
Abstract
Objective
To establish normal values of palatal bone growth in fetuses at different gestational weeks in the early stages of the second trimester and to explore the clinical application value of the four-step ultrasound screening method for fetal cleft lip and palate.
Design
A prospective study of prenatal ultrasound screening.
Setting
Secondary maternal and child health institutions.
Patients
300 fetuses of 12 to 20 +6 weeks gestation without cleft lip and/or palate; 8538 fetuses at high risk of cleft lip and palate with malformations or karyotypic abnormalities.
Interventions
None.
Main Outcome Measures
palatomandibular diameter (PMD) and transverse palatal diameter was measured and establish their typical values.
Results
(1) There is a typical “superimposed line” sign in the median sagittal section of the typically developing fetal face from 12 to 20+6 weeks of gestation. (2) The PMD and hard palate transverse diameter of fetuses from 12 to 20+6 weeks of gestation increased linearly with time. (3) Among 8538 high-risk fetuses, 21 cases of cleft lip and palate were diagnosed by the four-step ultrasound screening method in the early stages of the second trimester.
Conclusions
The median sagittal section of the typically developing fetal face in the early stages of the second trimester presents a typical “superimposed line” sign, and the PMD and transverse palatal diameter increase with time. The four-step ultrasound screening method for fetal cleft lip and palate in the early stages of the second trimester has high clinical application value.
Introduction
Cleft lip and palate is one of the most common birth defects, and its incidence has significant racial differences, ranging from approximately 1.5‰ ∼ 2.0‰ in Asians by birth census.1,2 The prognosis of different types and degrees of cleft lip and palate varies greatly. For example, surgery for simple cleft lip without combined cleft palate has better results, 3 but when cleft lip is combined with cleft palate, eating, speaking and hearing will be affected, 4 the surgeries become more numerous and difficult, and postoperative complications occur more frequently. There may be lifelong effects on the physiology and psychology of the child as well as a greater economic burden on the family and society. In recent years, there have been few reports on the early diagnosis of cleft lip and palate in pregnancy, mostly in combination with reports of other structural malformations and chromosomal abnormalities.5–7 Early diagnosis of fetal cleft lip and palate can provide sufficient time for prenatal genetic testing and counseling as well as for final decision making by the pregnant woman and her family, greatly reducing the associated physical and emotional toll. 8 In addition, as gestation increases, other organs of the fetus develop completely, especially when the fetus is at a fairly high gestational week; the echogenicity of other bony and soft tissue structures of the fetal face is enhanced, causing a gradual increase in factors that interfere with visualization of the fetal hard palate by ultrasound and thus making ultrasound diagnosis of fetal cleft lip and palate, especially cleft palate, very difficult.9,10 Therefore, it is important to explore early and accurate diagnosis of fetal cleft lip and palate. This study was conducted to establish the reference ranges of typical values of fetal palate-maxillary diameter and hard palate transverse diameter and their variation with gestational weeks and to explore the prenatal diagnostic value of the four-step ultrasound screening method to diagnose for cleft lip and palate.
