
Abstract
Objective
We sought to identify differences in 30-day medical and surgical complications in unilateral versus bilateral palatoplasty.
Design
The NSQIP-P 2015-2020 database was queried to identify cleft palate repairs using CPT codes. Cases were stratified as unilateral (Veau III) and bilateral (Veau IV) using ICD-9 and −10 codes.
Setting
A nationally representative random sample.
Patients/Participants
A total of 3791 cases were identified with 2608 undergoing unilateral repair and 1183 undergoing bilateral repair.
Main Outcomes/Measures
The postoperative outcomes of interest included surgical complications (surgical site infections, wound dehiscence), medical complications (pneumonia, urinary tract infection, seizure, cardiac arrest, bleeding/transfusions, systemic sepsis, unplanned intubation), readmission, and reoperation.
Results
The bilateral cohort was older (696 days versus 619 days, P < .001) and had longer operative times (157.3 min versus 144.5 min, P < .001). The unilateral cohort had more comorbidities including developmental delay, structural CNS abnormalities, need for nutritional support, and bleeding disorders. The bilateral cohort had statistically significant higher occurrences of wound dehiscence (2.1% versus. 1.2%, P = .03) and readmission (3.2% versus 1.7%, P = .01). On multivariate analysis, bilateral cleft repair (OR: 1.83, CI: 1.176-2.840, P = .007) and ASA class 4 (OR: 13.1, CI 2.288- 62.586, P = .002) were associated with greater odds of readmission.
Conclusion
Patients who underwent bilateral cleft repair had a higher proportion of 30-day postoperative complications and a two-fold increased odds of readmission. While palatoplasty is generally regarded as a safe procedure in the pediatric population, identifying factors related to an increased risk of early postoperative complications can help surgical teams better manage high-risk individuals.
Introduction
Orofacial clefting is one of the most common craniofacial abnormalities occurring in 1:500 to 1:2000 births. 1 When left untreated, cleft palate impairs oral competence, delays speech development, and leads to feeding difficulties. 2 Caused by unsuccessful embryonic facial fusion, cleft palate can occur in varying degrees of severity, ranging from a bifid uvula to complete clefting through the soft and hard palates and alveolar ridge. The Veau classification is used to describe cleft palate subtypes, with Veau III describing a unilateral complete cleft of the soft palate, hard palate, and alveolus, while Veau IV is a bilateral complete cleft of the soft palate, hard palate, and alveolus.3,4
Cleft palate repair is an integral part of treatment for children born with orofacial clefts. In a palatoplasty, the nasal and oral mucosal layers of the defect are each approximated in the midline to ensure soft-tissue closure of the defect, typically via a local mucoperiosteal flap. Due to the possibility of maxillary growth restriction with primary bone grafting during palatoplasty, surgeons conventionally opt not to close the bony defect of the cleft palate, though this varies by institution.5,6 Surgical repair of the cleft lip and palate is frequently performed within the first 1-2 years of a child's life, however the timing and staging of palatoplasty vary between cleft centers as the level of evidence for surgical and perioperative management is widely contested, particularly as they relate to functional outcomes.7–11
Palatoplasty is associated with various early, late, and long-term functional outcomes. Wound related complications are a serious and feared early complication in palatoplasty. Wound dehiscence, fistulas, secondary hemorrhage, and systemic infection can prolong hospital stay and necessitate additional interventions.12,13 However, literature regarding palatoplasty tends to focus on late complications such as the development of oronasal fistulas and velopharyngeal insufficiency (VPI) as well as long-term functional outcomes including malocclusion and maxillary growth restriction.14–19 While palatoplasty is generally regarded as a safe procedure in the pediatric population, identifying factors related to an increased risk of early postoperative complications can help surgical teams better manage high-risk individuals. We sought to identify 30-day medical and surgical complications in unilateral versus bilateral palatoplasty using a large, national cohort.
Methods
The NSQIP database from 2015 to 2020 was queried to identify all patients who underwent palatoplasty. The NSQIP is a validated national multicenter database capturing 30-day surgical outcomes. 20 In brief, NSQIP data is currently collected at over 700 hospitals in 49 states across the United States. Each case captures HIPAA compliant preoperative, intraoperative, and postoperative items. Therefore, the NSQIP can be viewed as a nationally representative random sample of surgical cases. The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not been verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors. This study was reviewed by the Institutional Review Board at the University of Utah and was considered exempt (IRB_00068446). Informed consent was not obtained as the ACS NSQIP is a de-identified dataset.
