
Abstract
Objective
To review the evidence supporting the use of buccal fat pad (BFP) in primary and secondary cleft palate repair and its short- and long- term clinical outcomes.
Design
Systematic review conducted by 2 independent reviewers following PRISMA guidelines.
Setting: None Participants
Articles were identified from three databases (Pubmed/Medline, Embase and Web of Science). Search terms included “cleft palate”, “palatoplasty”, “palate repair”, “buccal fat pad”.
Interventions
Use of BFP in primary and secondary cleft palatoplasty.
Main Outcome Measures
Primary outcomes were immediate postoperative complications, postoperative fistula, and maxillary growth. Secondary outcomes were palatal length, speech, and donor site morbidity.
Results
Ninety-one reports were retrieved after excluding duplicates. Twenty-three studies were included (13 case series and 10 comparative studies). Overall level of evidence was low. Randomized and non-randomized studies had a high risk of bias. In primary palatoplasty, BFP was more frequently used filling lateral relaxing incisions(57.4%), or in the hard-soft palate junction and covering mucosal defects(30.1%). In these patients, post operative fistula incidence was 2.8%. Two studies found wider transverse maxillary dimensions after BFP use. No higher incidence of bleeding, infection, dehiscence, or flap necrosis was reported. In secondary palatoplasty, no recurrent fistulas were reported for patients undergoing BFP for fistula repair.
Conclusions
BFP appears to be associated with a favorable impact in fistula prevention and management, as well as in transverse maxillary growth. However, there is a high heterogeneity among studies, high risk of bias and overall low quality of evidence. More high-quality research with long-term follow-up is warranted.
Introduction
Palatoplasty is a necessary surgery for patients with a cleft palate in order to reconstruct the altered intraoral anatomy and achieve normal speech. However, it remains a challenge to achieve a balance between optimal velopharyngeal function and optimal facial growth. 1 Congenital tissue deficiency demands extensive mobilization of mucosal layers to close the cleft, creating dead space between oral and nasal layers and exposing bone due to the use of lateral relaxing incisions. Healing by secondary intention can reduce maxillary growth,2-4 and lead to mispositioning of the levator veli palatini and shortening of the soft palate. 5 Failure to achieve a tension-free closure may lead to dehiscence or fistula, with reported rates of such varying from 0%-78%.6-8
Many adjunctive palatoplasty techniques, such as use of the buccal fat pad (BFP), have been described. BFP is a specialized adipose tissue localized in the masticatory space.9,10 It was described by Heister in 1727 as the Glandula molaris (molar gland).9,11 Bichat, in 1802, described it as a “ball” of adipose tissue between the buccinator, the masseter, and the skin. For this reason, it is also known as the Boule de Bichat. 12 Hudson et al reported in 1995 on four cases of the use of BFP in the closure of secondary palatal or dentoalveolar cleft defects. 13 Zhao et al first utilized BFP in primary cleft palate repair to cover the raw surface of the lateral relaxing incisions and/or fill the dead space between oral and nasal layers in the hard-soft palate junction. 14
Since then, BFP use in cleft surgery has notably expanded. Its access, availability, rich blood supply, and lack of a secondary surgical site2,4,15 have popularized its use among many cleft surgeons, with increasing reports in the literature for both primary and secondary palatoplasties. Theoretical advantages of BFP in cleft surgery include diminished tension and decreased fistula formation, scar contracture, and associated maxillary constriction.2,4,15 At this time, evidence for the use of BFP has not been systematically reviewed. The objectives of this systematic review are to identify the role of the BFP in primary and secondary cleft palate repair and the short- and long-term clinical outcomes of its use.
Methods
This study is a systematic review of previously published studies and does not involve any primary data collection from human participants; therefore, institutional review board approval and subjects’ consent were not required. The authors conducted a systematic search with no publication date restrictions in three databases (Pubmed/Medline, Embase and Web of Science) in September 2022 according to the search query described in Supplemental File 1. Keywords “cleft palate”, “palatoplasty”, “palate repair”, “buccal fat pad” were included. Historic keywords such as “Bichat fat pad” were included to minimize reporting bias. The inclusion criteria were studies involving human subjects, use of BFP in primary or secondary cleft palate repair, sample with five or more subjects in each of the groups, and written in the English language. Publications included were randomized trials, cohort, case-control, comparative studies, and case series. Exclusion criteria were BFP used for diagnoses other than cleft palate, animal or cadaveric studies, and literature review publications.
After the completion of the database search, we excluded duplicate entries then reviewed titles and abstracts. After a scoping review of these, we identified the outcomes to be evaluated. We delimitated our primary outcomes as immediate postoperative complications, postoperative fistula, and maxillary growth. Secondary outcomes were time to mucosalization of the donor site, palatal length, speech and donor site morbidity. Pertinent articles were retrieved in full-text and reviewed to determine if they fulfilled the inclusion criteria. The following data were retrieved: Title, authors, date of publication, country, study design, number of patients, indication for palatoplasty, palatoplasty technique, function of BFP, clinical outcomes, and time of follow-up. Database search, title and abstract review, and full manuscript review were completed by two authors (C.R.N. and L.O.L.). Conflicts in data collection or article selection were resolved by a third author (R.E.K.). After data collection, the data were synthesized in charts for comparison purposes.
The level of evidence of each study was evaluated using the criteria of the Oxford Centre for Evidence-Based Medicine. 16 The risk of bias of each non-randomized study was analyzed independently by two authors (C.R.N. and L.O.L.) using MINORS assessment tool, which evaluates eight domains in non-comparative studies and twelve domains in comparative studies. 17 A complete list of the domains evaluated is provided in Supplemental File 2. For this study, we consider low risk of bias if they fulfill all the domains requirements (except the “Prospective collection of data” in the MINORS tool to include retrospective studies), high risk of bias if they failed in reported adequately 2 or more domains, and moderate risk of bias the rest of them. In the case of randomized trials, the Cochrane risk of bias v.2.0 (RoB2) tool was employed. 18 This tool includes evaluation of bias in the following domains: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome and selection of the reported result. For this study, we consider a global low risk of bias if all the domains are scored as “Low risk”, high risk of bias if one or more domains are scored as “High risk” or two or more domains are score as “Some concerns”, and moderate risk of bias in all other cases. Consensus was reached between the two reviewers (C.R.N. and L.O.L.). Disagreements were resolved by the third author (R.E.K.). In case of sufficient homogeneity between studies, a quantitative analysis using Cochrane Review Manager tool (RevMan 5.4) was be performed. If not, we proceeded with a descriptive qualitative analysis.
