
Abstract
Objective
The Craniofacial Condition Quality of Life Scale (CFC-QoL) was used to evaluate the relationship between surgical burden and quality of life (QoL)
Design
Patient-parent dyads completed the CFC-QoL which queries the following QoL domains: Bullying, Peer Problems, Psychological Impact, Family Support, Appearance Satisfaction, and Desire for Appearance Change. Stepwise multivariate linear regressions were performed for each QoL domain.
Setting
Urban tertiary care center
Patients, participants
Pediatric patients with facial differences, and their parents.
Intervention
Survey study
Main Outcome Measure(s)
Demographic, diagnostic, and surgical characteristics were collected. Surgical burden was calculated as the standard deviation from the mean number of surgeries per diagnostic cohort.
Result
Patients (N = 168) were majority female (57.1%) and Hispanic (64.3%). Diagnoses were cleft lip and/or palate (CLP,n = 99) or other craniofacial conditions (CFC,n = 69). Average patient age was 2.3 ± 5.6 years at first reconstructive surgery and 12.3 ± 3.4 years at study enrollment. Patients received an average of 4.3 ± 4.1 reconstructive surgeries.
Worse Bullying was associated with higher surgical burden. Worse Peer Problems was associated with higher surgical burden, but only for children with non-CLP CFCs. Worse Family Support was associated with CFC diagnosis, female sex, and higher surgical burden. Worse Psychological Impact was associated with higher surgical burden. Worse Appearance Satisfaction was associated with younger age and with lower surgical burden. Greater Desire for Appearance Change was associated with older age, higher surgical burden, CLP diagnosis, female sex, and non-Hispanic ethnicity. Socioeconomic status did not predict QoL per patient self- or parent-proxy report.
Conclusions
Higher surgical burden was associated with worse QoL outcomes in multiple domains.
Keywords
Introduction
Patients with congenital facial differences often require reconstructive surgery to optimize their physical function and aesthetic appearance. The treatment timeline for these patients frequently involves multiple surgeries throughout childhood and adolescence, with one study reporting that patients in the United States with cleft lip and/or palate (CLP) receive an average of 8.6 surgical procedures before 21 years of age. 1 Reconstructive surgery of the face can have significant social ramifications due to appearance changes and the need to wear therapeutic devices. Additionally, serial surgeries can disrupt academic and social plans due to surgical scheduling, hospitalizations, post-operative limitations, and rehabilitation needs. Although surgical intervention is aimed at optimizing craniofacial form and function, it may have the unintended consequence of disrupting critical periods of social development and integration. 2 When treating facial differences over time, understanding the patient experience is critical in providing patient-centered care along with surgical benefit. An additional dimension is added to the provider-patient relationship in the realm of pediatric reconstructive surgery, as both patient and parent needs must be evaluated to optimize the clinical experience. When considering surgical intervention for children, evaluation of both patient self-report and parent-proxy report has been shown to empower clinicians to address gaps in quality of life in a manner that optimizes patient and parent satisfaction.3,4
Undergoing multiple procedures has been shown to be a risk factor for impaired psychosocial functioning in some pediatric patient populations, but no significant relationship between number of procedures and poor psychosocial outcome was found for patients with cleft lip and/or palate. 5 However, Potrema et al.'s prospective cohort study of patients with CLP found that multiple operations in children ages 8–10 years old was associated with increased anxiety and depressive symptoms later in life. 2 As treatment of facial differences considers both physical form and psychological health, it is important to understand how the quantity of reconstructive surgeries impacts quality of life in a diverse patient population. This study aimed to cross-sectionally assess the impact of demographic, diagnostic, and surgical variables on health-related quality of life (QoL) of pediatric patients with congenital facial differences.
Materials and Methods
Enrollment
Following approval by the University of California San Diego Institutional Review Board, the Craniofacial Condition Quality of Life Scale (CFC-QoL) was administered between March 2017 and November 2021 to children with congenital facial differences and their parents. Patients were eligible for this study if they were diagnosed with bilateral or unilateral CLP, isolated cleft lip, craniosynostosis, hemifacial microsomia, microtia, or dermatological conditions (including large vascular anomalies and congenital nevi involving multiple facial subunits). Patients between the ages of 7 and 21 years, and their parents, were recruited as dyads during routine clinic appointments by study staff. Dyads were excluded if their cognitive or communication skills precluded comprehension and completion of the study. Following consent, patients and parents completed the CFC-QoL and demographic questionnaires on paper in their preferred language of English or Spanish. Patients and parents were asked to complete the paperwork without communication with one another to minimize any external influence on responses. Study staff were available to answer questions and reviewed all forms for completion. Study staff then corroborated relevant information with electronic medical records and input final responses into a Research Electronic Data Capture (REDCap) tool hosted by our institution.