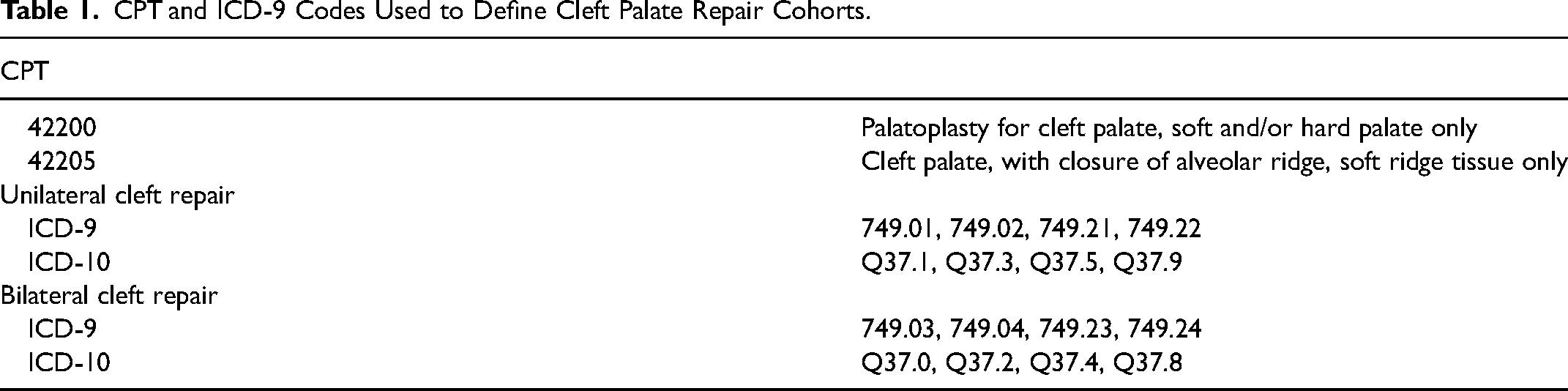
Cases were identified by current procedure terminology (CPT) codes. As CPT codes do not differentiate between unilateral and bilateral cleft repair, International Classification of Diseases, Ninth Revision and Tenth Revision, Clinical Modification (ICD-9-CM and ICD-10-CM) codes were used to identify Veau III (unilateral) and Veau IV (bilateral) morphology (Table 1).
CPT and ICD-9 Codes Used to Define Cleft Palate Repair Cohorts.
Patient demographics, surgical specialty, operative time, total length of stay (LOS), comorbidities, and ASA class were recorded. The postoperative outcomes of interest included surgical complications (surgical site infections, wound dehiscence), medical complications (pneumonia, urinary tract infection, seizure, cardiac arrest, bleeding/transfusions, systemic sepsis, unplanned intubation), readmission, and reoperation.
Statistical Analysis
Univariate analysis was performed using Chi-square tests for comparison of categorical variables and independent Fishers exact tests for comparison of continuous variables. To adjust for baseline differences between each cohort, multivariate analysis was performed using single-step multinomial logistic regression. Covariates for this model included bilateral palate repair, age, operative time, LOS, impaired cognitive status, structural CNS abnormality, need for nutritional support, and ASA class. All analyses were performed using R 4.2.1 (R Foundation, Vienna, Austria) and the p-value for statistical significance was set at P < .05.
Results
Patient Demographics
A total of 3791 patients who underwent unilateral and bilateral palatoplasty between 2015-2020 were identified. Of the cases, 2608 were categorized as unilateral (Veau III) and 1183 as bilateral (Veau IV). Within the unilateral and bilateral cohort, there was a predominance of White patients (66% and 66.4%) as compared to American Indian or Alaska Native (1% and 0.8%), Asian (7.6% and 8.9%) Black (8.2% and 8.4%) or native Hawaiian/Pacific Islander patients (0.7% and 0.4%). The mean age of the unilateral cohort was 1.7 years and the mean age of bilateral cohort was 1.9 years (P < .001). In regard to medical comorbidities, the bilateral cohort had a higher proportion of impaired cognitive status (17.3% v 13.9%, P = .006), structural CNS abnormality (5.5% v 3%, P < .001), need for nutritional support (8.3% v 5.3%, P < .001), and hematologic disorders (1.8% v 0.9% P = .017). Additionally, the bilateral cohort had a higher proportion of patients with an ASA class 3 (14.6%, P < .001). The bilateral cohort also had statistically significantly longer operative time (74.7 min versus 66.7 min, P < .001) and LOS (1.6 days versus 1.5 days, P = .004) than the unilateral cohort. Additional patient characteristics can be found in Table 2.
