
Abstract
Introduction
The Abbe flap is a standard intervention to treat upper lip deformities in patients with bilateral cleft lip. This two-stage procedure requires a 2 to 3-week period in which the superior and inferior lips remain connected. This study evaluates the safety of Abbe flap division and inset prior to 14 days’ time.
Materials and Methods
A single institution, 8-year review of all patients with a bilateral cleft lip who underwent Abbe flap reconstruction was performed. Patients were classified into two groups: those whom division was performed 14 days or later and those with division earlier than 14 days.
Results
A total of 26 patients were identified. Patients who underwent Abbe flap division in less than 14 days (n = 10) demonstrated an average time to division of 9.7 days (range 7–13 days) with no evidence of flap loss, wound breakdown or infection. Patients who underwent Abbe flap division within 14 days or more (n = 16) demonstrated an average time to division of 15 days with four minor complications and no flap loss.
Conclusion
Dividing the Abbe flap after the first postoperative week appears to be safe and without additional risk to flap loss or wound breakdown. A shorter time to Abbe flap division may decrease the burden of care on patients and their caregivers.
Introduction
The Abbe flap was first described by Dr. Robert Abbe in 1898 as a method of addressing the secondary correction of a bilateral cleft lip deformity. 1 This surgical technique is well suited for reconstructing a natural-looking philtrum, Cupid's bow, and central tubercle, in addition to restoring balance to the entire aesthetic unit through donor site correction of the relative excess vermillion projection from the lower lip. 2
The Abbe flap is a two-stage procedure. The first stage involves rotation of a pedicled flap from the lower lip, based on the inferior labial artery, into a defect created in the central upper lip. The pedicled flap is then left in place for approximately 2 to 3 weeks, to allow for neovascularization. The second stage involves division of the vascular pedicle and inset of the flap.
In his original paper, Robert Abbe mentions flap division and inset on day 12. Contemporary literature reference flap division from 10 days to 3 weeks and note that the surgeon can compress the native labial artery pedicle and check capillary refill of the inset flap to ensure viability.2,3 Although most references note division at 2–3 weeks,4–6 division has been mentioned to be possible in as early as 5 days. 7
The postoperative management between Abbe flap creation and division can be difficult for the patient and their caregivers, representing a large burden of care. With a skin bridge connecting the upper and lower lips, oral intake must be through a straw. Patients have mentioned experiencing difficulty eating and breathing in the time between flap creation and division and highlight that help and support from relatives was imperative to assist through this period. 8 In addition to difficulties with eating and breathing, this pedicled flap has the disadvantage of creating a temporary but significant facial deformity due to the visible skin bridge with patients often considering this condition a severe limitation in social interaction and body image.
Those in low resource settings may have an additional burden of care as the requirement of long periods to travel to the treatment center and limited patient support can provide another dimension of difficulty. Shortening the time between flap creation and division may enhance the patient experience and decrease the burden of care. Thus, this study seeks to evaluate flap survival outcomes of Abbe flap division prior to 14 days against the standard of 14 days or more.
Method
Following approval from the Institutional Review Board (IRB), a single institution, retrospective chart review was performed of all patients with a cleft who underwent Abbe flap reconstruction over an 8-year period (2015–2022). Patients were excluded if they had Abbe flap reconstruction for an iatrogenic defect such as a skin cancer excision.
The following demographic characteristics were extracted from the medical records of the study group: age at time of surgery, sex, presence of comorbidities, prior alveolar bone grafting, orthognathic surgery, operative time for Abbe flap reconstruction, presence of a complication between Abbe flap creation and division (dehiscence, wound breakdown, flap loss, infection), date of division, length of time to division, operative time of division, concurrent cleft rhinoplasty at time of division, complications after division, flap loss, any revision surgery and length to follow-up.
After obtaining demographic characteristics, patients were classified into two groups – those whom division was performed 14 days or later and those who had division performed earlier than 14 days. All procedures were performed by one of two experienced, senior surgeons. No specific criteria were used for when a flap would be divided – it was surgeon's choice. All flaps were full thickness flaps including skin, orbicularis oris muscle and mucosa. Flap size was generally consistent with a 10 mm width and 8 mm base.