Quality of Life
The CFC-QoL is a patient self-report and parent proxy-report outcome measure that assesses the QoL of children with facial differences. Both patient self-report and parent proxy-report versions are available in English or Spanish. The measure consists of 19 items comprising six QoL domains: Bullying (level of teasing and different treatment from peers), Peer Problems (level of difficulty making friends and in speaking with peers), Psychological Impact (level of anxiety and uncertainty about the future), Family Support (level of support from family in social settings and at home), Appearance Satisfaction (level of comfort with current physical features), and Desire for Appearance Change (degree of dissatisfaction with and motivation to change physical features). The development of the CFC-QoL has been previously described, including an iterative process consisting of a systematic literature review, expert opinion, and in-depth interviews in English and Spanish with patients and parents of patients with diverse craniofacial conditions. 6 Each domain was further optimized following item-reduction based on exploratory factor analysis. Domains were comprised of situational questions, with a response scale ranging from 0 = “never” to 4 = “almost always”. Higher scores indicated better QoL on the Appearance Satisfaction and Family Support scales and worse QoL on all other scales.
Demographic, Diagnostic, and Surgical Characteristics
Demographic indicators were collected via parent report and included patient age, sex (male/female), ethnicity (Hispanic versus non-Hispanic), and diagnosis (cleft lip/palate [CLP] versus other craniofacial condition [CFC]), insurance status (private/public), parent education, and parent occupation. Socioeconomic status (SES) was estimated in our population with three separate proxies: SES index, parent education, and parent occupation. The SES index was constructed based on geography-based attributes of the home address of each patient.7,8 The home address of each patient was entered into the United States Census Bureau database to retrieve the corresponding block group. Block groups are a subdivision of census tracts with 600–3000 people that provide a relatively granular level of area-based demographic data. 9 From each block group, the associated 2019 values for the following domains were extracted: median household income, median house value, median gross rent, percent of population below 150% of the poverty line, education index, and percent working class. These variables were used to construct the final SES index, which was divided into quintiles from lowest to highest SES. Occupation was coded into one of nine United States Federal Sector occupation groups as dictated by the Equal Employment Opportunity (EEO) Commission – management, professionals, technicians, sales workers, administrative support workers, craft workers, operatives, laborers, and service workers. 10 These were further characterized into “skilled” if the role typically required a 2 to 4-year college degree or vocational program, and “unskilled” if the role did not.
“Surgical burden” was calculated as the standard deviation of the number of reconstructive surgeries a patient has undergone from the mean number of surgeries for all patients within their diagnostic cohort. Diagnostic cohorts were defined as either CLP (n = 99, uni/bilateral cleft lip and/or palate) or other congenital CFC (n = 69, craniosynostosis, hemifacial microsomia, microtia, dermatological condition). Minor or non-craniofacial interventions such as myringotomy tubes and tonsillectomies/adenoidectomies were excluded.
Statistical Analyses
Demographic variables and CFC-QoL scores were analyzed using descriptive statistics. Chi-square tests, independent samples t-tests, and Fisher's Exact test were used to compare demographic variables and CFC-QoL scores between diagnostic cohorts. Stepwise multivariate linear regressions were performed to assess the associations between demographic and operative characteristics and CFC-QoL scores in each diagnostic cohort. Twelve regressions were run: one for each patient self-reported and parent proxy-reported CFC-QoL domain. The predictor variables used were diagnosis, patient sex, patient ethnicity, patient age, insurance type, parent education, parent occupation (EEO category), SES index quintile, age at first reconstruction, and surgical burden. An interaction term between diagnosis and surgical burden was also run to determine whether surgical burden predicted CFC-QoL scores differently per diagnostic cohorts.
