
Abstract
Objective
To assess a three-dimensional stereophotogrammetric method for palatal cast digitization of children with unilateral cleft lip and palate.
Design
As part of a collaboration between the University of Milan (Italy) and the University CES of Medellin (Colombia), 96 palatal cast models obtained from neonatal patients with unilateral cleft lip and palate were obtained and digitized using a three-dimensional stereophotogrammetric imaging system.
Main Outcome Measures
Three-dimensional measurements (cleft width, depth, length) were made separately for the longer and shorter cleft segments on the digital dental cast surface between landmarks, previously marked. Seven linear measurements were computed. Systematic and random errors between operators' tracings, and accuracy on geometric objects of known size were calculated. In addition, mean measurements from three-dimensional stereophotographs were compared statistically with those from direct anthropometry.
Results
The three-dimensional method presented good accuracy error (<0.9%) on measuring geometric objects. No systematic errors between operators' measurements were found (p > .05). Statistically significant differences (p < 5%) were noted for different methods (caliper versus stereophotogrammetry) for almost all distances analyzed, with mean absolute difference values ranging between 0.22 and 3.41 mm. Therefore, rates for the technical error of measurement and relative error magnitude were scored as moderate for Ag-Am and poor for Ag-Pg and Am-Pm distances. Generally, caliper values were larger than three-dimensional stereophotogrammetric values.
Conclusions
Three-dimensional stereophotogrammetric systems have some advantages over direct anthropometry, and therefore the method could be sufficiently precise and accurate on palatal cast digitization with unilateral cleft lip and palate. This would be useful for clinical analyses in maxillofacial, plastic, and aesthetic surgery.
Cleft lip and palate (CLP) represents the most frequent congenital malformation of the head and neck. Although the treatment of children with CLP has improved over the years, deficient growth of the maxilla is still common. The reasons for abnormal facial morphology in treated cleft individuals may involve two factors: intrinsic developmental deficiency or iatrogenic factors introduced by treatment (Oberoi et al., 2008).
Treatment of children with complete unilateral CLP (UCLP) can be achieved with diverse protocols (LaRossa, 2000; Rohrich et al., 2000; Kulewicz and Dudkiewicz, 2010). All protocols involve various surgical techniques with different considerations such as patient age; sequence of lip, soft palate, and hard palate closure; and treatment with presurgical maxillary orthopedics and orthodontics (Kulewicz and Dudkiewicz, 2010). Several papers have investigated craniofacial morphology in children with cleft disorders (Prahl et al., 2001; Yamada et al., 2003; Bugaighis et al., 2010; Gursoy et al., 2010). In particular, quantitative analyses of palatal morphology before, during, and at the end of the treatment are necessary to better appreciate the actual effect of the various protocols (Prahl et al., 2001; Yamada et al., 2003; Kulewicz and Dudkiewicz, 2010).
The palate and its three-dimensional (3D) reproductions with stone casts are complex structures that cannot be analyzed easily with conventional two-dimensional methods (photographs, radiographs) (Ferrario et al., 1998; Restrepo et al., 2008). The problem is particularly important for CLP patients, where the quantitative assessment of the depth of the cleft can be better done with 3D imaging methods (Braumann et al., 1999; Baek and Son, 2006; Restrepo et al., 2008; Boldt et al., 2009). Previous investigations used methods like the reflex microscope (Prahl et al., 2001; Krey et al., 2009), magnetic resonance imaging (Benacerraf et al., 2006), or contact digitizers (Ferrario et al., 1998; Yamada et al., 2003; Restrepo et al., 2008) to determine the 3D characteristics of cleft palates (Baek and Son, 2006; Proff et al., 2006). Although these methods were shown to be very accurate and to provide clinically relevant information, they all have several limitations, either requiring large and well-equipped measurement setups or providing only the 3D (x, y, z) coordinates of selected reference points, neglecting the surface characteristics of the palate.
Currently, palatal models of patients can be scanned by laser to obtain 3D virtual models that can be used to perform measurements needed for treatment planning (Baek and Son, 2006). Additionally, virtual models allow an easier communication between clinical areas and specialties due to the facility of sharing files. Biological structures can be scanned also by other optical instruments, like stereophotogrammetry, a method that is used most for the imaging of soft tissues (de Menezes et al., 2010; Rosati et al., 2010) but may be used efficaciously for stone casts also (Littlefield et al., 2005).
Although 3D virtual palatal models may be an advantageous tool in CLP patient analysis and planning, a necessary prerequisite is that measurements performed on these 3D virtual models are reliable and valid. Therefore, this study has the aim to assess a 3D stereophotogrammetric method for palatal cast digitization of children with UCLP. Data obtained with the 3D method will also be compared with conventional caliper measurements. In a first step, only conventional measurements of selected landmarks pairs will be made: The assessment of more complex information (surfaces, geodesic distances, angles) will be done only after demonstration of the suitability of stereophotogrammetry for simple palatal measurements.
