteotomy, we evaluated the frequency with which a “high” osteotomy was performed. Additionally, we measured the relationship of the inferior turbinate to the most superior extent of the nasal alar crease to evaluate whether our definition of a “high” LeFort I osteotomy could be performed.
Patients and Methods
Study Design and Sample
A single institution, retrospective review of all skeletally mature non-syndromic patients with unilateral cleft and palate (CLP) who underwent LeFort I osteotomies between 2013 and 2020 was performed. Institutional Review Board approval was obtained prior to the start of this study. Patients were included if they were skeletally mature, were diagnosed with a unilateral CLP, underwent a single-piece LeFort I osteotomy advancement, and had a diagnostic quality CBCT scan completed both pre- (T1) and post-operatively (T2) with the post-operative scan being less than 1 year after the LeFort I osteotomy. Patients were excluded from the study if they had a diagnosis of bilateral CLP or a craniofacial syndrome, underwent previous maxillary distraction osteogenesis, a concomitant or second orthognathic procedure in addition to the LeFort I maxillary advancement, a rhinoplasty prior to the T2 CBCT, or had abnormal anatomic structures that resulted in the failure to identify key landmarks required for measurement.
CBCT Evaluation
Dolphin Imaging Software (Patterson Dental, Saint Paul, MN) was used for CBCT visualization and measurements. Two reference planes were used to ensure standardization of CBCT head positioning: Frankfurt Horizontal and a vertical plane equidistant between the most medial portions of the bilateral orbital rims. The most inferior point of the pyriform aperture on the non-cleft side was established as the pyriform base for all measurements (Figure 1). The osteotomy height was defined as the vertical distance between the most anteromedial point of the osteotomy along the lateral pyriform rim and the most inferior point along the base of the pyriform aperture. The level of the inferior turbinate was defined as the most anterior point of the inferior turbinate at its attachment to the lateral aspect of the pyriform aperture. The most superior aspect of the soft tissue nasal ala was defined as the most superior point along the alar crease (Figure 1). This point was marked and superimposed onto the bony skeleton for measurement. The measurements performed for this study are as follows: the non-cleft side pyriform aperture to cleft side superior alar crease (PCS); the cleft side Le Fort I osteotomy to the cleft side superior alar crease (COCS); non-cleft side pyriform aperture to cleft side Le Fort I osteotomy (PCO); inferior-most point of the pyriform aperture to cleft side inferior turbinate (PCT); inferior-most point of the pyriform aperture to non-cleft side inferior turbinate (PNT); non-cleft side Le Fort I osteotomy to non-cleft side superior alar crease (NONS); inferior-most point of the pyriform aperture to non-cleft side Le Fort I osteotomy (PNO); inferior-most point of the pyriform aperture to non-cleft side superior alar crease (PNS) (Figure 1).