Results
Patient-parent dyads (N = 168) completed the CFC-QoL. The patient sample was primarily female (57.1%) and Hispanic (64.3%) (Table 1). Patients were separated into diagnostic cohorts of CLP (n = 99, uni/bilateral cleft lip and/or palate) or other congenital CFC (n = 69, craniosynostosis, hemifacial microsomia, microtia, dermatological condition).
Sample Descriptors.
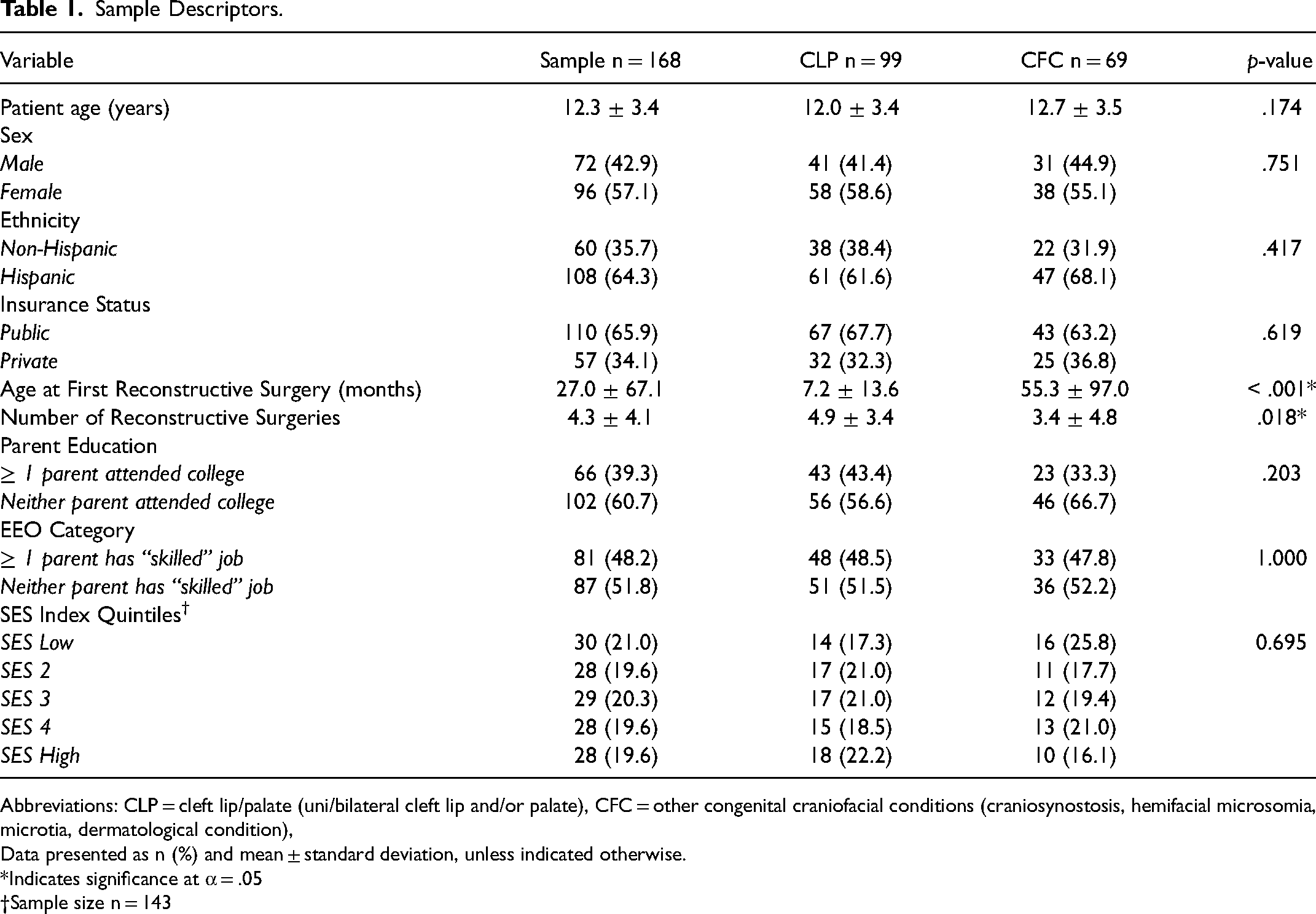
Abbreviations: CLP = cleft lip/palate (uni/bilateral cleft lip and/or palate), CFC = other congenital craniofacial conditions (craniosynostosis, hemifacial microsomia, microtia, dermatological condition),
Data presented as n (%) and mean ± standard deviation, unless indicated otherwise.