Materials and Methods
Patients and Data Acquisition
This trial is divided into two parts. In the first part, we will measure fetal PMD and transverse palatal diameter at different gestational weeks to obtain their typical values. First, 300 fetuses seen at our hospital between 12 and 20+6 weeks of gestation will be screened with ultrasound to obtain a median sagittal view of the fetal face. Fetuses from 12 to 20+6 weeks of gestation were divided into 9 groups by gestational week, and at least 30 fetuses were enrolled in each group. Gestational age was corrected by the last menstrual period combined with the gestational week estimated by the head-rump length at nuchal translucency (NT) scan. Inclusion criteria for pregnant women with typical values of measurement were as follows: (1) singleton pregnancy with a healthy newborn at postnatal follow-up; (2) patients who underwent multiple ultrasound evaluations between 12 and 20+6 weeks of gestation had their results included in the study only once. Exclusion criteria were the following: (1) blurred images and poor display of target structures due to maternal obesity, poor fetal position, etc.; and (2) ultrasound or postnatal confirmation of fetal differences. In the second part we will prospectively validate the diagnostic efficacy of the four-step ultrasound screening method for fetal cleft lip and/or palate in the early stage of the second trimester. High-risk fetuses included in the diagnosis were identified by consideration of the following factors: (1) fetal NT ≥ 3.0 mm; (2) presence of cardiac anomalies or other serious malformations; (3) family history of cleft lip and palate; (4) maternal nutritional deficiencies, endocrine disorder, viral infections during pregnancy or taking related medications (eg, hormones, anticonvulsants and sedatives); (5) history of maternal exposure to radiation and microwave radiation during pregnancy; (6) history of smoking and alcohol abuse. A total of 8538 fetuses at high risk of cleft lip and palate with malformations or karyotypic abnormalities were finally included. All pregnant women signed an informed consent form, which allowed the implementation of the clinical investigation study. This study was reviewed and approved by the Hospital Medical Ethics Committee (No. Anxi W&C Hospital 2020-1-5).
Ultrasound Data Collection
A GE GoldSeal Voluson E10 ultrasound instrument (GE Healthcare, Zipf, Austria) was used with a transabdominal probe C1-6-D at 1.0-6.0 MHz.
The standard section of the fetal face was obtained in the median sagittal plane according to the Practice guidelines for performance of the routine mid-trimester fetal ultrasound scan, 9 and the postnasal triangle oblique coronal plane and transverse section of the maxillary alveolar process were obtained according to the method reported by Alfred Abuhamad and Rabih Chaoui.6,10 The median sagittal plane was the standard NT measurement plane: the fetal facial contour lines were clearly shown, and the nasal bone surface skin line, nasal bone and nasal tip formed three short strong echogenic lines; the mandible was shown only as a round dotted strong echogenic signal; the fetal cranium clearly showed the thalamus, midbrain, brainstem, fourth ventricle and posterior cranial fossa pool (Figure 1A). The posterior nasal triangle oblique coronal section was defined as follows: a triangular structure composed of three strong echos, where the right and left side strong echogenic lines are the maxillary frontal eminence, the bottom side strong echogenic line is the alveolar process (primary palate), and the top strong echogenic point is 2 nasal bone cross-sections (Figure 1B). The transverse section of the maxillary alveolar process was defined as follows: the upper lip skin line was intact, with continuity of the upper alveolar process deep in the skin and hypoechoic baby teeth within it (Figure 1C). The collected median sagittal midpalatine – maxillary diameter 11 was measured by an experienced prenatal diagnostician (Figure 1A), and the transverse diameter of the hard palate 12 was measured in the oblique coronal plane of the posterior nasal triangle (Figure 1B). Each diameter was measured three times, and the average value was taken. Measurement criteria were as follows: (1) palatomandibular diameter: the line of the midpoint of the two ends of the hard palate (including the upper alveolar bone); (2) transverse diameter of the hard palate: the line of the outer edge of the upper alveolar spine at the bottom edge of the posterior nasal triangle.
