
Abstract
Objective
The surgical outcomes of novel two-flap palatoplasty adding a buccinator musculomucosal flap were compared with those of conventional two-flap palatoplasty to clarify the effects of lengthening the nasal mucosa of the soft palate using a BMMF in cleft lip and palate or cleft palate cases.
Design
Retrospective, comparative study
Setting
Tertiary, cleft team
Patients
Non-syndromic patients undergoing primary cleft palate repair using two-flap palatoplasty with BMMF (BMMF group) or conventional two-flap palatoplasty (non-BMMF group)
Interventions
Palatoplasty between January 2012 and March 2020
Main Outcome Measures
Perceptual Japanese speech evaluation, rate of an indication for additional speech surgery (AS), rate of incidence of oronasal fistula (IF) including spontaneously closing fistula, and rate of occurrence of oronasal fistula (OF) present for more than 3 months.
Results
Of 92 analyzed patients, 70 received two-flap palatoplasty with BMMF and 22 received two-flap palatoplasty. In the BMMF and non-BMMF groups, the respective percentage of hypernasality (no, mild) was 91.4% and 77.2%, no nasal emission was 71.4% and 63.6%, velopharyngeal function (competent, borderline competent) was 83.7% and 77.4%, intelligibility (very good, good) was 93.7% and 86.4%, AS was 1.4% and 13.6%, IF was 7.1% and 36.4%, and OF was 1.4% and 9.1%. Significant improvements were observed for AS (p = 0.0412) and IF (p = 0.00195) in the BMMF group, with no recorded major adverse effects.
Conclusion
Adding a BMMF on the nasal side of the soft palate to conventional two-flap palatoplasty significantly improved postoperative outcomes. This approach may therefore be a good option for cleft palate treatment.
Keywords
Introduction
The primary goals of cleft palate repair are closure of the cleft, provision of normal speech with adequate velopharyngeal function, and minimization of the effects on dentomaxillofacial growth. Many techniques have been reported to accomplish these aims. 1 In the two-flap palatoplasty technique reported by Bardach, 2 patients are able to achieve normal velopharyngeal function through reconstruction of the muscle sling. This approach can be adapted to a wide cleft and can close the palatal cleft with no tension in the areas of the hard and soft palate owing to the use of the highly movable bilateral mucoperiosteal flaps. As a result, the occurrence rate of fistula in two-flap palatoplasty is lower than in other methods,3,4 and so this technique is widely used worldwide.1,2,5,6
Abdollahi Fakhim et al. later developed a technique of lengthening the soft palate using double-layer Z-plasty in the oral and nasal mucosa for two-flap palatoplasty with intravelar veloplasty since they found that the conventional method could not provide adequate palatal length in some patients. 7 Similarly, Morrison et al. reported a method in which a buccal mucosal flap (BMF) was inserted into the nasal mucosa of the soft palate to lengthen it along with two-flap palatoplasty in patients with a cleft palate wider than 10 mm8. They confirmed that the soft palate was extended significantly by measuring actual distance. However, such postoperative results as perceptual speech evaluation and the rate of secondary speech surgery were not addressed in detail, and so the utility of lengthening the nasal mucosa of the soft palate in addition to two-flap palatoplasty remains unclear.
In our earlier use of conventional two-flap palatoplasty, we encountered cases in which the technique appeared insufficient for extending the soft palate to achieve normal velopharyngeal function for Japanese speech. Therefore, we developed a modified approach whereby a buccinator musculomucosal flap (BMMF) was inserted into the nasal mucosa of the soft palate to lengthen it. This study aimed to evaluate the usefulness of lengthening the nasal mucosa of the soft palate with a BMMF combined with two-flap palatoplasty through statistical comparisons of surgical outcomes with the conventional method.
Methods
Surgical Technique (Figure 1)
Our method was similar to that reported by Morrison et al. except that we used a BMMF instead of a BMF. 8 The oral mucoperiosteal flaps were elevated as in conventional two-flap palatoplasty while leaving the periosteum up to 2-3 mm from the incision line (Figure 1a, b). The nasal mucoperiosteal flaps were elevated and sutured with 5-0 braided absorbable sutures (Vicryl plus®, Ethicon, USA) (Figure 1c). The cleft muscles attached to the posterior edge of the hard palate were detached (Figure 1d). The nasal mucosa of the soft palate at 2-3 mm from the posterior edge of the hard palate underwent a horizontal incision, and a mucosa defect was made on the nasal side. The BMMF was elevated (Figure 1e) and inserted into the defect of the nasal mucosa through the space behind the greater palatine vessels, beneath the mucoperiosteal flap (Figure 1f). The muscle sling was reconstructed using intravelar veloplasty (Figure 1g). The mucoperiosteal flaps were sutured on the oral side (Figure 1h). Mucosal defects occurring on the oral side were covered with absorbent material (NEOVEIL sheet®, GUNZE MEDICAL LIMITED, Japan). The vascular pedicle of the BMMF required later removal during follow-up surgery.