Materials and Methods
Experimental Design
A total of 96 palatal cast models obtained from neonatal patients with UCLP attending the Fundación Clínica Noel de Medellín (Colombia) were analyzed. Palatal casts were collected during a clinical study performed to evaluate the 3D morphological effects of various treatments on the growing segments of dental arches of patients with UCLP.
The institutional ethics committee of the university CES approved this study.
Anatomical References (Landmarks) on Cleft Dental Casts
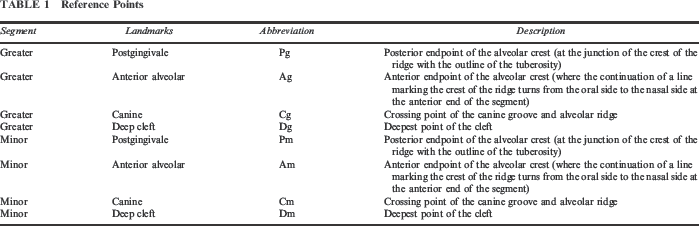
Before the digitization, landmarks were marked on each palatal cast. The anatomical reference landmarks assessed the two cleft segments separately. Landmarks were identified according to Prahl et al. (2001) and Yamada et al. (2003) (Table 1; Fig. 1).
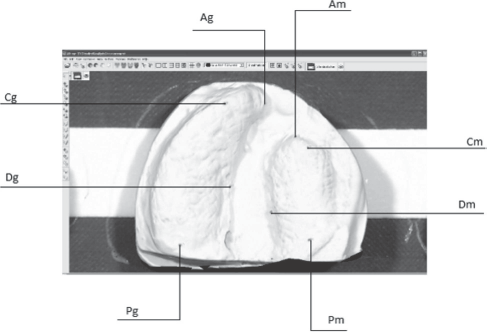
Landmark position.
Reference Points
Dental Cast Digitization
Using a commercial 3D stereophotogrammetry system (VECTRA-3D; Canfield Scientific, Inc., Fairfield, NJ), the palatal casts were digitized and the appropriate files were analyzed using the stereophotogrammetric software (de Menezes et al., 2010). The 3D coordinates of the selected landmarks were obtained. Overall, the 3D stereophotogrammetry system has already been found to assess the coordinates of soft tissue facial landmarks with good precision and reproducibility, without systematic errors among operators, calibration steps, and repeated acquisitions (de Menezes et al., 2010).
Digital Dental Cast Measurements
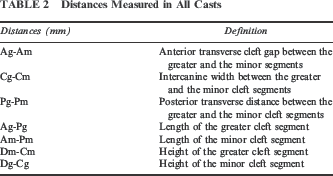
Using the landmark coordinates, anterior-posterior, transverse, and vertical linear distances were obtained as described in Table 2. All the measurements were made with the “point-to-point” distance tool of the stereophotogrammetric software (de Menezes et al., 2010).
Distances Measured in All Casts
Digitization Error
To investigate the reproducibility of the operators' tracings, the same landmarks were assigned and referenced twice by the same operator (A1 and A2).
Caliper Measurements
Using the landmarks described above, the same linear distances were measured on the palatal casts using a caliper with a 0.05-mm precision. The obtained values were compared with the 3D measures provided by the stereophotogrammetric system.
Accuracy on Objects of Known Size
To assess the accuracy of the 3D stereophotogrammetry instrument, a set of measurements were made using objects of known size and simple geometry (cubes and cylinders of different dimensions). Images of the geometric objects were taken with a measuring grid with a 1 −mm resolution (Fig. 2), and measurements were performed for linear distances (unit: millimeter), angles (unit: degree), and areas (unit: centimeter squared). Data were saved and analyzed using the processing software of the 3D stereophotogrammetry instrument (de Menezes et al., 2010; Rosati et al., 2010).
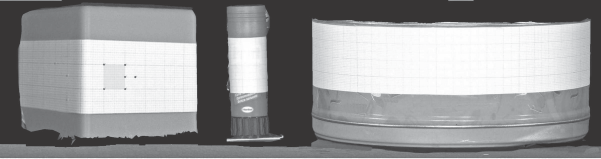
Geometric objects of known size with the measuring grid.
Statistical Analysis
For the assessment of system accuracy, means and standard deviations were computed for distances, angles, and areas calculated on the objects of known size. Accuracy errors (AE, unit: percentage) were used to compare the measurements with the reference values.

