
Abstract
Objective
We have used micro-computed tomography (CT) to elucidate the relationship between the muscle fibers in specimens with cleft palate. These findings could be useful for muscle reconstruction in cleft palate repair and to better understand cleft palate speech.
Design
Cadaveric anatomical study.
Participants
This study included three specimens with cleft palate
Intervention
The specimens were stained with phosphomolybdic acid and scanned by Micro-CT.
Main Outcome Measure(s)
The anatomy of the muscles.
Results
Using 2D projection images and 3D reconstruction models, subtle anatomical structures could be observed in the muscles. The attachment of the levator veli palatini (LVP) was not at the posterior edge of the hard palate or palatine aponeurosis (PA), but at the anterior 21.71-44.2% of the cleft edge. The palatopharyngeal (PP) was composed of two bundles: inferior and superior heads, which clasped the LVP. The uvularis was unevenly distributed, and located on both sides of the cleft edge, originating at the edge. The palatoglossus, superior constrictor of pharynx and anatomical structure around the pterygoid hamulus, were normal. The PA, PP and LVP were attached to the cleft edge from front to back, in that order. The position of the uvularis was not fixed.
Conclusions
With the help of Micro-CT technology, detailed anatomical features and the relationship between muscles could be visualized. In the specimen with cleft palate, muscles in the soft palate were associated with the pharyngeal muscles, which formed the 3D “velopharyngeal muscles complex.” These findings provide anatomical evidence for muscle reconstruction in cleft palate repair.
Introduction
The mechanism of speech production is very complex and involves the movement of multiple palatopharyngeal muscles. It is generally believed that velopharyngeal closure requires the cooperation of the contraction of the soft palate and the lateral and posterior pharyngeal walls. However, in cleft palate the muscles in the soft palate are congenital nonunion, leading to abnormal muscle movements and abnormal speech production. 1 Thus, studying the anatomy of these muscles in patients with cleft palate may guide muscle reconstruction in palatoplasty, help understand cleft palate speech and guide speech training after an operation.
Previous studies have evaluated the velopharyngeal musculature in children with cleft palate.2–13 MRI was used to show that the tensor veli palatini (TVP) muscle lacked continuity and its position was different from that in the non-cleft.3,10 Participants with cleft palate showed smaller and shorter TVP muscle, when compared with the non-cleft. 3 Also, the TVP muscle inserted at the posterior-lateral edge of the palatal cleft. 8
The volume of levator veli palatini (LVP) in infants with cleft palate has been found to be similar to that of the non-cleft. 5 Some studies have demonstrated that individuals with a history of cleft palate display a shorter LVP.4,6,11 Patients with cleft palate have a range of muscle bundle lengths and distances between muscle origins and velar thickness.2,4 Further, thickness of the LVP and symmetry at the point of its insertion into the velum is different between cleft and non-cleft patients. 12
Nasopharyngoscopy has demonstrated hypoplasia of the uvularis in cleft palate,4,7 and the uvularis was hypoplastic or absent in children with cleft palate.4,7,13 In the cleft condition, aponeurosis was dislocated and morphologically abnormal, but not absent. 9
To our knowledge, although several reports have dealt with the muscle bundles of the soft palate, no reports are available on muscle fibers in cleft palate. The effectiveness of cleft palate repair methods is still disputed, in part due to the lack of detailed knowledge of the anatomy of the cleft palate. 14 Indeed, detailed knowledge of the origin, insertion and relationship between muscle fibers in the cleft palate is essential for improving surgical techniques.
Materials and Methods
Our study included three fresh cadaveric heads acquired from aborted fetuses diagnosed with cleft palate, but with no other history of craniofacial deformities. One was a 28-week cleft of the soft and palate, up to the incisive foramen. Another was a 24-week cleft of the soft and hard palate, extending unilaterally through the alveolus. The third was a 22-week cleft of the soft and hard palate, extending bilaterally through the alveolus. The cadavers were donated to the [anonymized] Union Medical College for educational and research purposes. The present study is fully compliant with the laws in China, and was approved by the Ethical Institutional Committee of our hospital.
Sample Staining
Specimens were cut between the plane of the orbital floor and the plane of the oral floor, including tongue, palate and upper part of the pharynx. The tissue was soaked in 4% formaldehyde solution for 8 h before immersion in 3% phosphomolybdic acid solution for 14 days. Samples were removed and washed with 75% ethanol to remove excess solution attached on the surface.
Computed Tomographic Scanning
Histologically, iodine accumulates in the muscle fibers rather than in the connective tissues. This enables the detailed visualization of the muscle fibers on CT scan. 15 The Micro-CT scanner used in the present study was provided by the Institute of Laboratory Animal Science (phoenix v | tome | x s; GE Sensing & Inspection Technologies GmbH, Wunstorf, Germany). The sample was scanned using the following parameters: 60 kV, 400 μA, 400 views, 360-degree total rotation, 1156 s continuous rotation scan times and 800 ms exposure time per projection.
3D Model Reconstruction
The obtained images were saved in Digital Imaging and Communications in Medicine formats. All the images showed a contrast between connective tissues and muscle fibers. Afterward, all files were imported into Mimics (Mimics 20.0 × 64; Materialise NV) to reconstruct a 3D model of the muscles and palatine aponeurosis (PA). In Mimics, we established masks of various colors for different muscles and tendons. The threshold interval was defined as 2861-2861 Hounsfield units when a new mask was defined. Then, the “mask editing” function was used, and with manual editing the muscle fibers in the 2D slice plane were drawn according to the direction and origin of the fibers, using the same color for fibers with the same direction and source. To obtain 3D models of velopharyngeal muscles, the edited radiographs were gathered and stacked together using a 3D Calculate function.
