
Abstract
Objective
Investigate associations between socioeconomic indicators of healthcare access with family compliance with cleft-related otologic and audiologic care within an interdisciplinary model.
Design
Retrospective case series.
Subjects and Setting
Children born 2005–2015 who presented to the Cleft-Craniofacial Clinic (CCC) at a quaternary care children's hospital.
Interventions
Associations between main outcome measures and Area Deprivation Index (ADI), median household income for zip code, distance from hospital, and insurance status were evaluated.
Main Outcome Measures
Cleft types, ages at presentation to outpatient clinic (cleft, otolaryngology, and audiology), and ages at procedures (first tympanostomy tube insertion (TTI), lip repair, and palatoplasty) were measured.
Results
Most patients were male (147/230, 64%) with cleft lip and palate (157/230, 68%). Median age at first cleft, otolaryngology, and audiology visits were 7 days, 86 days, and 5.9 months, respectively. Private insurance predicted lower no-show rates (p = .04). Age at first CCC visit was younger for patients with private insurance (p = .04) and older for those who lived further from the hospital (p = .002). Age at lip repair was positively correlated with national ADI (p = .03). However, no socioeconomic status (SES) proxy or proximity to hospital was associated with delays in first otolaryngology or audiology examination or TTI.
Conclusion
Once children become established within an interdisciplinary CCC, SES appears to bear little influence on cleft-related otologic and audiologic care. Future efforts should aim to elucidate which aspects of the interdisciplinary model maximize multisystem cleft care coordination and increase access for higher risk populations.
Introduction
Delay of multidisciplinary treatment for children with non-syndromic orofacial cleft palate ± cleft lip (CP ± L) is associated with long-term developmental consequences affecting hearing, speech, swallowing, and dentition. Higher incidences of auditory malformations and subsequent problems with sound perception and speech progression make otologic and audiologic care a special priority during the child's first months of life. 1 Accordingly, the American Cleft Palate-Craniofacial Association (ACPA) recommends that children with CP ± L receive otologic care beginning at birth and audiologic evaluation by age 3 months or 9 months depending on results of newborn hearing screening (NBHS). 2 While the need for timely, coordinated treatment among multiple specialists may be challenging for many families, it is particularly difficult for those with limited resources. Caregivers from less privileged households have greater difficulty taking time off from work, obtaining reliable transportation to appointments, finding childcare for other children in the household, and covering direct and indirect costs with higher incidences of insurance coverage disruptions.3–6 Reducing barriers to care in patients of lower socioeconomic status (SES) is especially important given known associations between indicators of poverty and higher incidences of CP ± L, creating cyclic deleterious effects. 7
Multidisciplinary and interdisciplinary cleft clinics, pioneered by Dr. Herbert Cooper in 1938 and standardized using guidelines set forth by the ACPA in 1993, provide a centralized hub for cleft-related care.8,9 Modern craniofacial teams generally consist of cleft surgeons, orthodontists, audiologists, speech language pathologists, social workers, and more. 2 Though multiple surgical specialties are not required as part of the core team, access to otolaryngology subspecialty care is required for patients seen within an ACPA approved cleft center. 2
Our institution's Cleft-Craniofacial Clinic (CCC) care team composition reflects our aforementioned description of modern craniofacial teams. Our CCC began in the 1950s and has maintained longstanding team approval through the commission on approval of teams from the ACPA. 10 We provide virtually all cleft care in our greater metropolitan area and serve as a quaternary referral center for CCCs in the greater region. Our system for cleft-related otologic and audiologic care has remained consistent throughout our study period and is described here. Approximately half of our CCC appointments have an otolaryngologist embedded into the visit, while the remainder of patients see an otolaryngologist on the same day in an adjacent, on-site clinic. In addition, an audiologist is available at every CCC visit and may evaluate the patient in response to various prompts, including: failed hearing screening, clinician request at last visit, and/or clinician or parental concern regarding problems with hearing or communication on the day of the visit. In the absence of these prompts, patients receive audiology evaluation annually until reaching kindergarten at which point screening occurs through the school system.
Compared to non-interdisciplinary or standard multidisciplinary treatment, team care led by a designated care coordinator has been shown to streamline CP ± L-related treatment, reducing lapses in care while simplifying the lives of patients and families.2,8,9,11,12 For example, Austin et al. 12 found that children who were under the care of an individual provider had fewer surgeries and were less likely to have an audiologic examination in the last year compared to those receiving interdisciplinary treatment. However, even in the setting of interdisciplinary care, the literature is clear that children of lower SES and non-White race are at greater risk for higher incidences of delays in cleft repair.13–17 In addition, multiple studies have shown that lower SES is associated with larger lapses in otologic and audiologic treatment in children without cleft.18–22 Together, this demonstrates that lower SES pediatric populations face discrete disparities in cleft repair as well as in otologic and audiologic treatment. However, there has been virtually no work exploring whether lower SES predicts delays in otologic and audiologic care within cleft populations specifically. Furthermore, it is important to investigate this question within an interdisciplinary model as this is the gold standard endorsed by the ACPA to achieve holistic cleft care.2,23 The purpose of this study is to evaluate associations between socioeconomic indicators and markers of healthcare access with family compliance with cleft-related otologic and audiologic interdisciplinary care. We also assessed outcomes specific to cleft treatment in our investigation to provide comparability with populations previously described in the literature. We hypothesized markers of lower SES would be associated with delayed age at first cleft, audiology, and otolaryngology visit and corresponding surgical management.