Results
The search retrieved 152 reports, and 61 duplicate records were removed. Titles and abstracts for 91 records were screened, and 67 were excluded. Full-text review was performed for 24 reports. We also retrieved three additional reports from citation searching. Two reports were excluded because they did not meet the inclusion criteria. It was identified that two reports19,20 discussed the same cohort, and data was collected from the more updated report. 19 Two other reports4,21 were a poster presentation and the published manuscript of the same study, and data was collected from the manuscript. 4 Ultimately, 25 reports from 23 studies were included in the review. A PRISMA flowchart is presented in Figure 1. 22
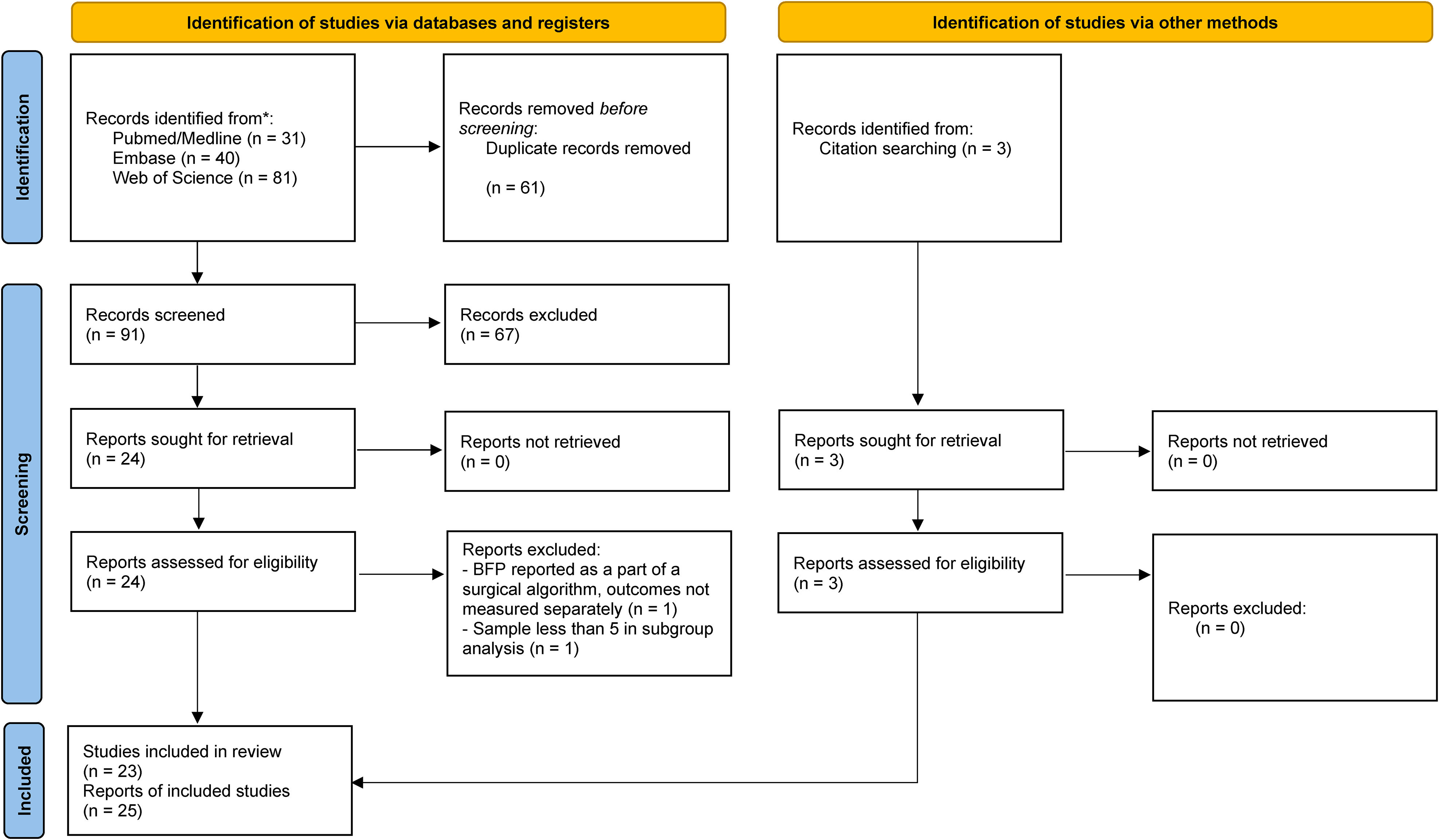
PRISMA flow diagram.
We reviewed 13 case series, 9 related to primary palatoplasty, 2 to secondary palatoplasty and 2 that addressed both. One study that addressed both primary and secondary palatoplasty had limited subjects in the secondary palatoplasty group, so this subgroup was not evaluated. One case series 23 described the authors’ usual surgical technique for palate repair, not focused specifically on BFP, but as it was a large sample of a major craniofacial center, and as the authors use BFP routinely in their primary palate repair, it was decided to include this report in our review. We also found 10 comparative studies: 8 related to primary palatoplasty, one related to secondary palatoplasty, and one related to a donor-site outcome.