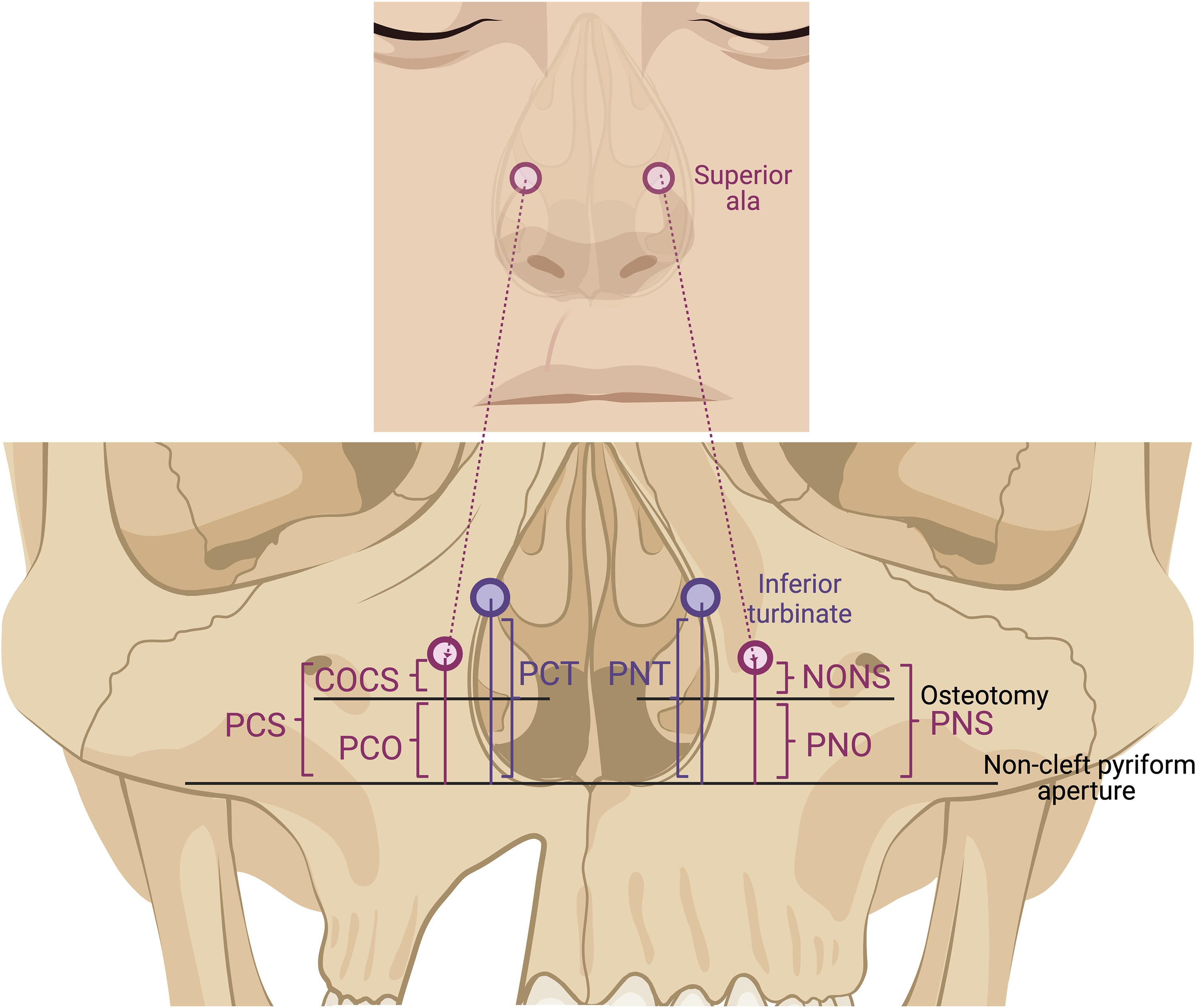
Graphic of the measurements on hard-tissue and soft-tissue windows on CBCT. Image made using BioRender. PCS: non-cleft pyriform aperture to cleft superior ala; COCS: osteotomy (on cleft side) to cleft superior ala; PCO: Non-cleft pyriform aperture to cleft side osteotomy; PCT: pyriform aperture to cleft inferior turbinate; PNT: pyriform aperture to non-cleft inferior turbinate; NONS: osteotomy (on non-cleft side) to non-cleft superior ala; PNO: non-cleft pyriform aperture to non-cleft side osteotomy; PNS: non-cleft pyriform aperture to non-cleft superior ala; the superior ala is the most superior portion of the alar rim, inferior turbinate is the most anterior location were the inferior turbinate meets the pyriform aperture. Non-cleft pyriform aperture is the base of the pyriform aperture on the non-cleft side.