Materials and Methods
A protocol to perform a retrospective case series was approved by the institutional review board of the University of Pittsburgh (#20060032). All patients born between 2005 and 2015 who presented to the CCC at a quaternary care children's hospital were initially included. Charts from 732 consecutive children were reviewed. Children with intact secondary palate (n = 168) and loss to follow-up after palatoplasty (n = 153), cleft care at an outside hospital (n = 67), first visit to CCC after 12 months of age (eg, due to adoption or relocation) (n = 5), and staged repair of the hard and soft palate (n = 1) were excluded. In addition, some comorbidities that could contribute to delayed care independent of SES, including genetic disorders such as 22q11.2 deletion syndrome and/or other significant medical complexity (n = 108), were excluded. The remaining 230 patients with CP ± L were included in analysis.
Patient demographics including sex assigned at birth, self-reported race, ethnicity, preferred language and religion, home address, and private vs public insurance were collected from the electronic medical record. Ages at presentation to outpatient clinic (cleft, otolaryngology, and audiology), ages at procedures (lip repair, palatoplasty, first tympanostomy tube insertion (TTI)), admission to neonatal intensive care unit (NICU) and transitional infant care, cleft type (cleft palate only, CP; unilateral cleft lip and palate; or bilateral cleft lip and palate), Veau classification, and NBHS results were also collected during chart review. Number of no show, cancelled, and completed visits with the CCC were recorded from scheduling records, and percentage of no show visits was calculated as

Categorical data were summarized as frequency (n) and percentage. Continuous data were not normally distributed (Shapiro-Wilk p < .05 for all continuous measures) and were summarized as median (range). Associations between patient characteristics, ages at presentation to clinic, and procedures and no shows, ADI, MHI, poverty, educational attainment, distance from the hospital, insurance status, race, ethnicity, preferred language, and religion were evaluated using Chi-squared tests, Spearman correlation, and Wilcoxon rank-sum tests. Stata/SE16.1 (StataCorp, College Station, TX) was used for all tests.
Results
Most patients were male (147/230, 64%) and had cleft lip and palate (CLP; 157/230, 68%) (Table 1). The majority of our patients were White, non-Hispanic (96%) and spoke English as a primary language (97.4%). Despite this homogeneity, children using private insurance were 56%, median national ADI was 66 (range 2–100), median state ADI was 6 (range 1–10), and MHI was $54,342 (range $23,342-$150,800), reflecting a socioeconomically diverse population (Supplementary Table 1). Median age at first cleft, otolaryngology, and audiology visits were 7 days, 86 days, and 5.9 months, respectively (Table 1). For those with CLP, median age at lip repair was 6 months (range 3–13.5 months) (Table 1). Median age at palatoplasty was 12.6 months (range 8.8–21.9 months) (Table 1). In the 228 patients with TTI, first TTI occurred at a median age of 6.1 months (range 1.6–19.3 months) (Table 1).