Indicates significance at α = .05
†Sample size n = 143
Average patient age was 2.24 ± 5.59 years at first reconstructive surgery and 12.3 ± 3.4 years at study enrollment. Patients received an average of 4.29 ± 4.06 surgeries. Patients with CLP were on average significantly younger than patients with a CFC at the time of their first reconstructive surgery (7.2 ± 13.6 months vs. 55.3 ± 97.0 months old, p < .001). Patients with CLP underwent significantly more operations than patients with a CFC did (4.9 ± 3.4 vs. 3.4 ± 4.8, p = .018).
Most families had public insurance (65.9%; Medi-Cal, Healthy Families, California Children's Services) while the remainder had a private insurer. For most patients, neither parent was college educated (60.7%), and neither parent held a “skilled” job per EEO categorization (51.8%). SES indices were evenly distributed between the two diagnostic cohorts (p = .695).
Craniofacial Condition Quality of Life Scale Responses
Average CFC-QoL score in each domain for patients and parents is displayed in Table 2. CFC-QoL scores were not statistically different between diagnostic cohorts for any domain except for a significantly higher score on Desire for Appearance Change reported by parents of children with CLP (p = .005).
Mean CFC-QoL Scores for Patients and Parents by Diagnostic Cohort.
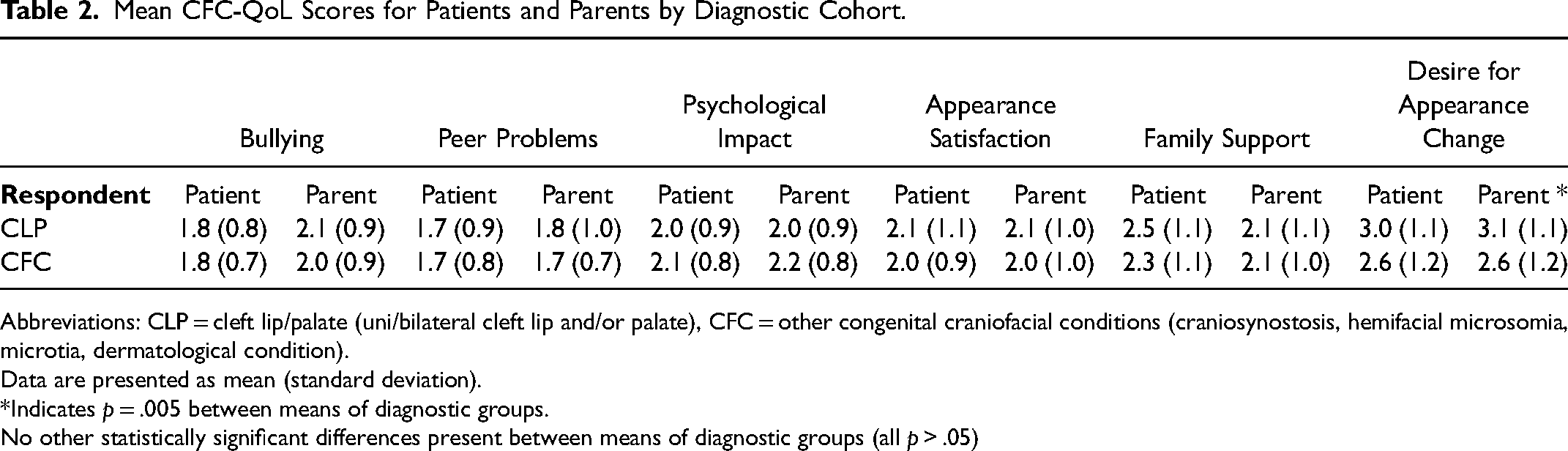
Abbreviations: CLP = cleft lip/palate (uni/bilateral cleft lip and/or palate), CFC = other congenital craniofacial conditions (craniosynostosis, hemifacial microsomia, microtia, dermatological condition).
Data are presented as mean (standard deviation).
