
Abstract
Objective
Evaluate infants with Robin Sequence (RS) who were successfully treated with conservative airway measures alone vs. those who failed and eventually underwent surgical airway intervention after a protracted course of conservative management.
Design
Retrospective review of prospectively gathered database.
Setting
Large tertiary care institution.
Patients
Infants diagnosed with RS (n = 122) who underwent primary airway management at a single institution from 1994–2020.
Main Outcome Measure
Patient demographics, nutritional and respiratory status, laboratory values, and polysomnographic results were compared between patients who were discharged after successful conservative airway management (Group 1, n = 61) and patients that underwent surgical airway intervention after failing a prolonged course of conservative management (Group 2, n = 61). Receiver operating characteristic (ROC) curve analysis was done to assess continuous variables that may predict failure of conservative airway management.
Results
122 infants with RS were investigated. While several variables were significantly different between groups, the following polysomnographic
Conclusions
We identified factors in infants with RS that were associated with severe UAO that failed to improve despite weeks of conservative airway management. Our results may expedite earlier definitive treatment of these critical patients and reduce risks for known complications of prolonged UAO.
Introduction
Robin sequence (RS), the clinical triad of micrognathia, glossoptosis, and upper airway obstruction (UAO), affects approximately 1 in 8500 births.1,2 Infants may present with wide phenotypic variability, ranging from infrequent respiratory and/or feeding difficulties to severe UAO and failure to thrive. 3 Treatment options range from conservative modalities, namely prone positioning, oropharyngeal hygiene, nutritional support, and nasopharyngeal intubation,4–6 to operative interventions, such as subperiosteal release of floor of mouth, 7 tongue-lip adhesion,8–14 tracheostomy,15,16 and mandibular distraction osteogenesis.17–24
Pediatric sleep apnea has both short-term and long-term deleterious effects on multiple organ systems and the importance of early diagnosis and treatment of UOA in infants with RS has been increasingly recognized. Several studies have documented neurobehavioral and neurocognitive deficits associated with pediatric obstructive sleep apnea (OSA),25–28 which some argue are irreversible if OSA is left untreated. 29 Hypertension, increased heart rate, impaired left ventricular function, and changes in right ventricular dimensions have also been reported in children with long-standing OSA.30–32
At our institution, infants with RS are managed by a multidisciplinary team that provides a holistic and deliberate approach to the management of these complex patients. Except in cases of immediate, emergent airway compromise, every effort is made to treat UAO using conservative measures alone. Nevertheless, our group and others have demonstrated that some patients who may initially improve with conservative interventions, ultimately fail this approach and require a surgical airway procedure.33,34 While our institution previously published clinical factors associated with successful conservative airway management in infants with RS, 35 a direct comparison with patients who failed conservative airway treatment was not performed. To establish an evidence-based set of guidelines, we therefore designed a study to review airway management in patients with RS at our tertiary care center and identify clinical factors that may predict failure of conservative airway management in these complex patients and avoid an unnecessary, prolonged preoperative course.
Methods
A retrospective review of a prospectively gathered database was undertaken for patients with RS who underwent primary airway management at a large tertiary care hospital from 1994–2020. After obtaining IRB approval, the study cohort was identified by performing a search within the billing departments for the Division of Plastic and Reconstructive Surgery, as well as Otolaryngology and Neonatology, using International Classification of Diseases, version 9 (ICD-9) codes for anomaly of jaw size and related diagnoses (524.00, 524.06, 524.10) as well as Current Procedure Terminology (CPT) codes for tongue-lip adhesion (TLA), mandibular distraction osteogenesis (MDO), and tracheostomy (41510, 20690/20692, and 31600/31601/31603/31605, respectively). In addition, a review of an IRB approved, prospectively gathered database for patients with RS maintained by the Division of Plastic and Reconstructive Surgery was performed to cross-reference with billing data.
Inclusion criteria consisted of patients with RS who were managed at our institution. When available, polysomnogram (PSG) data was included if it was completed within 90 days before admission, during the hospital stay or before any surgical treatment was performed. In patients who were discharged after successful conservative management, PSG was included if performed within 90 days of discharge. Patients with micrognathia and non-obstructive respiratory failure (eg, congestive heart failure, renal failure), as well as those who received definitive airway management at an outside hospital, were excluded from the study.
Information recorded from all cases included demographic characteristics, preexisting medical conditions and/or associated syndromic diagnosis, consecutive weight measurements during admission, PSG (when available), surgical treatment and discharge. In addition, hospital factors such as type of nutritional gavage feeding, type of respiratory support, and desaturation events were recorded.
Maximum titratable bicarbonate (maxHCO3) and maximum carbon dioxide (maxCO2) were drawn via capillary blood gas (CBG). PSG data were obtained as previously described by our group 36 and the following variables were collected: Total apnea-hypopnea index (AHI), obstructive apnea-hypopnea index (OAHI), central apnea index (CAI), lowest oxygen saturation (%), sleep time with O2 saturation < 90%, mean ETCO2 and maximum ETCO2.