Patient Characteristics (N = 230).
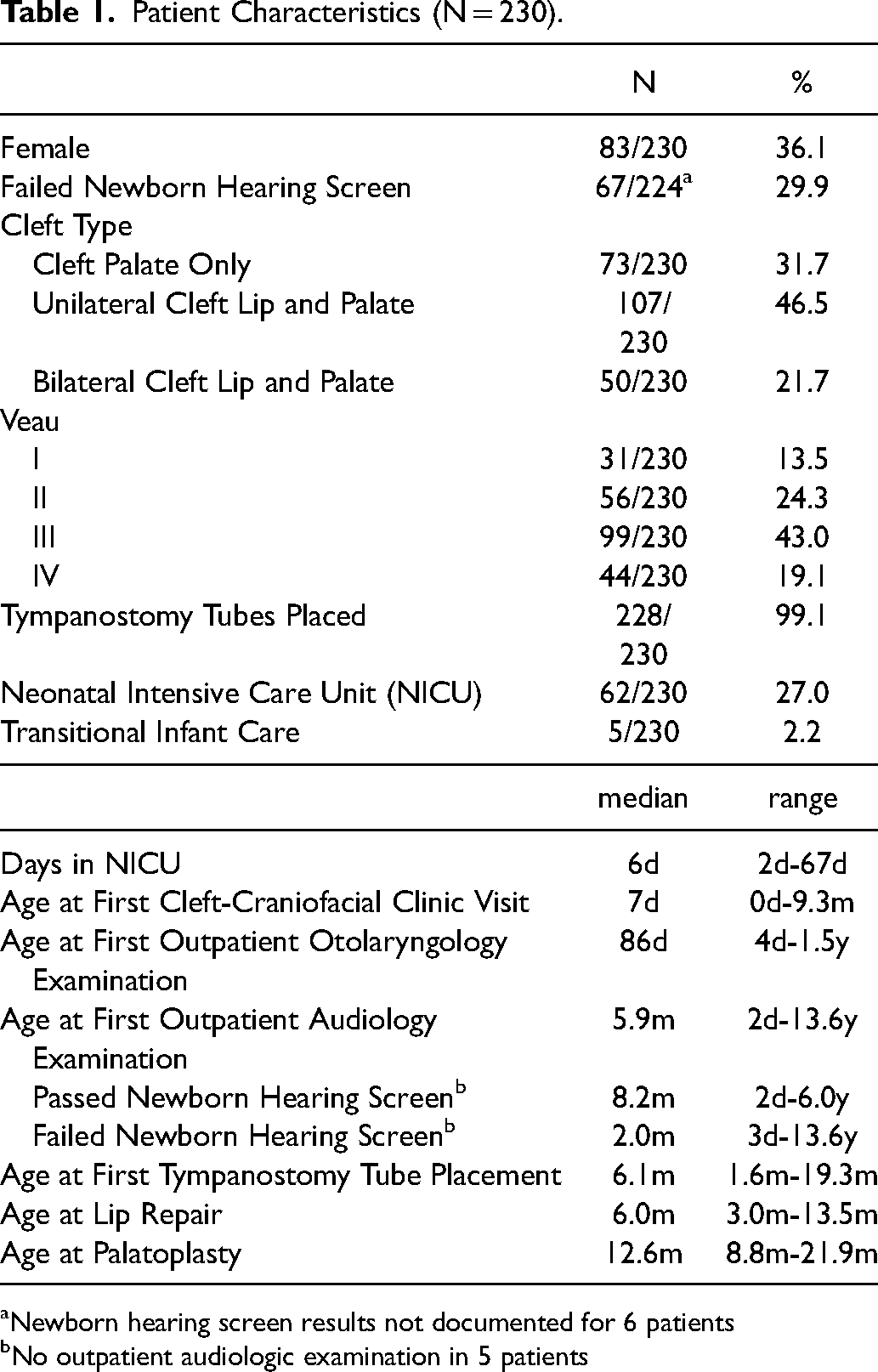
Newborn hearing screen results not documented for 6 patients
No outpatient audiologic examination in 5 patients
Pennsylvania Hearing Screening and Intervention program follows guidelines set forth by the Infant Hearing Education, Assessment, Reporting and Referral Act with benchmarks of hearing screening, diagnosis, and treatment or intervention within 1, 3, and 6 months of life, respectively. Newborn hearing screening (NBHS) should enable timely audiology evaluation. Patients with referred NBHS for at least 1 ear were significantly younger at first audiology examination compared with those who passed their NBHS (z = 5.81, p < .001). Therefore, sub-analyses were performed separately in the failed and passed NBHS groups for this outcome. Similarly, patients admitted to the NICU were significantly older at first CCC visit (18.5 days, range 0–173 days vs 6 days, range 1–283 days, z = -7.17, p < .001) (Supplementary Table 2) and palatoplasty (median 13.1 years, range 9.6–21.9 years, vs median 12.4 years, range 8.8–19.3 years, z = -2.68, p = .008) (Supplementary Table 2) compared with those who were not admitted to the NICU. Therefore, sub-analyses were performed separately in the NICU and no NICU groups for these outcomes.
Age at first CCC visit was younger for patients with private insurance compared with public insurance only (p = .04) (Figure 1). Age at first CCC visit was positively correlated with greater state ADI (rho = 0.259, p = .04) (Figure 2) and longer distance from home address to the hospital (rho = 0.237, p = .002) (Figure 3). In patients with NICU admission, age at first CCC visit was also negatively correlated with MHI (rho = -0.134, p = .04) (Supplementary Figure 1). Age at lip repair was positively correlated with national ADI (rho = 0.173, p = .03) (Figure 4). Finally, no shows to CCC were less common in patients with private insurance compared to those with public insurance only (p = .04) (Figure 5). However, no socioeconomic proxy or proximity to the hospital was associated with a delay to first otology or audiology examination or TTI (Supplementary Tables 2 and 3). Associations between any care delays with race, religion, or preferred language were not found. However, sample sizes of non-White, non-English speakers in our study were too small to beget significance (4.4% and 2.6%, respectively). In addition, religion was inconsistently reported, with only Christian denominations specified and all others classified as other (41.3%), none (31.7%) or not listed (.9%), making conclusions regarding non-Christian religions challenging.
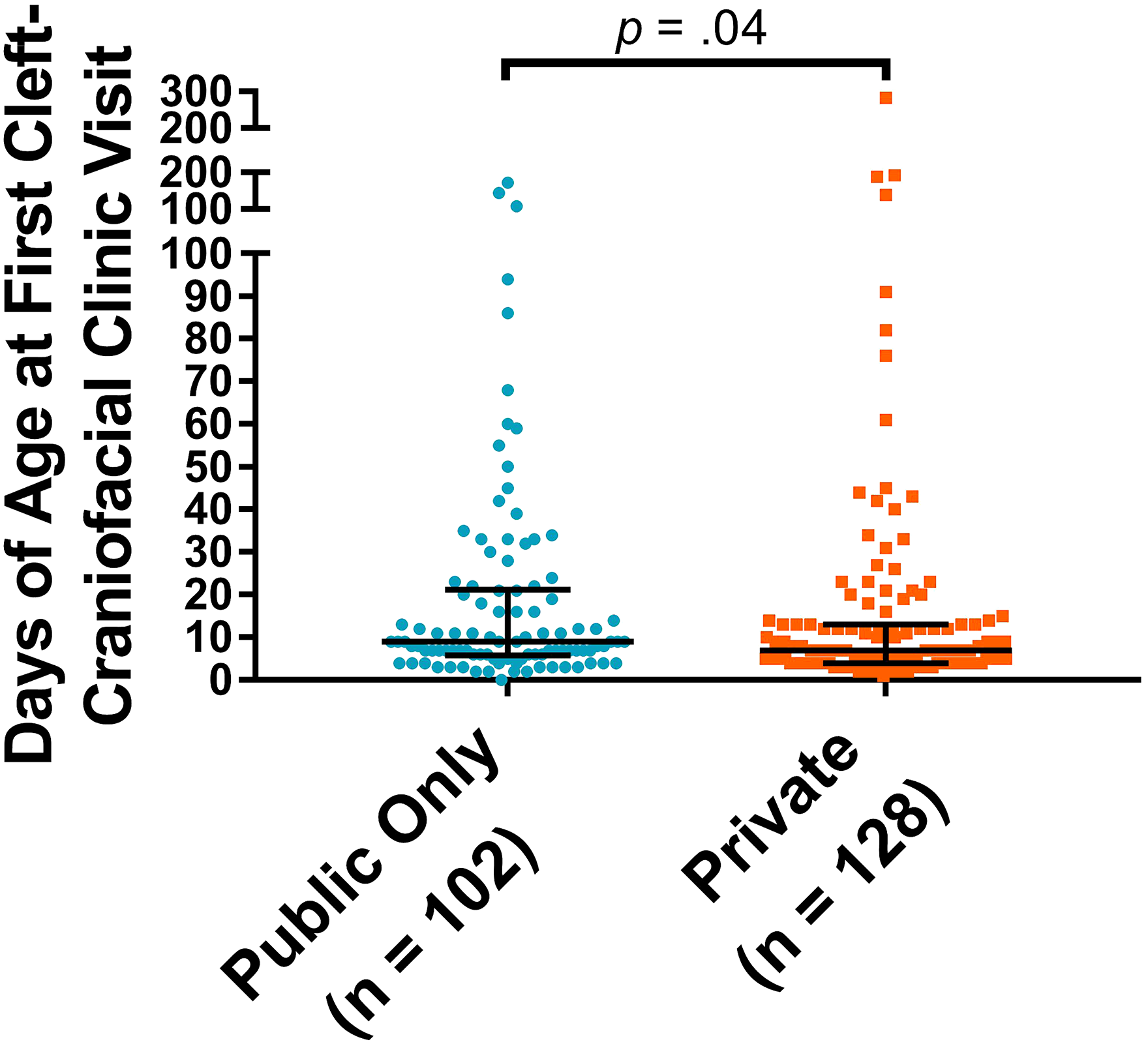
Patients with private insurance were younger at first cleft visit compared with those with public insurance only (median 7 days, range 1 day-9.3 months vs median 9 days, range 0 days-5.7 months). Bars show median and interquartile range.