Indicates p = .005 between means of diagnostic groups.
No other statistically significant differences present between means of diagnostic groups (all p > .05)
Quality of Life Domains
See Table 3 for regression analysis results. Higher surgical burden was significantly associated with worse CFC-QoL scores for Bullying (patient self- and parent proxy-report), Family Support (parent proxy-report) and Psychological Impact (parent proxy-report), and with greater Desire for Appearance Change (patient self- and parent proxy-report). Lower surgical burden was significantly associated with higher Appearance Satisfaction (parent proxy-report). CLP was significantly associated with greater Desire for Appearance Change (parent proxy-report) and Family Support (patient self-report). Age was significantly associated with higher Appearance Satisfaction (patient self-report). Female sex was significantly associated with increased Bullying (patient self-report) and greater Desire for Appearance Change (parent proxy-report). Non-Hispanic ethnicity was significantly associated with greater Desire for Appearance Change (parent proxy-report). Socioeconomic status indices did not significantly predict CFC-QOL scores per patient self-report or parent proxy-report in any regression model. An interaction term between diagnosis and surgical burden was input in each stepwise regression and was non-significant in eleven of twelve regressions run. The exception was Peer Problems per parent proxy-report. Post-hoc analysis showed that surgical burden was significantly positively associated with parent-reported Peer Problems for children with CFC (r = .399, p < .001) but not for children with CLP (r = .167, p > .05).
Stepwise Multivariate Linear Regression Results.
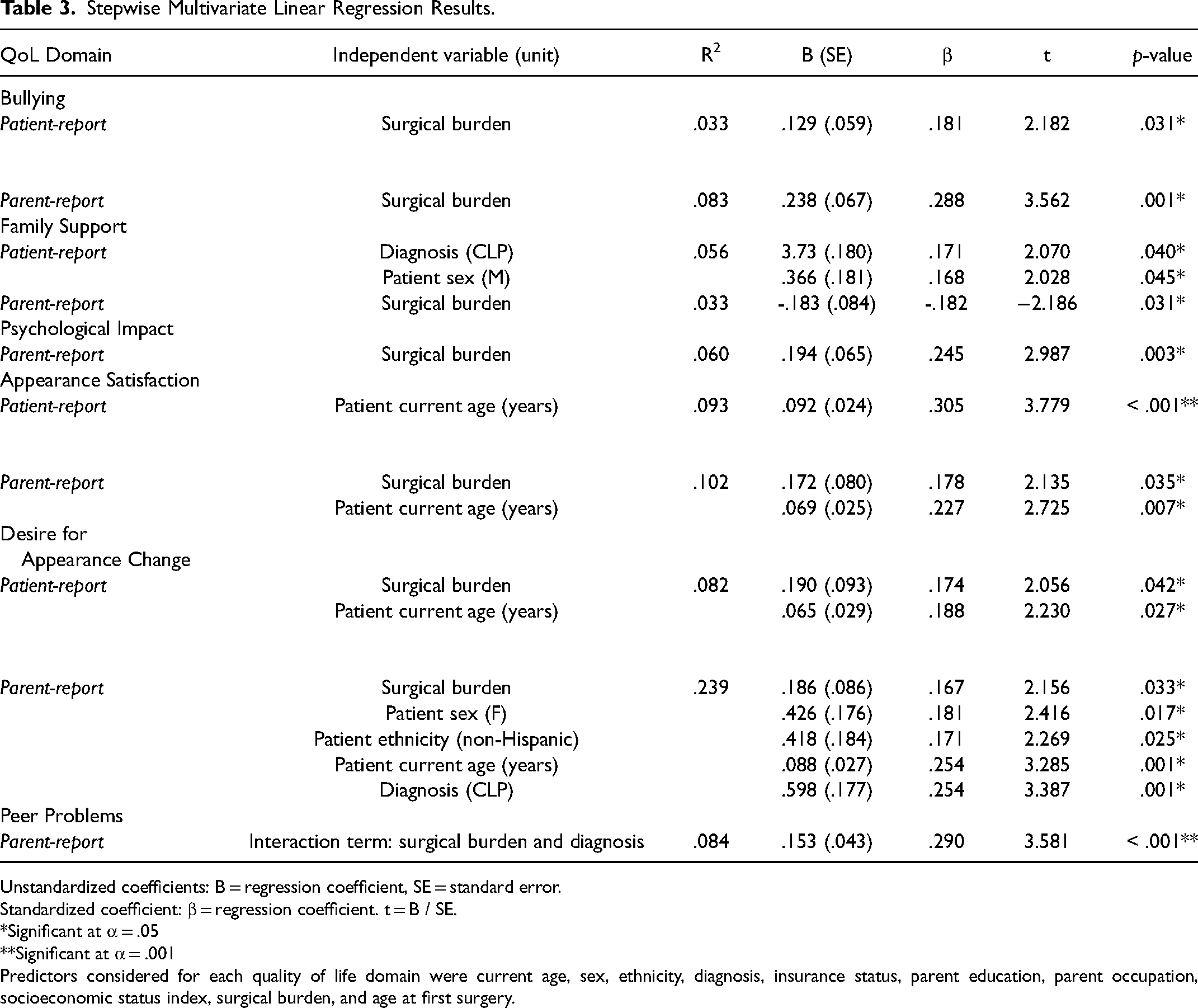
Unstandardized coefficients: B = regression coefficient, SE = standard error.