Unilateral Versus Bilateral Cleft Palate Patient Characteristics.
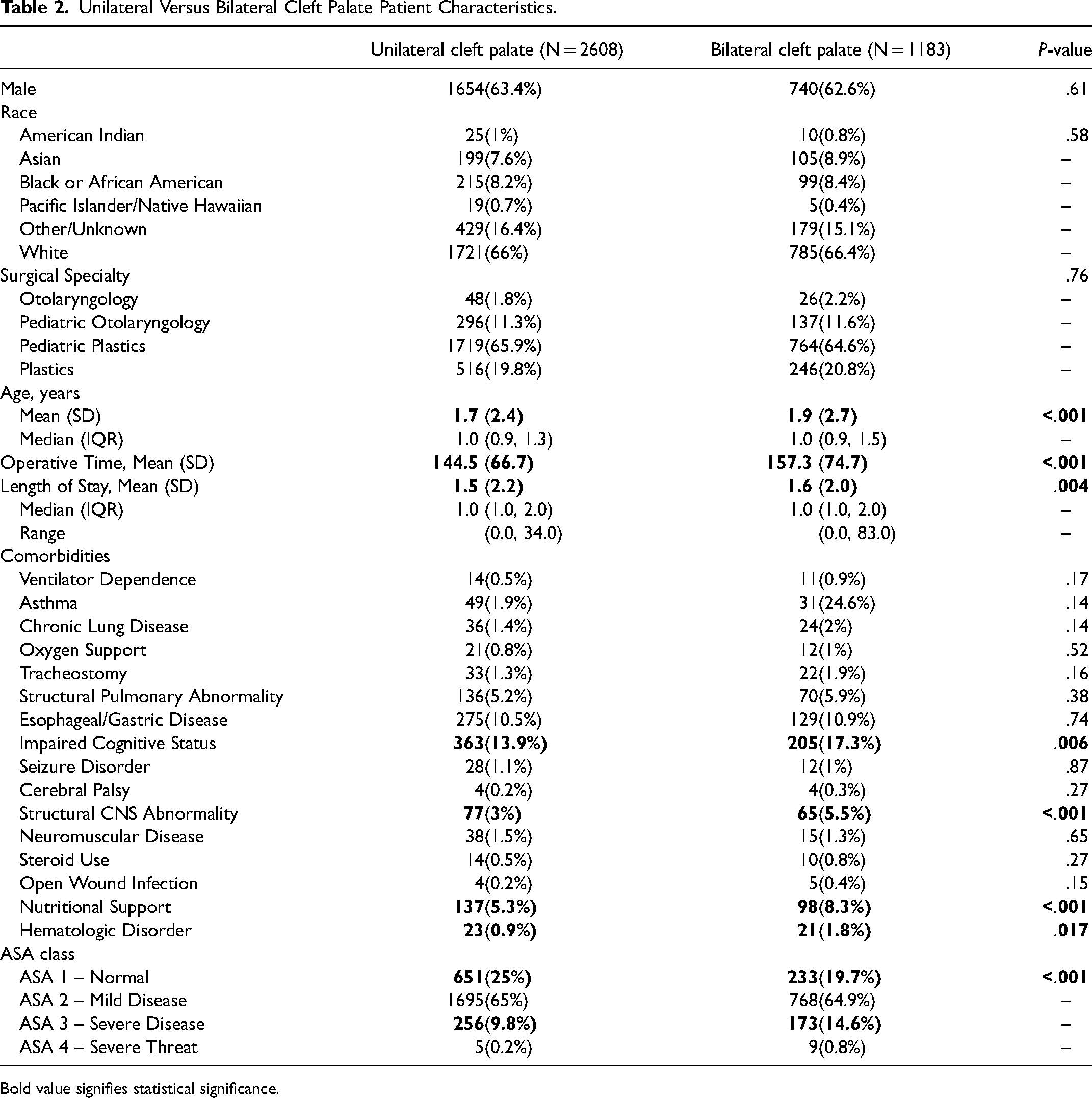
Bold value signifies statistical significance.