There is a high level of heterogeneity between the studies, including study design, sample, inclusion criteria, the indication for and manner in which BFP is utilized, comparative material, palate repair surgical technique, outcomes, and length of follow-up (range 3 weeks-9 years). The overall level of evidence is low. Non-randomized studies have a high risk of bias according to MINORS, as well as the only RCT evaluated according to RoB2. Due to these limitations, we performed only a qualitative description of the studies included. The detailed description of the studies is shown in Tables 1 and 2. Risk of bias assessment is presented in Tables 3 and 4.
Outcomes, Follow-Outcomes, Follow-Up and Evidence Level in Case Series Studies.
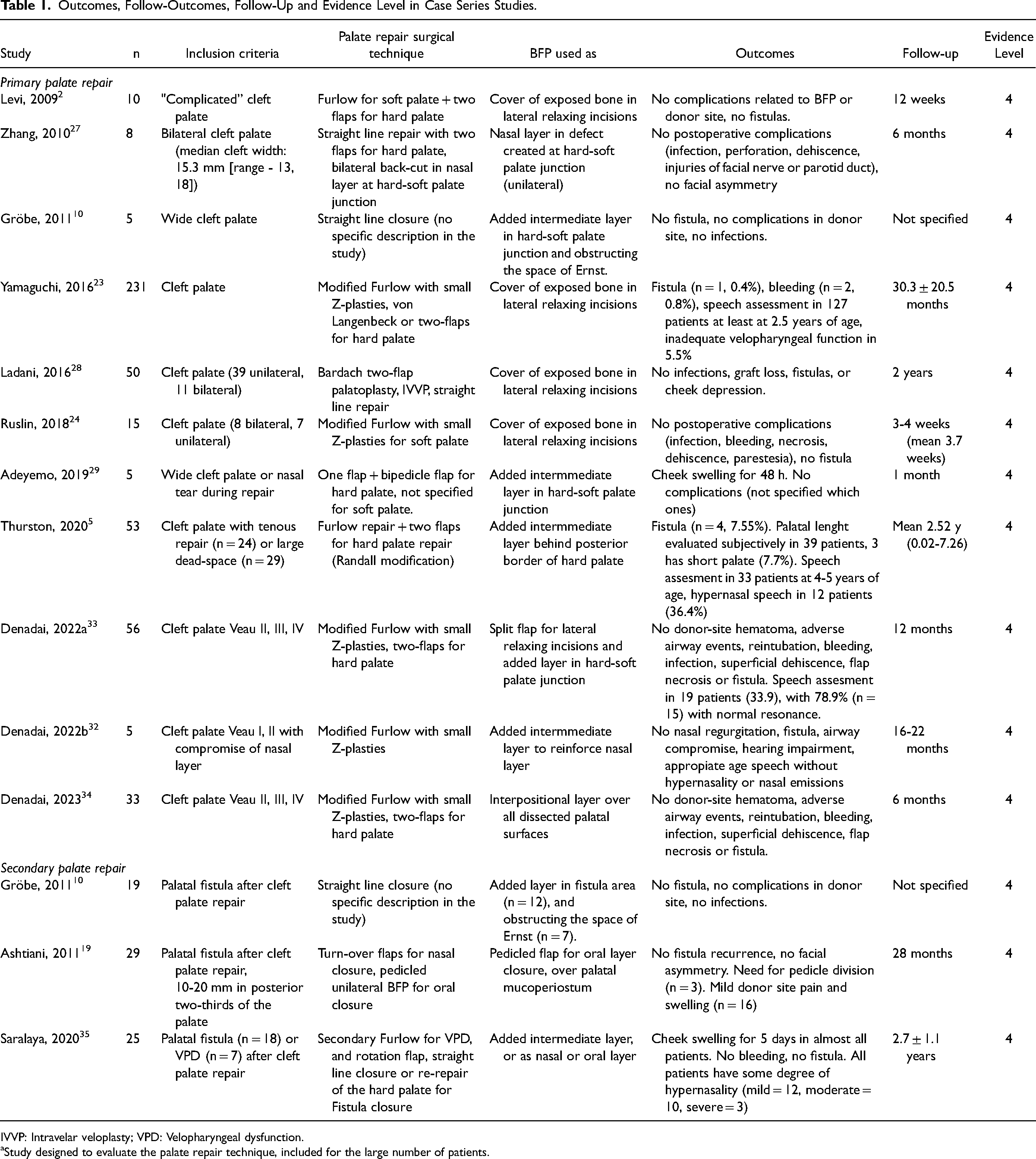
IVVP: Intravelar veloplasty; VPD: Velopharyngeal dysfunction.
Study designed to evaluate the palate repair technique, included for the large number of patients.
Outcomes, Follow-Up and Evidence Level in Comparative Studies.