Standardized coefficient: β = regression coefficient. t = B / SE.
Significant at α = .05
Significant at α = .001
Predictors considered for each quality of life domain were current age, sex, ethnicity, diagnosis, insurance status, parent education, parent occupation, socioeconomic status index, surgical burden, and age at first surgery.
Discussion
The face is the social organ of the body, allowing people to interface with the world, and playing an important role in both social and career-related pursuits. Studies have shown people draw trait inferences based on facial appearance, with discrete opinions formed within milliseconds of interaction. 11 The gravity of a facial difference is evident and can cause significant impacts on social-emotional well-being.
When approaching treatment of a facial difference, there are a variety of viewpoints to consider. From a layperson's perspective, there is a strong societal motivation to look “normal”, if not “beautiful”, as evidenced by the multi-billion-dollar beauty and personal care industry. From a patient perspective, there may be pressure to conform to societal ideals of cosmesis and to pursue all surgical options to live life with minimal hindrance. These motivations may be balanced by financial constraints, personal tolerance for surgical interventions, and personal outlook on life. In pediatric patients, the parent perspective must also be considered, as this is often the decision-making party. Parents may balance the same pressures of society, finances, surgical tolerance, and personal outlooks. However, they may feel the added pressure to advocate for children who are not old enough to understand or voice their opinions. Ultimately parent and patient perspectives may conflict, as seen in this study. Finally, the surgical perspective must be considered. A surgeon has technical ability and financial motivation to operate, however, these must be weighed against the medical and psychosocial indications for each operation and realistic post-operative outcomes. Our single-center cross-sectional study aimed to evaluate the multi-party considerations in reconstructive surgery for pediatric patients with facial differences and found surgical burden to be largely associated with worse quality of life outcomes.
Demographic Characteristics and Quality of Life
Our cohort demonstrated significant associations between QoL and the demographic factors of sex and age. Parent proxy-report demonstrated that female sex predicted greater Desire for Appearance Change. This impact of sex on perceived appearance and self-esteem has been described in previous research in populations with and without CLP diagnoses.12,13 In our study, patient-report and parent-proxy report demonstrated that younger age was associated with worse Appearance Satisfaction. These findings may suggest that appearance satisfaction increases with age due to greater self-acceptance and sense of self. An increase in benefit-finding with age has been previously demonstrated in the general population, with age fostering the ability to construe positivity from adversity. 14 Perhaps a facial difference can confer indirect benefits in a patient's life, including personal growth, positive social relationships, and empowerment to help others. Additionally, younger patients may have worse Appearance Satisfaction as they may have more severe dysmorphology as they await age-linked operations (eg, primary rhinoplasty for patients with cleft in teenage years. In our study, a greater Desire for Appearance Change was associated with older age, indicating a potential benefit from continuing to offer surgical repair at later ages, even if patients express satisfaction with their features.
