
Abstract
Objective
To perform a systematic review and meta-analysis to determine if day case cleft lip surgery has an impact on complications and 30-day readmission rate.
Design
A systematic review was conducted using PRISMA guidelines. Databases included; PubMed, Science Direct, Ovid and Cochrane. Search terms; “Day Case”, “Day Care”, “outpatient”, “Ambulatory” AND “Cleft”, “Cleft Lip”. Meta-analysis was performed using RevMan 5.
Setting
Eligible study types included; randomised controlled trials, observational studies (prospective and retrospective) and case series.
Patients/Participants
Paediatric patients undergoing primary cleft lip repair.
Interventions
Day case surgery versus inpatient admission post-operative.
Main Outcome Measure(s)
Primary outcome measure: Primary cleft lip repair performed as a day case in paediatric patients. Secondary outcome measures: 1. Complication rates and 30-day re-admission to hospital rate. 2. Patient suitability for day case surgery.
Results
Ten papers with 13 804 patients undergoing primary cleft lip repair were included, 28% were discharged on the day of surgery (Range 17%-81%). There was no significant difference in complication rate between the inpatient and day case cohorts. There was a significant reduction in 30-day readmission rates in the day case cohort.
Conclusions
This meta-analysis indicates there is no difference in complication rates for patients discharged on the day of surgery compared to those admitted overnight. Complications encountered were infrequent, non-life threatening and often occurred more than 24 h following discharge. There was an observed reduction in 30-day readmission rates for day-case patients. This is likely to represent a variation in baseline characteristics which deemed them suitable for day case surgery pre-operatively.
Keywords
Introduction
Cleft lip and/or palate is one of the commonest congenital abnormalities worldwide with a global incidence of 1.2 per 1000. Depending on the subtype of cleft, these children undergo numerous hospital visits and inpatient stays throughout their life with a significant burden on both the family and the health service. 1 Repair of the cleft lip is the earliest operation and is usually performed between 3 to 6 months of age. Historically, the infant would remain in hospital for up to 7-10 days postoperatively for observation. 2 Over recent decades there has been a trend towards discharging the child on the day of surgery with an increasing number of publications demonstrating it is safe to do so. This is due to multiple factors including improved surgical technique, safer anaesthetic agents, an increase in regional anaesthesia as well as parental desires for convalescence in a familiar environment. 3
The first retrospective review to compare the outcomes of day case cleft lip repair to inpatient cleft lip repair was published in 1999. 4 This concluded there was no significant difference in outcomes between the two groups and showed a quicker time to feeding in the ambulatory group. Since then the adaptation to day case surgery has been demonstrated across the world in both developing and developed countries. Despite this, some surgeons and anaesthetists remain cautious and there are varying rates of uptake across centres worldwide.
Advantages of day case surgery for both the child and the parents include; reduced anxiety and psychological burden, better sleep pattern at home, a lower risk of nosocomial infection and more recently a lower risk of Covid-19, with better overall parental satisfaction rates.3,5 There are additional benefits for the health service, with reduced costs and better bed utilisation. 6
Despite these advantages, the underlying concern of patient safety following general anaesthesia remains, particularly when operating in proximity to the airway of young and potentially vulnerable infants. With the added apprehension of ensuring optimisation of post-operative analgesia to maintain adequate oral intake. The decision making remains the responsibility of the operating surgeon and anaesthetist but the parents also have a key role as they advocate for their child.
This systematic review and meta-analysis aims to establish the evidence basis for day case primary cleft lip repair in terms of both patient safety and suitability to aid surgical decision making with an evidence basis. We hypothesise there will be no significant difference in either complication rate or 30-day readmission rate between the day case and inpatient cohort.
Methods
A systematic review was conducted using PRISMA (Preferred Reporting Items for Systematic reviews and Meta-analyses) guidelines. The preliminary database search included PubMed, Science Direct, Ovid and The Cochrane database. Search terms included; “Day Case”, “Day Care”, “Outpatient”, “Ambulatory” AND “Cleft”, “Cleft Lip”.
Eligible study types included; randomised controlled trials, observational studies (prospective and retrospective) and case series.
Authors screened titles and abstracts independently using the ‘Covidence’ application for systematic reviews. Duplicates were removed from the search process. Full titles were then reviewed and those meeting the inclusion criteria were included for data analysis. A further search of the references of each full text article included was performed to ensure all relevant papers were incorporated.
A meta-analysis on peri-operative management of cleft lip repair published in 2021 was found during the review process. This meta-analysis covered five variables; arm restraints, wound closure, peri-operative antibiotics, day case or inpatient surgery and feeding restrictions. Despite the inclusion of day case or inpatient surgery as one of their variables, only six studies (3448 patients) were included in their analysis. Several studies were found outside of the scope of this initial meta-analysis and therefore we proceeded with our systematic review and analysis. 7
Primary Outcome Measure
Primary cleft lip repair surgery performed as a day case in paediatric patients.
Secondary Outcome Measures
Complication rates and 30-day re-admission to hospital rate.
Patient suitability for day case surgery.
Inclusion Criteria
Studies including day case primary cleft lip repair in children with a comparison inpatient group. The definition of ‘Day Case surgery’ is in reference to the British Association of Day Surgery definition: The patient must be admitted and discharged on the same-day, with day surgery as the intended management. Studies contained a mixture of isolated cleft lip repairs and cleft repairs with adjunctive reconstructive procedures.
Exclusion Criteria
Studies which involved cleft palate repair alone without cleft lip repair or those involving secondary cleft lip revision were excluded. Primary repairs performed on adult patients were excluded, in addition to primary cleft lip repair performed under local anaesthetic, with this cohort tending to be adult patients.