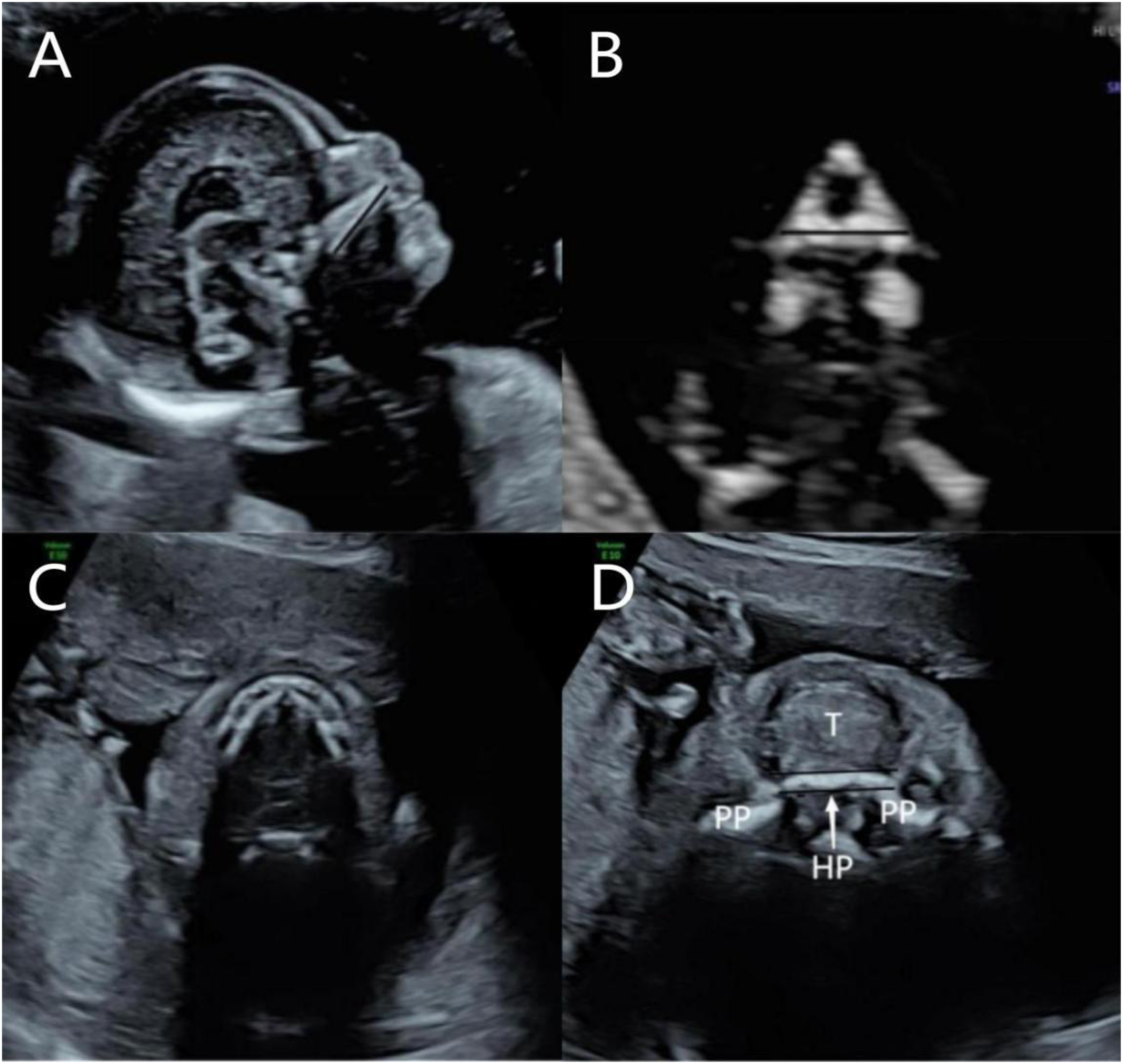
The cross-section of the four-step screening method for diagnosis of fetal cleft lip and palate in the early stage of the second trimester. (A) Median sagittal section (black straight line is the measurement line); (B) Oblique coronal section of the posterior nasal triangle (black straight line is the measurement line); (C) Transverse section of the alveolar process of the maxilla; (D) Cross-section of the horizontal plate of the palate. (HP: palatal horizontal plate; PP: maxilla; T: tongue).