Patients were divided into two groups, based on definitive airway management. Group 1 patients were discharged from the hospital after successful treatment using only conservative measures that included lateral/prone positioning, oropharyngeal hygienic support, enteric nutritional feeding, and respiratory support, including nasopharyngeal tube insertion by otolaryngology. Patients in Group 2 failed a prolonged course of conservative treatment and underwent surgical airway procedures, including tracheostomy, TLA, and MDO.
Multidisciplinary Team Protocol
All infants with suspected RS at CNH are managed by a multidisciplinary team protocol. For in-patients, consultation from key team members is obtained with 24–48 h of admission, including plastic surgery, otolaryngology, genetics, pulmonary medicine, general surgery, as well as speech/feeding therapy. Bedside flexible endoscopy is performed to assess the airway. If patients have not shown significant improvement with conservative airway management after several days, they undergo direct laryngoscopy/bronchoscopy (DLB) and drug induced sleep endoscopy (DISE), as well as PSG. Conservative measures were attempted for as long as possible, until both the family and multidisciplinary deemed further efforts to be either futile or unsafe. Patients who meet the GILLS criteria8,37 are offered TLA, in addition to MDO, the latter now being our procedure of choice for most patients. Infants with severe dysmorphia, hypotonia, or multi-level airway obstruction undergo tracheostomy, which is otherwise reserved as a final option.
Statistical Methods
Baseline demographics and hospital factors were compared between the two groups (conservative vs. surgical management). Unpaired t-test and Wilcoxon-Mann-Whitney U tests were used to compare normally distributed and skewed continuous data, respectively. Categorical variables were compared using the Chi-square test and Fisher's exact test (if any of the expected cell sizes was less than 5). Additional analysis was completed in patients with PSG