Results
A total of 26 patients who underwent Abbe flap for cleft lip reconstruction were identified. The average length to follow up was 584.8 days (range 18–1819). The majority of patients were male (n = 23, 88.5%). The mean age at surgery was 20.2 years (range 13–44 years). Syndromes were noted in three patients: one patient with Kabuki syndrome and two patients with Van Der Woude Syndrome. One patient, in the division performed 14 days or later group, was a former smoker, having quit one month prior to Abbe flap reconstruction, otherwise no other patient had a history of smoking or vascular disease, including inflammatory disease. Fifteen patients (57.7%) had prior alveolar bone grafting. The mean operative time for Abbe flap creation was 115.7 min. No patients were noted to have a complication between flap creation and flap division. Overall, the mean time to division was 12.96 days (range 7–16) with a mean operative time of 120.5 min. Abbe flap division with concurrent cleft rhinoplasty was performed in 16 (61.5%). Minor complications were noted in 6 (23%) patients. This included three patients with hypertrophic scars, two lower lip cysts and one widened scar with alopecia. Orthognathic surgery was performed in 11 (42.3%) patients with 9 (81.8%) of these patients having this performed prior to Abbe flap and two patients after Abbe flap reconstruction. Revision surgery was performed in 6 (23%) patients at an average of 432.5 days from Abbe flap division. Regarding revision surgery, 3 (50%) patients had fat grafting, 2 (33.3%) patients with scar excision and 1 (16.7%) patient with superior lip shortening for vermillion excess (Table 1).
Time to Division Group Comparison.
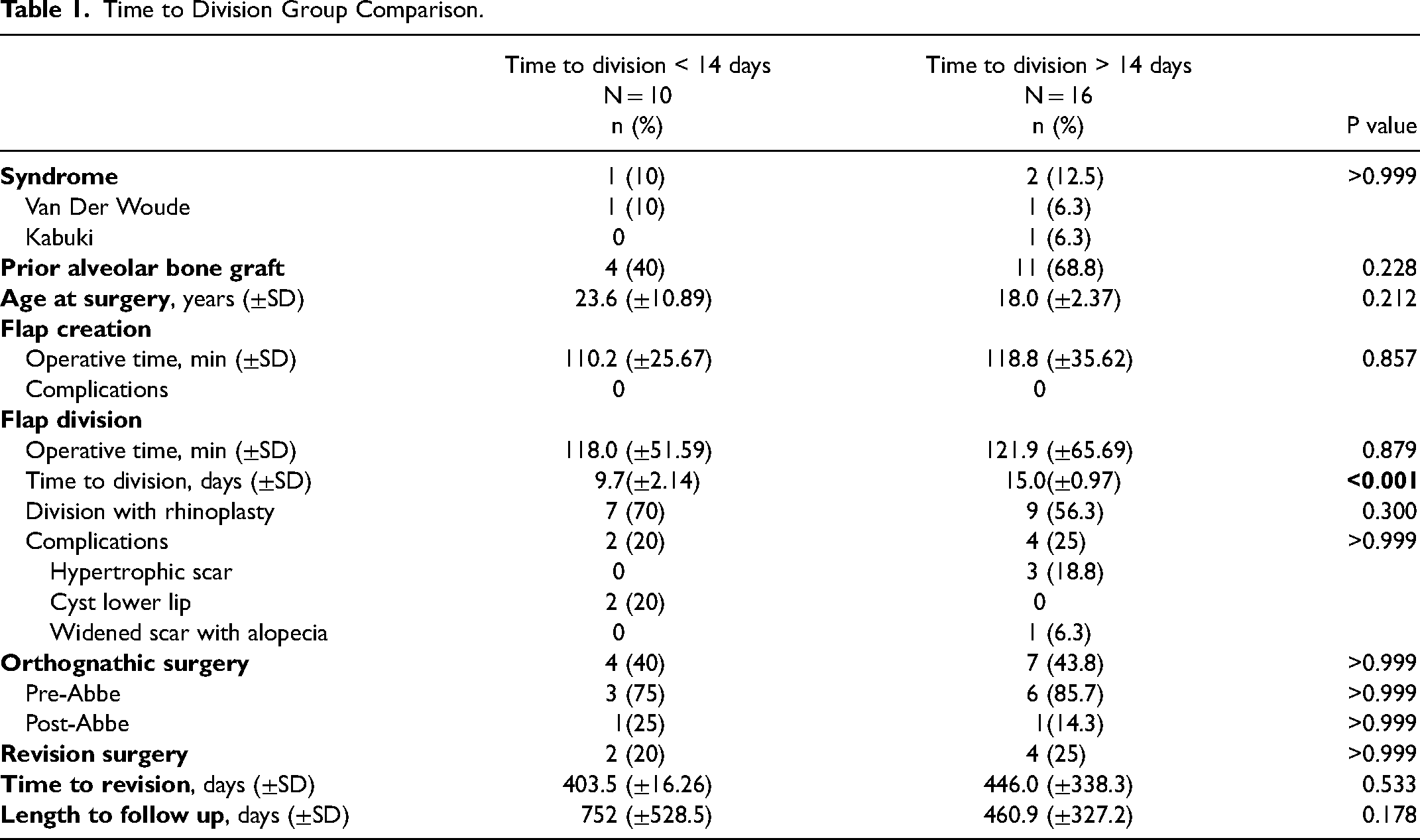
10 patients underwent Abbe flap division in less than 14 days (average time to division 9.7 days, range 7–13 days). The average age at operation was 23.6 years. No complications were noted between Abbe flap creation and division. At the time of flap division, 7 (70%) patients had a concurrent cleft rhinoplasty. There were no instances of flap loss, partial flap loss or localized skin necrosis (Figure 1). Two patients (20%) were noted to have a minor complication after division, which consisted of a lower lip cyst in each case (1 suture abscess, one mucosal cyst). Two patients had revision surgery at an average of 403 days from flap division. Of the revision surgeries, 1 patient had a shortening of the lip while the other had scar excision. The mean length of follow up was 752 days (Table 1).