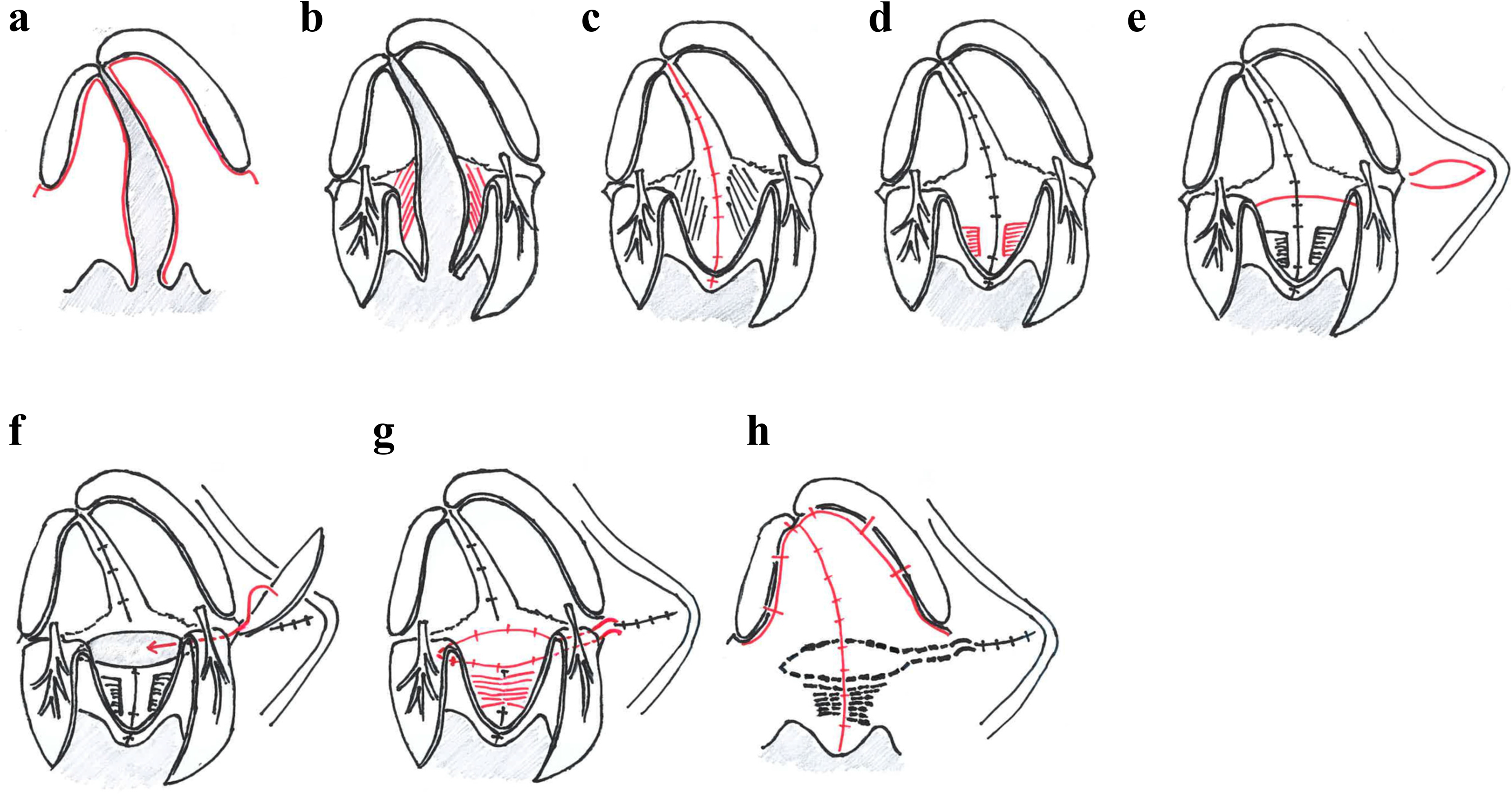
Surgical procedure of two-flap palatoplasty with a BMMF. a, b) The oral mucosal flaps are elevated as in conventional two-flap palatoplasty (cleft muscles in red). c) the nasal mucosa is sutured. d) The cleft muscles are detached. e) A horizontal incision (red) is made in the nasal mucosa and the BMMF is elevated. f) The BMMF is inserted into the defect of the mucosa. g) The BMMF is sutured and the muscle sling is reconstructed. h) The oral mucoperiosteal flaps are sutured.