data available. Summary statistics for continuous variables were presented as mean with standard deviation for normally distributed data and median with interquartile range (IQR) for skewed data. Categorical data were summarized as frequencies with percentages. Normality assumptions were checked using a statistical test (eg, Shapiro Wilk test) as well as graphical methods (eg, histogram, q-q plot). A multivariable logistic regression analysis was performed to determine the independent hospital and patient factors associated with failed conservative management. Variables were selected in the multivariable model based on statistical significance (p < 0.05) in the univariate analyses.
To assess the predictive ability of continuous variables found to be significantly different between groups on univariate and multivariable analyses, we performed receiver operating characteristic (ROC) curve analysis. Accuracy was graded based on the area under the curve (AUC) defined as “poor” (AUC 0.60–0.70), “fair” (AUC 0.70–0.80), “good” (AUC 0.80–0.90), and “excellent” (AUC 0.90–1.00). 38 The optimal cut-points were calculated using the Youden index (J) method. 39 This method calculates the optimal cut-point by maximizing the Youden function which is the difference between true positive rate and false-positive rate over all possible cut-point values. Sensitivity and specificity at the optimum cut point was also calculated. All statistical tests were two-sided and were performed at the 5% level of significance unless otherwise stated. Stata software, version 15.1 MP (Stata Corporation, College Station, Texas, USA) was used for all statistical analyses.
Results
122 infants were included. Syndromic association was noted in roughly half of all patients (50.4%). Demographic results are summarized in
Overall Demographics.
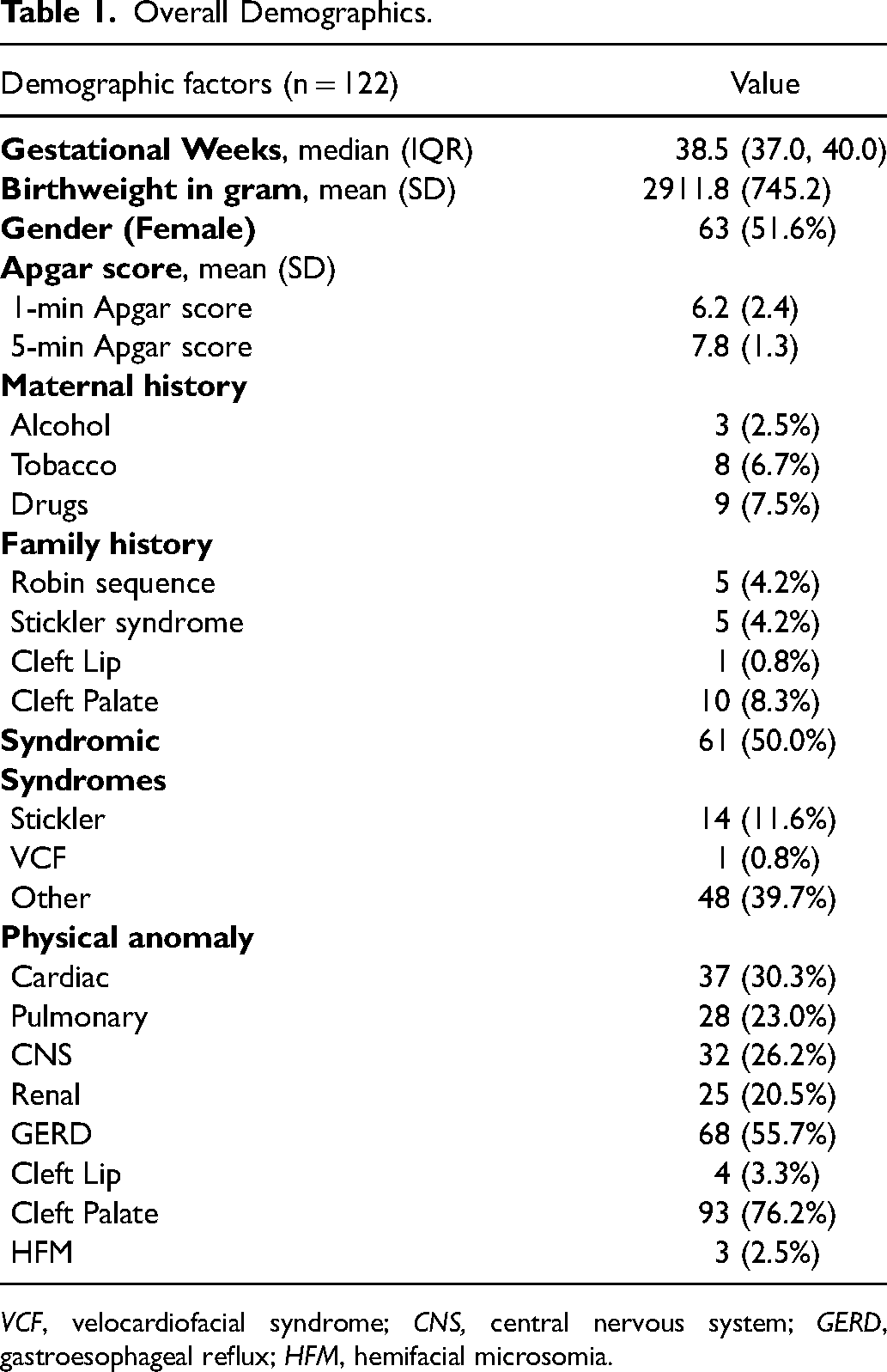
VCF, velocardiofacial syndrome; CNS, central nervous system; GERD, gastroesophageal reflux; HFM, hemifacial microsomia.
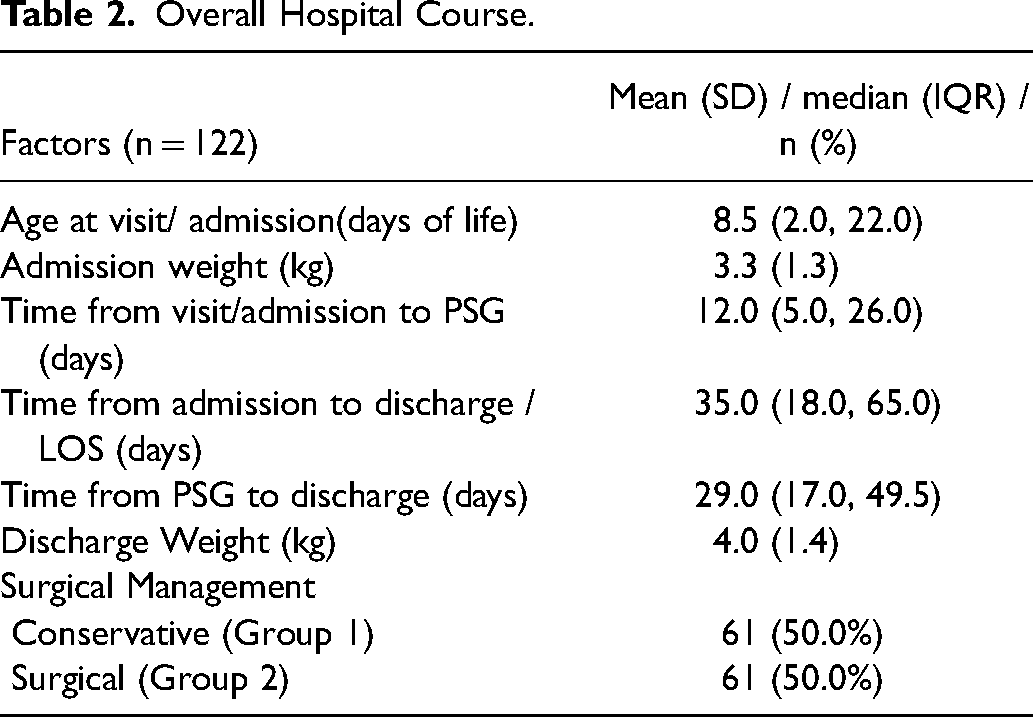
Overall Hospital Course.