16 patients underwent Abbe flap division within 14 days or greater (average time to division 15 days, range 14–17 days). The average age at operation was 18 years. No complications were noted between Abbe flap creation and division. Regarding the one patient who was a former smoker, no complication was noted. At the time of flap division, 9 (56.3%) patients had a concurrent cleft rhinoplasty. There were no instances of flap loss, partial flap loss or localized skin necrosis (Figure 2). Four patients (25%) experienced minor complication after division. Complications consisted of 3 hypertrophic scars and 1 patient with a widened scar and alopecia. Four patients had revision surgery at an average of 447 days from flap division. Of the revision surgeries, 3 consisted of fat grafting while 1 consisted of scar excision. The mean length of follow up was 480 days (Table 1).
Discussion
Current standard practice for Abbe flap reconstruction involves the division and inset of the flap two to three weeks after the primary procedure,4–6 a length of time with historical basis in Dr. Robert Abbe's initial description of 12 days. 1 While the majority of literature is in agreement with the time to division, safe flap division has been performed in as little as 5 days. 7
The 2–3 week time between Abbe flap creation and division is likely based on the paramedian forehead flap, considered the gold standard for nasal reconstruction, that was first used in ancient India. 9 Paramedian forehead flap is similarly conducted in two stages with most investigators dividing after 3 weeks, which has been deemed as adequate time for inset healing to the recipient bed. 10 Flap takedown prior to this time has been uncommon due the widely held assumptions of the fragility of the flap along with a potentially unreliable vascular supply consisting of the vertical axial vessels. 11 While these assumptions have driven current standards, Somoano et al. recently demonstrated that paramedian forehead flap trunk division is safe and effective when accelerated to as little as 1 week 11 which has significant implications for improving the quality of life of patients by substantially reducing the time patients face limitations prior to division. We therefore sought to explore the safety of Abbe flap division prior to two weeks with the goals of reducing the burden of care associated with two-staged reconstructions and improving the patient experience.
In our study, we found that there was no difference in flap survival between patients with bilateral cleft lip that underwent Abbe flap division between week one and two and after week two. Neither patient groups experienced complications between Abbe flap creation and division, while 20% of patients from the shorter time to division group (<14 days) and 25% of patients from the longer time to division group (>14 days) experienced minor complications following division that were unlikely related to the time of division and inset. Importantly, the shorter time to division group did not experience a significant increase in revision rate due to poor scarring or contour irregularities as compared to the longer time to division groups, suggesting that a robust blood supply is maintained.
The decision to pursue a shorter time of division and inset was prompted by patient complaints regarding burden of care associated with the time between surgeries and to address the needs of patients traveling from abroad. Compressing the pedicle manually prior to the time of division and inset is a safe way to confirm adequate capillary refill. This can be done in the office prior to proceeding to surgical separation. Although the authors found that Abbe flap division can be safely done as early as 7 days, we do not recommend pursing a shorter time period.
This study revealed a majority, 88.5%, of patients were male. This discrepancy may be partially explained by the fact that there is an excess incidence of males with orofacial clefts. In fact, the sex ratio (male/female) for cleft lip and palate is approximately 2:1 male-to-female. 12 When specifying bilateral cleft lip, there is an even higher incidence of its occurrence in male patients. 13
The average length to follow up was about 585 days ranging from 18 days to 1819 days. While 18 days is a short period to evaluate the long-term outcome, it does allow for evaluation of flap viability or necrosis, which was a main outcome explored in this study. For this reason, we did not exclude this patient.
It is important to note that only one patient, in the division performed 14 days or later group, had a history of smoking. This patient did not have any complications. No patients had a history of vascular disease, including inflammatory disease. These variables are important when considering division and inset of an Abbe flap between one and two weeks as they have a strong effect on the micro-vascularization and are associated with flap necrosis and failure.14,15
The stability of Abbe flap division and inset between week one and two may be attributed to its nature as a well-perfused axial flap (similar to a paramedian forehead flap) with its basis on the labial branches of the facial artery and its incorporation of a direct cutaneous vascular supply. 16 Axial flaps have been demonstrated to show a significantly higher survival as compared to flaps with no direct cutaneous supply. 17 Additionally, the intraoral mucosa is known for its rapid wound healing capacity 18 and has been shown to be reached extensively by perforators of the facial and labial arteries. 19 Considering that the Abbe flap inset involves vascular ingrowth from the level of skin, muscle and mucosa, this rich vascular supply may be a contributing factor allowing for flap division prior to two weeks with no instances of flap necrosis.