Results
The 3D models intuitively show the morphology and spatial relationship between velopharyngeal muscles in cleft palate (Figures 1–3). The illustration of the cleft palatal muscular architecture is drawn for clarity (Figure 4). The more severe the cleft palate, the worse is the muscle development. Muscles in palate and pharynx were closely connected. The inferior and superior heads of the palatopharyngeus (PP) clasped the levator veli palatini (LVP) in the middle. The tensor veli palatini (TVP) extended to the PA after bypassing the pterygoid hamulus, which connected with the superior constrictor of the pharynx (SC) and the PP. The PA was thin and overlayed with the anterior end of the PP. The PA, PP and LVP were found at the cleft edge, from anterior to posterior position. Lastly, the origin of uvularis was not fixed and had a nonuniform distribution in the two sides of the cleft.
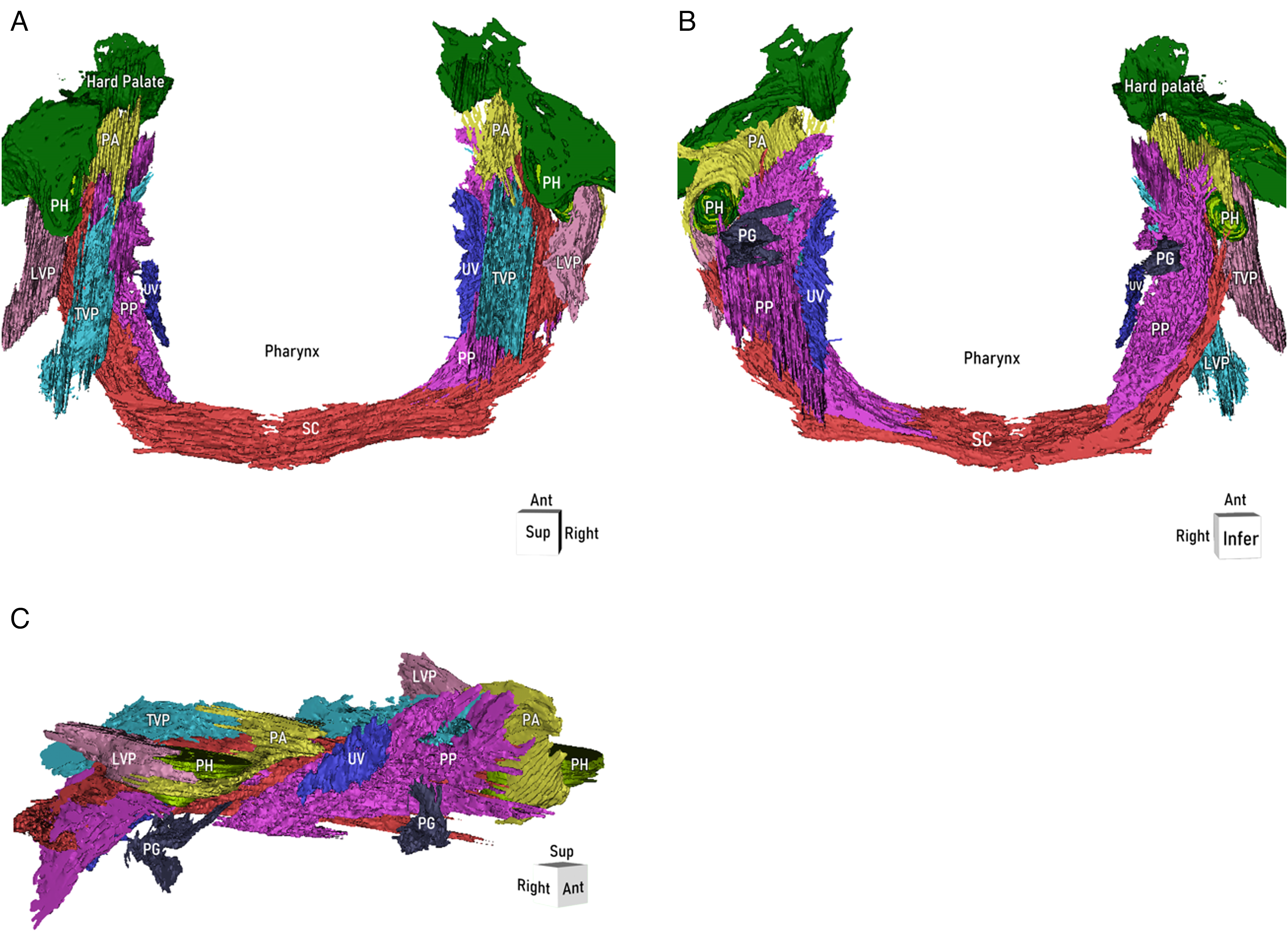
Three-dimensional model of the palatopharyngeal muscles in the clefts of the soft and hard palate extending bilaterally through alveolus, which demonstrating the spatial relationship between them. Green lines depict the posterior part of the hard palate. Purple lines depict the muscle fibers of the palatophrayngeus (PP). Light blue lines depict the muscle fibers of the levator veli palatini (LVP). Deep blue lines depict the muscle fibers of the uvularis. Pink lines depict the muscle fibers of the tensor veli palatini (TVP). Gray lines depict the muscle fibers of the palatoglossus. Red lines depict the muscle fibers of the superior constrictor of pharynx (SC). Yellow lines depict the palatine aponeurosis. (A) Bottom view of the three-dimensional model. (B) Superior view of the three-dimensional model. (C) 45° side view of the three-dimensional model on the right side. PP, palatophrayngeus; LVP, levator veli palatini; UV, uvula; TVP, tensor veli palatini; PA, palate aponeurosis; SC, superior constrictor; PH, pterygoid hamulus; PG, palatoglossus; Ant: anterior; Post: posterior; Sup: superior; Infer: inferior.