Study designs excluded; conference abstracts, case reports, letters to editor and non-English language papers.
Bias
Individual studies were assessed for bias using the MINORS instrument described and validated by Slim and colleagues. The subjective overall quality of the studies included was good. One difficulty encountered by all studies is that they were retrospective and by extension had no blinding or control groups. Despite this, studies were well designed, all including consecutive patients and all included clear aims and outcome measures. There was also a low rate of excluded patients with clear and valid justification for those that were.
Confounding bias was an issue across all studies due to the nature of the topic and study design, with comorbid patients more likely to have been pre-selected to the inpatient cohort and healthy patients to the day case cohort. Furthermore, there was variability in the presence of and/or the quality of appropriate statistical analysis. Overall, all studies had MINORS scores between 13 and 17 with a mean of 15, a score >16 is regarded as high quality.
Statistical Analysis
Analysis was performed in RevMan 5. A combination of tabulated and written data was extracted from each paper. Patients were labelled as having had a complication or readmission event. For complications, 10 812 patients were included from 8 studies and for readmission 13 804 patients were included from 10 studies. When studies were thought to contain results that should be excluded, inter-study heterogeneity was assessed using Chi-squared and I-squared values. Heterogeneity for included studies was low throughout. Overall effects were measured with Z-scores with significance at P-values less than .05.
Results
Initially twelve articles were included in the systematic review however two articles had to be excluded due to limitations of the available data in the paper, thus, ten papers were included in the final meta-analysis. The study by Santos et al. was excluded from analysis as data was not provided for the complication and readmission rates separated by each cohort. 8 The study by Hopper at al. was also excluded from analysis as the coding system used by the hospital meant complications following discharge could not be associated with the prior admission for cleft lip repair. 9 This meant that complication data was not available for patients who underwent a cleft lip repair as a day case. Furthermore, this group used 48-h as their cut-off for readmission as opposed to the more commonly occurring 30-day cut-off in the remaining studies. Figure 1. Shows the PRISMA breakdown.
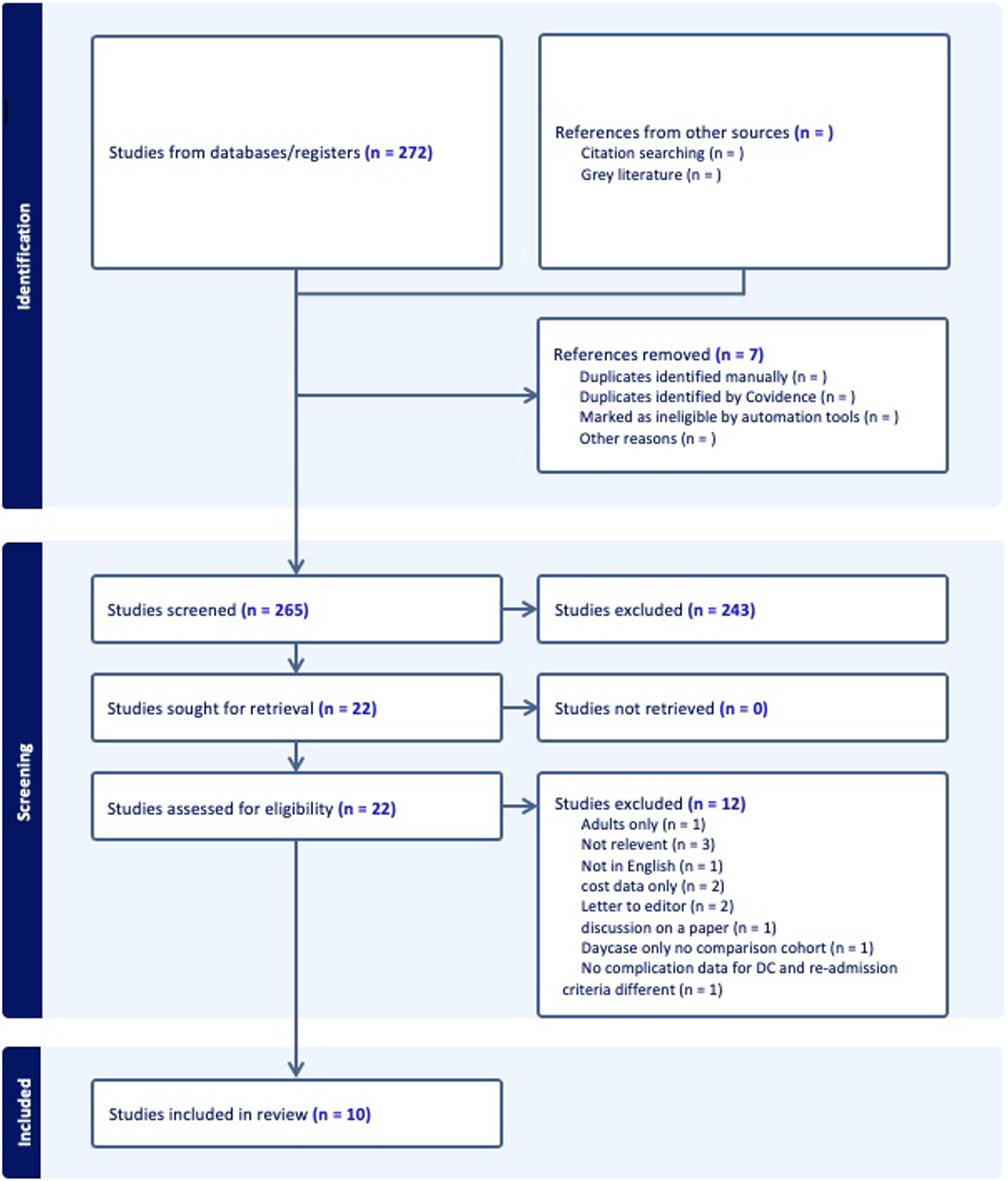
PRISMA flowchart for selection of articles included for review.