As the physical and social limitations imposed on a patient within the period prior to Abbe flap division are significant, attempts to improve patient and caregiver experience and reduce the overall burden of care should be considered, provided that the surgical result is not compromised. The importance of identifying a “compliant patient” in the success of the Abbe flap has been previously stressed due to the limitations in diet, speech, and socialization that results for a period of 2–3 weeks. 20 Studies have found that patients categorized as mouth breathers with pre-existing nasal obstruction have reported respiratory difficulty after Abbe flap creation and before division. 21 Additionally, patients may have worsened body image 22 which may be magnified for younger patients and patients residing in areas of the world where facial anomalies are already extremely stigmatized and ostracizing. Therefore, the process of partnering with the patient and caregiver requires substantial pre-operative education on part of the health system regarding both the functional limitations of the flap and the potential psychosocial harm that may result from living with a temporary visible tissue bridge deformity. 22 We believe that shortening the length of time before division to under two weeks without increasing complications will significantly reduce the burden of care and improve patient experience.
One of the current limitations of performing Abbe flap reconstruction in resource limited settings is the 2–3 week wait time between the first and second stage of the procedure prior to flap division. As various studies have found complication rates following cleft care magnitudes higher in low-resource settings compared to their high-income counterparts, 23 there is a crucial need to provide adequate follow-up time to prevent potentially debilitating complications. The two-stage nature of the procedures thus requires greater resources, such as time, finances, operative capacity and patient education on the part of the health organization. While successful two stage reconstructions in resource-limited settings have been performed, their success required multiple mission trips and longer patient wait times between stages. 24 As short term mission-based models in low and middle-income countries are traditionally 1 to 2 weeks in length, demonstrating safety of division earlier than 2 weeks’ aids in making Abbe flaps a more viable option to include in mission-style programs. Furthermore, in center based care, the shortened time to division and inset will facilitate reconstruction in patients who must travel long distances to their treatment center and may have limited resources.
From the perspective of the patient, the most significant barrier to receiving treatment for cleft lip or palate anomalies in the regions of sub-Saharan Africa, the Middle East, North Africa, South Asia, and Southeast Asia has been found to be the cost of transportation. 25 Costs of transportation may be high due to lack of appropriate infrastructure making domestic travel difficult, or traveling long distances to reach treatment center bases. 25 By reducing the time between procedures to less than 2 weeks, there may be a reduced need for an additional trip, greatly reducing the financial burden of transportation and making an Abbe flap a viable means of reconstruction.
As congenital cleft anomalies have been associated with a high degree of social stigmatization in low resource areas, 26 reducing the time patients have to spend with a significant facial deformity will also substantially reduce the risk of social rejection and long-standing psychosocial harm to patients undergoing a 2-stage reconstruction. The reduction of time from Abbe flap creation to division thus has significant implications for the quality of life of a patient, both in terms of physical and social limitations resulting from the newly created deformity, as well as in reducing the most significant barrier to treatment that remains the financial burdens associated with transportation.
Limitations of this study include a small, non-randomized sample size. Additionally, the authors are unable to assess the viability of the muscle or functional aspects or oral function as dynamic assessments, such as video or photograph, have not been recorded. This, however, can be a topic of a future study. Finally, the authors cannot draw a conclusion that the Abbe flap should be divided earlier than 14 days. We simply suggest that division before 14 days (between 7 and 13 days) can be a safe option and deserves further attention.
Future direction for this topic includes a randomized controlled trial exploring outcomes with Abbe flap division earlier than 14 days compared to those divided after 14 days. Additionally, surveys may be obtained by patients and their caregivers pre-and post-surgery to further assess burden of care. Finally, perfusion studies may be performed to objectively quantify the course of reperfusion and earliest safe day for division.
Conclusion
In conclusion, division and inset of an Abbe flap between day 7 and 14 may be a safe treatment option. While we cannot conclude that the Abbe flap should be divided earlier than 14 days, we suggest that division earlier than 14 days can be a safe option and warrants further attention. A shorter time to Abbe flap division can decrease the burden of care on patients and their caregivers and provide advantages to care in low-resource settings.

Patient with Abbe flap division at 7 days (top) and 9 days (bottom).

Patient with Abbe flap division at 17 days (top) and 14 days (bottom).
Footnotes
Acknowledgements
This study received ethical approval from the New York University IRB. This is an IRB-approved retrospective study, all patient information was de-identified and patient consent was not required.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.