Design and Patients
This retrospective clinical trial was approved by the medical ethics committee of Nagano Children's Hospital (no. S-04-13). The patients underwent primary cleft palate repair between January 2012 and March 2020 at Nagano Children's Hospital or related institutions and received perceptual Japanese speech evaluation at our hospital. The exclusion criteria were as follows: 1) syndromic, 2) insufficient medical data, and 3) undergoing palatoplasty other than two-flap palatoplasty with the BMMF (BMMF group) or conventional two-flap palatoplasty (non-BMMF group). Conventional two-flap palatoplasty was mainly employed at our institutions in 2012 and 2013. We gradually introduced two-flap palatoplasty with the BMMF until the exclusive use of this mothed from 2018. Two surgeons performed all of the operations. One surgeon (K.F.) operated from January 2012 to April 2017, with the other (K.Y.) operating from May 2017 to March 2020. No preoperative orthodontics were performed, and the postoperative protocol was identical for all patients.
Outcome Measurements
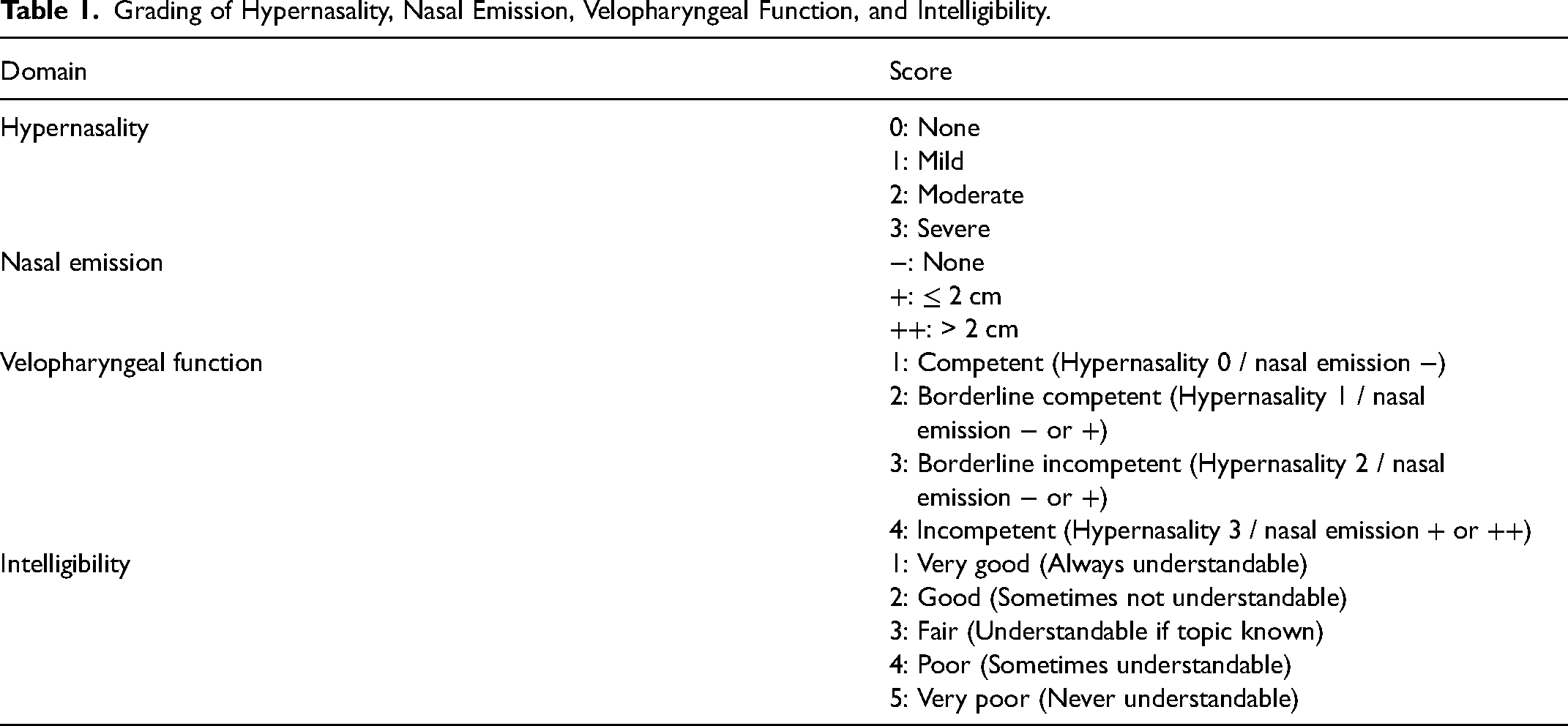
Surgical outcomes included perceptual Japanese speech evaluation, the rate of indication for additional speech surgery (ie, patients with a velopharyngeal gap [VP gap]), the incidence rate of oronasal fistula, and the occurrence rate of oronasal fistula. Perceptual Japanese speech examination by speech language pathologists included hypernasality, nasal emission, velopharyngeal function (VPF), and intelligibility (Table 1). Hypernasality was graded on a four-point scale (0: none, 1: mild, 2: moderate, 3: severe). Nasal emission was measured during soft blowing with a nasal aspirometer. When soft blowing was not possible, hard blowing was used. Nasal emission was classified as a three-point scale (-: none, +: ≤ 2 cm, ++: > 2 cm). VPF level was expressed by a four-point scale according to the results of hypernasality and nasal emission (1: competent [hypernasality 0 / nasal emission −], 2: borderline competent [hypernasality 1 / nasal emission − or +], 3: borderline incompetent [hypernasality 2 / nasal emission − or +], and 4: incompetent [hypernasality 4 / nasal emission + or ++]). Intelligibility was rated on a five-point scale (1: very good [always understandable], 2: good [sometimes not understandable], 3: fair [understandable if topic known), 4: poor [sometimes understandable], 5: very poor [never understandable]). If the patient received more than one perceptual speech evaluation, the results from the test closest to the age of 5 years were used.