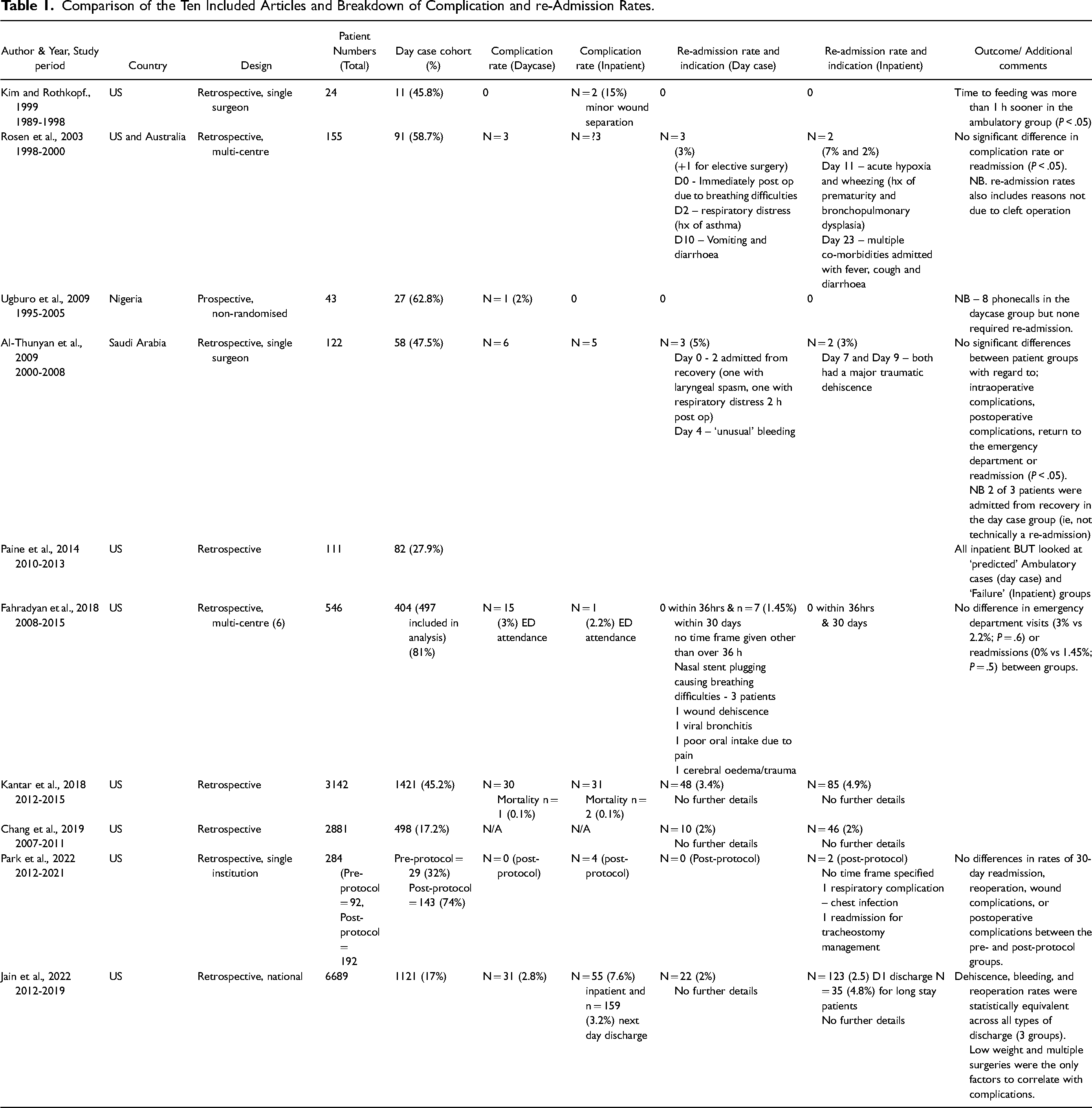
All studies included were retrospective in nature with a mixture of single centre and multi-centre studies from both developing and developed countries. The range of years spanned 1989 to 2021. Table 1. Shows a breakdown and comparison of the ten included studies.
Comparison of the Ten Included Articles and Breakdown of Complication and re-Admission Rates.