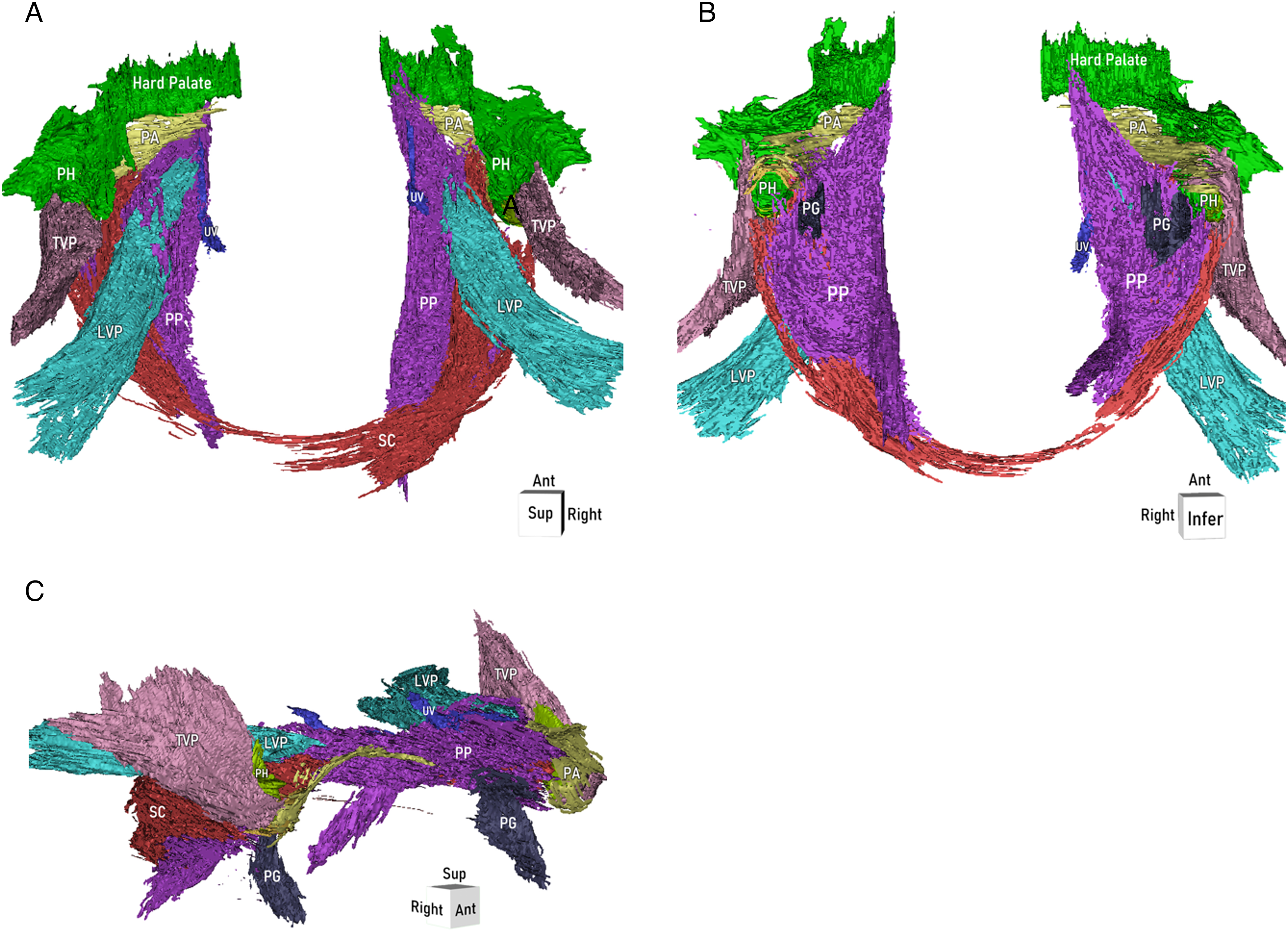
Three-dimensional model of the palatopharyngeal muscles in the clefts of the soft and hard palate extending unilaterally through alveolus, which demonstrating the spatial relationship between them. Green lines depict the posterior part of the hard palate. Purple lines depict the muscle fibers of the palatophrayngeus (PP). Light blue lines depict the muscle fibers of the levator veli palatini (LVP). Deep blue lines depict the muscle fibers of the uvularis. Pink lines depict the muscle fibers of the tensor veli palatini (TVP). Gray lines depict the muscle fibers of the palatoglossus. Red lines depict the muscle fibers of the superior constrictor of pharynx (SC). Yellow lines depict the palatine aponeurosis. (A) Bottom view of the three-dimensional model. (B) Superior view of the three-dimensional model. (C) 45° side view of the three-dimensional model on the right side. PP, palatophrayngeus; LVP, levator veli palatini; UV, uvula; TVP, tensor veli palatini; PA, palate aponeurosis; SC, superior constrictor; PH, pterygoid hamulus; PG, palatoglossus; Ant: anterior; Post: posterior; Sup: superior; Infer: inferior.