Grading of Hypernasality, Nasal Emission, Velopharyngeal Function, and Intelligibility.
Patients meeting the following criteria were examined by multiview videofluoroscopy and nasopharyngoscopy to check for the presence of a VP gap: (1) VPF level of 3 or 4 and intelligibility of 3-5, and (2) VPF level of 3 or 4 or intelligibility of 3-5, with recommendation by speech language pathologists. Patients were judged as having a VP gap for gaps of 1 mm or more on multiview videofluoroscopy and a clear VP gap on nasopharyngoscopy. A VP gap was determined as an indication for additional speech surgery.
The incidence rate of oronasal fistula included cases in which a postoperative fistula was noted in medical records, even those in which the fistula appeared to have closed spontaneously from a physical point of view within three months. The occurrence rate of oronasal fistula was calculated as the incidence rate of oronasal fistula minus the cases of fistula that closed spontaneously within three months. Fistula size was measured as well.
Statistical Analysis
Comparisons of surgical results and perceptual speech evaluation age were made using the Mann–Whitney U test, while those of operation weight and maximum cleft width were performed with the t-test. The Mann–Whitney U test was employed for comparisons of perceptual speech evaluation. Differences in the rate of indication for additional speech surgery, the incidence rate of oronasal fistula, and the occurrence rate of oronasal fistula were analyzed by Fisher's test. A p-value of less than 0.05 was considered statistically significant.
All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan). EZR is a graphical user interface for R commander (The R Foundation for Statistical Computing, Vienna, Austria) that has been modified to add statistical functions frequently used in biostatistics. 9
Results
A total of 137 patients underwent primary palatoplasty in the enrollment period, among which 70 received two-flap palatoplasty with BMMF and 22 received conventional two-flap palatoplasty (Figure 2). Forty-five patients were excluded.