Patient ages ranged from 2.25 to 28.8 months across the studies, however two papers included patients over the age of 12 months which skewed the overall age range. With these two papers excluded the age range was 2.25 to 10.2 months.10,11
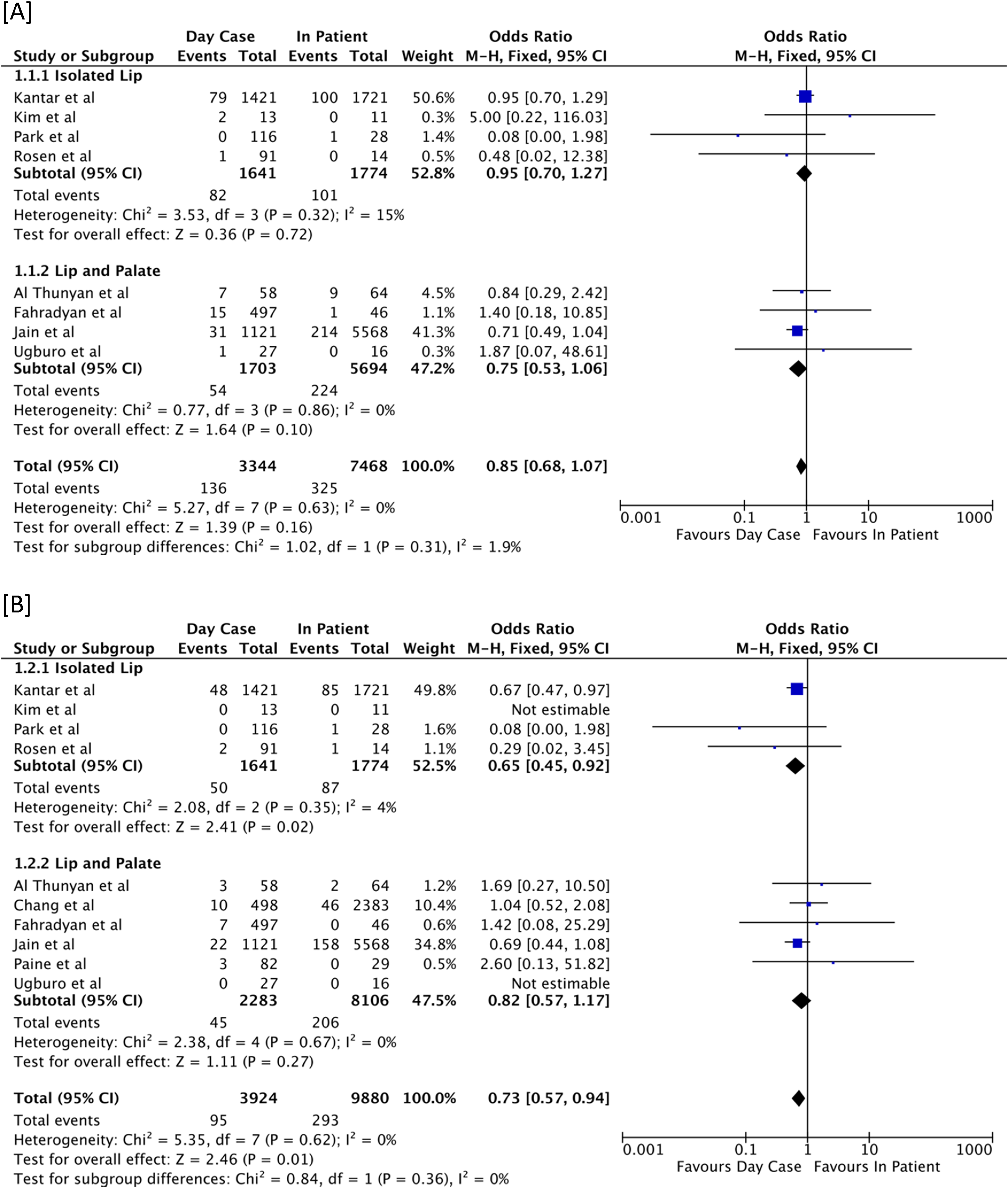
Most studies included multiple cleft subtypes (complete and incomplete cleft lip, both unilateral and bilateral with or without cleft palate). Jain et al. included patients of only one subtype; unilateral cleft lip and palate. Adjunctive procedures included; primary rhinoplasty, gingivoperiosteoplasty, tympanostomy tubes, soft palate repair and urological procedures. If studies are separated into those containing isolated lip repairs and those containing lip and palate repairs, subgroup analysis does not reveal any inter-group heterogeneity or any difference between groups for either complication or readmission rates. Please see Figure 2 for the box plots of the data analysis on complications and 30-day readmission rates between patients undergoing cleft lip surgery only and those undergoing both cleft lip and palate surgery.
A total of 13 804 patients undergoing primary cleft lip repair were included across the 10 studies with 3924 patients discharged on the day of surgery (28%). The same-day discharge rate varied from 17% to 81%. Only studies which compared a day case cohort to an inpatient cohort were included. Jain et al. had three comparative groups; same-day discharge, next day discharge and later discharge. For the purposes of the data analysis both the ‘next day discharge’ and ‘later discharge’ groups were considered as ‘inpatient’.
We specifically looked at two outcomes; [1] complication rate and [2] 30-day re-admission to hospital rate. Each individual paper reported no significant difference in these two measures between the day case and inpatient cohorts. Table 1 includes a comparison of complication and re-admission rates across the ten studies.
Surgical Complications
The paper by Chang et al. was excluded from the analysis of complication rates as they only reported readmission rates.(13) The paper by Paine et al. was also excluded as they retrospectively moved patients from the ambulatory to the inpatient group when a complication occurred. (10) This created two groups: ambulatory and ambulatory failure. An inherent bias is therefore created towards ambulatory care as this group by definition had no complications.
A total of 10 812 patients are included from 8 studies, 3344 patients had surgery as a day case (31%). The overall complication rate in the day case group was 4.1% (n = 136) and 4.4% in the inpatient group (n = 325).
Inclusion of relevant excluded studies (Chang et al. and Paine et al.) creates significant (P = .0004) heterogeneity with an I2 of 72% demonstrating their removal from analysis is sensible. With the eight included studies, there is non-significant heterogeneity with an I2 of 0% demonstrating very low heterogeneity and good congruity between the results presented by the included studies.
The overall Odds Ratio is 0.85. There is a non-significant (P = .16) overall effect (Z = 1.39) indicating there is no difference in the complication rate for patients undergoing cleft lip surgery as a day case or as an inpatients. This data is illustrated in the box plot shown in Figure 2A.