For palatal cast measurements, together with the descriptive statistics (mean and standard deviation), the mean absolute difference (MAD) across each data set was calculated. The MAD is the average of absolute differences between the values of two sets of measurements. Paired Student's t tests were used to compare the systematic errors between the replicate measurements. A p value of .05 or less was used to assess statistical significance. The technical error of measurement (TEM) was used to evaluate the random error. The TEM or Dahlberg's error is calculated as

Finally, another accuracy estimator, an error magnitude relative to the size of the measurement (REM), was obtained by dividing the MAD by the grand mean for that variable, represented as a percentage. Thus, smaller percentages correspond to more precise measurements. According to Weinberg et al. (2004), REM scores were divided into five precision categories: Values less than 1% were considered excellent; from 1% to 3.9%, very good; from 4% to 6.9%, good; from 7% to 9.9%, moderate, and those exceeding 10% were considered poor.
The same calculations (MAD, TEM, and REM) and statistical tests (paired Student's t tests) were made to compare linear distances obtained by stereophotogrammetry and by caliper.
Results
Objects of Known Size
Table 3 reports the measurements obtained on the objects of known size for linear distances, angles, and areas. The differences between measurements obtained on the geometric objects were quite low and were nearly similar to the resolution of the grid. Thus, except for small round objects (with an error of 1.21%), the AE when measuring geometric objects was lower than 0.9%.
Accuracy of the Stereophotogrammetric System

Digitization Error
No systematic errors between measurements obtained on two different occasions by the same operator (A1 and A2) were found (Table 4; all p values from the paired Student's t tests were larger than .05). All mean differences were lower than 0.2 mm, with MADs ranging between 0.05 mm (Dg-Cg distance) and 0.32 mm (Cg-Cm distance). Accordingly, the lowest TEM was found for the Dg-Cg, Ag-Pg, and Am-Pm distances, and the largest, for Cg-Cm. Lower TEM values correspond to more repeatable measurements: The random error was lower than 0.7 mm for all distances. According to the ranking described by Weinberg et al. (2004), all REM values were considered excellent or to have very good precision.
Differences Between Repeated Acquisitions *
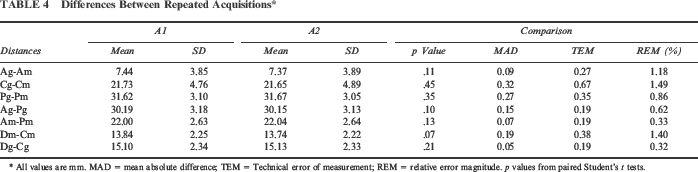
All values are mm. MAD = mean absolute difference; TEM = Technical error of measurement; REM = relative error magnitude. p values from paired Student's t tests.
Palatal Measurements: Caliper Versus Stereophotogrammetry
In Table 5, data obtained by two different methods (caliper versus stereophotogrammetry) were compared. For all distances, except for Cg-Cm distances, significant systematic errors were found (all p values of paired Student's t tests were smaller than 5%), with MAD values ranging between 0.22 and 3.41 mm. Consequently, REM rates were scored as moderate for Ag-Am and poor for the Ag-Pg and Am-Pm distances. Indeed, apart from the Ag-Pg and Am-Pm distances, all TEMs had small random errors (lower than 1.06 mm). Caliper measurements were larger than 3D stereophotogrammetry measurements for distances Pg-Pm, Am-Pm, Dm-Cm, and Dg-Cg and lower for distances Ag-Am and Ag-Pg (Fig. 3).
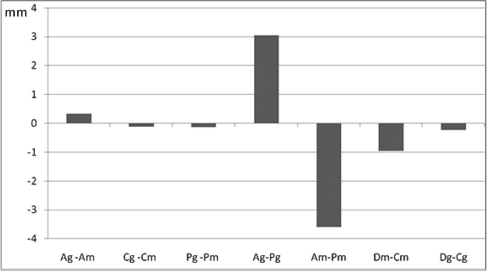
Difference between 3D stereophotogrammetry and caliper measurements. Positive values indicate 3D stereophotogrammetry overestimation; negative values indicate caliper overestimation.
Comparison Between Linear Distances Obtained by Stereophotogrammetry (VECTRA System) and by Caliper *
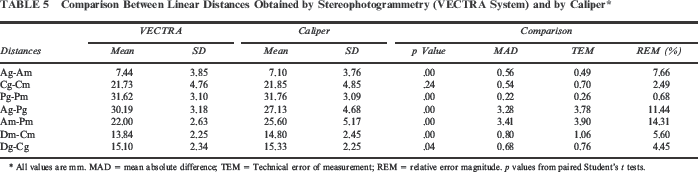
All values are mm. MAD = mean absolute difference; TEM = Technical error of measurement; REM = relative error magnitude. p values from paired Student's t tests.