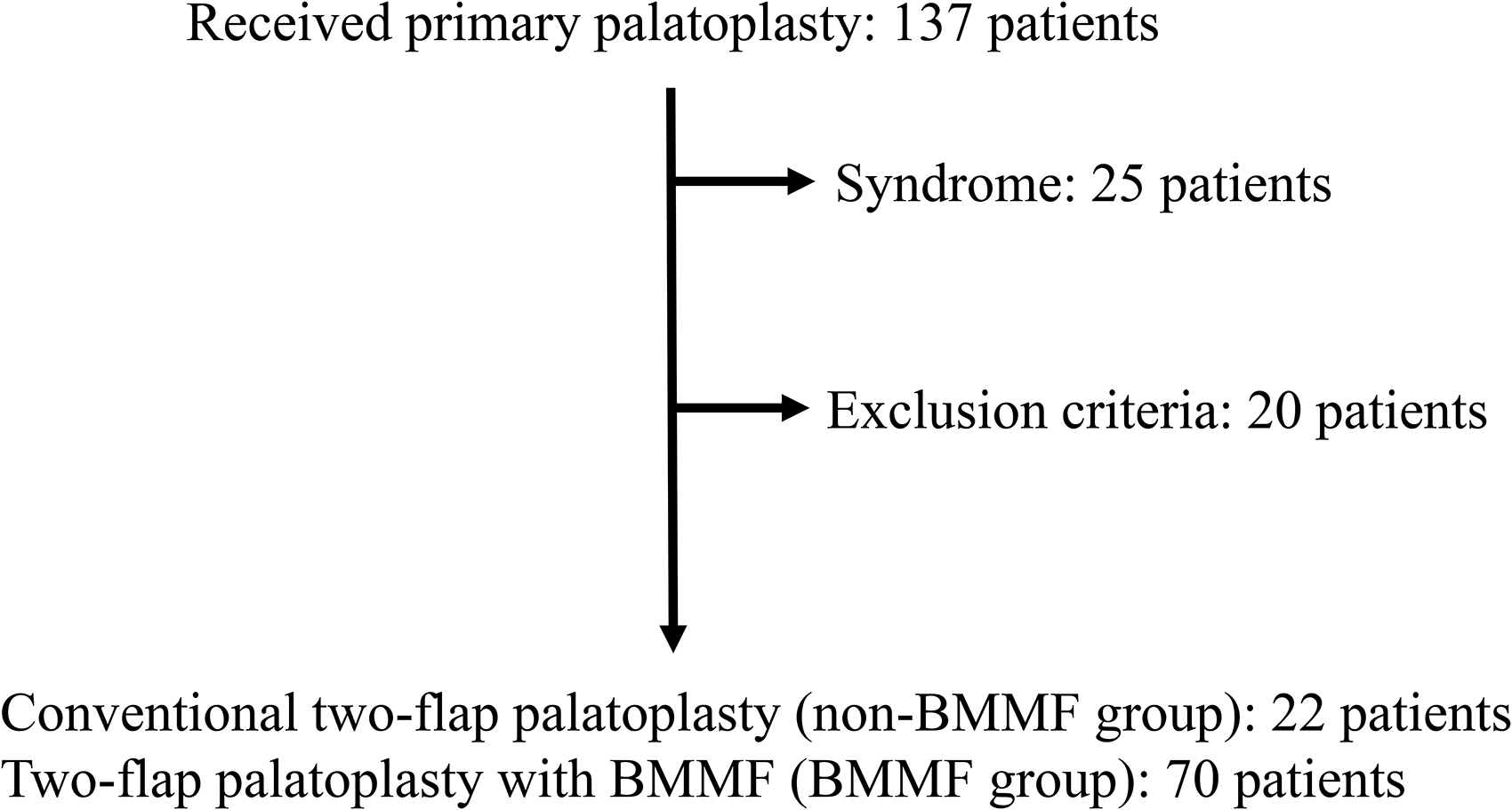
Patient flowchart.