30-Day Readmission
All included studies used 30-days as their cut-off and so are comparable. A total of 13 804 patients are included from 10 studies, 3924 patients had surgery as a day case (28%). The overall 30-day readmission rate in the day case cohort was 2.4% (n = 95) and 2.9% (n = 293) in the inpatient cohort. With the ten included studies, as with complication rates, there is a non-significant study heterogeneity with an I2 of 0%. The overall Odds Ratio is 0.73. There is a significant (P = .01) overall effect (Z = 2.46) suggesting that patients in the day case cohort are less likely to require readmission within 30 days. Figure 2B shows the box plot of the data analysis across all included studies in terms of 30-day readmission rate.
The temporal relationship and indications for re-admission were assessed across all included studies. Two studies (Kim et al. and Ugburo et al.) had no re-admissions within 30-days in either cohort. Three studies provided no details on the indication and timing of re-admission in either cohort (Kanatar et al., Chang et al. and Jain et al.) and the study by Paine et al. did not indicate which cohort their indications for re-admission related to. The four remaining studies (Rosen et al., Al-thunyon et al., Fahradyan et al. and Park et al.) provided a breakdown of indications, with only two of these studies including the specific post-operative day of re-admission. Due to the low numbers in these four studies no meaningful statistical analysis could be performed. For reference, the indications have been listed in Table 1.
Discussion
Initial evidence emerged in the 1990s to demonstrate day case cleft lip repair is safe in a select group of patients, with comparable outcomes and complications to those children managed as an inpatient. 4 Despite multiple publications to support this over the proceeding decades there remains a wide variation in the proportion of children undergoing primary cleft lip repair as a day case across centres. In this systematic review, day case rates varied from as low as 17% 12 to 81%. 8
Another issue raised in the literature which contributes to this wide variation is the lack of standardisation of what authors classify as ‘day case’ or ‘ambulatory’ surgery. Within the term ambulatory some authors include patients discharged within 24 h of surgery. This cohort is clearly not equivalent to a cohort of patients discharged on the day of surgery without an overnight stay in hospital. All of the included papers in this meta-analysis used the term ‘day case’ or ‘ambulatory’ to mean the patient was discharged on the same-day as surgery.
Regardless of the initial decision pre-operatively, if there is any concern intra-operatively or in the post-operative period the child will be admitted for observation. This standard was evident throughout the papers included in this systematic review. The safety of performing primary cleft lip repair as a day case procedure relies on the judgement of both the surgical and anaesthetic team. Inpatient stay affords time for observation for complications, the ability to give intravenous fluids if there is inadequate oral intake post-operatively, as well as the option of both IV analgesia and stronger analgesia than would be available at home.
Safety and Patient Suitability
Evidence to support the safety of day case surgery in children is prominent across the studies included in this systematic review as well as in the anaesthetic literature. The Italian society of paediatric surgeons and paediatric anaesthesiologists produced a consensus report following a meeting in 2015. General criteria which must be fulfilled to consider discharge of a child on the day of surgery include; ASA I-II, the presence of a responsible adult to transport the child and care for them, live within one hour of the hospital and have a telephone available. This report was further subdivided into specific surgical procedures. For cleft lip repair the consensus was there was sufficient evidence to support the feasibility of day case surgery but the ultimate decision would be based on surgeon choice. 3
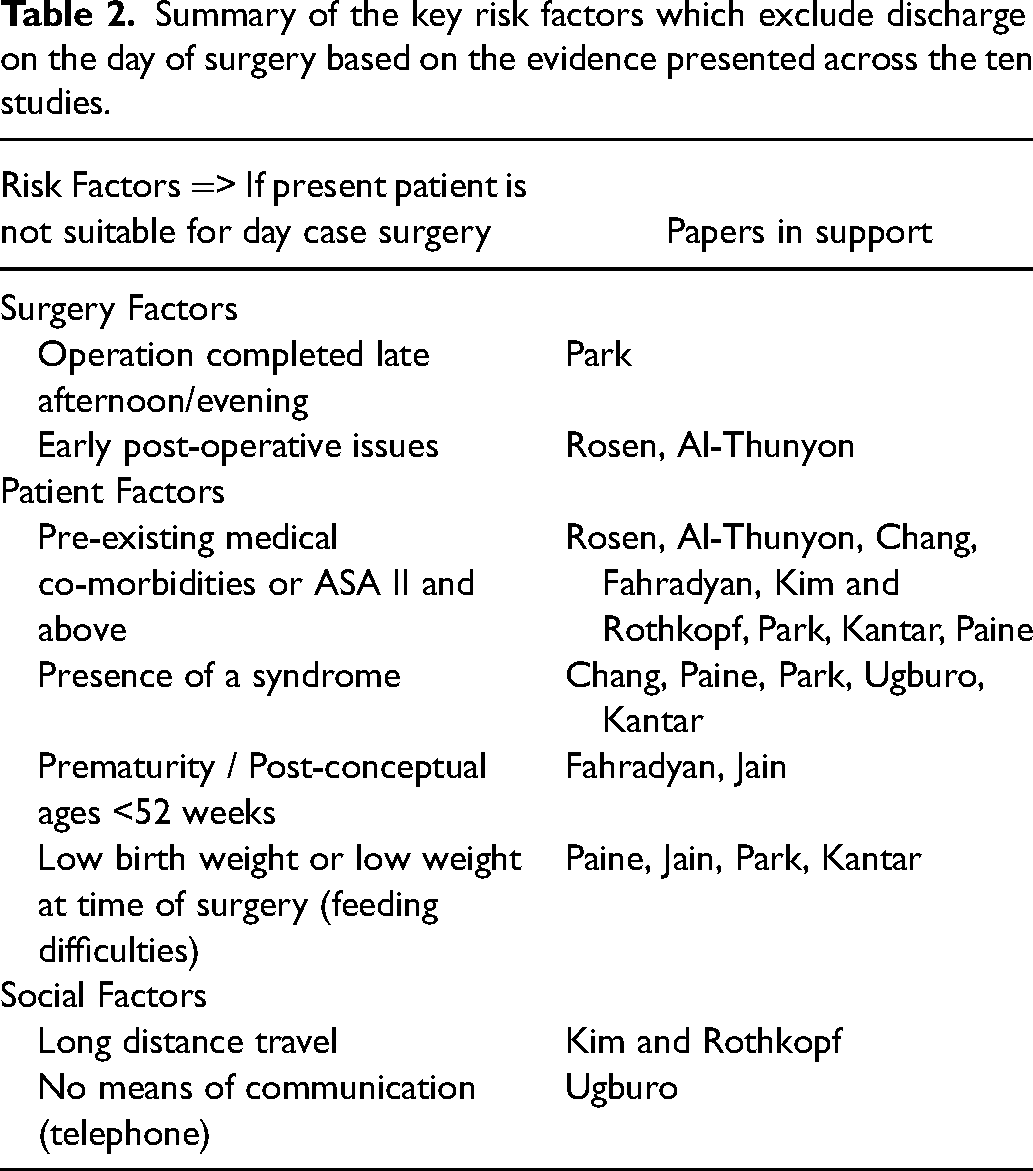