Patient Factors by Type of Airway Management.
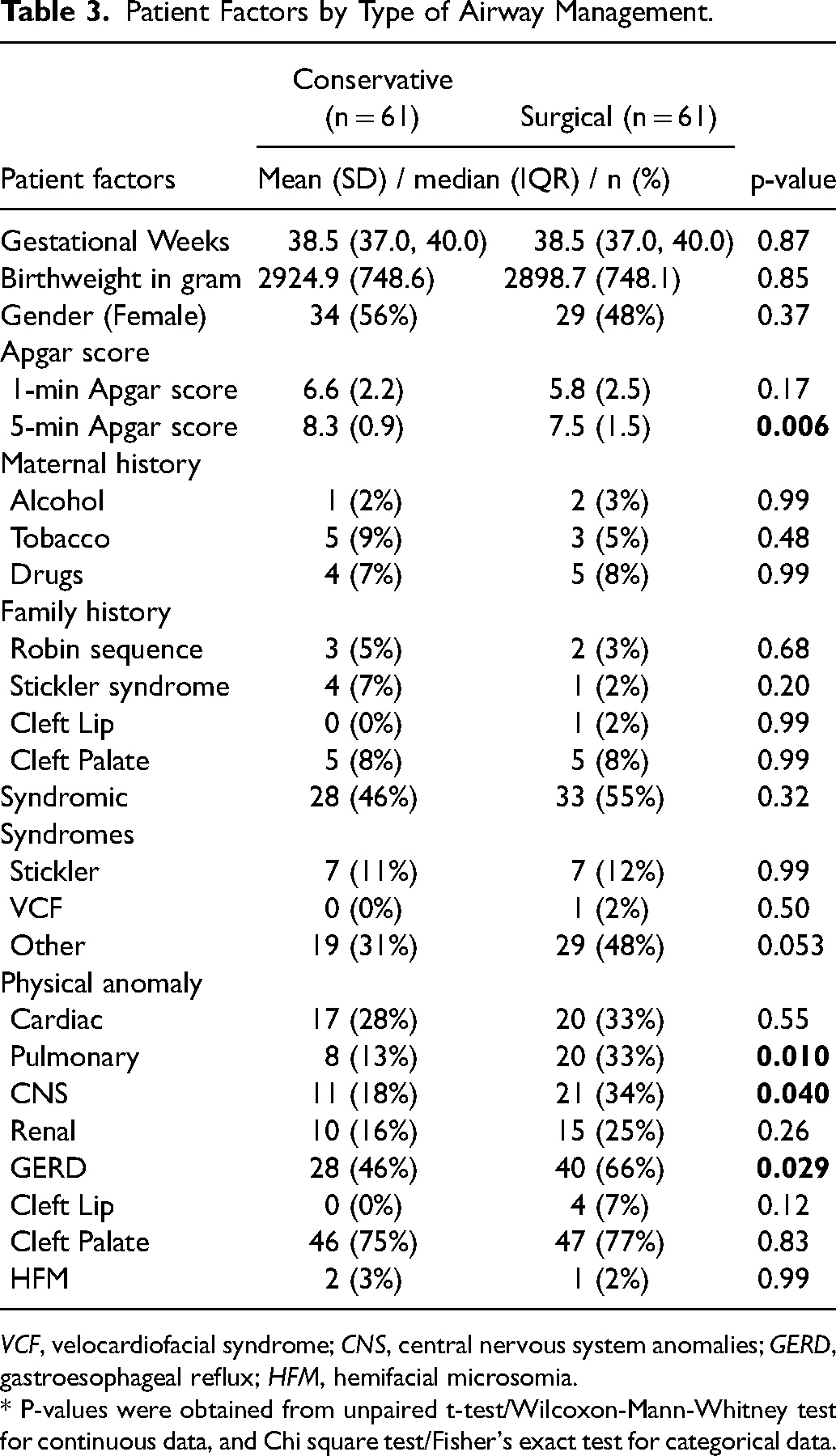
VCF, velocardiofacial syndrome; CNS, central nervous system anomalies; GERD, gastroesophageal reflux; HFM, hemifacial microsomia.
* P-values were obtained from unpaired t-test/Wilcoxon-Mann-Whitney test for continuous data, and Chi square test/Fisher's exact test for categorical data.
Hospital Factors by Type of Airway Management.