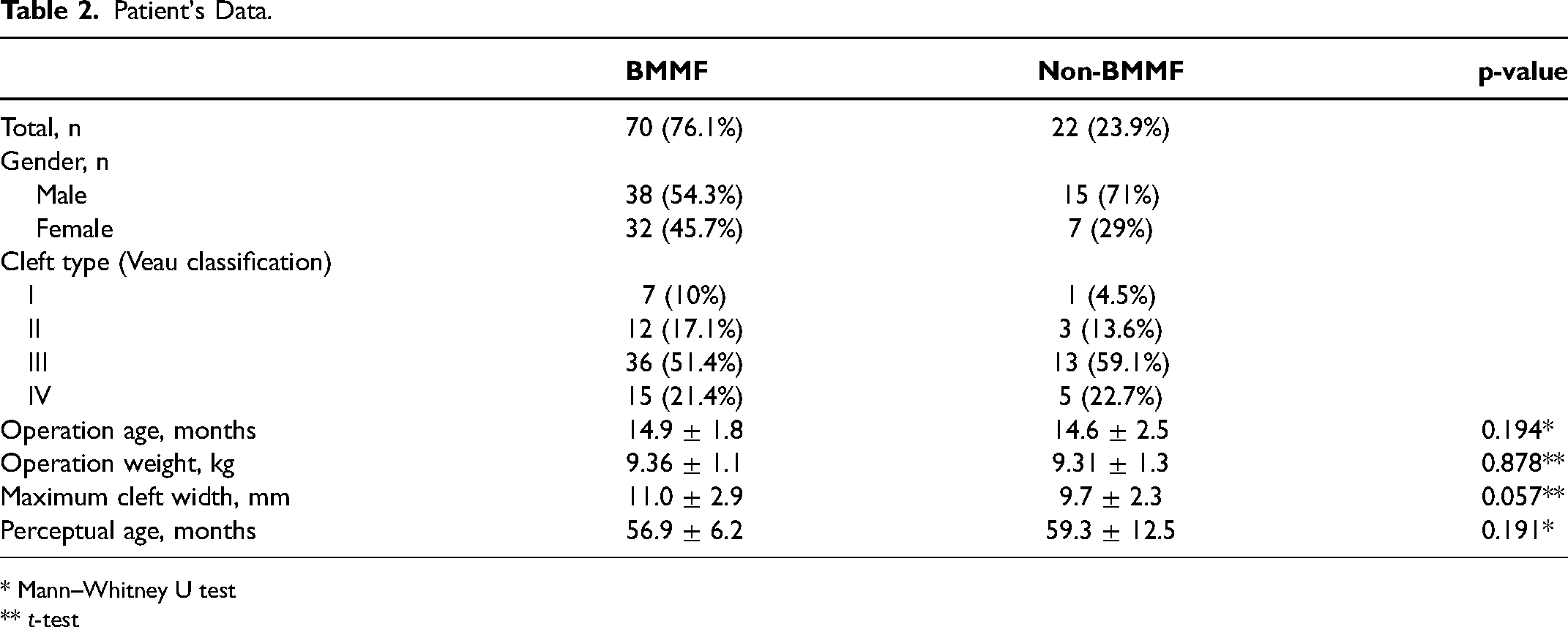
The clinical characteristics of the BMMF and non-BMMF groups were summarized in Table 2. We observed no statistical differences for mean age at surgery, weight at operation, maximum cleft width, or age at perception Japanese speech evaluation between the groups.
Patient's Data.
* Mann–Whitney U test
** t-test
The procedural results of the study groups are presented in Table 3. The percentage of none (0) or mild (1) hypernasality was 91.4% in the BMMF group and 77.2% in the non-BMMF group. The rate of no nasal emission (-) was 71.4% the in BMMF group and 63.6% in the non-BMMF group. The percentage of competent (1) or borderline competent (2) VPF was 85.7% in the BMMF group and 77.5% in the non-BMMF group. Very good (1) or good (2) intelligibility was recorded in 95.7% and 86.4% of the BMMF and the non-BMMF patients, respectively. No significant differences were seen between the groups.
Surgical Results of BMMF and non-BMMF Groups.
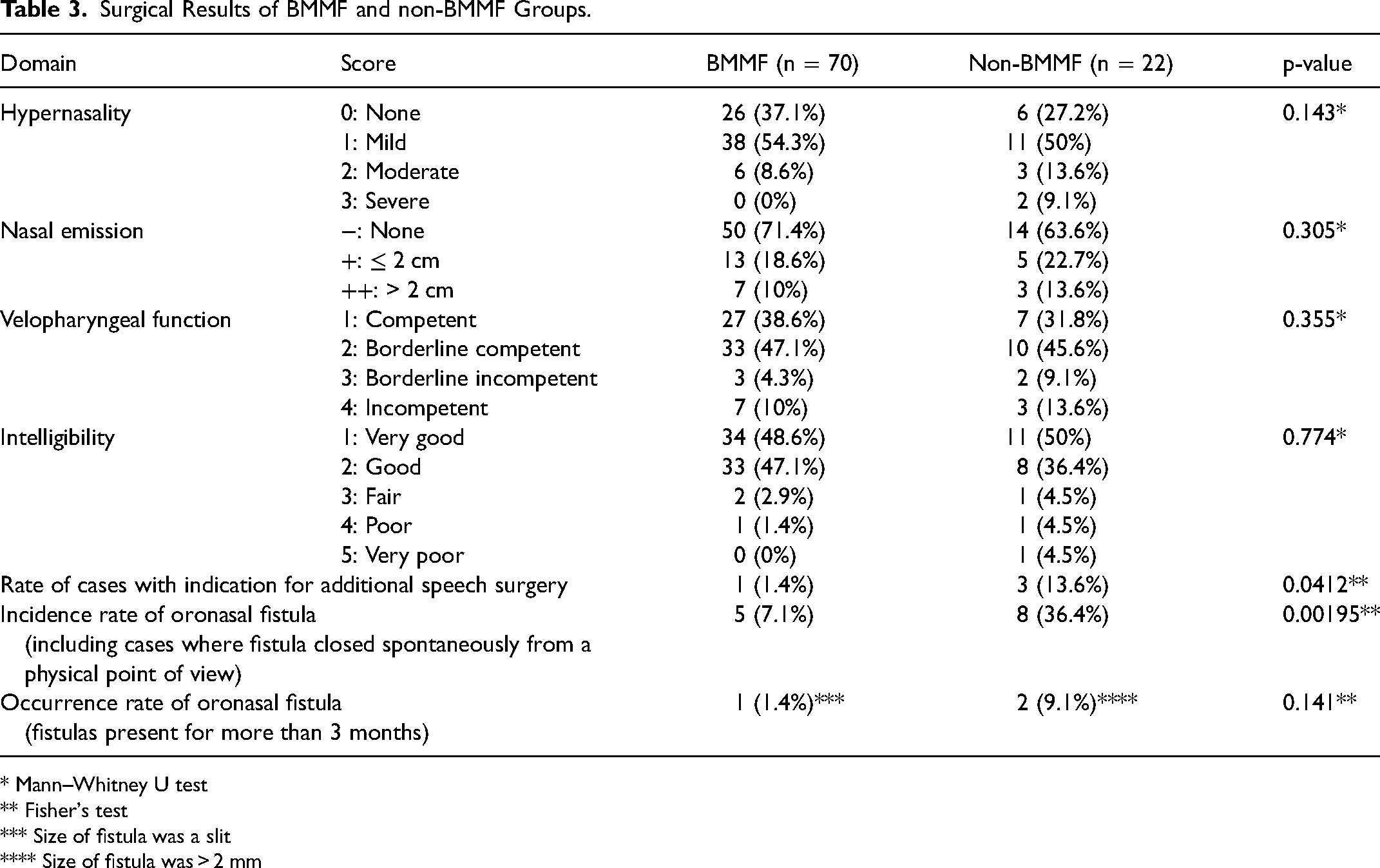
* Mann–Whitney U test
** Fisher's test
*** Size of fistula was a slit
**** Size of fistula was > 2 mm
The rate of an indication for additional speech surgery was 1.4% in the BMMF group and 13.6% in the non-BMMF group, which was a significant difference (p = 0.0412). The incidence rate of oronasal fistula was also significantly lower in the BMMF group (7.1% vs. 36.4%, p = 0.00195). The occurrence rate of oronasal fistula was 1.4% in the BMMF group and the 9.1% in the non-BMMF group. It was not a significant difference. The measured size of fistulas was a slit in the BMMF group, but larger than 2 mm in two patients in the non-BMMF group.
Discussion
This study was the first to compare the surgical outcomes of the novel two-flap palatoplasty using BMMF with those of conventional two-flap palatoplasty. Our technique significantly decreased the rate of an indication for additional speech surgery and incidence rate of oronasal fistula and might therefore represent a good choice for cleft palate treatment.