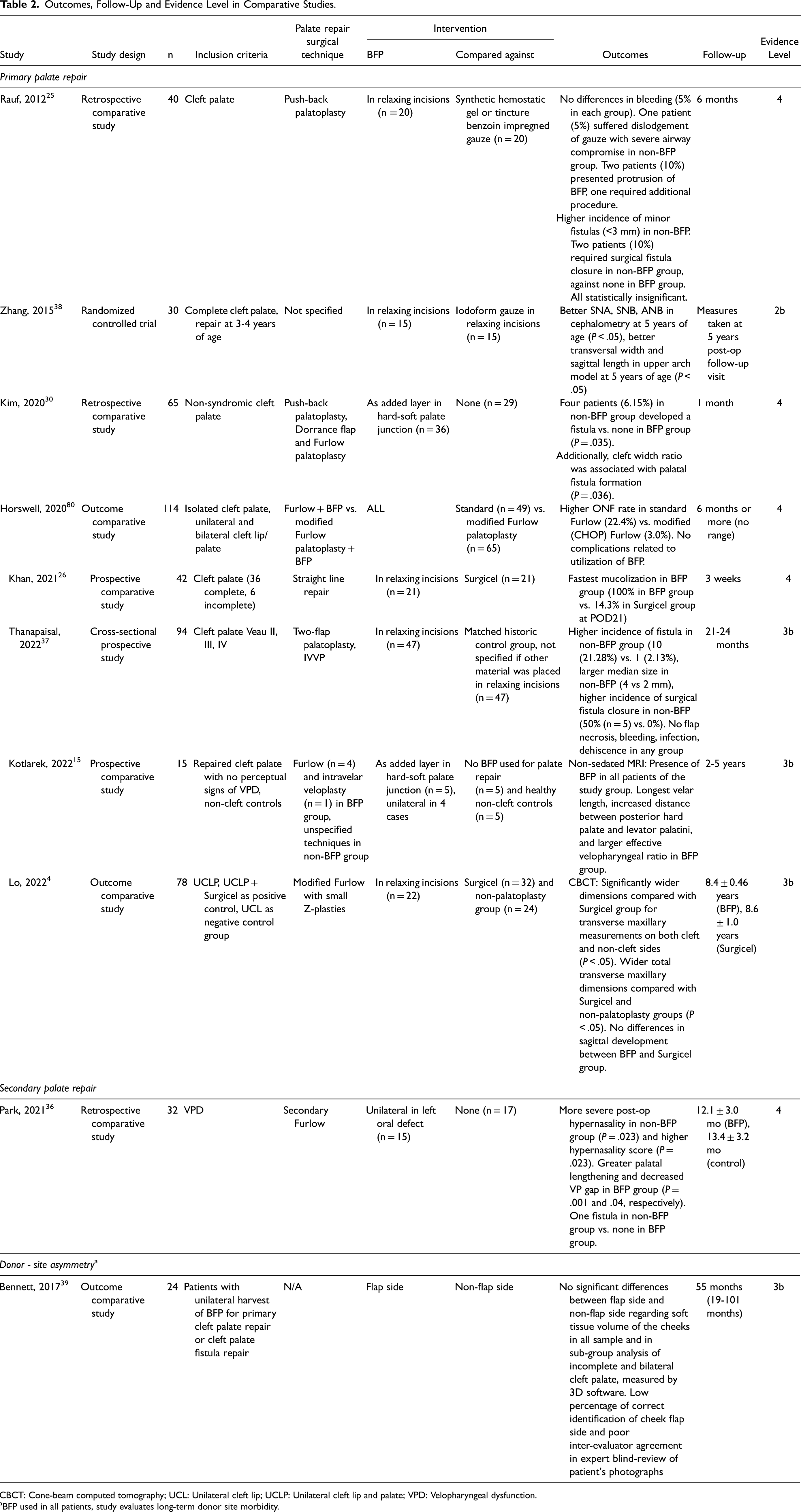
CBCT: Cone-beam computed tomography; UCL: Unilateral cleft lip; UCLP: Unilateral cleft lip and palate; VPD: Velopharyngeal dysfunction.
aBFP used in all patients, study evaluates long-term donor site morbidity.
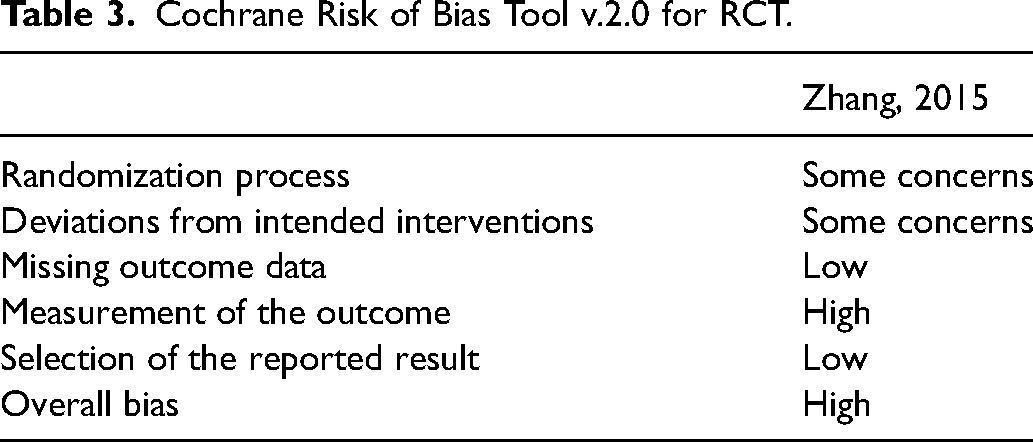
Cochrane Risk of Bias Tool v.2.0 for RCT.