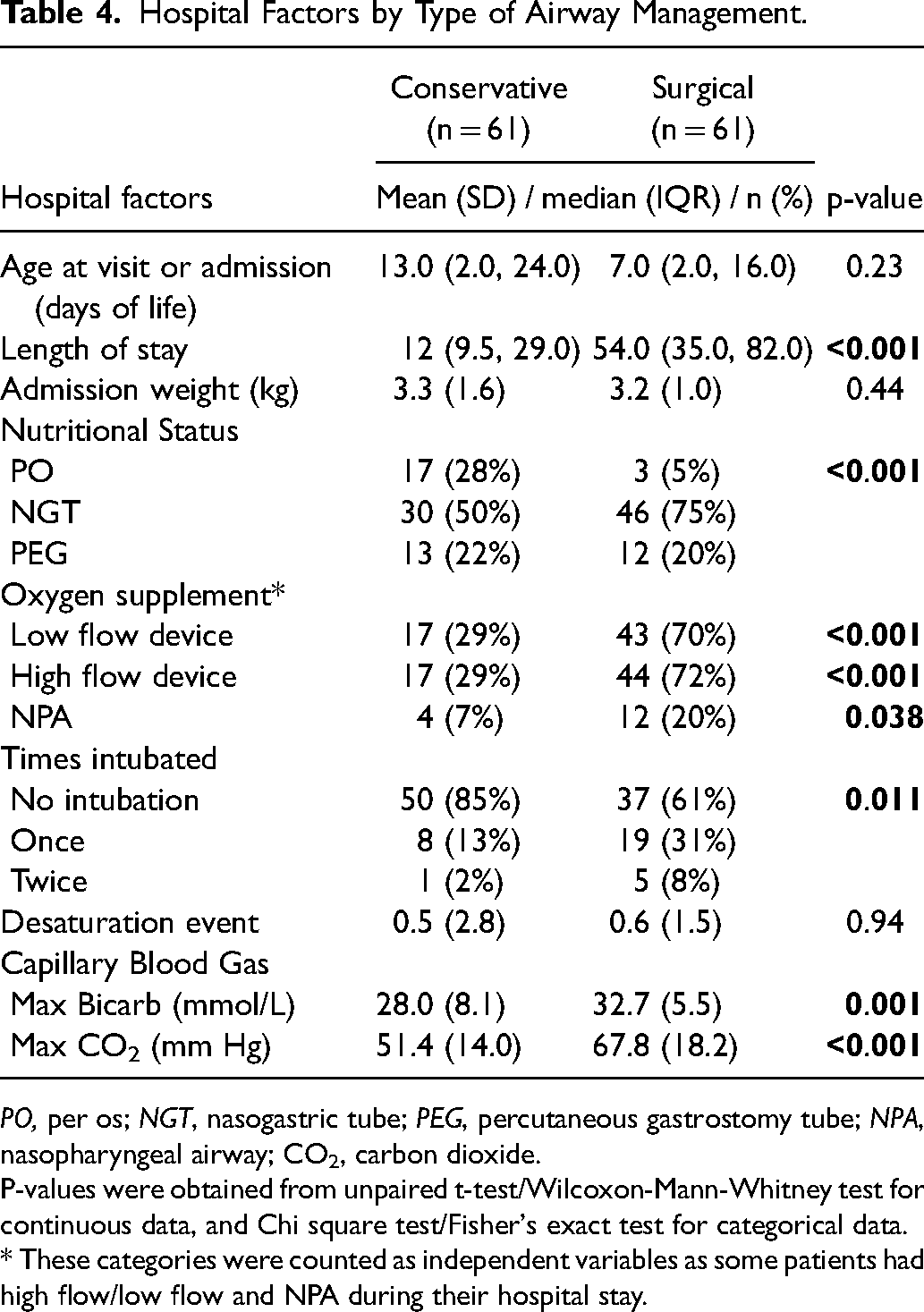
PO, per os; NGT, nasogastric tube; PEG, percutaneous gastrostomy tube; NPA, nasopharyngeal airway; CO2, carbon dioxide.
P-values were obtained from unpaired t-test/Wilcoxon-Mann-Whitney test for continuous data, and Chi square test/Fisher's exact test for categorical data.
* These categories were counted as independent variables as some patients had high flow/low flow and NPA during their hospital stay.
To further investigate the independent hospital and patient factors associated with failure of conservative airway management, we performed a multivariable logistic regression analysis on the statistically significant variables identified by univariate analysis above (highlighted in Tables 3 and 4). This multivariate model demonstrated that none of the parameters identified by univariate analysis were statistically correlated with unsuccessful conservative airway measures, with the exception of greater LOS correlating with a surgical airway procedure (adjusted odds ratio 1.03, 95% CI: 1.01–1.06, p = 0.040).
PSG could not be obtained for intubated patients or those on significant O2 support, for obvious reasons (n = 18, 14.8%). In addition, patients who rapidly improved with conservative measures did not undergo PSG (n = 25, 20.5%), at the discretion of the neonatology team. Hence, a total of 79 patients (64.8%) had PSG data available. The median age at PSG was 23.0 days (IQR: 11.0, 49.0 days). As noted above, patients in Group 2 had surgery at a median of 14.0 days (8.0, 22.0) after sleep study was obtained. PSG variables are shown in
PSG Variables by Type of Airway Management.