Socioeconomic status, as represented by parent education, parent occupation (EEO category), and SES index quintile, was not associated with QoL in our cohort. Pediatric patients at our institution with limited means receive pro bono reconstructive care through partnerships with charitable organizations; therefore, this finding elucidates the influence of SES on QoL when the barrier of access to care is removed. Our findings demonstrate a patient experience that is not significantly linked to one's financial status. This contrasts with previous studies, which have found that lower socioeconomic status generally correlates with worse psychosocial quality of life in children with oral health concerns, 15 asthma, 16 and other debilitating chronic diseases. 17 Future studies are warranted beyond our single-institution investigation, and with longitudinal follow-up, to further characterize the impact of socioeconomic status on the psychosocial quality of life of our patients when controlling for access to surgery.
Diagnostic Characteristics and Quality of Life
We found that in comparing the CLP and CFC diagnostic cohorts, patients with CFCs reported worse Family Support, while parents of patients with CLP reported greater Desire for Appearance Change. Otherwise, QoL domains were not significantly associated with diagnosis. From a child's perspective, the characteristics or severity of a facial difference may not be appreciated, as all facial differences may be viewed as “different” without nuance to influence self-perception or treatment by other children. From a parent perspective, the lack of difference in QoL between diagnoses may reflect conceptualization of their child as being cast under the umbrella of “different.”
Surgical Characteristics and Quality of Life
Greater surgical burden was significantly associated with worse Bullying. Patients with greater surgical burden may have more apparent physical dysmorphologies, which can incite negative attention from peers. Greater surgical burden was also significantly associated with less Family Support, which may reflect families not having adequate resources and education to adequately meet the medical and social demands of a child with a craniofacial condition. Greater surgical burden was also associated with worse Psychological Impact. This is an interesting phenomenon, as patients are ostensibly achieving greater functional and cosmetic results with more surgeries. However, surgical care can detract from academics, extracurriculars, and vacation time, all of which healthy children can partake in without having to balance peri-operative precautions and surgical schedules. The negative psychological impact could also be linked to the association between greater surgical burden and greater Desire for Appearance Change. Patients requiring more surgery than their cohort average may have more severe facial differences, leading to greater impacts on quality of life. Patients with greater surgical burden may also be more likely to be unsatisfied with their results, as they continue to pursue an ideal aesthetic or functional goal which may be unrealistic in the context of their disease severity.
When comparing CLP and CFC cohorts, the age at first reconstruction and number of reconstructions was significantly different. An interaction term exploring the difference in impact of surgical burden between diagnostic cohorts was run in each multivariate regression to assess significance. In almost all the regressions, this term did not reach significance, while surgical burden alone did, suggesting that surgical burden significantly impacts our patient's QoL, and this relationship is similar across diagnostic cohorts.
Limitations
Patients in our analysis were stratified into cleft lip and/or palate and other craniofacial conditions. The diagnoses were not further stratified by severity of dysmorphology, which could influence the timing and number of surgical interventions. Sub-stratification was not conducted as these diagnoses are rare in the population and would result in an underpowered analysis. Accordingly, future studies would benefit from a larger sample size and analysis after stratification of diagnoses by severity and syndromic status. Another limitation of this study is in the accuracy of the SES designation employed. The SES index calculation is an estimate based on block groups, which are area-based and may not accurately reflect the financial capabilities of individual residents. To address this, multiple proxies of SES were used including insurance status and parent occupation. Separately, this study focuses on the quality of life of patients who are willing and able to engage with medical and surgical care, therefore not capturing the experience of those who may face other barriers to care. Additionally, portions of the data were collected before the COVID-19 pandemic, while other portions of the data were collected while public health measures such as mask-wearing mandates were in place. A recent analysis by our group comparing self-report and parent-proxy report data collected before versus during the pandemic revealed better psychosocial quality of life reports during the pandemic. 18 This is a consideration that was not accounted for in the analysis of this manuscript. Finally, the study is limited by reliance on cross-sectional data. Longitudinal analysis is essential to offer insight into the understanding how surgical burden impacts quality of life in this population.
Conclusions
This study employed patient self- and parent-proxy report to evaluate QoL in a sample of children with facial differences and found that surgical burden cross-sectionally predicted worse QoL in several domains. Sex, age, and diagnosis were associated with aspects of QoL, while socioeconomic status was not. These findings convey the need to critically assess the unique pros and cons of craniofacial surgery for a patient in the context of their biopsychosocial environment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
None of the authors have financial interests to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.