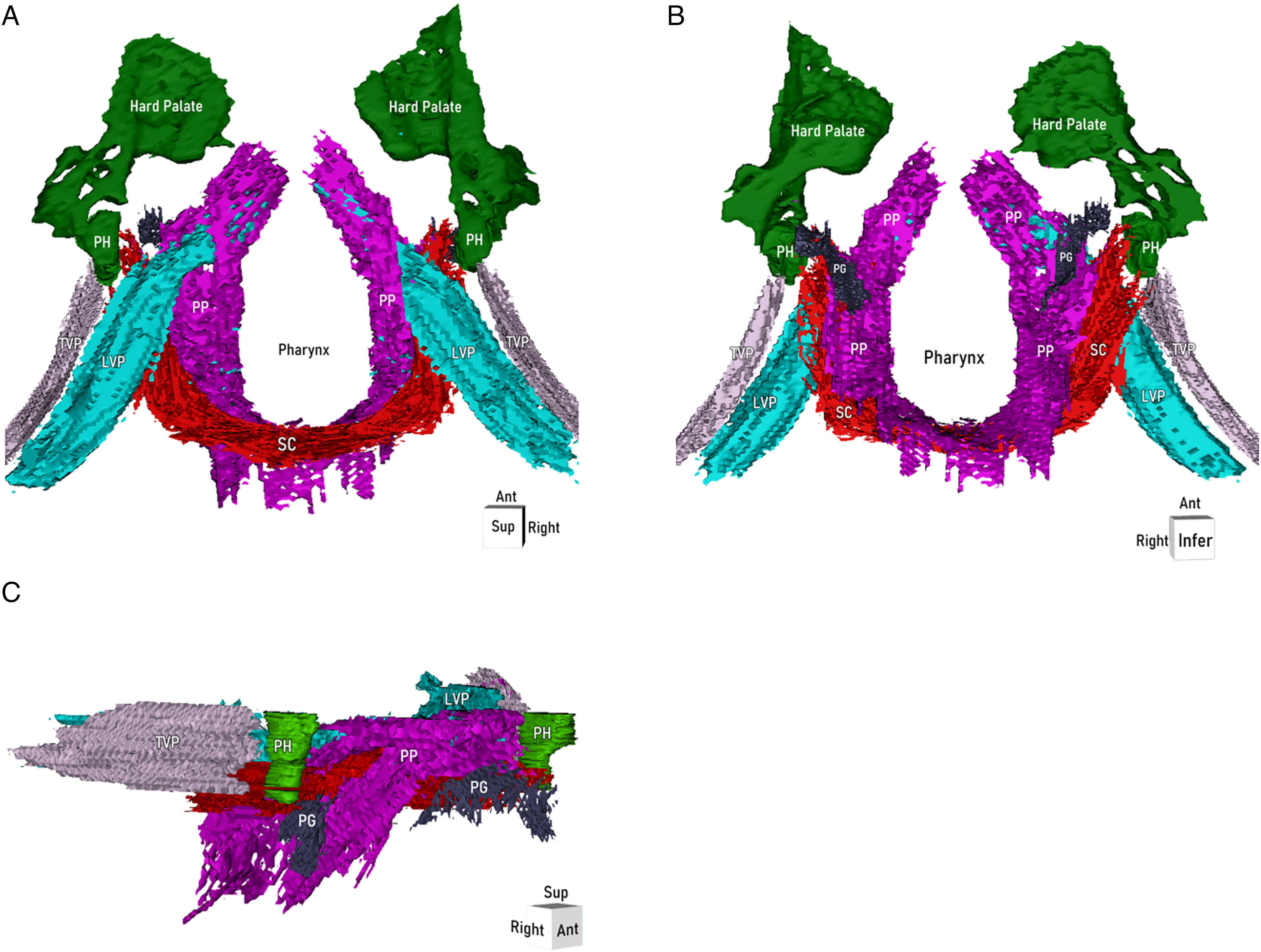
Three-dimensional model of the palatopharyngeal muscles in the clefts of the soft and hard palate, up to the incisive foramen, which demonstrating the spatial relationship between them. Green lines depict the posterior part of the hard palate. Purple lines depict the muscle fibers of the palatophrayngeus (PP). Light blue lines depict the muscle fibers of the levator veli palatini (LVP). Pink lines depict the muscle fibers of the tensor veli palatini (TVP). Gray lines depict the muscle fibers of the palatoglossus. Red lines depict the muscle fibers of the superior constrictor of pharynx (SC). (A) Bottom view of the three-dimensional model. (B) Superior view of the three-dimensional model. (C) 45° side view of the three-dimensional model on the right side. PP, palatophrayngeus; LVP, levator veli palatini; TVP, tensor veli palatini; SC, superior constrictor; PH, pterygoid hamulus; PG, palatoglossus; Ant: anterior; Post: posterior; Sup: superior; Infer: inferior.
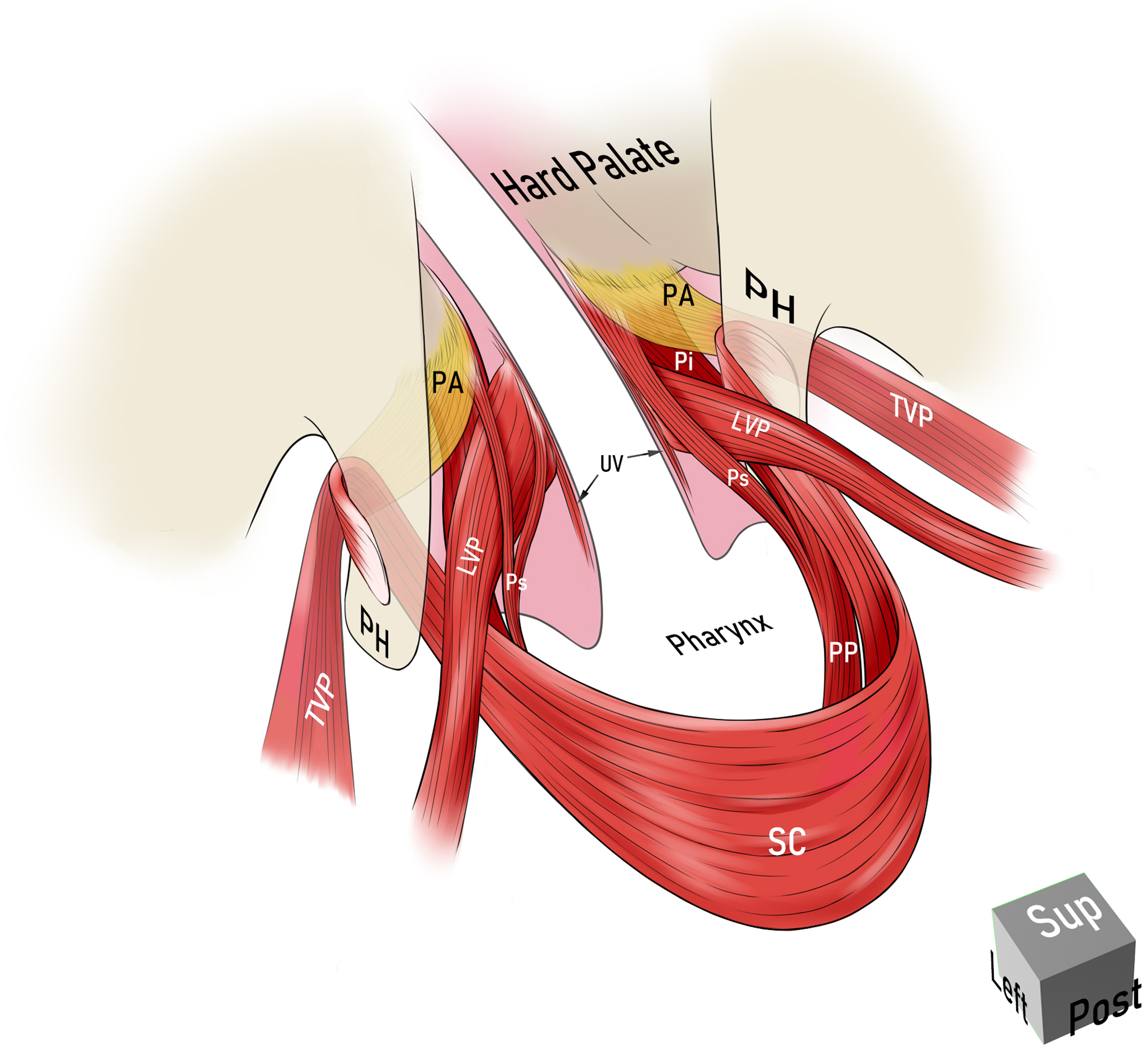
Illustration of the velopharyngeal muscles in the cleft palate showing the spatial relationship between them. The figure shows the posterolateral view of the soft palate on the left side. Pp, the posterior head of the PP; LVP, levator veli palatini; SC, superior pharyngeal constrictor. Illustration of the palatal muscular architecture showing the spatial relationship between the muscles in the clefts of the soft and hard palate extending unilaterally through alveolus. The figure shows the view of the soft palate on the left rear. PP, palatophrayngeus; Ps, the superior head of the palatopharyngeus; Pi, the inferior head of the PP; LVP, levator veli palatini; TVP, tensor veli palatini; SC, superior constrictor; PA, palate aponeurosis; UV, uvula; PH, pterygoid hamulus; Ant: anterior; Post: posterior; Sup: superior.