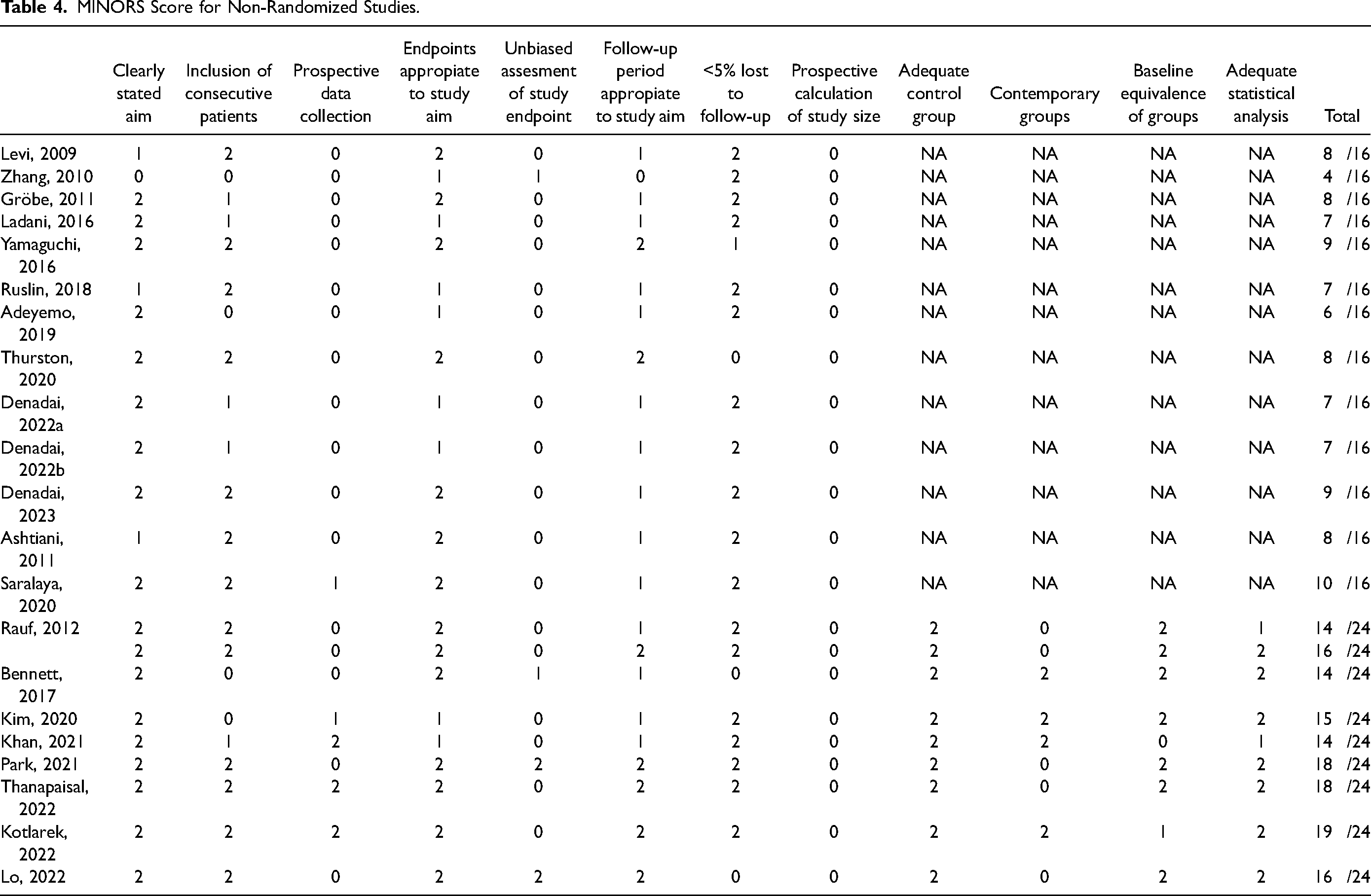
MINORS Score for Non-Randomized Studies.
Utility and Indications of Buccal Fat Pad
In primary palatoplasty, BFP is used to cover exposed bone in lateral relaxing incisions in 431 (57.4%) patients,2,23-28 as an intermediate layer at the hard-soft palate junction,5,10,29-31 or to reinforce nasal tears or compromised mucosa in 226 (30.1%) patients.5,27,32 It can also be split to serve both functions 33 or cover all the denuded palatal bone deep to the oral flaps 34 as described in 94 (12.5%) patients (Figure 2). In secondary cases, BFP is similarly used as an added intermediate layer,10,35 as a filler in the space of Ernst, 10 as a tunneled flap filling defects in oral or nasal layer,35,36 and as a pedicled flap over the oral mucoperiosteal flaps, filling defects in the oral layer. 19 In this last case, 3 of 29 patients required a second procedure to divide the pedicle.
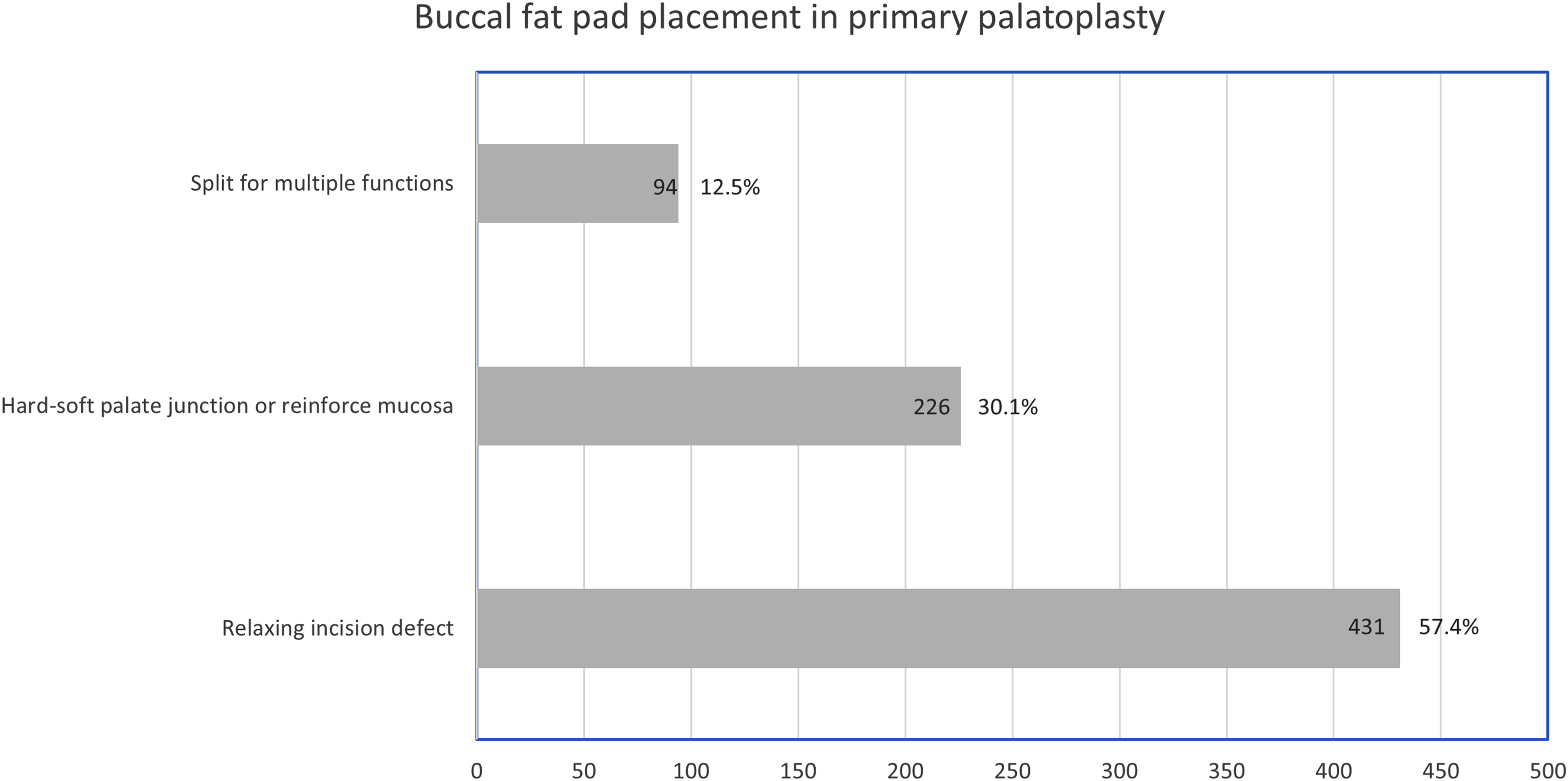
Buccal fat pad placement in primary palatoplasty.