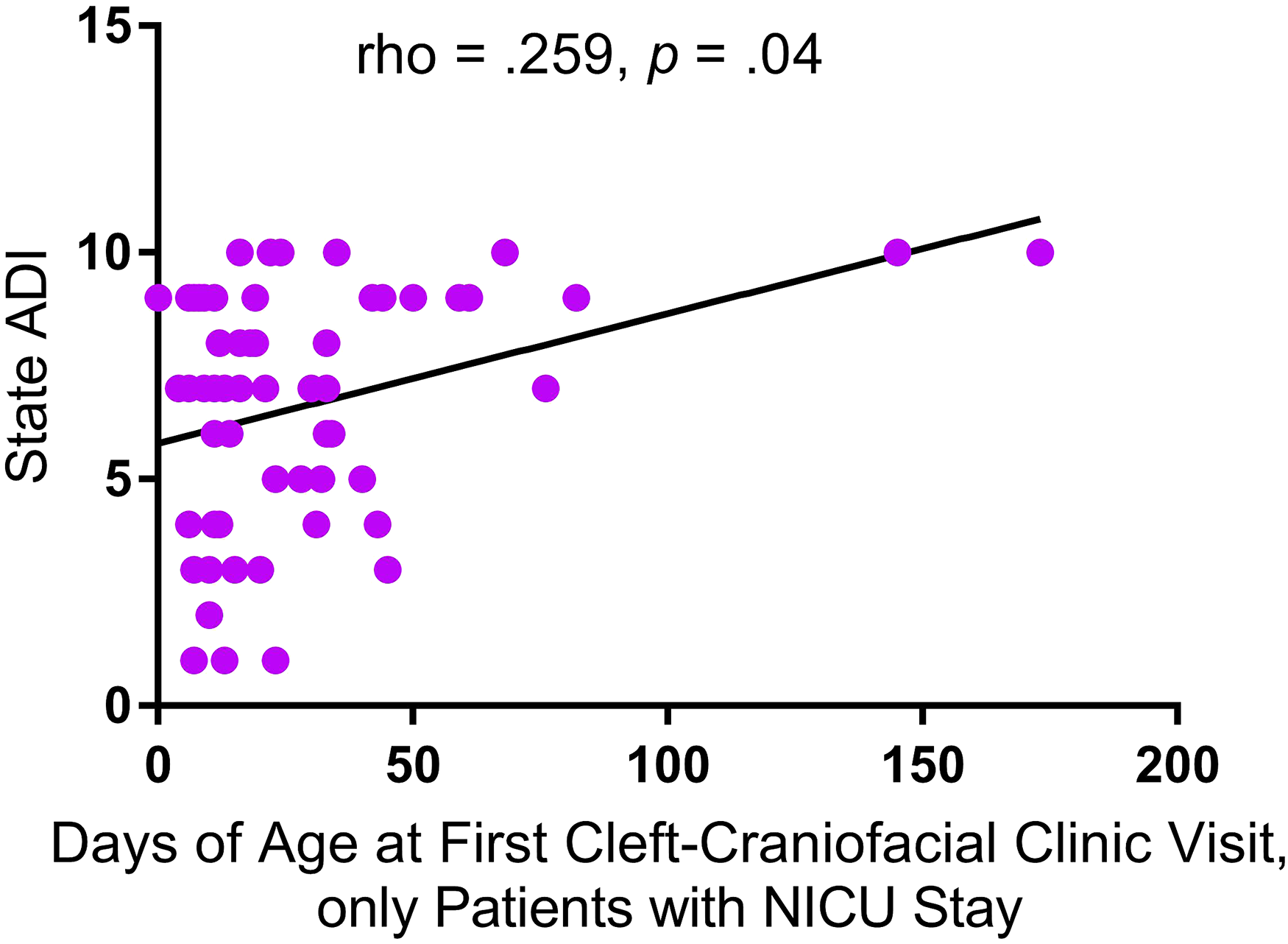
Greater state area deprivation Index (ADI) was associated with older age at first cleft-craniofacial clinic visit.