LeFort I Surgical Technique
A CBCT was performed for pre-operative orthognathic assessment and surgical planning. All patients underwent pre-operative decompensatory orthodontic treatment. A standard single-piece Le Fort I osteotomy was performed through an upper gingivobuccal sulcus incision. Subperiosteal and submucosal dissection was used to expose the pyriform aperture and lateral nasal wall, which is bounded superiorly by the origin of the inferior turbinate. The osteotomy was generally placed as high as possible along the lateral nasal wall. Post-operative CBCT scans were performed at a maximum of 1-year after surgery to avoid capturing any post-operative relapse.
Statistical Analysis
Distances were calculated as statistical means with 95% confidence intervals. Statistical significance was evaluated using student's t-test with statistical significance defined as a p value less than 0.05. Six random patients were measured by the same evaluator 5 months after the initial analysis to measure the intra-rater reliability, which was assessed using the Intraclass Correlation Coefficient (ICC).
Results
Patient Demographics and Surgical Characteristics
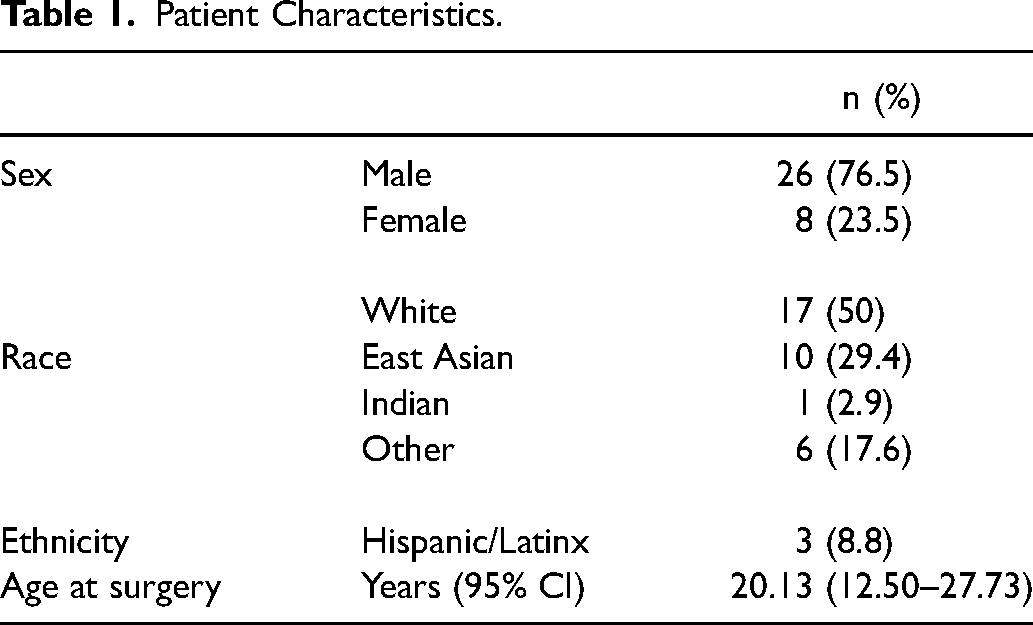
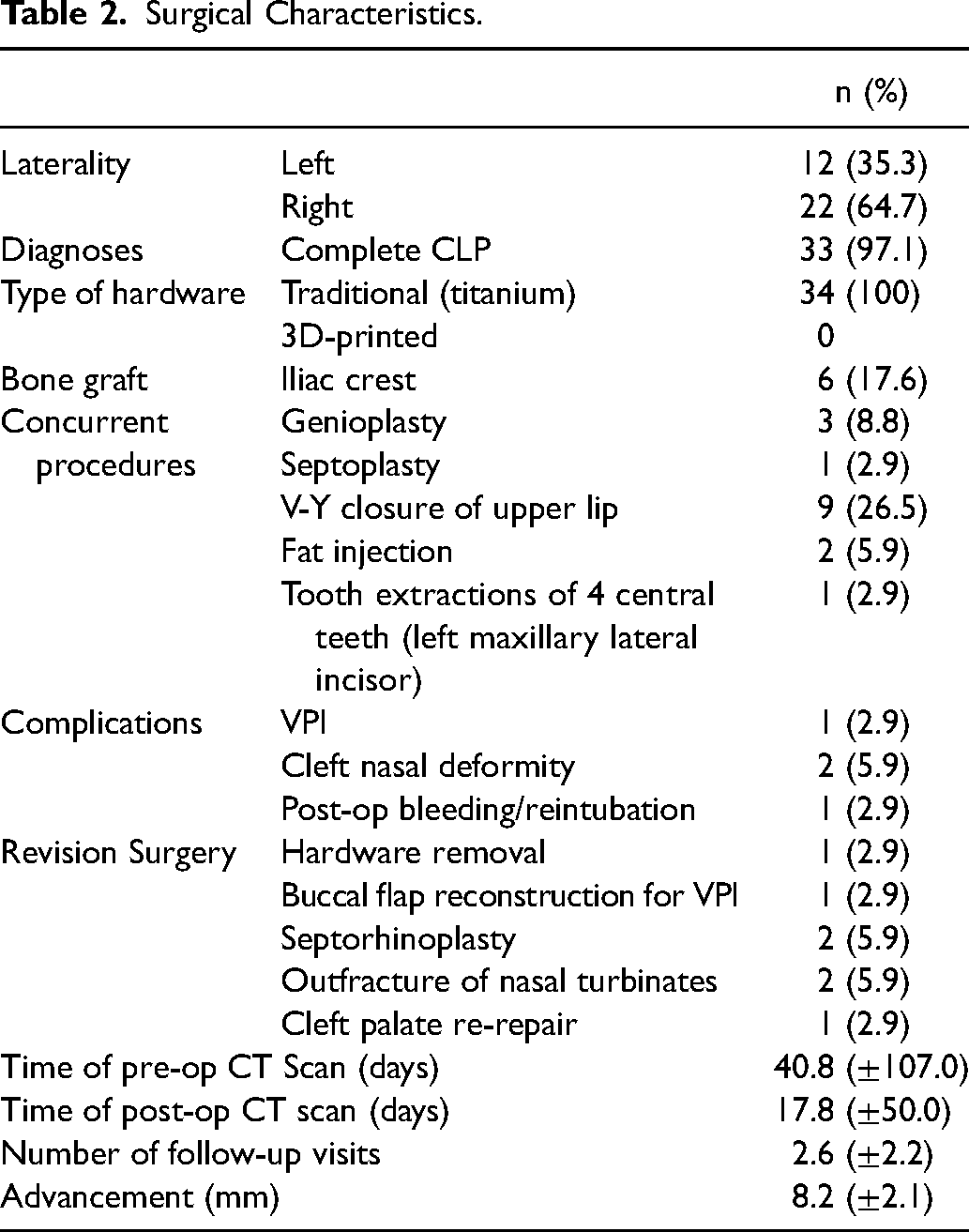
A total of 63 patients with non-syndromic cleft lip and palate who received a single-piece LeFort I osteotomy between the year 2013 and 2020 were identified. Twenty-eight patients with bilateral cleft lip and palate were excluded. An additional patient was excluded because they underwent a rhinoplasty at the same time as the LeFort I procedure, leaving 34 final participants. The study cohort consisted of 26 males and 8 females who possessed 12 left-sided clefts and 22 right-sided clefts. The average age at the time of surgery was 20.13 years (95% CI 12.50–27.73) (Table 1). Post-operative CBCT scans were performed an average of 17.79 days but no more than 1 year after surgery (Table 2). On average, patients attended 2.6 follow-up visits.
Patient Characteristics.
Surgical Characteristics.
Location of Osteotomy
The intra-rater reliability for all study measurements was excellent (κ = 0.903, p < 0.001).