The indications for BFP vary. Some studies propose use in all primary palate repairs that require a relaxing incision,23-26,28,30,34,37 while others restrict its use to “wide or complicated” clefts,2,5,10,29 bilateral clefts, 27 or cases with nasal mucosal tears or closures under tension.5,29,33 Different techniques for palate repair have been reported with BFP, including straight line,10,26,27 Furlow,2,5,21,23,30,32-35 push-back,25,30 Bardach,2,5,28,37 and von Langenbeck palatoplasty.23,29 In secondary cases, BFP is used for oronasal fistula repair10,19,35 and palatal lengthening for velopharyngeal dysfunction.35,36
Perioperative Complications
There are no reports of a higher incidence of bleeding, infection, airway obstruction, partial dehiscence or flap necrosis in patients who underwent BFP.2,10,23-25,27-29,33-35,37
Mucosalization
The time for BFP mucosalization was reported to be 2-4 weeks
Fistula
Fistula formation was the outcome most frequently reported. For primary repair, we found 10 case series and 3 comparative studies that evaluate this outcome. The incidence of postoperative fistula was 0%,2,10,24,27,28,32-34 0.4% 23 and 7.55% 5 in the case series, with samples between 5 and 231 patients. Comparative studies found a higher incidence in patients who do not undergo BFP,25,30,37 ranging from 0%-10% in BFP groups vs. 13.8%-21.28% in non-BFP groups. In summary, approximately 19 (2.8%) patients undergoing primary palatoplasty with BFP use developed a fistula. Of note, there was variable follow-up duration, and the definition of fistula was not strictly adhered to across studies. Patients who do not undergo BFP experienced a larger median fistula size 37 and higher rates of secondary fistula closure.25,37
Three cases series were included for secondary palate repair, as well as a comparative study. No recurrent fistulas are reported for patients undergoing BFP for oronasal fistula repair though follow-up duration is either not specified or between 2 to 3 years.10,19,35,36
Palatal Length
Some studies describe increased palatal length in long-term follow-up following palatoplasty where BFP was an added layer at the hard-soft palate junction. One case series 5 noted 92.3% of patients had a subjective adequate or “long” palate post-palatoplasty. Kotlarek et al 31 found a longer velar length, increased distance between posterior hard palate and levator veli palatini muscle, and a larger effective velopharyngeal ratio in patients who underwent primary palatoplasty with BFP.
Maxillary Dimensions
Lo et al 4 compared BFP (n = 22) vs. Surgicel (n = 32) in relaxing incisions during primary palatoplasty at 9-10 months of age with cone beam CT scans taken at 9-year follow-up visits. This study showed wider transverse dimensions in total maxillary width for patients with BFP use. There were no significant differences in sagittal development of the maxilla between the groups.
Zhang et al 38 conducted a randomized trial comparing BFP (n = 15) vs. iodoform gauze (n = 15) in relaxing incisions during primary palatoplasty at ages between 3-4 years old. At the 5-year follow-up visit, the BFP group demonstrated better cephalometry measurements, including SNA, SNB and ANB, as well as greater transverse width and sagittal length based on upper arch dental models.
Speech
Several case series reported speech-related outcomes.5,23,33-35 However, these studies utilized heterogeneous speech assessment methods and palatoplasty techniques. Notably, Park et al 36 evaluated hypernasality in patients with VPD undergoing secondary Furlow where BFP filled an oral defect created by incomplete advancement of the anteriorly-based oral mucosal flap. The BFP group developed less severe hypernasality and lower hypernasality scores.
Donor Site Morbidity
Mild donor-site pain was reported in 16 of 29 (55.2%) patients in one of the studies. 19 Patients may also experience cheek swelling for 2-5 days postoperatively.19,29,35 There were no reports of donor-site hematoma33,34 or facial nerve or parotid duct injuries.24,27
Long-term facial symmetry has also been studied following unilateral BFP harvest.19,27 Bennet et al
39
investigated facial dimensions measured by 3-dimensional photography in patients who underwent unilateral BFP for primary or secondary palatoplasty after a mean follow-up of
Discussion
This systematic review addresses the current role of the buccal fat pad in primary and secondary cleft palate surgery, as well as immediate and long-term clinical outcomes. Twenty-five articles were reviewed from an initial search of 152 records. Unfortunately, the level of evidence was generally low. Comparative studies had evidence grades between 3b-4 according to the Oxford Centre for Evidence-Based Medicine, and a RCT with a grade of 2b but with a high risk of bias according to Cochrane RoB2. Non-randomized studies, including case series and comparative studies, also have a high risk of bias according to MINORS assessment tool.