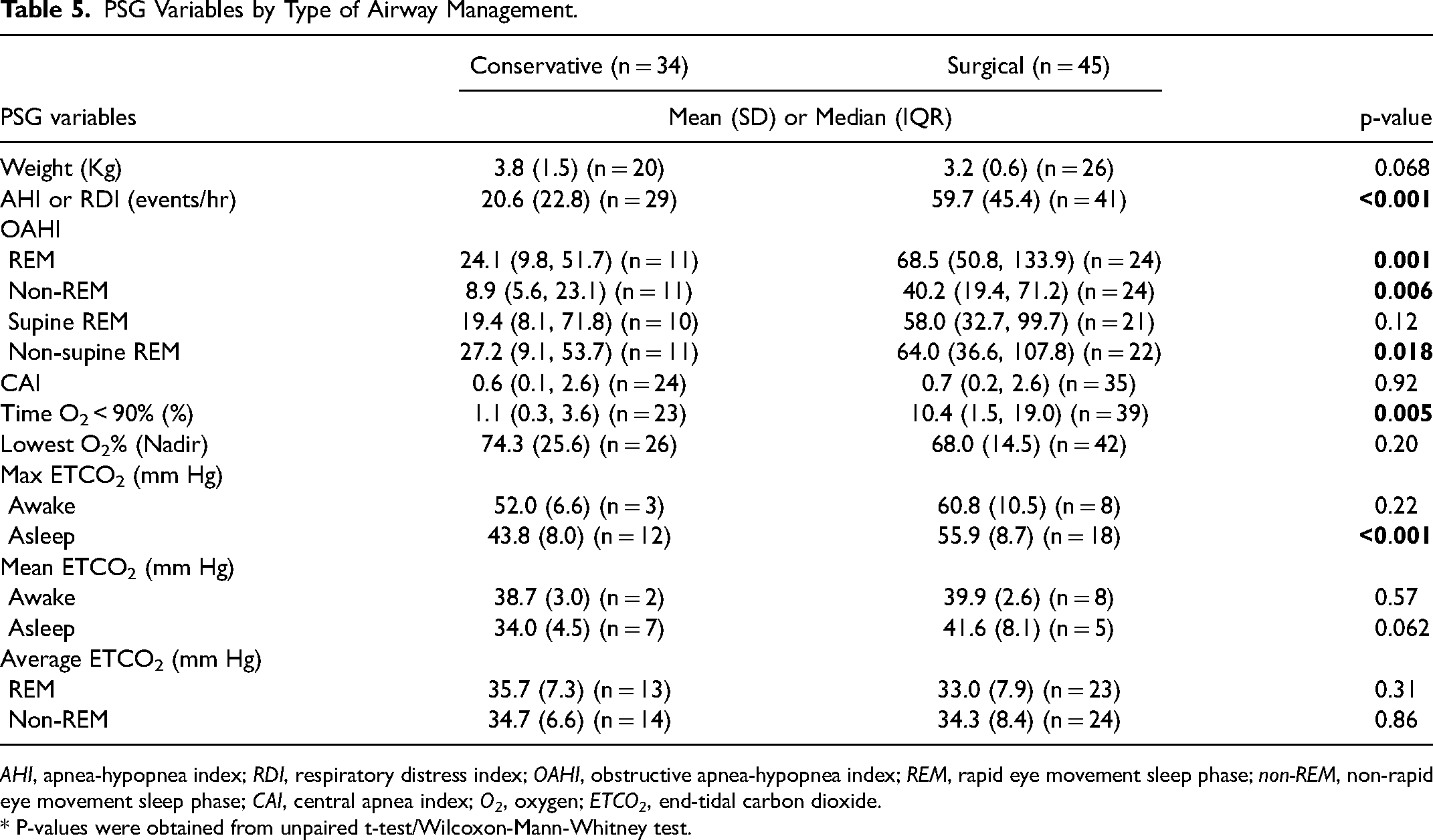
AHI, apnea-hypopnea index; RDI, respiratory distress index; OAHI, obstructive apnea-hypopnea index; REM, rapid eye movement sleep phase; non-REM, non-rapid eye movement sleep phase; CAI, central apnea index; O2, oxygen; ETCO2, end-tidal carbon dioxide.
* P-values were obtained from unpaired t-test/Wilcoxon-Mann-Whitney test.
ROC curve analysis was done on those continuous variables that were statistically different between groups, as identified by previous univariate analysis. AHI, OAHI REM, OAHI Non-REM, and maximum ETCO2 (asleep) were shown to be “good” predictors for surgical airway management (
Supplemental Figure
ROC Analysis.