Several studies performed a regression analysis to assess the impact of multiple variables on successful day case surgery. A summary of the key risk factors described and the associated papers in support of this is shown in Table 2. These factors have been divided into: social factors (travel distance, communication methods), patient factors (prematurity, low birth weight, presence of a syndrome and comorbidities) and surgical factors (AM/PM operating list, early post-operative concerns). These recommendations are based on the statistical analysis in individual studies rather than from this meta-analysis.
Summary of the key risk factors which exclude discharge on the day of surgery based on the evidence presented across the ten studies.
It is apparent that day case surgery is not appropriate for all children and the success ultimately relies on appropriate patient selection in the pre-operative period to ensure the complication and re-admission rates remain low. This in itself leads to an inherent selection bias across the two cohorts which must be considered in the interpretation of results. Patients at higher risk of complications or readmission, such as those with multiple comorbidities or syndromic phenotypes, are more likely to have been electively assigned to an inpatient group. This would lead to the ambulatory group being an overall healthier cohort, making them more likely to have recovered successfully post operatively and less likely to require readmission which was the finding of this meta-analysis.
Several of the papers included in this systematic review performed a subgroup analysis to determine specific risk factors that when present pre-operatively warrant an inpatient stay for observation following primary cleft lip repair. Chang and colleagues used the technique of uplift modelling to determine which patients are suitable for discharge on the day of surgery. Analysis was performed to determine the impact of ASA score, age, co-morbidities and the type of procedure on the success of day case surgery. They concluded at least 40% of children would benefit from primary cleft lip repair as a day case procedure and there would be no impact on the remaining 60% whether they were discharged on the day or not. Patients who would benefit most were those with no history of respiratory or neurological comorbidities, non-syndromic patients and those undergoing fewer procedures or isolated cleft lip repair only. 13
Paine and colleagues reviewed 111 patients undergoing primary cleft lip repair who remained in hospital for one night post-operatively as per the senior authors’ practice. They used three indicators to determine which patients would ‘fail’ discharge on the day of surgery: ongoing need for IV narcotics, insufficient oral intake or overnight desaturations. The presence of these indicators predicted 26% of patients would fail discharge on the day of surgery. Eighteen patients did not eat on the first day of surgery, nine patients had a ‘respiratory event’ – all of whom had underlying cardiac or respiratory comorbidities and six required intravenous narcotics. Significant risk factors for ‘failure’ included; ASA 2 or more (P < .001), low birth weight (P = .002), cardiac concerns (P = .001) and presence of a syndrome (P = .005). 14 Al-Thunyan and colleagues are also in support of admitting children with pre-existing cardiac co-morbidities and advise admission for any patient showing signs of respiratory issues in the early post-operative period. 5
Rosen and colleagues concluded that day case cleft lip repair may be suitable for children with no comorbidities that have adequate supervision at home. They also stated the best indicator for appropriateness of discharge on the day of surgery may in fact be based on the immediate post-operative recovery period. 15
Fahradyan and colleagues found the following risk factors to be significant for admission to hospital; the presence of cardiac, respiratory, neurological, genitourinary and gastrointestinal comorbidities, history of prematurity and post-conceptual age less than 52 weeks. The two most significant were respiratory co-morbidities and post-conceptual age <52 weeks. Interestingly, the presence of a syndrome alone was not predictive of admission to hospital unless it was associated with an underlying comorbidity. 16