Immediate Postoperative Outcomes
One of the major concerns about BFP use is its potential for perioperative infection or other complications. There is no indication that patients who undergo BFP reconstruction have higher rates of complications such as bleeding, infection, airway obstruction, partial dehiscence, or flap necrosis. Additionally, mucosalization of the BFP raw surface such as during placement in palatoplasty relaxing incisions occurs relatively quickly over 2-4 weeks and is marginally faster in comparison to Surgicel placement in the relaxing incisions (full mucosalization by POD21 vs. POD28).
Fistula
One of the most frequently reported outcomes with BFP use is fistula formation. Reports of fistula rates following palate repair are variable, ranging from 0 to 78%8,40 with an overall incidence of postoperative fistula of 8.6% (95%CI [6.4-11-1%]), according to one meta-analysis. 40 Approximately thirty risk factors associated with this outcome have been studied such as timing of the surgery, type and width of the cleft, surgery techniques and surgeon's experience.8,40,41 Salimi et al found that the most frequently studied risk determinants did not present consistent patterns across different studies, other than a high heterogeneity and a general low quality of evidence. 8 In the case of association of cleft width and type, the variety of measurement methods makes comparison problematic.8,41,42 Some authors have hypothesized that tissue deficiency present, measured by the relation between the width of the cleft and the width of the palatal shelves, is a more important factor in fistula formation than cleft width or type, 43 but other reports have shown mixed results.7,30,37,44,45 Many of the reports analyzed in this systematic review claim that adding BFP in cases with wide clefts improves results and diminishes rates of fistula formation. Thanapaisal et al 37 and Kim et al 30 found a significant association between fistula formation and cleft width and ratio of cleft width, respectively. These studies also found a protective effect of the BFP, even though they utilized it in a different manner – covering lateral relaxing incisions in the first case and inset at the hard-soft palate junction in the latter. Others have also utilized BFP for wide clefts2,10,29 or in cases of mucosal tears or residual defects.2,5,27,29,32,36 In our review, all comparative studies that measured fistula rates reported lower rates in patients undergoing palotoplasty with BFP, including primary25,30,37 and secondary 36 palatoplasties. These studies found a larger median fistula size and higher rates of needing fistula closure in non-BFP groups.
Close proximity to the palate and almost universal availability could provide an attractive alternative to alloplastic materials in cases of tissue deficiency, especially in low-resources settings. However, one important drawback is the lack of an algorithm of when to use BFP. Adjectives as “wide” or “complicated” cleft palate have been mentioned to justify BFP use in cleft palate repair but without objective definitions. Furthermore, there is a high variability in palatoplasty techniques and in utilization of the BFP, thus precluding a more robust analysis. The evidence suggests that the use of buccal fat during primary palatoplasty may decrease fistula rates; however, longer-term studies that control for palatoplasty technique, cleft anatomy, and cleft dimensions are necessary to draw a more definitive conclusion.
BFP may have utility in oronasal fistula repairs. Grobe et al 10 reported on twelve cases with palatal fistulas, particularly in the hard-soft palate junction. The authors placed BFP as an intermediate layer between oral and nasal mucosa, occluding the dead space. They reported complete healing in all cases. Saralaya et al 35 also reported a case series with 18 patients. In their study, BFP was place in a similar fashion to that described by Grobe, while also replacing oral mucosal layer after nasal closure with turnover flaps. They also reported complete healing in all cases.
Asthiani et al 19 reported on 29 patients in whom BFP was used as a pedicled flap over the palate rather than tunneled underneath oral mucoperiosteum as described by other authors. Re-epithelializaton was observed in all patients, and only three required surgical division of the pedicle after four weeks. One patient experienced a residual fistula.
Fistula repair is a challenging procedure due to previous scarring and paucity of tissue.46,47 Many local flaps have been utilized for the closure of palatal fistulae, including tongue flaps,48-52 buccinator flaps,53-55 and facial artery based-myomucosal flaps.56-59 BFP has been previously used for closure of other oro-maxillary defects.60,61 For fistula repair, BFP has been recommended for closure of fistulae localized to the posterior two-thirds of the palate and in defects up to 20 mm in diameter. 19 The experience presented in these studies is valuable, with high rates of success. Although they have small sample sizes, BFP appears to be a successful technique for fistula repair.
Maxillary Growth
Maxillary growth disturbance is a common sequela of cleft lip and palate repair.3,62,63 Sagittal dimensions of the upper jaw are the most affected, with orthognathic surgery in up to 38.1% of patients with bilateral clefts and 30.2% of those with unilateral clefts. 1 Transverse dimensions are also affected, which may lead to posterior crossbite, dental crowding, and occlusal interference.21,64 Many factors have been implicated, including intrinsic growth deficiencies but also iatrogenic restriction due to surgical repair performed at an early age. 62 Scarring after palate repair is believed to be one of the most important extrinsic factors. Several strategies to decrease this negative impact has been described, including delayed hard palatal closure, 65 use of vomer flaps with lip repair,66,67 two-staged palatoplasty, 3 elimination of one or both lateral relaxing incisions in narrower clefts, 68 among others. BFP application in primary cleft palate repairs has been advocated to diminish the area of exposed bone in the lateral relaxing incisions and possible subsequent scarring.4,23-26,34,38 Lo et al 21 found that patients with BFP placed in lateral relaxing incisions had wider transverse maxillary dimensions. The authors hypothesized that adding vascularized fat over lateral denuded surfaces minimized scar formation and associated growth restriction from soft tissue contracture. However, sagittal maxillary dimensions were similar between patients who underwent BFP placement vs Surgicel placement, confounding this theory of improved maxillary growth with autologous BFP placement. Zhang et al 38 did find better transverse and sagittal maxillary dimensions in cephalometry and in upper dental arch models; however, their study has a high risk of bias regarding some concerns about the randomization process, deviations from intended interventions, and measurement of the outcomes, and the sample size was small (15 patients in each arm). Other important consideration is that, in this study, primary palatoplasty was performed between 3-4 years of age. Data about the impact of age at time of palatoplasty in maxillofacial growth is conflicting. 69 We believe this preclude a pooled analysis with other studies where palatoplasty was performed at a younger age. Overall, studies with follow up until facial skeletal maturity and less risk of bias are required to confirm these encouraging findings. More important than possible maxillary growth restriction is understanding if BFP use in management of cleft palate may reduce the burden of care such as a decrease in number of dental visits or a reduction or elimination of the period of maxillary palatal expansion.