A four-step approach to diagnosing fetal cleft lip and/or palate in the early stages of the second trimester was adopted as in the following description. In the first step, the presence of the “superimposed line” sign is observed on the median sagittal view of the fetal face. 13 If the “superimposed line” sign is absent, secondary cleft palate should be suspected. Step 2: consisted of measuring the palatomandibular diameter on the median sagittal view and comparing it with the growth curve table to see if the PMD was shortened or if there was a “maxillary gap” sign.14,15 In step 3, on the oblique coronal section of the posterior nasal triangle, the integrity of the bottom primary palate was observed,16,17 the transverse hard palate diameter was measured and compare with the growth curve table while paying attention to the shortening of the bottom primary palate. In step 4, first, the upper lip skin line was observed on the transverse section of the maxillary alveolar process for completeness and for any interruption of the continuity of the upper alveolar process at the deeper part of the skin, and then the last part of the secondary hard palate was exposed by angling toward the cephalic side of the fetus and cutting diagonally through the lower jaw or lower lip, that is, examining a cross-section of the horizontal plate of the palate (Figure 1D). At this point, the probe was tilted to the cephalic side again, and the transverse section of the hard palate in front of the horizontal plate up to the maxillary alveolar process could be explored to complete the scan of the entire secondary hard palate and observe whether it was continuous. All fetal palates were identified, images were preserved, information was recorded, and all fetal pregnancy outcomes were followed. Fetuses that were aborted or induced early in the second trimester were examined clinically or autopsied after delivery; fetuses for whom pregnancy was continued were subjected to a detailed facial ultrasound examination at the second trimester and were examined for cleft lip and palate (CLP) after delivery to obtain a clinical diagnosis or pathologic findings.
Statistical Methods
SPSS 26.0 was used for statistical processing. The Kolmogorov‒Smirnov method was used to test the normality of the data. Normally distributed measures were expressed as the mean ± standard deviation. One-way ANOVA and Welch's test were used for overall comparisons between different gestational weeks, and an independent samples t-test was used for comparisons between adjacent gestational weeks (corrected P < .006 was statistically significant). The correlation between normal fetal palate-maxillary diameter and hard palate transverse diameter and gestational week was analyzed by linear regression with cross-validation of the linear regression equation. Count data were expressed as frequencies (rates). Differences were considered statistically significant at P < .05.
Results
Analysis of Fetal PMD and Palatal Transverse Diameter Measurements at Different Gestational Weeks
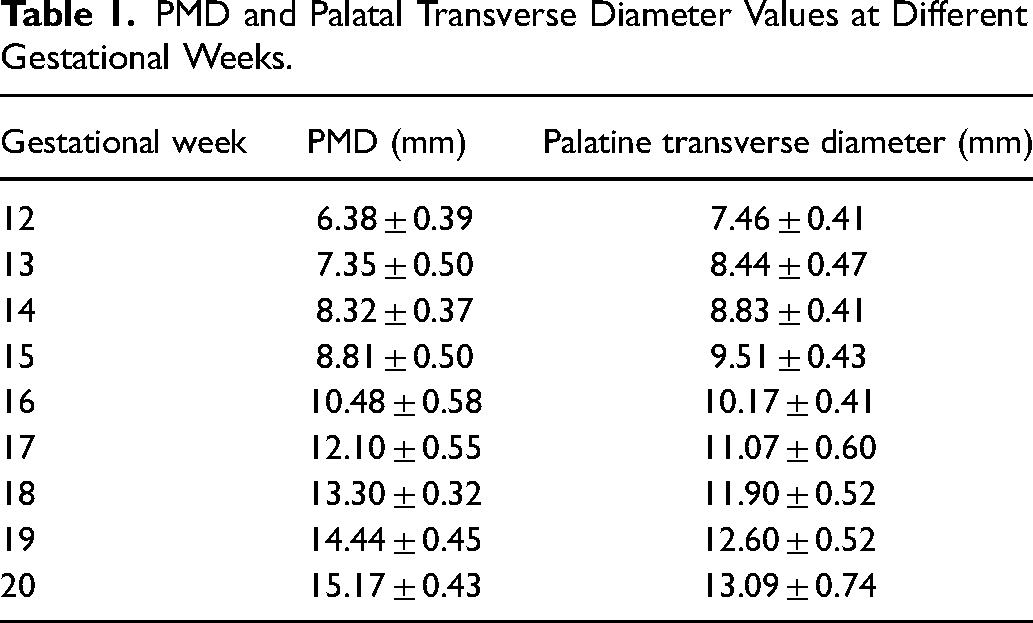
The typical “superimposed line” sign can be seen in the median sagittal view of the typical fetal face from 12 to 20+6 weeks of gestation, after which the “superimposed line” sign gradually becomes indistinct. The fetal PMD and transverse palatal diameter increased with increasing gestational weeks (F (PMD) = 1705.2; F (transverse palatal diameter) = 422.5, P < .001), and the differences were statistically significant in each gestational week compared with the previous gestational week (all P < .05) (see Table 1). The regression equations for fetal PMD and transverse palatal diameter from 12 to 20+6 weeks of gestation were Y (PMD) = 1.16X (weeks of gestation) – 7.86 (R2 = 0.967) and Y (transverse palatal diameter) = 0.71X (weeks of gestation) – 1.04 (R2 = 0.926), respectively.