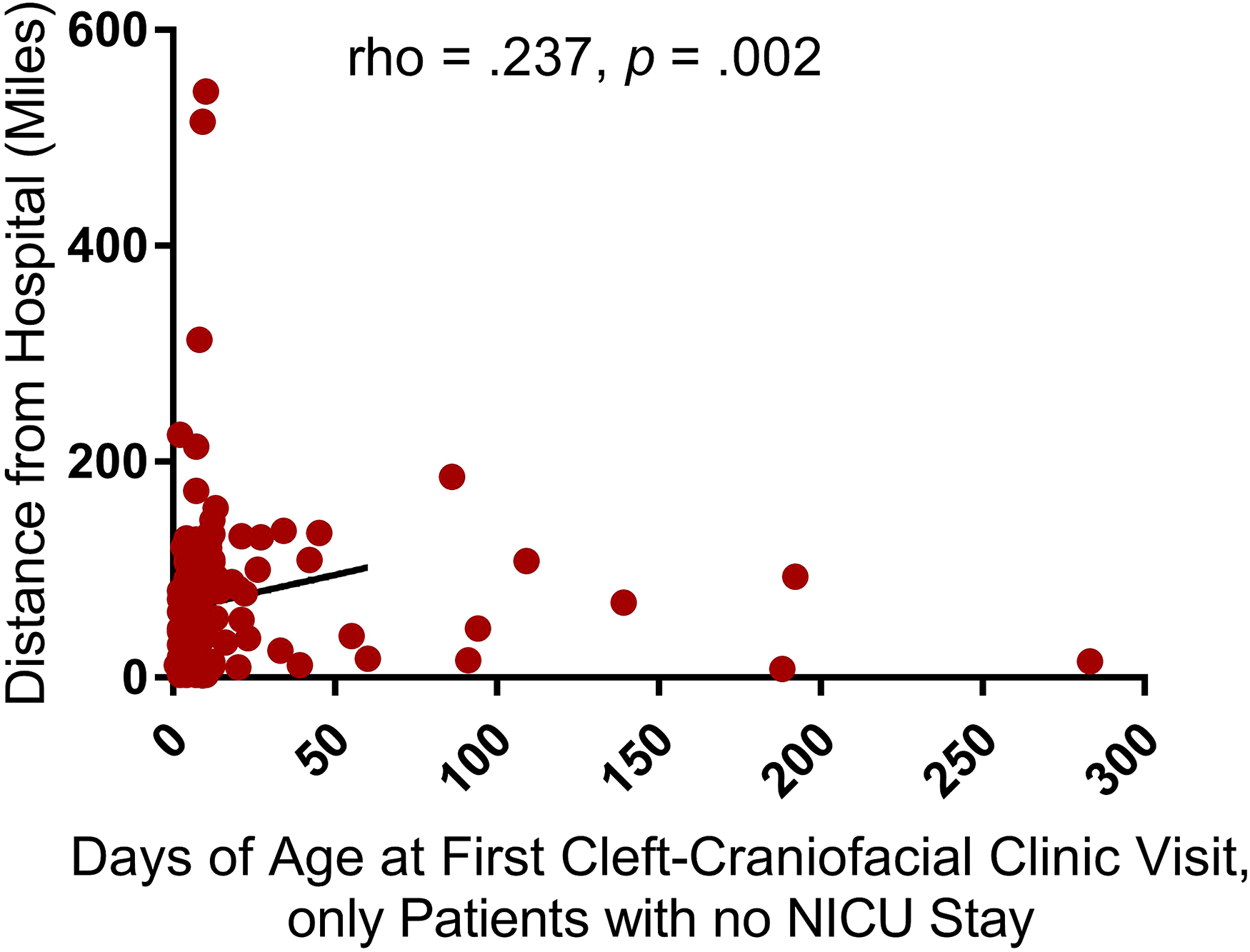
Longer distance from the hospital was associated with older age at first cleft-craniofacial clinic visit.
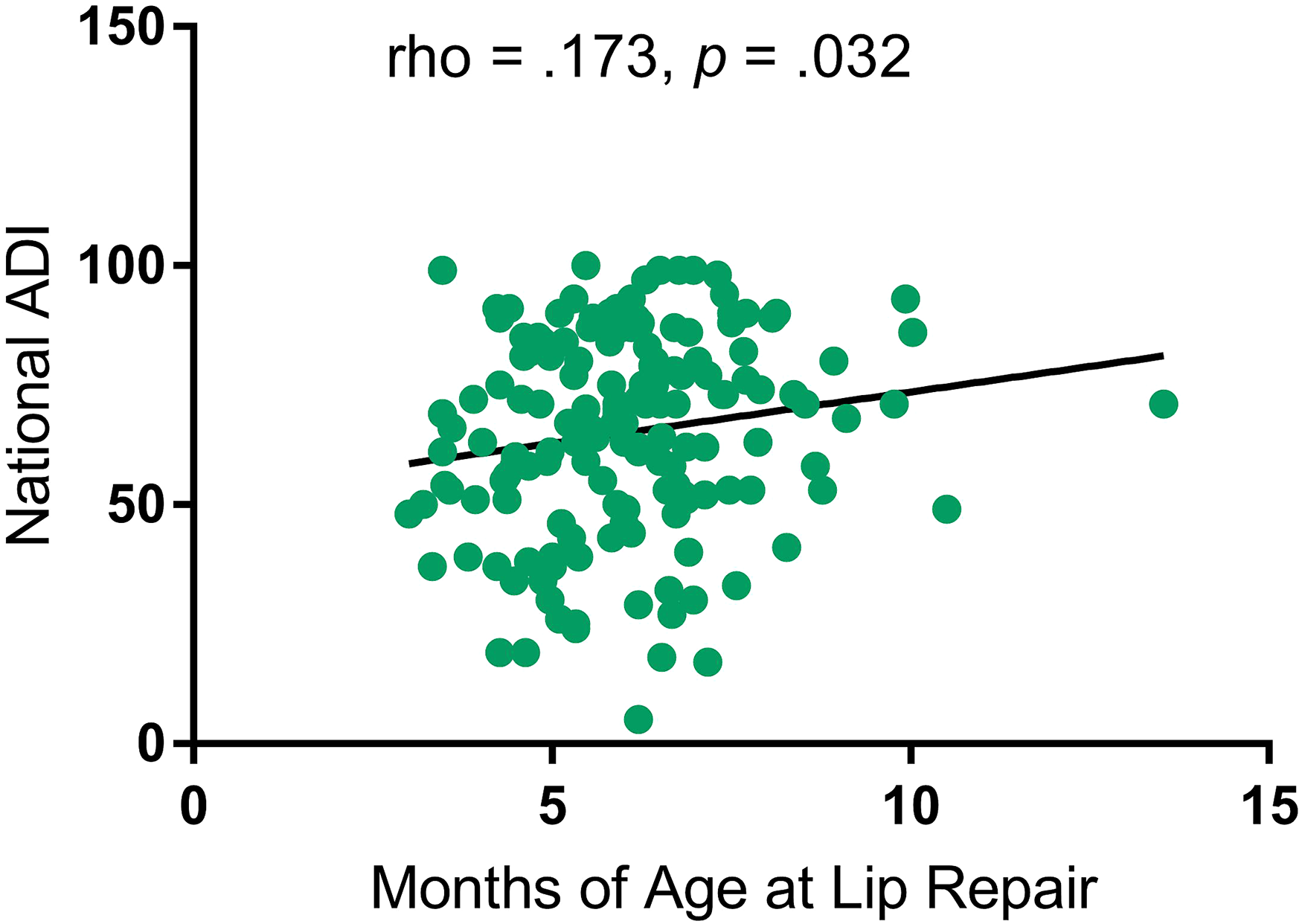
Greater national area deprivation Index (ADI) was associated with older age at lip repair.