Jain and colleagues demonstrated an increased length of stay was associated with prematurity, nutritional deficiencies requiring support, gastrointestinal disease and a longer operation time. Two factors also correlated with complication rates; low weight at the time or surgery and multiple surgeries. 12
Park and colleagues demonstrated outcomes following a change to their surgical protocol for babies with both UCL and BCL. To be considered suitable for discharge on the day of surgery patients had to be non-syndromic and the operation had to take place in the morning or early afternoon. Patients with cardiac and airway abnormalities as well as prior feeding difficulties were excluded from the surgical protocol. Despite the implementation of this surgical protocol only 81% of the UCL group and 56% of the BCL group were discharged on the day of surgery, reflecting the importance of individual assessment of patients based on surgical factors and patient specific risk factors. 17
The study by Santos and colleagues was excluded from our data analysis as they only presented outcomes of their new ambulatory protocol with all patients being discharged on the day of surgery. Their exclusion criteria for day case surgery were; low weight, airway problems, the presence of a severe malformation or syndrome and no parent/guardian available. 8
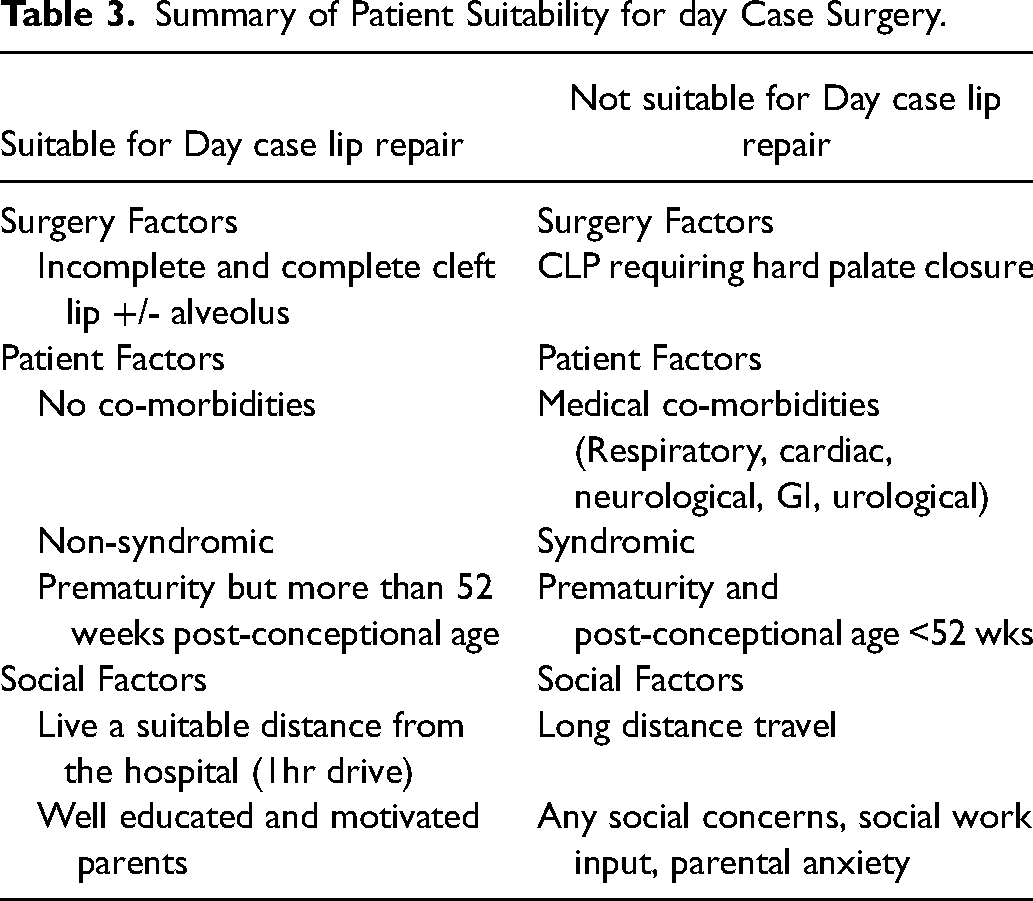
Summary of Patient Suitability for day Case Surgery.
Analysis of Patient Suitability
With improvements in surgical techniques and anaesthetic methods, there is good evidence that cleft lip surgery can be performed on a day-case basis. However, there will always be patients for whom an inpatient stay post-operatively remains the safest option. These may be patients with complex medical issues, those who will not have easy access to outpatient postoperative care or those who have care needs that may not be met if discharged the same day as their operation.
Ideally, using the 10 studies included in this review, we would assess the factors that might make a patient more or less likely to have a complication or readmission. This would allow us to provide guidance for future clinicians in how best to select patients for day-case surgery. Individual studies do contain the rates of various medical conditions, ASA grades and syndromic status of the patients in each of their ambulatory and inpatient cohorts. However, there is no consistency across the studies.
For example, Al Thunyan et al. and Fahradyan et al. include a total number of patients with comorbidities. Kantar et al., Paine et al., Chang et al. and Rosen et al. report the frequency of comorbidities involving varying systems of the body without providing a total. It is clear that one patient may in fact have multi-system disease and so for these studies, the proportion of patients in each cohort with a comorbidity cannot be calculated in the same way as Al Thunyan et al. and Fahradyan et al. In the study by Jaine et al., they identify the proportion of patients with comorbidities but do not reveal the proportion in each cohort. Importantly, these studies do not indicate if the patients who had a complication or required readmission had a comorbidity which may have contributed to the outcome. Paine et al. and Park et al. both label their cohorts using ASA score whilst Kantar et al. only indicate how many of their patients have an ASA score of 3 or above. Ugburo et al. do not provide details of the comorbid status of their patients and Santos et al. share only their ambulatory exclusion criteria.
Whilst many of the papers conduct their own logistic regression analysis to determine possible predictors of readmission or complication, the heterogeneity with which each of the studies presents their data unfortunately precludes any combined analysis. Access to their individual study data would allow for a meta-regression analysis, enabling clinicians to make a more informed decision about which patients are safe candidates for day-case cleft lip surgery.
Complications and Re-Admission
All individual studies included in this systematic review concluded there was no significant difference in complication rates between the two cohorts. Our meta-analysis of 10 studies confirms there was no significant difference across the two cohorts, with a rate of 4.1% in the day-case cohort and 4.4% in the inpatient cohort.