Palatal Length and Speech
It has been proposed that BFP may help create a longer velum.10,15,27 Kotlarek et al 15 conducted a study to determine the surgical impact of the pedicled BFP flap on the levator veli palatini muscle and surrounding velopharyngeal anatomy. Through magnetic resonance imaging 2 to 5 years post-palatoplasty, the authors found that the BFP group had a longer median velar length than both the non-BFP group and non-cleft controls. The main limitation of this study is the small sample size, with only five patients in each group.
Some studies discussed speech outcomes. However, there was significant heterogeneity in speech assessment methodology as well as in palatoplasty technique among studies. For these reasons, we cannot include a robust analysis of speech outcomes related to BFP use in palatoplasty. Of note, Park et al 36 found less hypernasality in the BFP group, likely associated with an increased length of the soft palate. In this study, BFP was employed to cover a mucosal defect left by the transposition of the myomucosal posterior-based oral flap in secondary Furlow palatoplasty performed for VPD. Saralaya et al 35 also used BFP as an adjuvant in secondary Furlow palatoplasty for VPD correction. BFP was used in a similar fashion as that reported by Park. They do not report preoperative speech assessments; however, the BFP subgroup showed persistent hypernasality post-operatively (5 of 7 patients had moderate-severe hypernasality postoperatively). Secondary Furlow palatoplasties without the addition of BFP have been performed for VPD correction with improvement in standard speech outcome measures.70-73 Determination of the BFP's impact on speech outcomes during secondary palotoplasty will require more rigorous and standardized investigation as many surgical and non-surgical factors can influence speech and speech development.
Donor Site Morbidity
BFP resection has recently gained significant interest and popularity in facial esthetics. Despite short-term subjective improvement in facial contour, there is a lack of data about long-term outcomes,74,75 along with questions about how BFP resection influences facial ageing. Cheek hollowing, earlier deepening of the nasojugal fold, lack of the support of the medial cheek and middle cheek fat, are among the effects attributable to volume loss of the buccal fat pad. As such, there are concerns of short-term and long-term donor site deformities and facial asymmetries from BFP utilization in cleft repair. Interestingly, Bennett et al did not find significant differences in volume between both cheeks in 24 patients who have underwent unilateral BFP flaps for cleft repair after a mean follow-up of 55 months. 39 They similarly did not find any significant subjective differences in a blinded evaluation of clinical photographs by surgery residents. Although the results of this study are encouraging, it has a relatively short period of follow-up, considering that primary palatoplasty is usually performed around 1 year of age and most secondary repairs are done in childhood. Most surgeons who use BFP in a routine basis argue that the volume of BFP used for reconstructive purposes is not enough to impair facial contour and that up to two-thirds of the BFP remains in the cheek, protecting against visible deformation.2,39,46 Some studies also have shown that the BFP body in children has a different distribution of the fat when compared to adult BFP 76 and that the average BFP volume almost doubles between childhood and adulthood. 77 Understanding how all these factors influence long-term outcomes is a pending task and requires further investigation.
Limitations
Beyond limitations in individual studies, there are a few limitations of this specific systematic review protocol that are notable. First, only articles written or translated to the English language were included in this systematic review. While some systematic reviews in the cleft literature incorporate non-English references,78,79 it is not a universal practice, 40 and non-English references tend to be a minority of articles that meet inclusion criteria. 78 Second, a small sample size of five subjects was utilized for inclusion criteria. This lower cutoff was chosen to incorporate more articles discussing the utility of BFP tissue in primary and secondary cleft palatoplasty as the technique is relatively new. In this particular systematic review, the majority of articles were published in the last 10 years. If a more stringent exclusion criterion was selected such as 10 or more subjects, then five case studies would have been eliminated. This adjustment may decrease the heterogeneity and bias found in this systematic review, but it would also diminish the already limited published evidence on BFP use in cleft palatoplasty.
Conclusions
BFP has been used in a variety of manners in primary and secondary cleft palate repair. There is some encouraging evidence regarding its role in fistula prevention and management, as well as a favorable impact in reducing maxillary growth restriction. Use of BFP in palate repair appears to be associated with low rates of donor site deformity and postoperative complications. However, there is a high heterogeneity among studies and overall low quality of evidence. Thus, more high-quality research with long-term follow-up in the utilization of the buccal fat pad for primary and secondary palatoplasty is warranted.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231206238 - Supplemental material for Buccal Fat Pad in Primary and Secondary Cleft Palate Repair: A Systematic Review of the Literature
Supplemental material, sj-docx-1-cpc-10.1177_10556656231206238 for Buccal Fat Pad in Primary and Secondary Cleft Palate Repair: A Systematic Review of the Literature by Carolina Romero-Narvaez, Lawrence O. Lin and Richard E. Kirschner in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656231206238 - Supplemental material for Buccal Fat Pad in Primary and Secondary Cleft Palate Repair: A Systematic Review of the Literature
Supplemental material, sj-docx-2-cpc-10.1177_10556656231206238 for Buccal Fat Pad in Primary and Secondary Cleft Palate Repair: A Systematic Review of the Literature by Carolina Romero-Narvaez, Lawrence O. Lin and Richard E. Kirschner in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656231206238 - Supplemental material for Buccal Fat Pad in Primary and Secondary Cleft Palate Repair: A Systematic Review of the Literature
Supplemental material, sj-docx-3-cpc-10.1177_10556656231206238 for Buccal Fat Pad in Primary and Secondary Cleft Palate Repair: A Systematic Review of the Literature by Carolina Romero-Narvaez, Lawrence O. Lin and Richard E. Kirschner in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
We would like to thank Dr. Ibrahim Khansa for providing valuable insights during the review process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.