Clefts of the soft and hard palate, extending bilaterally through the alveolus (Figure 1)
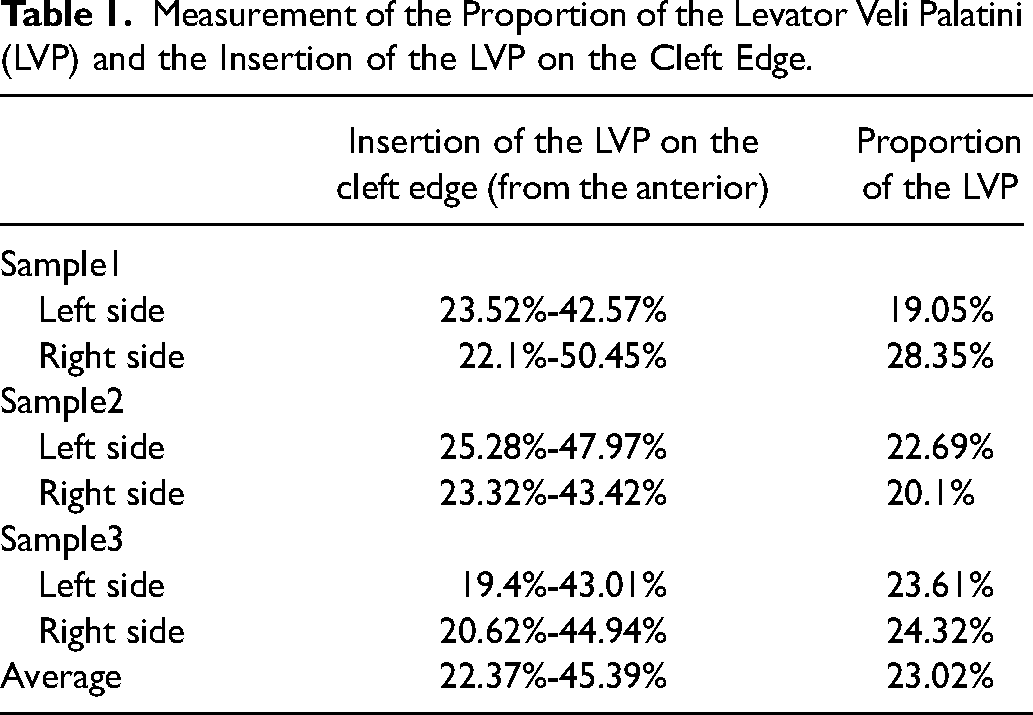
The LVP came from the lateral superior position and reached the cleft edge. The LVP did not join the contralateral side in the middle of the soft palate. The attachment of the LVP did not reach the hard palate and was located at about the anterior one third of the soft tissue edge. The LVP accounted for about one fourth of the length of the soft palate. Specifically, the range of the LVP on the left side stopped at the soft edge and was located at anterior 25.28-47.97% of the anterior portion of the cleft edge. The length of the LVP on the left side accounted for 22.69% of the length of the soft palate at the cleft edge, i.e., from the posterior edge of the hard palate to the end of the soft palate. The range of the LVP on the right side also stopped at the cleft edge and was located at 23.32-43.42% of the anterior portion of the cleft edge. The LVP on the right side accounted for 20.1% of the length of the soft palate at the cleft edge (Table 1). The anatomy of LVP on both sides was similar.
Measurement of the Proportion of the Levator Veli Palatini (LVP) and the Insertion of the LVP on the Cleft Edge.
PP originated from the posterior edge of the hard palate and the edge of the cleft, and ran posteriorly along the cleft edge. It is distributed in the soft palate and pharyngeal wall, being the largest muscle connecting the soft palate and pharynx. The PP was divided into two bundles according to its position, which grasped the LVP in the middle. The inferior head was thin and originated from the margin of the cleft edge and the posterior edge of the hard palate, located in the oral surface of the LVP. It went along the fissure edge to the pharyngeal wall. The superior head was relatively slender and originated from the cleft edge and the posterior edge of the hard palate, located in the nasal surface of the LVP. The two bundles of PP intersected and fused in the anterior and posterior LVP, and moved posteriorly to the lateral pharyngeal wall. Some muscle fibers are also distributed in the posterior pharyngeal wall. At the margin of the cleft, the PP extended from the posterior margin of the hard palate to the pharynx, which covered the anterior and posterior parts of the LVP.