Postoperative Complications
Regarding surgical complications, the unilateral and bilateral cohort had low proportions of superficial, deep incisional, and organ space SSI's. The bilateral cohort had a statistically significant higher proportion of wound dehiscence (2.1%, P = .029). In regard to medical complications, both cohorts had low proportions of pneumonia, urinary tract infection, cardiac arrest requiring CPR, bleeding and transfusions, systemic sepsis, and unplanned intubation. The bilateral cohort had a higher proportion of seizures (0.3%, P = .03). Additionally, the bilateral cohort had higher occurrences of readmission (3.2%) when compared to the unilateral cohort (1.7%, P = .004). (Table 3)
Unilateral Versus Bilateral Cleft Palate 30-day Postoperative Complications.
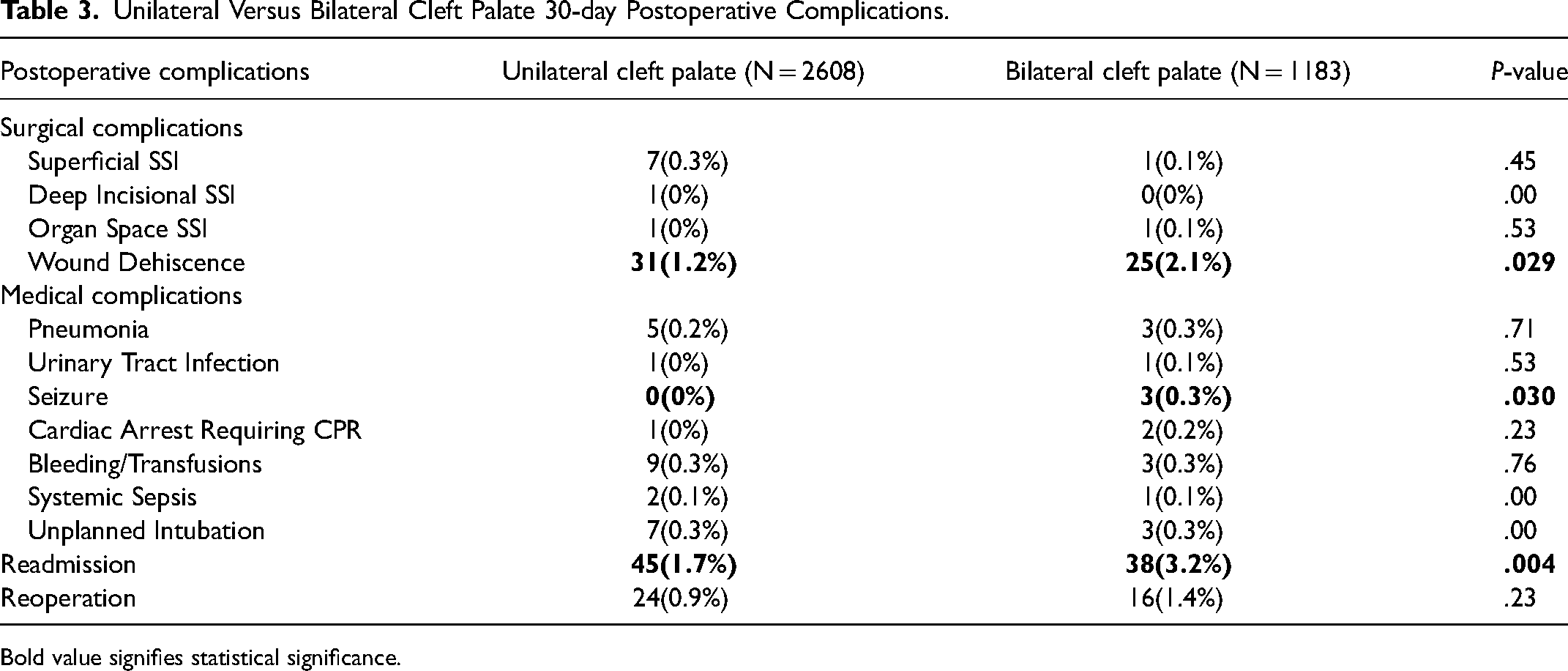
Bold value signifies statistical significance.