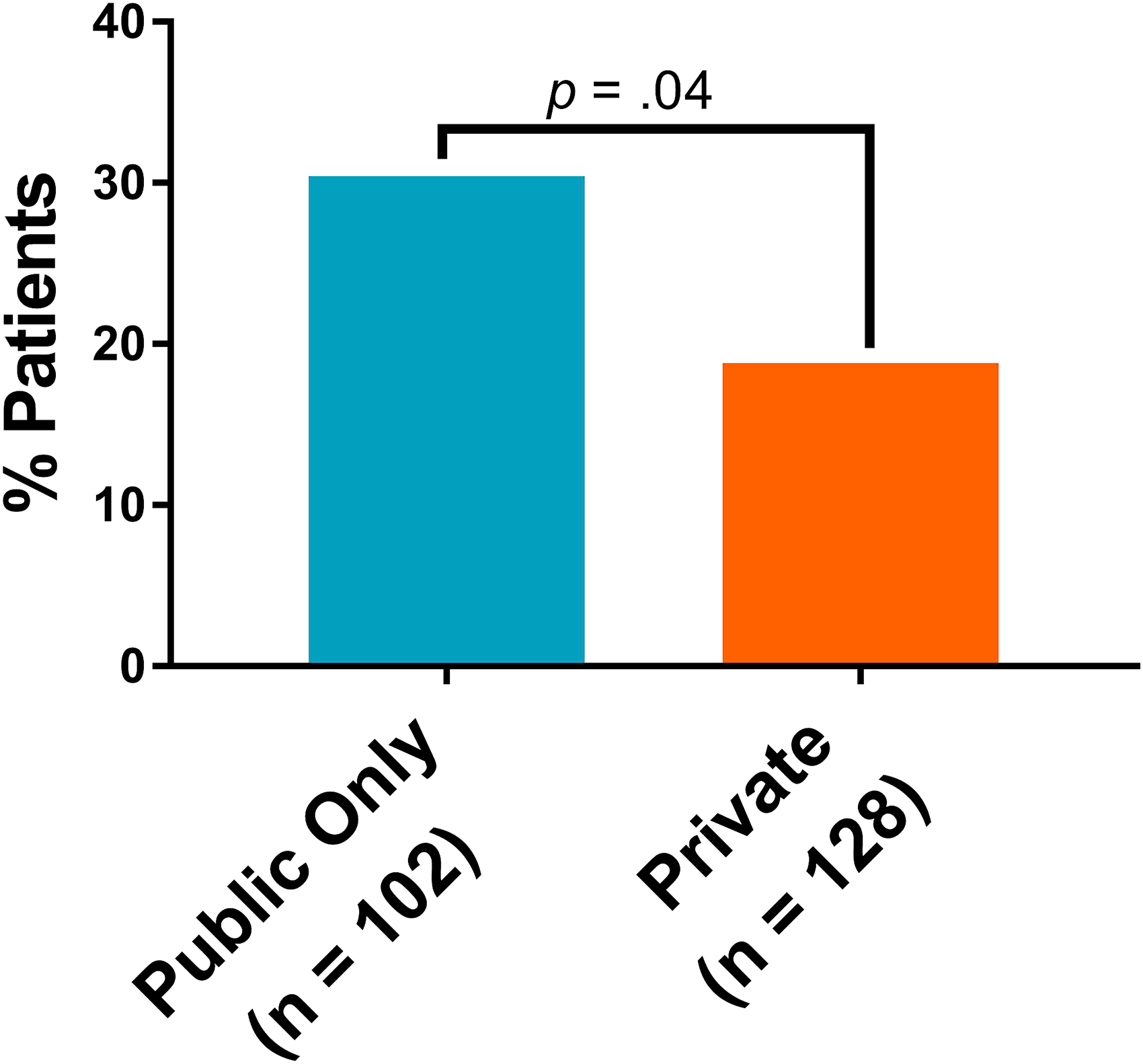
No shows to cleft-craniofacial clinic were less common in patients with private insurance (24/128, 18.8%) compared to those with public only insurance (31/102, 30.4%) (p = .04).