PMD and Palatal Transverse Diameter Values at Different Gestational Weeks.
The Four-step Ultrasound Screening Method for Diagnosing Fetuses with Cleft Lip and Palate
Among the 8538 high-risk fetuses, 21 cases of cleft lip and palate were detected by the four-step screening process, including 9 cases of median cleft lip and palate, which showed loss of the “superimposed line” sign, shortening of the PMD and interruption of the primary palatal continuity at the base of the posterior nasal triangle oblique coronal section on the sonogram. In 5 cases of bilateral cleft lip and palate, the sonogram showed the disappearance of the “superimposed line” sign, the appearance of the “maxillary gap” sign and the interruption of the primary palatal continuity at the base of the postnasal triangle oblique coronal section or significant shortening of the transverse diameter of the palate. In 7 cases of unilateral cleft lip and palate, the sonogram showed the presence of the “superimposed line” sign, interruption of the primary palatal continuity at the base of the postnasal triangle oblique coronal section, or significant shortening of the transverse palatal diameter (Figure 2). One case of simple cleft palate was missed.
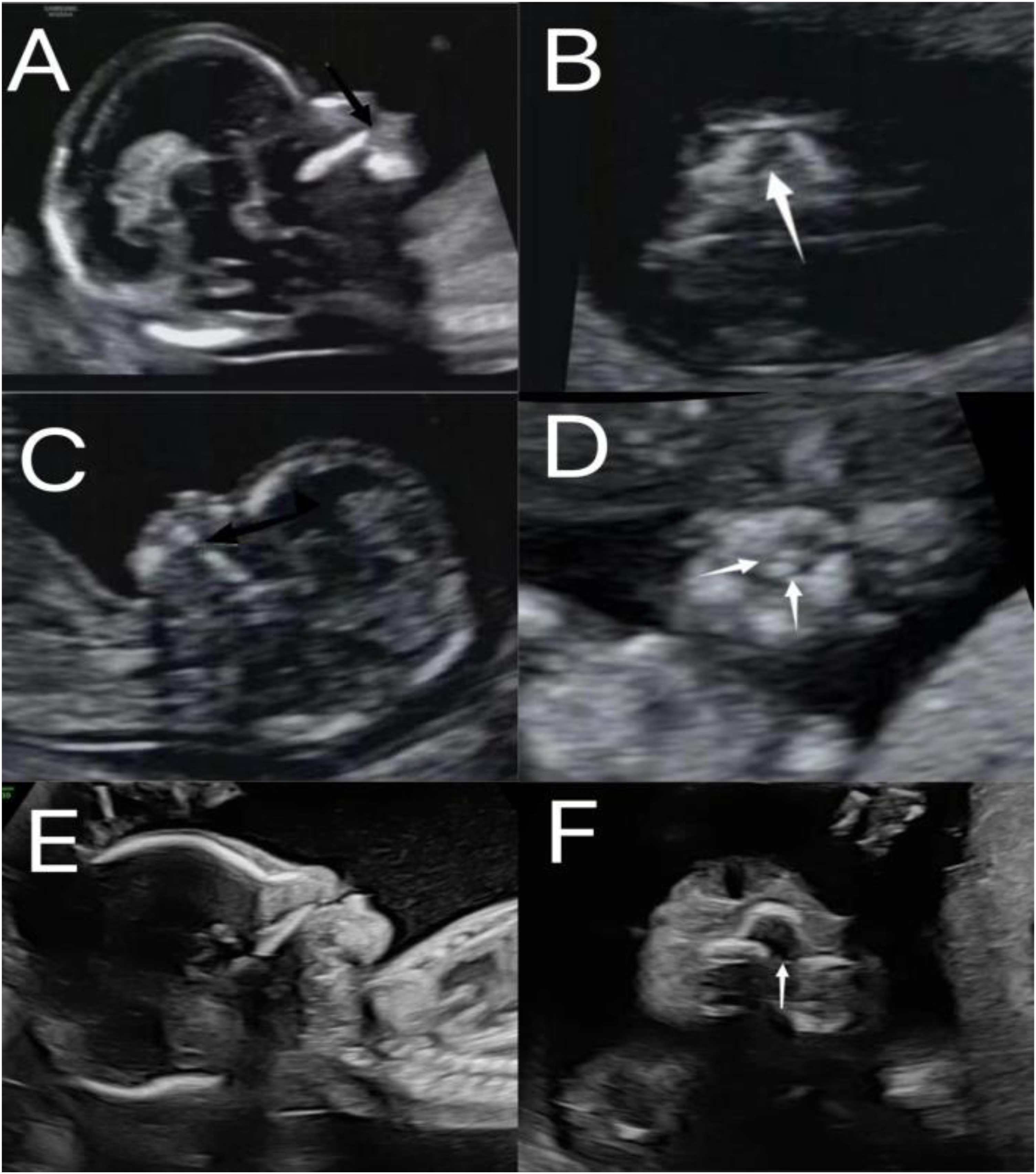
Sonogram of different types of cleft lip and palate. (A, B) Median cleft lip and palate; (C, D) Bilateral cleft lip and palate; (E, F) Unilateral cleft lip and palate; Black arrow: “maxillary gap” sign; white arrow: primary palatal continuity interruption at the base of the postnasal triangle oblique coronal section.
Follow-up Results
Of the 21 cases of cleft lip and palate, 9 fetuses with median cleft lip and palate, 5 fetuses with bilateral cleft lip and palate, and 5 fetuses with unilateral cleft lip and palate were electively induced and confirmed after delivery. In 2 cases of unilateral cleft lip and palate, chromosomal examination did not show any significant diagnoses, the pregnancy was continued to full term, and the diagnosis was confirmed after delivery. One case of simple cleft palate was missed among 8538 high-risk fetuses, and there were no false-positive cases.
The Effectiveness of the Four-step Ultrasound Screening Method
When the results of ultrasound diagnosis in the early second trimester were compared with the follow-up results, the sensitivity of diagnosing fetal cleft lip and palate using the four-step ultrasound screening method in the early second trimester was 95.5%; the corresponding specificity was 100%, the positive predictive value was 100%, and the negative predictive value was 100%.