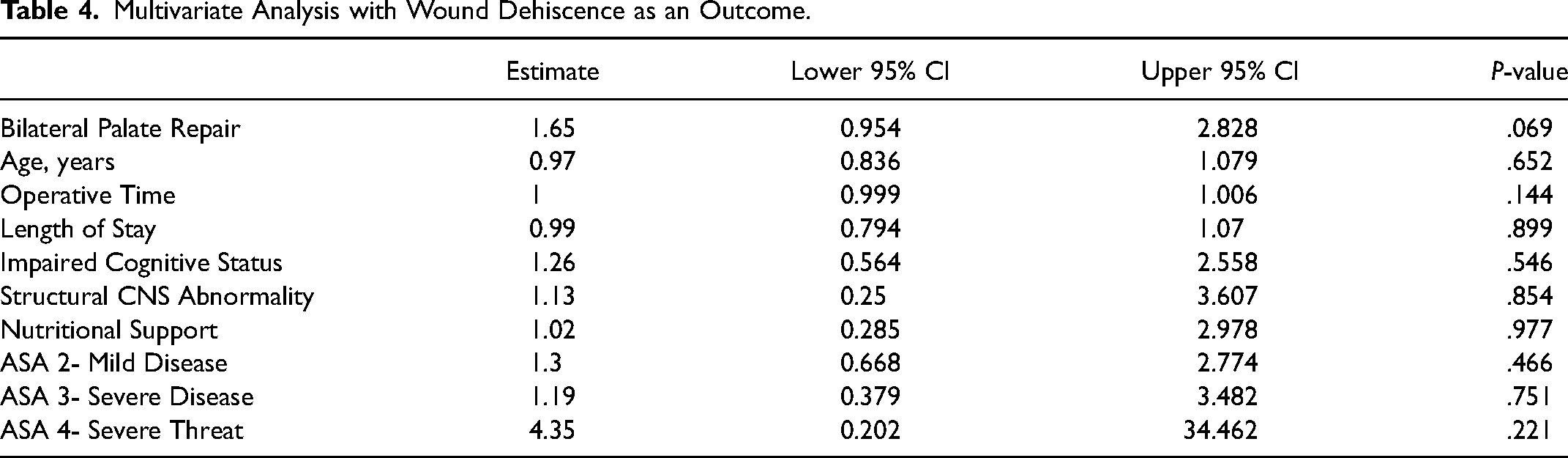
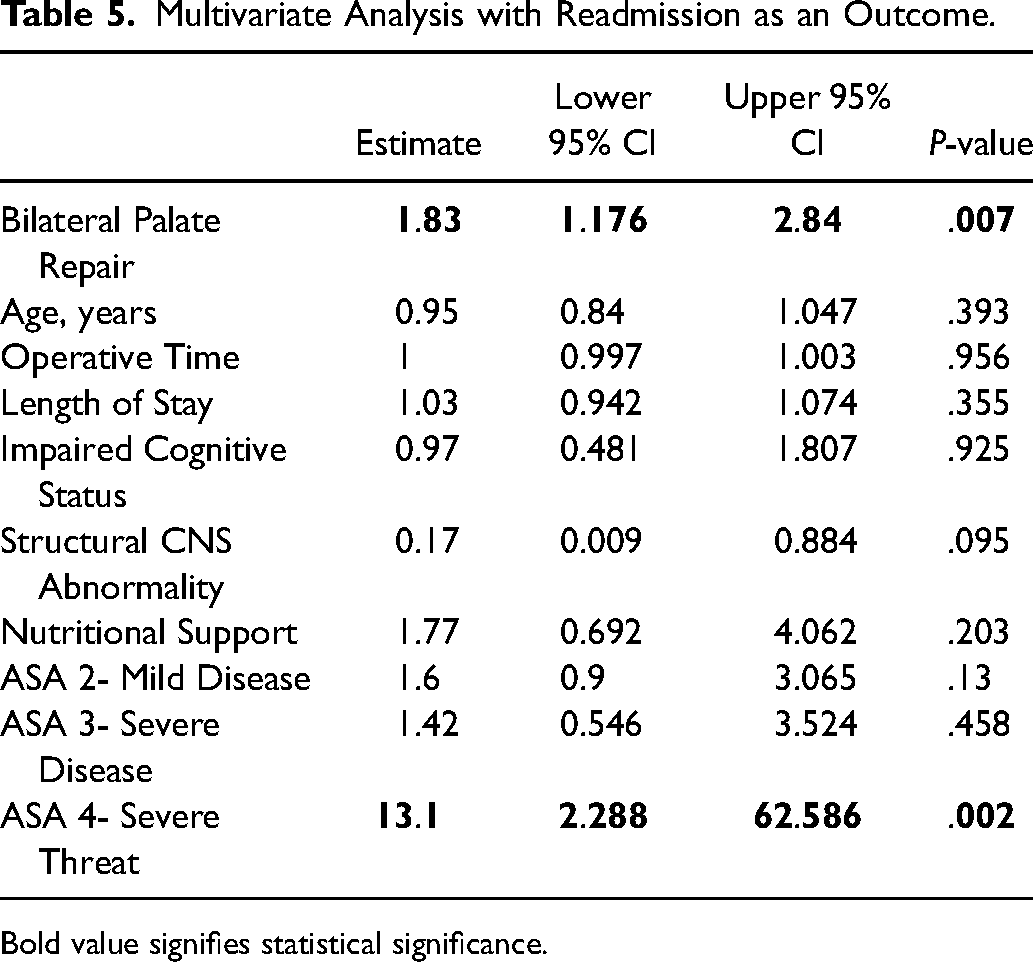
In a multivariate analysis with wound dehiscence as the outcome of interest, bilateral palate repair, age, operative time, LOS, impaired cognitive status, structural CNS abnormality, need for nutritional support, or ASA class were not associated with increased odds (Table 4). In a multivariate analysis with readmission as the outcome of interest, bilateral palate repair was associated with 1.83 times greater odds of readmission (CI: 1.176-2.840, P = .007). Additionally, ASA class 4 was also associated with 13.1 times increased odds of readmission, (CI 2.288- 62.586, P = .002). Readmission was not associated with age, operative time, LOS, impaired cognitive status, structural CNS abnormality, need for nutritional support, or ASA class 2 and 3 (Table 5).
Multivariate Analysis with Wound Dehiscence as an Outcome.
Multivariate Analysis with Readmission as an Outcome.
Bold value signifies statistical significance.
Discussion
Palatoplasty remains a challenging surgical procedure. The risk of significant adverse sequelae can impact crucial patient functioning, speech development, and quality of life. Early postoperative complications related to palatal closure including infection and wound complications can have an impact on long-term outcomes. Therefore, it is important to identify which patients are a greater risk of early postoperative outcomes to better inform cleft management.
While our results demonstrated that the overall proportion of complications remained relatively low in both cohorts, it remains intuitive that bilateral palatoplasty had a higher proportion of wound dehiscence. Wider clefts may predispose incisions to greater incisional tension leading to a theoretical higher possibility of dehiscence. Wider cleft palates are associated with increased complications and poorer outcomes following cleft palate repaired with one study demonstrating increased operative time and worsened postoperative sequela in higher Veau classifications. 21 However, early complications such as bleeding, dehiscence, airway compromise, infection, and return to operating room were not observed. Chouairi et al. similarly examined a national cohort of patients undergoing palatoplasty from 2012-2016 and found that despite an increased proportion of comorbidities in those who underwent bilateral palatoplasty, no differences in early postoperative complications were identified. 22 On multivariate analysis, our bilateral palatoplasty cohort demonstrated near statistical significance for increased odds of wound dehiscence. While this was not statistically significant, we believe our analyses may be limited by the overall low proportions observed in both cohorts.