Previously reported surgical outcomes for conventional two-flap palatoplasty were hypernasality (none, mild) of 70-91.1%, nasal emission (none, mild) 79.8-90%, VPF (competent, borderline competent) of 79.3-81.9%, intelligibility (good, fair) of 86-90%, additional speech surgery rate of 5.3-12%, and occurrence rate of oronasal fistula of 0.9-20%.6,9–11 Our surgical outcomes for the non-BMMF two-flap palatoplasty were similar to those reports. Accordingly, we considered the possibility that adding a BMMF could improve results.
The adoption of two-flap palatoplasty with BMMF significantly decreased the rate of an indication for additional speech surgery (ie, patients with a VP gap), with increased rate of none or mild hypernasality. Huang et al. described that the position of the muscle sling was at the flexure of the soft palate while speaking. 12 Morrison et al. developed a technique in which a BMF was inserted into the nasal mucosa of the soft palate to lengthen it in two-flap palatoplasty and observed mean lengthening of the velum of approximately 10.5 mm8. In light of those studies, we thought that the muscle sling moved posteriorly roughly 10 mm so that the soft palate could contact the posterior wall of the pharynx more easily with our procedure. As a result, the rate of hypernasality due to anatomical abnormalities could be decreased. We also considered two other contributing factors to our results. First, the muscle sling was prevented from returning to the anterior position since the BMMF acted as a physical obstacle. Second, the scar contracture was reduced because the position of the scar between the palatal and nasal mucosa of the soft palate was changed.