Intraoperative measurement of maxillary advancement was 8.20 mm (95% CI 4.00–12.40 mm). Only one (2.9%) of the osteotomies performed was found to be above the level of the superior alar crease. The average distance from the pyriform base to the superior alar crease was 12.17 mm (95% CI 4.00–20.34 mm) (Table 3). The average distance from the pyriform base to the origin of the inferior turbinate was 14.80 mm (95% CI 4.61–24.98 mm). The variance in the distance from the pyriform base to the inferior turbinate on the cleft side is 36.22mm2. The variance in that same measurement is significantly lower on the non-cleft side at 16.09 mm2.
Measurements of the Distances on Both the Cleft and non-Cleft Sides.
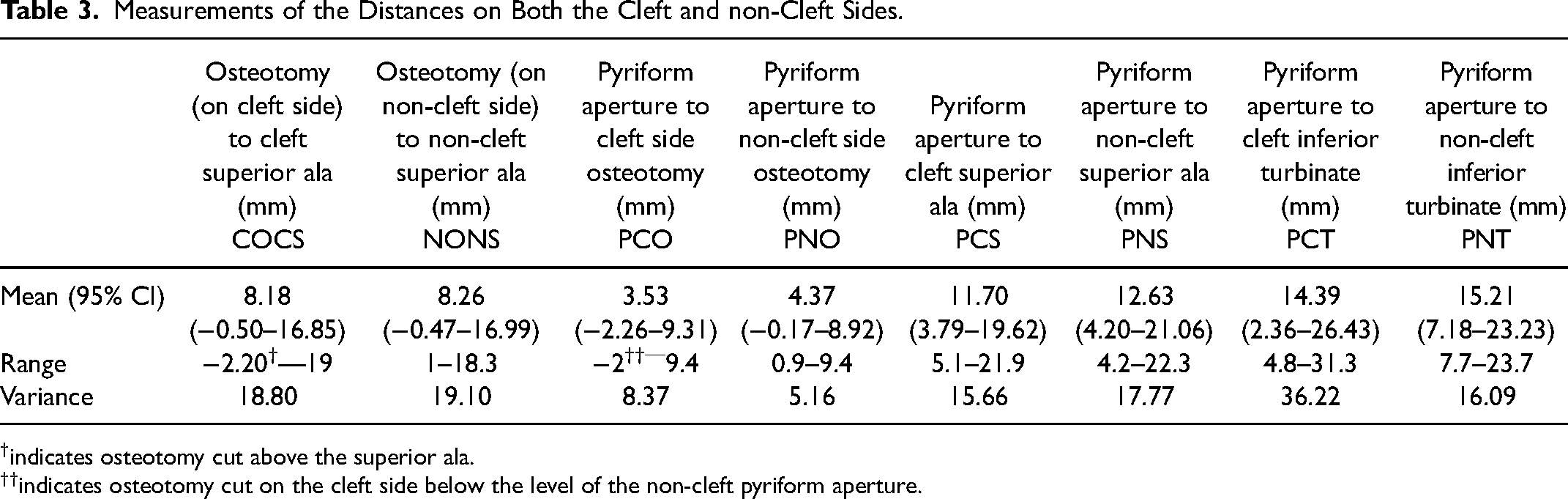
indicates osteotomy cut above the superior ala.
indicates osteotomy cut on the cleft side below the level of the non-cleft pyriform aperture.
On average, the origin of the inferior turbinate was located 2.83 mm (95% CI 1.45–4.20 mm) above the ipsilateral superior alar crease. On the cleft side, the inferior turbinates are above the level of the superior alar crease 73.53% (25/34) of the time. On the non-cleft side, the inferior turbinates are above the level of the superior alar crease 76.48% (26/34) of the time. Therefore, in approximately 75% of patients with unilateral CLP, a high osteotomy would be anatomically possible.