The TVP originated at the base of the skull and passed downwards. It then bypassed the pterygoid hamulus and extended into the PA. The latter was very weak and attached to the posterior edge of the hard palate. The PA was located at the nasal surface of the muscles in the soft palate, covering the PP. It connected with some muscle fibers of SC and PP on the medial side of the pterygoid hamulus. Some muscle fibers of SC were attached to the pterygoid hamulus, forming a unit. There was a clear gap between the PA and pterygoid hamulus, forming a pulley-like structure (Figure 5).
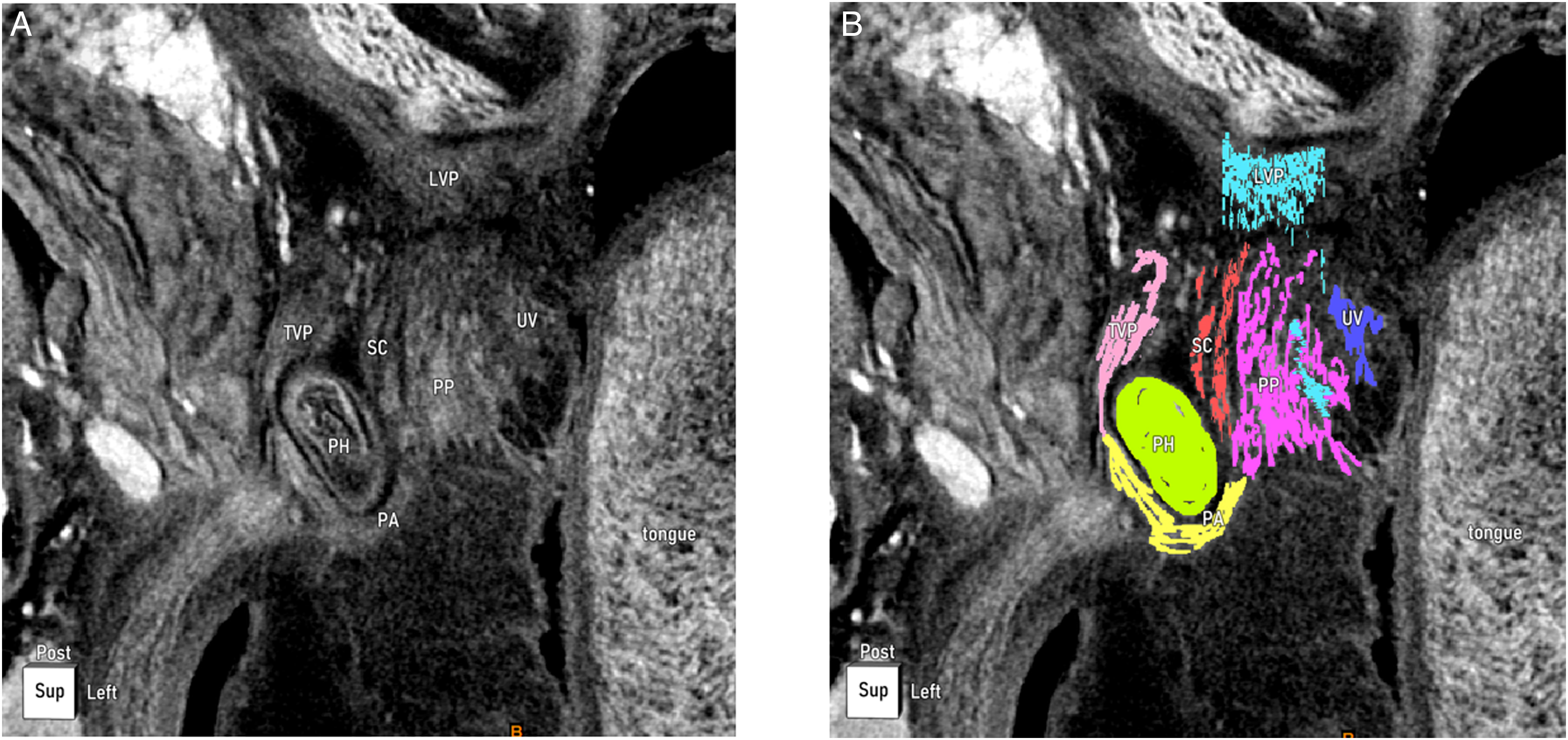
Photographs from the horizontal plane on the lateral side demonstrating the delicate anatomy around the left pterygoid hamulus. The tensor veli palatini (TVP) extends to the aponeurosis and bypasses the hamulus to form the palatine aponeurosis, which connected the palatopharyngeus (PP) and the superior constrictor (SC). There was a distinct gap between the palatine aponeurosis and the pterygoid hamulus. The left is the two-dimensional projection graph and the right is the edited two-dimensional plane in Mimics. The green color depicts the pterygoid hamulus. The pink, yellow, red, and purple lines depict the tensor veli palatini, palatine aponeurosis, muscle fibers of the SC, and muscle fibers of the PP, respectively. PP, palatopharyngeus; PA, palate aponeurosis; SC, superior constrictor; PH, pterygoid hamulus; LVP, levator veli palatini; Post: posterior.
The uvularis was very weak and distributed on both sides of the cleft edge. The volume and length of the muscle fibers on the two sides showed differences. The uvularis originated from the cleft edge and PA, but origin position was different at the two sides. Then it traveled posteriorly along the medial side of the cleft edge and attachment on the two sides was not symmetrical.
The palatoglossus was very slender and originated from the inferior head of the PP. It passed down and ended laterally at the base of the tongue, forming the palatoglossus arch.
The SC was similar in shape to a semicircle, wrapping around the lateral side of the PP and forming the lateral and posterior pharyngeal wall. Some SC muscle fibers wrapped around the pterygoid hamulus, forming a unit with the hamulus. Some muscle fibers were attached to the PA on the medial side of the pterygoid hamulus.