Discussion
The results of this study showed that the typical “superimposed line” sign was seen in the midsagittal view of the normal fetal face in the early and early second trimester, and the “maxillary gap” sign was present in the midsagittal view of the cleft lip and palate fetus.13–15 The “superimposed line” sign in the median sagittal view of the typical fetal face represents the fusion of the secondary palate with the plow bone at the midline, and the plow bone at the distal end of the palate is shown as a superimposed line; however, in the secondary median cleft palate, the strong echogenic line formed by the secondary palate is absent, and only a single line of the plow bone at the midline is seen instead of the normal superimposed double line. 13 In our study, 9 fetuses with median cleft lip and palate and 5 fetuses with bilateral cleft lip and palate showed loss of the “superimposed line” sign. The “maxillary gap” sign in the median sagittal section of the cleft lip and palate fetus is a sign of cleft palate involving the secondary palate bone and the disruption of the continuity of the secondary palate bone; this is a valid sign for detecting cleft palate in early pregnancy. In our study, 9 fetuses with median cleft lip and palate, 3 fetuses with bilateral cleft lip and palate, and 2 fetuses with unilateral cleft lip and palate showed the “maxillary gap” sign. Chaoui et al. 15 reported that a maxillary gap greater than 1.5 mm or complete palatal agenesis in median sagittal section can be seen in 69% of fetuses with nonisolated cleft lip and palate, 35% of fetuses with isolated cleft lip and palate, and not in normal fetuses. The results of this study show that the PMD and transverse palatal diameter increase with increasing gestational weeks (12∼20+6 weeks) in typical fetuses, and the median sagittal section shows the “superimposed line” sign. This study provides a reference standard for typical values of fetal PMD and transverse palatal diameter, which can provide a more reliable basis for ultrasound diagnosis of fetal cleft lip and palate; the possibility of secondary cleft palate should be considered once the fetal PMD becomes significantly shorter. The PMD was significantly shorter in all nine fetuses with median cleft lip and palate in our study. The primary palate at the base of the posterior nasal triangle was observed in oblique coronal section, and the presence of primary or complete cleft palate was considered when the primary palate was deficient with interrupted continuity or significantly shortened transverse palatal diameter. All 21 fetuses with cleft lip and palate in this study showed discontinuity or shortening of the primary palate at the base of the posterior nasal triangle in oblique coronal view. In a prospective study involving 3D ultrasound, the diagnosis of cleft lip and palate by looking at the posterior nasal triangle oblique coronal section in early pregnancy had a sensitivity of 87.5% and a specificity of 99.9%. 17 In difficult cases, 3D ultrasound can help to show the facial and posterior nasal triangle oblique coronal views, which are important for early diagnosis of cleft lip and palate.17–19 The maxillary alveolar process was observed on the transverse section of the maxillary alveolar process, and when the maxillary alveolar process was defective with interrupted continuity and loss of normal curvature, cleft alveolar process or complete cleft palate was considered. In our group, all 21 fetuses with cleft lip and palate showed interrupted continuity and loss of normal curvature of the maxillary alveolar process.
Early diagnosis of fetal malformations has received increasing attention in recent years, but ultrasound diagnosis of cleft lip and palate in the early stages of the second trimester has rarely been reported.20–22 Usually, a single section of the fetal face is selected for scanning by ultrasound, and although using a single section has some value in diagnosing fetal cleft lip and palate, it has limitations in confirming cleft palate.21,22 In this study, the sensitivity and specificity of the four-step ultrasound screening method for diagnosing high-risk fetuses with cleft lip and palate in the early and early stages of the second trimester were high because the four-step screening method enabled assessment of palatal bone development from three views of the fetal face (ie, the median sagittal view, the postnasal triangular oblique coronal view, and the transverse view of the maxillary alveolar process) to diagnose for various types of cleft lip and palate (Figure 3).