Discussion
Interdisciplinary cleft teams following ACPA guidelines are designed to optimize treatment uniformity and mitigate delays in care for children with CP ± L. While research has shown that lower SES predicts delays in cleft repair despite interdisciplinary coordination,13–15,26 the influence of SES on timely audiologic and otologic management in interdisciplinary cleft care remains largely unexplored. The present work identifies important associations between proxy measures of lower SES and healthcare access with delays in care for children with CP ± L in an interdisciplinary CCC; a cohort previously described by Shaffer et al. 27 Pediatric patients with CP ± L who lack private insurance and live in areas characterized by low MHI and high ADI were more likely to experience delays in establishing care and timing of cleft lip (CL) repair. Lack of private insurance also predicted durational care discontinuity as reflected in higher rates of appointment no-shows. However, outside of a higher incidence of missed appointments, proxy measures of lower SES were not associated with delays in otologic or audiologic management. These findings largely contradict our hypothesis that markers of lower SES predict delays in cleft-related audiology and otology treatment. Instead, our results suggest that SES bears little influence within interdisciplinary otologic and audiologic care in cleft populations.
In our cohort of 230 patients, most were male and had CLP. This is consistent with national trends which show higher cleft incidences in males vs females as well as of CLP vs CL or CP alone.28–30 The average age to first CCC appointment was 7 days. In patients without NICU admission, lack of private insurance, lesser affluence as reflected in lower MHI and higher ADI, and further distance to the hospital all predicted older age at first CCC visit. In comparison, Zaluzec et al. 26 reported an average age of first CCC appointment to be 1 month but found no differential impact according to insurance type. While the reason for this dissimilarity is unclear, it may be related to differences in the prevalence of private insurance between the authors’ study and our own (15% vs 56%, respectively). Distance to CCC, although not a proxy for lower SES, appears to be a notable barrier in practice settings such as ours which is the only children's hospital serving our large geographic region. Of those admitted to the NICU, patients were more likely to be older at first appointment if they lived in a neighborhood of lower MHI. Studies have demonstrated several associations between hearing loss and indications associated with NICU admission, including: sepsis, mechanical ventilation, loop diuretic or vancomycin use, premature birth, low birth weight, and critically elevated bilirubin.31–33 Furthermore, mechanical ventilation is a known confounder in auditory brain stem response testing, placing patients who require mechanical ventilation at an even greater risk for delays in auditory evaluation.34,35 Therefore, children of lower SES with cleft and NICU admission may be particularly vulnerable to audiologic care delays and may benefit from referral prior to first CCC appointment.
The average age to establish care with an otolaryngologist and an audiologist was 86 days and 5.9 months, respectively. 208/230 (90%) patients were seen by an otolaryngologist within 6 months. 41/63 (65%) children who failed NBHS were seen by an audiologist within 3 months while 90/156 (58%) of those who passed NBHS were seen by an audiologist within 9 months. The authors’ review of the literature yielded no directly comparable data specific to cleft populations. However, in a report which investigated 704 appointments conducted in a multidisciplinary, urban cleft program, Dahiya et al. 23 found that 125/338 (37%) appointments which failed to occur within ACPA-recommended timeframes were delayed because of untimely audiology and/or otolaryngology visits.
Lip repair marks the first surgical encounter for most of our patients and serves to optimize aesthetic appearance and facial growth while also improving oral structural integrity for patients who require future palatoplasty. 26 In addition, it provides an opportunity for parents of children with CLP to discuss palate repair planning with their cleft surgeon. 13 Our median age at lip repair was 6.0 months with 156/157 (99%) patients receiving repair within the ACPA recommended latest age of 12 months. 2 This is slightly later than recent studies which show median ages of lip repair at 4.5 months, 30 4.7 months, 26 and 5.6 months. 15 On average, we found that patients residing in less affluent neighborhoods characterized by a higher national ADI were older at lip repair. Separate works have identified minority race, non-English native language, and child protective service involvement as additional predictors of delayed lip repair.26,30
Delay in CP repair may be even more consequential than CL repair given its association with velopharyngeal insufficiency leading to long-term atypical speech production. 36 Furthermore, studies have shown that patients with CP and delayed palatoplasty develop compensatory speech patterns which are more likely to be refractory to speech therapy and result in chronic problems with articulation, hypernasal resonance, and glottal stops.13,36 Consequently, the ACPA recommends surgery no later than 18 months of age. 2 Our median age at palatoplasty was 12.6 months with 224/230 (97%) patients receiving palate repair before age 18 months and 100% before age 22 months. Comparable studies have found average ages of palatoplasty at 12.1 months, 13 13.5 months, 30 14.1 months, 26 and 21.6 months. 15 Harb et al. 13 found associations between timing of CP repair with race and income. In their study, White children received palatoplasty on average 0.7 months before Black children and children born into the highest (> 75th percentile) income bracket received palatoplasty 0.8 months earlier than those in the lowest (< 25th percentile) income bracket. 13 Similarly, Abbott et al. 16 identified non-White race and public insurance as predictors of slightly older age at palatoplasty (1.5–3.5 weeks and 1.2 weeks, respectively). In the present study, age at palatoplasty was not significantly associated with any SES proxy, even when looking at the CP only subgroup (data not shown). An important distinction between our study and those mentioned is a difference in specificity to interdisciplinary care. That is, our study population exclusively received interdisciplinary care while the aforementioned studies’ populations lacked care model uniformity.13,16 While the reasons for these variances are likely multifactorial, our lack of association between age at palatoplasty and SES proxy suggests that once patients become established in an interdisciplinary clinic, a higher level of care coordination may mitigate SES-associated disparities.