Clefts of the soft and hard palate, extending unilaterally through the alveolus (Figure 2)
The anatomy of LVP was similar to the clefts of the soft and hard palate, extending bilaterally through the alveolus cleft palate, moving downward from the lateral superior direction and stopping at the cleft edge. The LVP on the left side stopped at the cleft edge, and was located in the anterior portion, 23.52-42.57%, of the cleft edge. The length of the LVP on the left side occupied 19.05% of the length of the soft palate. The LVP on the right side also stopped at the cleft edge, and was located at a portion 22.1-50.45% of the anterior portion of the cleft edge. The LVP on the right side accounted for 28.35% of the length of the soft palate at the cleft edge (Table 1).
The PP was divided into inferior and superior heads, grasping the LVP in the middle. The posterior head was not distinguished. The cleft side and the non-cleft side of the inferior head were similar, relatively thick, located in the oral surface of the LVP. It originated from the fissure, PA and the posterior edge of the hard palate, going along the fissure to the lateral pharyngeal wall. The superior head was located on the nasal surface of the LVP. The superior head of the cleft side was similar to the clefts of the soft and hard palate, extending bilaterally through the alveolus. It originated from the cleft edge of the posterior hard palate and fused with the inferior head in anterior and posterior of the LVP. Some muscle fibers of the superior head on the non-cleft side attached to the PA anteriorly, and some muscle fibers originated from the posterior edge of the hard palate, PA and the fissure anteriorly. Then it walked posteriorly along the cleft edge.
The anatomy of TVP, uvularis, palatoglossus, SC and pterygoid hamulus was similar to the clefts of the soft and hard palate, extending bilaterally through the alveolus.
Clefts of the soft and hard palate, up to the incisive foramen (Figure 3)
The LVP was similar to the above two types, which were attached at the fissure. The attachment of LVP did not reach the posterior edge of the hard palate. The LVP on the left side stopped at the cleft edge and was located at a position 19.4-43.01% from the anterior portion of the cleft edge. The length of the LVP on the left side occupied 23.61% of the length of the soft palate. The LVP on the right side stopped at the cleft edge and was at anterior position, 20.62-44.94% from the cleft edge. The LVP on the right side accounted for 24.32% of the length of the soft palate at the cleft edge (Table 1).
The PP was similar to the clefts of the soft and hard palate, extending bilaterally through alveolus. The anatomical relationship between the TVP, PA and the pterygoid hamulus was not observed because the PA did not stain. In this specimen, the uvularis was not visible, possibly due to poor staining.
Discussion
Phosphomolybdic acid accumulates more in muscle fibers and tendons than in connective tissue, which can be observed in the CT scans. 15 Detailed muscle fibers could be visualized by this method. Our team used similar methods satisfactorily to study the nasolabial muscles and the muscles at the corner of the mouth.16–20 In this study, we scanned four cadaveric specimens with cleft palate by Micro-CT. Fine anatomical features and the relationship between muscles were observed in the images and 3-D models. This was essential for muscle movement during speech production and to improve the cleft palate surgery technique.
The main purpose of cleft palate repair is to close the cleft and restore muscle function. This may be helpful to restore normal speech and swallowing, minimizing at the same time the impact on the function of the eustachian tube. 21 At present, a variety of surgical techniques are performed to repair the cleft palate,22–23 but it is difficult to decide which one is optimal. At present, there is a lack of research on the anatomy of palatopharyngeal muscle fibers in cleft palate. This causes blind spots in the knowledge required for muscle reconstruction during surgery, and no standard muscle reconstruction protocol has been accepted. Herein we report previously undescribed anatomical features of cleft palate, providing an anatomic basis for improving cleft palate surgery.
Anatomical Characteristics of the PP and LVP
The LVP originated from the petrosal bone, with some muscle fibers connecting to the eustachian tube cartilage by the fascia. The LVP traveled from the superolateral direction obliquely to the median line to meet the contralateral part, which occupied the middle 34-39.8% of the soft palate.24–26 The LVP plays a key role in velopharyngeal closure, causing the uplift of the middle soft palate and maintaining the movement of the uvularis during contraction. 27 It is generally believed that the reconstruction of LVP should be emphasized in cleft palate repair. Based on our study, the termination of LVP was located at the anterior 22.37-45.39% of the cleft edge in soft palate, not the posterior edge of the hard palate or the PA. The length of the LVP in the cleft edge accounted for 23.02% of the soft palate. Therefore, the LVP can be found in the anterior 1/3 of the soft palate during surgery, rather than in the posterior margin of the hard palate. After separating part of the LVP, the broken ends should be sutured to reconstruct the normal anatomy and to restore function.
It has been reported that the PP originated from the posterior margin of the thyroid cartilage and the lateral wall of the pharynx, which traveled superiorly into the soft palate.24,25 Based on our previous research, the PP was divided into three bundles by the LVP: inferior, superior and posterior head. 26 The inferior head was the widest, and was located on the oral surface of the LVP, attaching to the posterior margin of the hard palate, palatal aponeurosis and soft palate. The superior head was very thin and located on the nasal surface of the LVP, attaching to the PA and surrounding mucous membranes. The posterior head was also thin, laid behind the LVP and was attached to the LVP and uvularis. 26
In the present study, the PP was divided into superior and inferior heads, but the posterior one could not be observed in cleft palate. These two heads clasped the LVP, converging anteriorly and posteriorly to the LVP. Then these two heads went along the cleft edge to the lateral pharyngeal wall, with a small amount of muscle fibers distributed in the posterior pharyngeal wall. The inferior head was located on the oral surface of the LVP and was anteriorly attached to the PA, posterior margin of the hard palate and cleft edge. The superior head of the cleft side was attached to the PA, the posterior margin of the hard palate and the cleft edge anteriorly. The non-cleft side had few muscle fibers attached to the PA anteriorly, and some muscle fibers originated from the posterior edge of the hard palate, PA and the cleft edge. Previously, we found that the inferior head of the PP accounted for about one third of the anterior portion of the soft palate at the midline, whereas the posterior head of the PP accounted about one third of the posterior portion of the soft palate. 26 The PP was the largest muscle connecting the soft palate and the pharynx. The PP antagonized the LVP, restricting excessive lifting of the soft palate, but was also able to synergize with it to lift the soft palate. At the same time, the superior head of the PP can limit the excessive lifting of the LVP. The PP could elevate the pharyngeal wall and move the lateral pharyngeal wall toward the midline by the combined action of the superior pharyngeal constrictor, which plays an important role in velopharyngeal closure.26,28 Therefore, one should pay attention to the reconstruction of the PP during surgery. The latter should be removed from the ectopic insertion point and placed in its normal position.