Bilateral palatoplasty had a nearly two-fold increased odds of readmission, independent of age, operative time, and medical comorbidities. Previous literature has suggested that infants with comorbidities and increased Veau classification demonstrate improved perioperative outcomes if they were older at time of cleft palate repair. 23 To mitigate the increased risk of postoperative complications in bilateral repair, literature has suggested that repair before 6 months of age is contraindicated and delaying repair after 225 days of age may lead to improved perioperative outcomes.23,24 Additional factors related to an increased occurrence of hospital readmission for bilateral repairs could be due longer operative time, greater risk of swelling, higher possibility of injury to surrounding structures, and a longer overall duration under anesthesia
The odds of readmission were increased by nearly 2-fold in bilateral palatoplasty and 13-fold in those with an ASA class of 4. The higher proportion of comorbidities and ASA class of 3 or above in the bilateral cohort ultimately suggests that a greater proportion of these individuals may have been syndromic, ultimately affecting perioperative outcomes. Previous research has demonstrated that systemic disease and syndromic diagnosis is the greatest single predictor of short and long term complications following palatal repair.25–27 One study demonstrated a 37-fold increased incidence of postoperative complications including bronchospasm, accidental extubation, reintubation, obstruction, hypoxia, unplanned intensive care unit admission in patients with structural or functional airway anomalies. 25 Thus, postoperative respiratory complications remain the greatest risk to syndromic individuals. 26 To mitigate the risk of readmission and postoperative complications in bilateral cleft palate repair, syndromic patients, those with systemic disease, and those with increased comorbidities may be candidates for an increased length of stay and close follow up following palatoplasty.
During the last decade, the shift towards outpatient surgery has increased due to increasing healthcare costs and advances in postoperative care. Complication rates in primary outpatient surgery are similar to that of inpatient surgery yet, in the United States, greater than 70% of palatoplasty repairs are still admitted to the hospital for at least 1 night. 28 Inpatient hospital stay after cleft palate repair has been reported to range from 1 to 14 days, indicating highly heterogenous treatment concepts. Our results demonstrated a median LOS of 1 day for both cohorts with an interquartile range of 1-2 days in the unilateral and bilateral cohorts. Though, LOS was not found to be associated with an increased odds of complications on multivariate analysis, previous analyses have suggested that an increased length of stay is independently associated with an increased odds of postoperative complications. 29 Previous literature has identified a subset of patients in which same day discharge may be contraindicated, including syndromic diagnosis, systemic disease, chronic lung disease, longer operative time and anesthetic duration, and longer time to postoperative oral intake.29–31 Our data demonstrate an increased odds of readmission for those undergoing bilateral palatoplasty and those with an ASA class of 4. These factors should be considered when deciding if patients are candidates for same day discharge. Additionally, surgeons may consider implementing an ERAS protocol to improve perioperative outcomes and reduce LOS in suitable candidates, which has been shown to shorten LOS without an increased complication rate.32–34
While early postoperative complications remain relatively low in our cohort, late postoperative complications including the development of a palatal fistula and velopharyngeal insufficiency (VPI) remain key outcomes of interest to cleft teams. Greater occurrences of palatal fistula have been demonstrated in those with bilateral cleft palate.14,15 Additionally, bilateral cleft repairs experience higher rate of VPI, oronasal fistulas, with syndromic children at a greater risk of oronasal fistulas, VPI, and adverse speech outcomes.27,35–38 While late postoperative outcomes could not be captured, they remain important outcomes that can impact crucial patient functioning, speech development, and quality of life.
We recognize that this study is not without limitations and therefore should be interpreted within the context of its design. In utilizing the ACS-NSQIP-P database, we are bound to specific variables which limits the breadth of this research. As cleft care has been demonstrated to differ significantly from one center to another in regard to the chronology of therapeutic steps, surgical technique of cleft repair, and perioperative management, these factors may represent significant confounders that cannot be accounted for. Additionally, late and long-term outcomes of interest including palatal fistula, VPI, maxillary hypoplasia, and the need for additional orthognathic surgery could not be captured.
While the overall proportion of postoperative complications remains low in unilateral and bilateral cleft palatoplasty, the observed results that bilateral repair is associated with increased proportions of wound dehiscence and an increased odds of readmission should be used to guide patient-provider counseling when discussing the inherent risks associated with palatoplasty.
Footnotes
Author Contributions
All authors above appropriately contributed to the development of this manuscript. The conceptualization of the goals/aims of the article were driven by Alvin Kwok, Jay Agarwal, Dana Johns, and Jessica Marquez. The formal acquisition of the data was carried out by Jessica Marquez and Jack Sudduth. Data analysis was conducted by Devin Eddington. Jessica Marquez, Ashraf Patel, Kaylee Scott, Jack Sudduth, Erin Kim, Dana Johns, Jay Agarwal, and Alvin Kwok were involved in drafting and revising the final version for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.