Bozola described the BMMF as well-vascularized. 13 The potentially high tension of the nasal mucosa after closing the cleft was reduced by a horizontal releasing incision in our procedure, and the nasal and oral mucosa could be better vascularized by insertion of the BMMF into the defect on the nasal side. Accordingly, the incidence rate of oronasal fistula was improved significantly. On the other hand, we found that the rate of postoperative fistula formation varied depending on the time of the fistula; as a postoperative fistula might close spontaneously, it will be necessary to clarify when a conclusive fistula should be judged.
Other reported methods to lengthen the soft palate include Furlow Z-plasty and the modified double opposing Z-plasty. The additional speech surgery rate was 0-12.7% for Furlow Z-plasty14–17 and 5.5% for the modified double opposing Z-plasty. 18 The oronasal fistula rate was 3.6-10.6% for Furlow Z-plasty and 0.4% for the modified double opposing Z-plasty. Both methods have shown good results for lengthening the oral and nasal mucosa. We aimed to lengthen the nasal mucosa only due to our observed difference in periosteal continuity between the nasal and oral mucoperiosteal flaps after flap elevation. When elevating the nasal mucoperiosteal flaps, we did not incise the periosteum other than the cleft margin. Hence, the longitudinal periosteal continuity of the nasal mucoperiosteal flaps remained at that time, which rendered lengthening of the nasal mucosa impossible. To lengthen the nasal side of the palate, we made a transverse incision in the nasal mucosa of the soft palate and divided it from the periosteum of the hard palate. Meanwhile, the oral mucoperiosteal flaps were more flexible and mobile than the nasal ones since we cut the periosteum around the hard palate and detached it when the oral mucoperiosteal flaps were elevated. The oral mucoperiosteal flaps of the hard palate could be moved posteriorly in a manner similar to a V to Y style, and then separated from the domed bony hard palate and straightened to where the nasal mucosa moved. Accordingly, the oral side of the soft palate became positioned posteriorly under the same effect of lengthening the oral side vertically. We postulate that there are four key benefits of the transverse incision and the BMMF interpolation technique. First, the transverse incision of the nasal mucosa is more effective in reducing vertical tension of the nasal mucosa than the modified opposing Z-plasty because the incision distance is longer. Second, for the same reason, it is also highly effective in lengthening the nasal mucosa. Third, we keep to the cleft muscles on the nasal mucosa during elevation of the oral mucoperiosteal flaps. The cleft muscles are stripped from the nasal mucosa as needed when we reconstruct the muscle sling. Both ends of the muscle sling are attached to the nasal mucosa. Therefore, the muscle sling can also be moved more posteriorly. Fourth, the insertion of a BMMF can compensate for the deficiency of tissue in the nasal mucosa. Owing to the above advantages, we were able to achieve a relatively low indication rate for additional speech surgery and occurrence of oronasal fistula compared with other methods. However, such rates cannot be simply compared due to variability in languages, methods of speech evaluation, and diagnostic criteria for fistula. In our cohort, we considered that a few patients might have benefitted from more extension of the velum as we observed cases with a VP gap. It is conceivable to add lengthening of the oral mucosa to further lengthen the soft palate in our technique, such as by including Z-plasty to the mucosa of the oral side of the soft palate.
The BMMF technique has several demerits. Secondary surgery is needed to cut the perforator of the BMMF. Mann et al. reported no serious complications using a BMMF. 19 Similar to this report, we didn’t have serious complications with a BMMF. But we encountered a few minor complications. Two patients bit the BMMF and complained of severe pain while eating since the BMMF overlapped with the alveolar crest due to postoperative scarring. Other patients might have experienced difficulty brushing the teeth. It will be important to monitor for these issues during the postoperative period.
Limitations
Since this retrospective study was conducted on patients around the age of 5 years, longer observation is needed regarding speech performance. We also observed that the rate of no/mild hypernasality increased in the BMMF group, albeit not significantly. Additional follow-up of larger groups is needed to clarify this and other findings.
Conclusion
Using the two-flap palatoplasty with BMMF method, the rate of an indication for additional speech surgery was decreased significantly by lengthening of the soft palate. The incidence rate of oronasal fistula was also improved significantly by insertion of the well-vascularized BMMF into the nasal soft palate. Two-flap palatoplasty with BMMF may therefore be a good option to improve postoperative outcomes over the conventional technique.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.