In general, the relationship between low SES and missed appointments is well documented in the literature.21,37,38 Low-income families are less likely to have private insurance and are more likely to miss appointments which negatively impacts care quality.20,21 Our study found that children who lack private insurance had a higher rate of missed appointments. No shows were less common in patients with private insurance (24/128, 18.8%) compared to those with public insurance only (31/102, 30.4%) (p = .04). This is consistent with other single-institution studies whose populations received interdisciplinary care26,39 and suggests that barriers for children who lack private insurance persist despite enhanced care coordination.11,16
Associations were found with proxy measures of lower SES and delays in cleft care but not otologic or audiologic management. That is, once patients became established in the interdisciplinary clinic, SES did not appear to influence timing of audiologic and otologic examinations nor TTI. While our review of the literature yielded no studies investigating the influence of SES on cleft-related otologic and audiologic care for direct comparison, these findings are in notable contrast to the delays in otologic and audiologic care typically seen in children of lower SES without cleft. For example, in a pediatric population without cleft, McCoy et al. 21 found that patients with public insurance and patients who lived in neighborhoods with lower MHI experienced delays between otologic consult and TTI. The authors also showed that patients with public insurance had TTI at an older age compared to those with private insurance. Similarly, in a separate study on children without cleft, Zhang et al. 22 found that patients who lacked private insurance and were of non-White race had comparatively greater delays in auditory examination.
As a retrospective case series using proxy measures for SES, this study has many limitations. Firstly, our study was not designed to delineate to what degree this lack of association between SES and cleft-related otologic and audiologic management is due to interdisciplinary care. However, our results support the merit of this model as the gold standard for multisystem cleft care. 2 In addition, demographic variables such as race, insurance type, and zip code provide indirect measures of SES and fall short of characterizing the complexity of unique individual environments. Our data rely on the veracity of medical records and accuracy of patient-reported information which may be considered sensitive such as preferred language, race, religion, and home address. For example, patients may not disclose a non-English preferred language due to concern for receiving lower quality care.40,41 Additionally, our study is missing data. Race and ethnicity were declined or unspecified for 6 patients, preferred language was unspecified in 5 patients and religion was unspecified in 2 patients. MHI (n = 4), poverty and education level (n = 4), and distance from hospital (n = 1) were missing for patients due to relocation out of state or unavailability of census information. Due to our inherently limited patient population, the sample size was driven by all available patients born during a 10-year interval rather than an a priori power analysis. Finally, the generalizability of our study is limited by its specificity toward urban, quaternary centers which serve a large geographic area and because our patient demographic is mostly White, non-Hispanic, and speaks English as a preferred language.
Conclusion
This study examined the influence proxy measures of SES and healthcare access have on timely cleft, otologic, and audiologic care at a single institution interdisciplinary CCC. Associations were found between lower SES and delays in cleft treatment but not otologic or audiologic treatment, suggesting that interdisciplinary care may play a role in mitigating SES influence on cleft-related otologic and audiologic management. It is important to recognize that interdisciplinary care reflects a dynamic care model made of many intercalating parts. Therefore, future efforts should aim to elucidate which aspects of the interdisciplinary model maximize multisystem cleft care coordination and increase access for higher risk populations.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231186275 - Supplemental material for Social Determinants of Health in Early Otologic and Audiologic Evaluation in an Interdisciplinary Cleft-Craniofacial Clinic
Supplemental material, sj-docx-1-cpc-10.1177_10556656231186275 for Social Determinants of Health in Early Otologic and Audiologic Evaluation in an Interdisciplinary Cleft-Craniofacial Clinic by Daniel R. Awad, Noel Jabbour, Matthew Ford, Jennifer L. McCoy, Jesse A. Goldstein and Joseph E. Losee, Amber D. Shaffer in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656231186275 - Supplemental material for Social Determinants of Health in Early Otologic and Audiologic Evaluation in an Interdisciplinary Cleft-Craniofacial Clinic
Supplemental material, sj-docx-2-cpc-10.1177_10556656231186275 for Social Determinants of Health in Early Otologic and Audiologic Evaluation in an Interdisciplinary Cleft-Craniofacial Clinic by Daniel R. Awad, Noel Jabbour, Matthew Ford, Jennifer L. McCoy, Jesse A. Goldstein and Joseph E. Losee, Amber D. Shaffer in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656231186275 - Supplemental material for Social Determinants of Health in Early Otologic and Audiologic Evaluation in an Interdisciplinary Cleft-Craniofacial Clinic
Supplemental material, sj-docx-3-cpc-10.1177_10556656231186275 for Social Determinants of Health in Early Otologic and Audiologic Evaluation in an Interdisciplinary Cleft-Craniofacial Clinic by Daniel R. Awad, Noel Jabbour, Matthew Ford, Jennifer L. McCoy, Jesse A. Goldstein and Joseph E. Losee, Amber D. Shaffer in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-4-cpc-10.1177_10556656231186275 - Supplemental material for Social Determinants of Health in Early Otologic and Audiologic Evaluation in an Interdisciplinary Cleft-Craniofacial Clinic
Supplemental material, sj-jpg-4-cpc-10.1177_10556656231186275 for Social Determinants of Health in Early Otologic and Audiologic Evaluation in an Interdisciplinary Cleft-Craniofacial Clinic by Daniel R. Awad, Noel Jabbour, Matthew Ford, Jennifer L. McCoy, Jesse A. Goldstein and Joseph E. Losee, Amber D. Shaffer in The Cleft Palate Craniofacial Journal
Footnotes
Meeting Information
Presented as poster at the American Academy of Head and Neck Surgery (AAO-HNSF) Annual Meeting in Philadelphia, Pennsylvania from September 10th to 14th, 2022.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.