Discussion
The variety of methods for facial analyses using 3D reconstructions is offering a significant change in the process of diagnosis, providing information for planning and evaluating medical procedures and treatments (He et al., 2010). The stereophotogrammetric systems are being spread into the anthropometric laboratories as good-quality instruments for morphologic facial examinations; they have with several advantages over previous methods, such as fast acquisition, limited cost, and lack of dangerous procedures, thus becoming the leading tool for surface investigations (Weinberg et al., 2004; Wong et al., 2008; de Menezes et al., 2010).
At the same time, dental casts can be digitized using laser scanners (Oosterkamp et al., 2006; Kecik and Enacar, 2009), and the digital models can be used in association with the 3D facial images, allowing the clinician to analyze the relationships between soft tissues and dental arches without submitting the subjects to radiographic scans (Rosati et al., 2010). Independently of the technique used, the precision and validity of the method are essential for a reliable analysis of craniofacial deformities (Weinberg et al., 2004). The present study showed that a commercial stereophotogrammetric system can be used to digitize the palatal casts of children with UCLP. There are several other anthropometric studies that analyzed palatal cleft deformity using highly sophisticated, computerized analytical methods (Bilwatsch et al., 2006; Chen et al., 2010), but these methods are not usually available outside the center that developed them.
Measurements on the geometric objects of known size showed a good accuracy; the obtained values were close to the real values, ranging from 0.04% to 1.21%, with a mean accuracy error of 0.50%. Actually, the minimal differences found might be associated with the operator digitization or the printed grid used.
To evaluate the reproducibility of measuring 3D virtual models, a set of linear distances was selected among those most used for the quantitative analysis of UCLP. All reference landmarks were marked on the palatal cast surface prior to stereophotogrammetric imaging. Indeed, previous investigations found that sets with marked landmarks were associated with smaller errors than were unmarked ones (Weinberg et al., 2004; Wong et al., 2008).
The used method was reproducible in measuring the studied linear distances. No systematic errors were found; on average, the differences (MAD) between repeated measurements were lower than 0.32 mm. The MAD and the REM are reported as an accuracy assessment, with a simple calculation and interpretation (Weinberg et al., 2004; Wong et al., 2008).
In analyzing the errors between the two different systems of acquisition, systematic errors were found for all measures (p < .05) except for Cg-Cm. This could be because the landmarks Cg and Cm are located on the crest of the alveolar segments in an anatomical position that allows an “easy” positioning of the caliper. The differences found between the two measurement methods are in agreement with previous studies that performed linear measurements between reference points with digital calipers directly on cast models (Suzuki et al., 1999; Naidu et al., 2009). In both studies, this procedure was found to produce errors not only during the positioning of the landmarks but also during distance measurement and when transferring the data into the computer (Nagy and Mommaerts, 2007). Indeed, we also observed that the contact of the caliper tip on the palatal cast landmark often canceled the dot, inducing imprecision in the measurements. In a global analysis, caliper measurements of linear distances were larger than relevant values obtained by 3D stereophotogrammetry.
Considering the MAD computed between the two different methods, on most occasions the values were lower than 0.8 mm; hence, almost all measurements seemed to have a good accuracy. A different trend was found for the anterior-posterior distances Ag-Pg and Am-Pm, which had MADs of 3.28 and 3.41 mm, respectively. Actually, these same distances, followed by Ag-Am, showed moderate and poor scores, respectively, according to the classification used by Weinberg et al. (2004). The REM analysis was important because it offered an estimate of the relative magnitude of errors independently of the absolute dimensions (Weinberg et al., 2004). Both anterior-posterior distances showed very large relative errors, which prevent the use of caliper in clinical practice or research. All the other linear distances had TEM values lower than 1.06 mm. The largest reproducibility was found for the distance Pg-Pm, with a TEM of 0.22 mm. However, the distances Ag-Pg and Am-Pm showed somewhat larger errors. It could be presumed that a large inaccuracy during the positioning of the caliper tip might be due to the point location: Ag and Am are cleft-edge points of the alveolar segments, located near the deformities.
Conclusion
Measurements recorded by the 3D stereophotogrammetric system appear to be sufficiently accurate and reliable for assessing stone casts of newborn patients with UCLP. The 3D stereophotogrammetric systems have several advantages over direct anthropometry and gradually are becoming more affordable, replacing classical methods to quantify surface topography. The present study found that the method could, therefore, be useful for clinical analyses in maxillofacial, plastic, and aesthetic surgery.
Further investigations will assess more complex palatal measurements and structural information (surface areas and curvature, geodesic distances and angles) starting from the images recorded by the 3D stereophotogrammetric system.