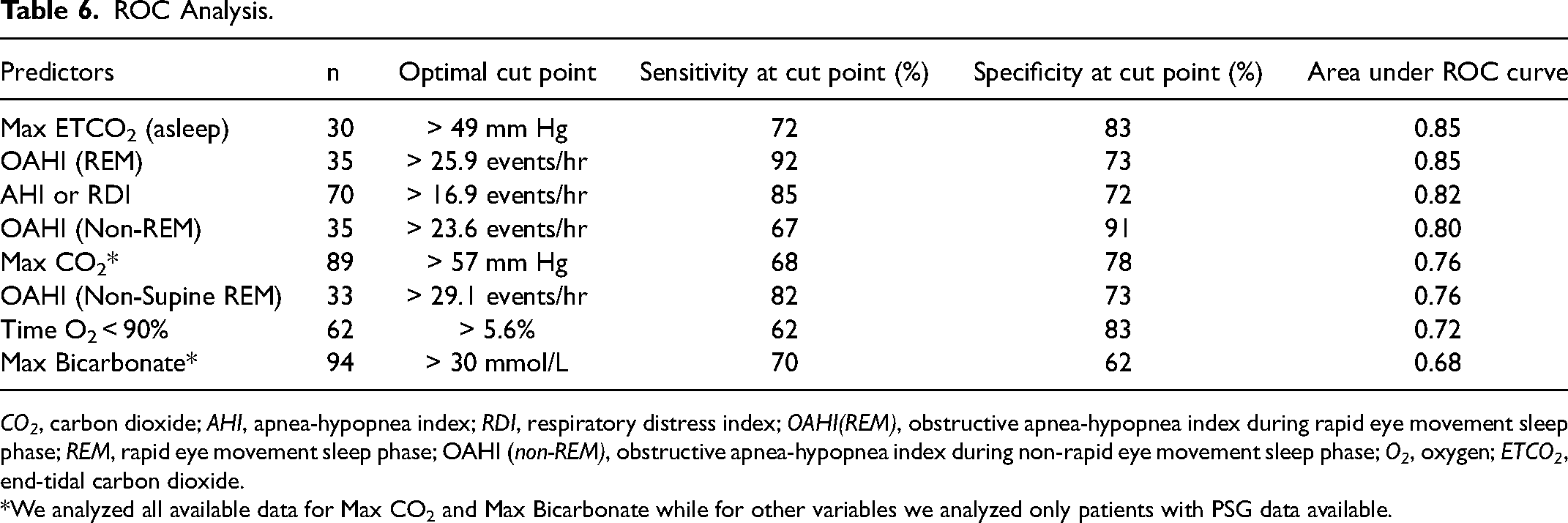
CO2, carbon dioxide; AHI, apnea-hypopnea index; RDI, respiratory distress index; OAHI(REM), obstructive apnea-hypopnea index during rapid eye movement sleep phase; REM, rapid eye movement sleep phase; OAHI (non-REM), obstructive apnea-hypopnea index during non-rapid eye movement sleep phase; O2, oxygen; ETCO2, end-tidal carbon dioxide.
*We analyzed all available data for Max CO2 and Max Bicarbonate while for other variables we analyzed only patients with PSG data available.
Discussion
While the need for surgical airway intervention may be obvious in some patients with RS, optimal treatment for a significant proportion of patients may be less apparent. The decision-making process to cease futile conservative airway interventions and proceed with a surgical airway procedure in these patients lacks consensus and remains controversial. The authors therefore designed the current study with the primary objective of identifying clinical factors in infants with RS who fail a prolonged course of conservative airway management. The current investigation represents the largest single institutional study specifically designed to address this challenging issue of predicting failure of conservative airway management.
The authors’ primary impetus for the current investigation was the growing body of evidence supporting concerns that delayed correction of airway obstruction in the pediatric population may pose a significant increased risk for future problems. Speech and language delays, 40 hypertension, cardiac dysfunction, and abnormal autonomic system, 41 cor pulmonale, aspiration pneumonia, and/or failure to thrive, hypoxic brain damage, impaired mental development have been documented in young patients with chronic OSA,16,42 as well as increased risk for hyperactivity and aggression, anxiety and depression,25,43 and deficits in spatial memory, verbal comprehension, and reasoning,44–46 although the majority of these studies were done in young children and not in infants. Additionally, care of infants with RS can require prolonged hospitalization, ranging from 10 to 60 days,47–50 and translate into exorbitant costs of care; moreover, the mortality rates of up to 13.7% for infants with RS are not inconsequential,3,16,48,49,51 with incidences as high as 26% for syndromic patients alone.14,52 With these considerations in mind, we aimed to identify and compare infants with RS managed by our multidisciplinary team after successful conservative airway measures vs. those who failed a prolonged course of conservative treatment and ultimately, underwent a definitive surgical airway procedure. It is important to underscore that operative airway intervention was not performed until a median period of 23.0 days after admission and 14.0 days after PSG. Thus, patients were treated conservatively for a number of weeks before a definitive surgical airway procedure was performed. This provided a unique opportunity to investigate uncharacterized differences between those patients who were successfully managed with conservative measure alone vs. those who ultimately failed and required a definitive surgical airway.