The majority of complications reported across the studies did not require re-admission. Common complications included wound dehiscence, minor bleeding or a respiratory tract infection which could all be managed in the outpatient setting. In the United Kingdom as part of the centralised cleft care facilities, families have direct contact with a cleft nurse specialist during the postoperative period. Where minor postoperative issues arise, patients’ guardians can easily communicate with an appropriate clinician. Access to this advice over the phone provides comfort for carers and mitigates the need for lengthy and often unnecessary re-attendance to surgical centres.
Patients who developed complications largely fell into two categories, children that developed issues in the early post-operative period and the remaining children who developed complications several days following discharge. If any early issues or concerns were identified the child was admitted overnight for observation regardless of the pre-planned discharge pathway. Notably, two of the included studies included this ‘complication’ as a re-admission, despite the decision being made in the recovery room prior to discharge.5,15 Children requiring re-admission to hospital following discharge presented a minimum of 24 h later. This suggests that remaining in hospital for observation on the night of surgery alone would not have prevented the complication developing nor the need for re-admission when it was required. Fahradyan et al., performed a multiple regression analysis and showed patients with a syndromic diagnosis (P = .013) and respiratory comorbidities (P = .022) were more likely to be readmitted.
Despite no individual study demonstrating a significant difference in readmission rate, pooled analysis with appropriate study weighting suggests that day-case surgery may improve readmission rates, with a significantly lower readmission rate in this cohort. Individual studies are limited by their small sample size and thus in a single study a large observed difference would be required to demonstrate a significant difference in readmission rates. Pooling data from multiple studies increases the sample size, which in turn reduces sampling error, increasing statistical power and overall reducing the possibility of a type II error. These significant findings may be attributed to the baseline characteristics of this cohort, who are more likely to be healthier at baseline with fewer co-morbidities and therefore deemed suitable for discharge on the day of surgery.
Limitations
The primary limitation of a systematic review and meta-analysis such as this is the very nature of the studies used. All 10 included studies are retrospective observational comparative studies. This type of study allows for a review of factors that influence patient outcome but the overall effect of the intervention in question is often difficult to elucidate. At baseline, due to the nature of this study there is confounding bias as pre-selected factors which may affect the overall outcome are also used to select the cohort patients are placed in, either inpatient or day case. The overall effect of this is that complications may be more likely to occur in the inpatient cohort due to higher baseline risk factors resulting in day case surgery appearing safer, with fewer complications. Additionally, if a patient in the inpatient cohort experiences a postoperative issue, this is likely to be recorded as a complication. Whilst if the same complication occurs at home following day case surgery, this event may require readmission.
Secondly, there is a large amount of inter-study heterogeneity which precludes data analysis of the baseline characteristics of each cohort across studies. Despite all studies using the same retrospective methodology, they vary greatly in size and demographic, with some studies including multiple hospitals across a nation. The study by Kim et al. had only 24 patients, whilst Jain et al. included nearly 7000 patients. Larger studies tend to provide more statistical power with narrower confidence intervals whilst smaller studies are less likely to appropriately represent the population and as a result are more exposed to type II errors. The relative weight of each study based on their size is however accounted for in our statistical analysis.
Given the scarcity of studies reporting the safety of day case cleft lip repair, with only 12 relevant studies and 10 included in our meta-analysis, the time period for included operations spanned over four decades from 1989 to 2021. Details regarding operative and anaesthetic specifics are sparse within individual studies and therefore improvements in peri-operative care in more recent years cannot be accounted for in the data analysis. This undoubtedly may increase the likelihood of successful, safe ambulation following cleft lip repair in the later cohorts.
Furthermore, eight of the included studies are based on data from the United States whilst there are just two studies relating to operations performed elsewhere in the world, Saudi Arabia and Africa. The healthcare system in the US is relatively unique with a mixture of privately funded care through insurance as well as publicly aided Medicare and Medicaid. This healthcare system model may alone impact the outcomes we are looking at, notably, the length of stay may also be influenced by the associated cost.
Although there is representation from both developed and developing countries the data is heavily skewed to the US. The impact of resource availability in less developed countries cannot be understated and is likely to directly affect the safety of performing cleft lip surgery as a day case. Patients in developed countries are able to be discharged in the knowledge that local healthcare services are readily available. This enables clinicians to safely lobby for early discharge. However, studies from developing parts of the world highlight the difficulties faced by a scarcity of healthcare facilities and resources. In particular, Ugboro et al. exclude patients whose family do not have access to a mobile phone - a consideration that likely wouldn’t be taken in a developed country as there is an assumption emergency healthcare would be locally available should the patient need it. Overall this makes clinicians in developing countries more cautious about performing these operations as day case procedures.
Conclusion
This meta-analysis supports the safety of day case primary cleft lip repair. There appears to be no increase in complication rate if patients are discharged home the same day as their operation. The complications encountered in the day case cohort were inconsequential and occurred more than 24 h following discharge thus an inpatient stay would not have prevented these complications.
Additionally, there is evidence to suggest that patients who undergo cleft lip repair and are discharged the same day are less likely to require readmission. Careful pre-operative assessment of patients’ suitability for day-case surgery is likely to have been a significant factor in contributing to the apparent reduction in readmission rates. It must be noted the recommendations for patient suitability for day case surgery listed in Table 3 are based on this systematic review but they are not statically supported by the meta-analysis due to the limitations previously discussed.
Day-case surgery has clear benefits; lower costs, improved bed efficiency and increased patient and carer satisfaction. Clinicians however should maintain a low threshold for readmission in the perioperative period to ensure that day-case surgery remains a safe and valid option for children undergoing primary cleft lip repair.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.