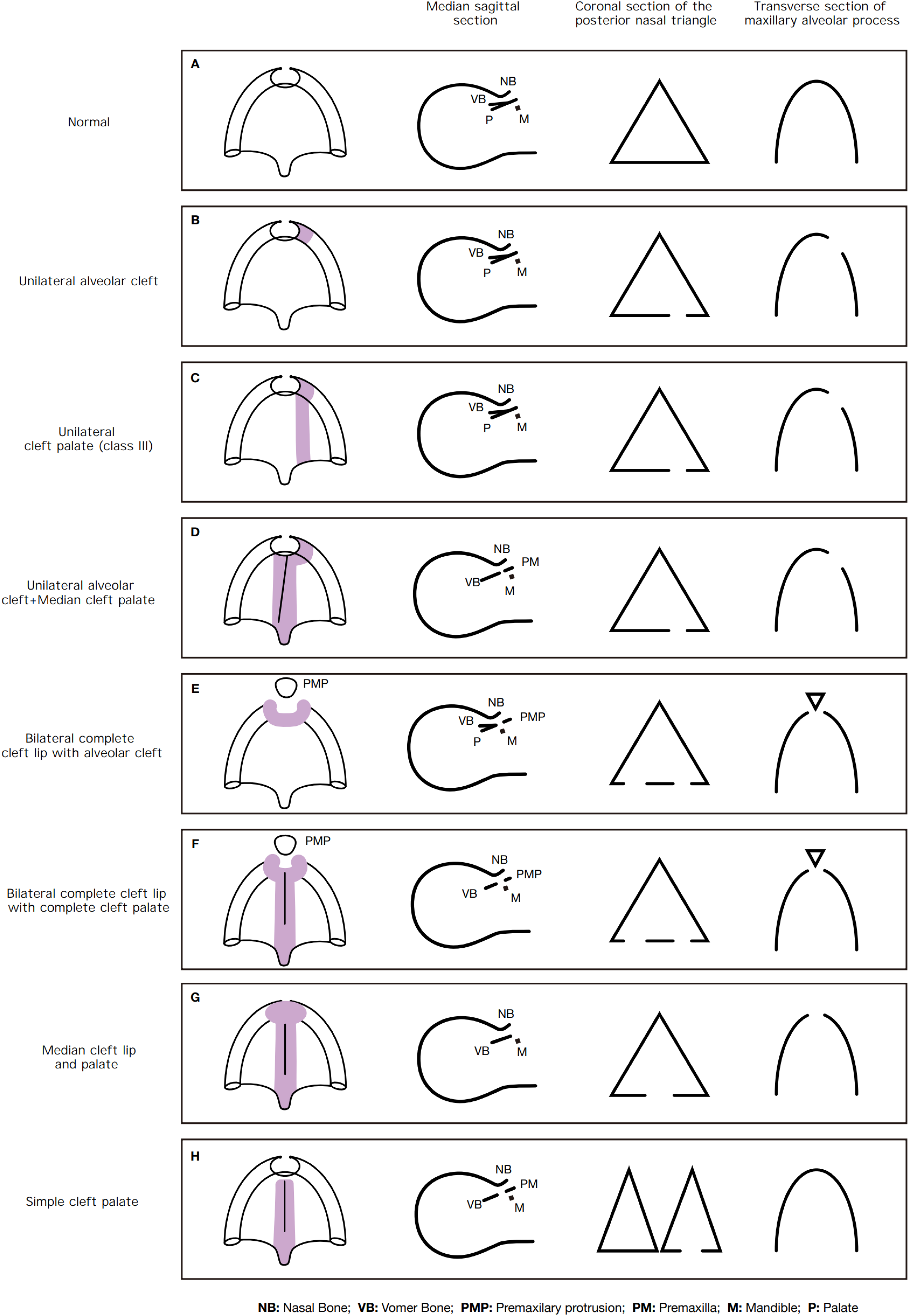
Cleft lip and palate pattern chart.
However, the current study also has some limitations. The present study was targeted to assess only the bony structures of the palate and therefore had poor sensitivity for the simple cleft palate of class I (soft palate cleft). Moreover, we did not screen a large number of cleft lip and palate cases, which makes it difficult to analyze the diagnostic efficacy with other imaging indicators and early pregnancy laboratory screening indicators. The current study was a single-center study, and our measured PMD and transverse palatal diameter were only for Chinese individuals and therefore not representative of other races or regions.
Conclusion
In this study, we established the reference ranges of typical values of fetal palate-maxillary diameter and hard palate transverse diameter from 12 to 20+6 weeks of gestation and their variation patterns with gestational weeks. In addition, we discussed the clinical significance of the four-step ultrasound screening method for fetal cleft lip and palate in the early stages of the second trimester to provide a data platform and targeted ultrasound examination method for improving the accuracy of prenatal diagnosis of early fetal cleft lip and palate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.