Discussion
A “high” Le Fort I osteotomy includes more of the upper maxilla to achieve better midface projection in patients with a cleft lip and palate and maxillary hypoplasia. In this study, the “high” Le Fort I osteotomy was defined as originating above the superior alar crease. To gauge the feasibility of performing such a “high” osteotomy, we measured the relationship between the osteotomy and the superior alar crease of the overlying soft tissue. In all but one osteotomy, the superior alar crease was found to be more superior than the Le Fort I osteotomy. Although uncommon in practice, in order to investigate the feasibility of performing our definition of a “high” Le Fort I osteotomy, we also measured the relationship of the inferior turbinate to the superior alar crease. On average, the superior alar crease was found to be inferior to the origin of the inferior turbinate, making our definition of a “high” osteotomy theoretically feasible.
Norholt et al. described a “high” Le Fort I osteotomy as one that includes portions of both the maxilla and zygomatic prominence, extending from the pyriform aperture to the canine fossa and then posteriorly to the infraorbital margin 3–4 mm below the orbital rim. 16 However, the height at which the cut should begin along the pyriform fossa was not specified. Rather, they suggested the height would depend on the extent of the deficiency. Strong et al. also included zygomatic involvement for a “high” LeFort I osteotomy but did not provide specifics either. Several studies utilize the term “high” Le Fort I osteotomy but fail to elaborate on what that procedure entails.8,14,17 Others have described “high” Le Fort osteotomies in cadaver studies using various skeletal landmarks such as the infraorbital foramen to define the location of the osteotomy, but none relate it to the pyriform aperture.16,18
From a technical perspective, the medial starting point and ultimately the height of the Le Fort I osteotomy is bounded by the bony inferior turbinate. Alternatively, the osteotomy could turn superiorly to include more of the maxilla; however, the thin bone of the anterior wall of the maxillary sinus makes such a maneuver treacherous. 16 Fracturing the anterior wall of the maxilla can disturb proper alignment and fixation of the Le Fort I osteotomy segment, and some surgeons posit that the zygomatic, not the anterior maxillary, portion of the cut is actually the most important aspect of the osteotomy for establishing facial symmetry and appropriate convexity.8,16 Furthermore, previous groups describing the “high” osteotomy depict the medial portion of the osteotomy as a straight line starting from the lateral nasal wall. 19 Thus, determining the precise height between the nasal floor and the inferior turbinate is critical to performing a “high” osteotomy.
You et al. simulated high Le Fort I osteotomies in cadaveric skulls from individuals who did not have orofacial clefts and found the “high” osteotomy was performed 10.3 mm (6.5 to 15 mm) above the nasal floor. 19 However, You's dry cadaveric skulls lacked soft tissue references, hindering their ability to measure the effect of a high osteotomy on the soft tissue of the midface. Moreover, patients with orofacial clefts have aberrant nasal anatomy that creates high inter- and intra-patient variability. This turbinate asymmetry and atypical nasal anatomy in patients with CLP have been demonstrated previously and are reflected in these large ranges and variances of turbinate heights in our study.20,21 In our cohort, the overall average height of the inferior turbinate was 15 mm, which falls within the range demonstrated by You et al., but, notably, the heights of our inferior turbinates also range from 4.8–31.3 mm on the cleft side and 7.7–23.7 mm on the non-cleft side. 19
This study is not without its limitations. This is a single center study with a limited cohort of patients. While this study demonstrated appropriate intra-rater reliability, there is still an element of subjectivity in choosing the points in three-dimensional space with which to base our measurements. Future studies should include more thorough evaluation of soft tissue changes after standard and “high” LeFort I osteotomies in addition to objectively measuring the heights of the osteotomies compared to the nasal floor. Additionally, the data in this study may not be transferable to patients with bilateral clefts and class III patients without a cleft. There are certainly advantages to a “high” osteotomy, especially in patients with orofacial clefts. 8 Achieving a “high” osteotomy, however, is only physically achievable approximately 75% of the time.
Conclusions
Reliably performing a “high” LeFort I osteotomy which includes the alar rim in patients with a unilateral cleft is physically achievable about 75% of the time but is often not clinically feasible due to variance in the vertical position of the inferior turbinate in relation to the alar.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.