In specimens with cleft palate, the PP was closely associated with the LVP. The inferior and superior heads of the PP were located on the oral and nasal surfaces of the palatopharyngeal muscle, respectively, which clasped the LVP in the middle. The PP and LVP were the most important muscles in the soft palate. They were closely connected and coordinated to play a major role in lifting the soft palate. 26 Their anatomical relationship should be restored as much as possible during surgery. Herein we found that the PP was ectopically attached to the posterior edge of the hard palate and ran along the cleft edge, whereas the LVP came from the outer upper part and ended at about the anterior one third of the cleft edge, located between the inferior and superior heads of the PP. This could help fast identification of PP and LVP during surgery. Anatomical separation is then carried out to reconstruct their spatial relationship.
Anatomical Characteristics of the Uvularis, Palatoglossus and SC
The uvularis was located in the middle of the soft palate, on the nasal surface of the LVP, which was the uppermost muscle of the soft palate. It originated from the PA, surrounded the soft tissue anteriorly, and did not reach the posterior edge of the hard palate. It ran posteriorly at the midline of the soft palate and terminated at the middle of the cleft edge. 29 Previous studies using nasopharyngoscopy demonstrated absence or hypoplasia of the uvularis in individuals with cleft palate.4,7 Schenck et al. observed absence of the uvularis in 4 participants with cleft palate from the oblique coronal MR images. 4 Uvularis fibers in cleft palate were very thin and distributed non-uniformly on the two sides of the cleft. The uvularis originated from the cleft, but not always at the same position; sometimes stopped at the front section, and others at the middle of the soft palate. Therefore, it is difficult to find and restore the anatomy of the uvularis, which can be retained in the nasal mucosa and sutured in position.
The palatoglossus originated from the inferior head of the PP, moved down to the lateral base of the tongue, and was covered by the mucous membrane to form the palatoglossus arch. The SC was a semicircular muscle that enclosed the posterior and lateral walls of the pharynx, and originated at the posterior edge of the medial pterygoid plate and the posterior end of the mylohyoid line. The SC moved inward and posteriorly along the pharyngeal wall and intersected with PP on the lateral pharyngeal wall, forming the lateral and posterior walls of the velopharyngeal portal. Then it traveled to the posterior pharyngeal wall and joined the contralateral muscle tract in the midline.28,30 During surgery, the muscles in the pharynx should be protected. Excessive dissection may cause scar and disrupt blood supply, which in turn may affect the movement of the soft palate and pharyngeal walls.
The Relationship Between the Muscles
The TVP originated from the base of the medial pterygoid plate and the eustachian tube cartilage, and passed straight downward to form the PA after passing the pterygoid hamulus. The PA fanned out toward the midline, continuing with the contralateral aponeurosis.24,25,31 In a previous study, we found that the PA was attached to some muscle fibers of the SC and PP instead of the medial side of the pterygoid hamulus. The muscle fibers of the SC were attached to the pterygoid hamulus by a tendon, which formed a unit. There was a gap between this unit and the PA, forming a pulley-like structure.31,32 The latter studies showed that the anatomy around the pterygoid hamulus of the cleft palate was similar to that observed in non-cleft individuals. There was a gap between the SC and PP on the medial side of the pterygoid hamulus. During surgery, damage to this area should be minimized by blunt separation of the space between SC and PP. The PP can be further pushed inward to reduce the tension of closure.
Koch et al. found that the aponeurosis inserted on the posterolateral edge of the hard palate after coursing around the pterygoid hamulus. 9 In our study, we found that the TVP bypassed the pterygoid hamulus to form the PA, and connected with some muscle fibers of the SC and PP. This resulted in a connection between the palatal and pharyngeal muscles. The LVP was clasped by the two heads of PP, which formed a unit closely coordinated with soft palate movements. These findings suggest that the muscles of the soft palate are closely related to those in the pharynx. The movement of the soft palate is not independent, but is coordinated with the movement of the lateral and posterior pharynx walls. Therefore, we believe that the palatopharyngeal muscles constitute a complex.
Limitations
Since this study only featured three specimens, further studies should include a larger sample size. Also, specimens were slightly deformed during preparation and staining, which was corrected by using diagrams.In the clefts of the soft and hard palate, up to the incisive foramen, the uvularis was not visible. The uvularis in cleft palate was very thin and located in the middle of the soft palate, which possibly led to poor staining. Researchers were not blind to the diagnosis, and we could not provide evidence for the sliding properties of the pulley-like structure in the area of the pterygoid hamulus. Thus, future studies should be performed on the biomechanical action of the muscles around the hamulus.
Conclusions
Our study reveals previously unreported elaborate anatomical features of the velopharyngeal muscles in the cleft palate, providing an anatomical basis for improving cleft palate surgery techniques. The LVP was attached 21.71-44.2% from the anterior portion of the cleft edge. This provides a guide for positioning the LVP during surgery. The PP is divided into inferior and superior heads, which are located on the oral and nasal surfaces of the LVP, respectively. These two heads both attach to the PA, the posterior margin of the hard palate, and the cleft margin anteriorly. The PP is closely related to the LVP, which plays an essential role in soft palate movement. This anatomical relationship should be protected and reconstructed during surgery. The uvularis is located on both sides of the cleft, which originates from the fissure edge. The uvularis was dysplastic and unevenly distributed, which is difficult to dissect intraoperatively. Palatoglossus muscle, pharyngeal muscle and the anatomical structure around the pterygoid hamulus were normal, which suggests that palatoglossus and pharyngeal muscle, and also the PA and the pterygoid hamulus, should be protected during surgery to minimize damage. The palatal muscles and pharyngeal muscles formed a muscle complex.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant No.81971853).