In our study of 122 patients, we identified both categorical and continuous clinical factors associated with failure of conservative airway management. Categorical factors included: (1) greater incidence of systemic anomalies; (2) need for supplemental O2 support. Continuous clinical factors associated with failure of prolonged, conservative airway management included: (1) maximum CO2; and (2) maximum HCO3 on capillary blood gas, as well as; (3) AHI; (4) OAHI during REM; (5) OAHI during non-supine REM sleep; (6) OAHI during non-REM sleep; (7) time with O2sat <90%; and (8) maximum ETCO2 (asleep) during polysomnography (
Other groups have promulgated their indications for surgical airway intervention. While desaturation events are the most frequently reported indication for surgical intervention in RS patients with upper airway obstruction 53 our findings suggest this criterion has poor predictive value. Our study did not find a significant difference in the nadir spO2 between groups, with a mean nadir spO2 of 74% in Group 1 and 68.0% in Group 2 (p > 0.05). Similarly, though our study identified that time O2 saturation < 90% to be a significant predictor of failed conservative airway management on univariate analysis (Group 1 vs. Group 2, 1.1% vs. 10.4%, p < 0.005), ROC analysis documented this variable to be only a “fair” predictor (AUC = 0.72).
Markers of carbon dioxide retention have also been described as indicators for surgical airway management in patients with RS.2,12,47,51,54–57 Fahradyan and colleagues (2019) reported the use of CBG CO2 in 73 patients with RS and stated that ROC curves with cutoff value of pCO2 level of 49.5 were the best among other variables in terms of specificity and sensitivity combination as an indication for surgical intervention. 58 Kwan and associates (2021) also noted that a PCO2 cutoff of 55 mmHg (sensitivity = 55.7%; specificity = 91.3%; AUC = 0.78) and a HCO3 cutoff of 30 mEq/L (sensitivity = 56.2%; specificity = 95.0%; AUC = 0.80) were most predictive of patients who “required” a surgical airway. 59 Neither of these studies specifically documented how the authors determined their surgical airway indications. It is also somewhat disconcerting that most patients (greater than 70%) in these studies “required” a surgical airway, despite the widely held belief that the majority of patients with RS can be successfully managed without a surgical airway. Our own study provides some support for the association of CO2 retention with eventual failure of conservative airway management in patients with RS. Nonetheless, the current study demonstrated that both CBG CO2 and HCO3 were only “fair” and “poor” predictors of prolonged failed conservative airway management, AUC of 0.76 and 0.68, respectively, while maximum ETCO2 while asleep during PSG was one our strongest predictors (AUC = 0.85). Interestingly, the use of maximum ETCO2 as a criterium for surgical intervention in RS is not reported in the literature. In their experience of conservative versus surgically managed RS patients, Runyan et al. found no difference in mean ETCO2 between groups. 60 Kam and colleagues also found no difference in mean ETCO2 when comparing those managed conservatively vs. surgically. 61 However, neither group independently reported maximum ETCO2, whereas the current study specifically investigated both factors as potential predictors of failed conservative airway management, though mean ETCO2 was not significantly different between groups.
This lack of consensus regarding indications for surgical airway was underscored by a recent survey study by Fan et al., who found a wide range of minimum AHI for surgical intervention, with 78% using a threshold of at least 10 events/hour, and 35% of at least 20 events/hour. 62 Reddy and associates also provided a literature review revealing mean AHI ranging from 6.4 to 52.6 events/hour in surgical management of RS. 63 Runyan and colleagues recommend surgery be considered at an AHI of 20 events/hour based on their 10-year retrospective review, 60 while Cladis et al. recommend intervention for AHI > 5 events/hour. 64 Our PSG analysis provides added granularity to the quantification of AHI by independently comparing OAHI during REM and non-REM sleep and when positioned supine and non-supine in REM. Sleep stage impacts tone, with REM sleep associated with hypotonia of the chest wall and upper airway muscles. 65 Accordingly, OAHI in REM sleep was significantly higher in patients who eventually failed conservative airway management; this factor was also a “good” predictor of the need for surgical intervention by ROC analysis (AUC 0.85, cut point 25.9 events/hour).
The diagnostic appropriateness of PSG in the infant population is not without controversy. Daftary and colleagues recently documented OSA parameters well above the standards set by the American Academy of Sleep Medicine.66 Their investigation in healthy full-term infants at a mean age of 19.6 days demonstrated a mean AHI of 14.9 events/hour, though the majority were hypopneic events. While the current study documented AHI cut point of 16.9 events/hour, we also identified OAHI (REM) cut point of 25.9 events/hour and OAHI (non-REM) cut point of 23.6 events/hour. These latter two parameters were not specifically studied by Daftary and associates, but their findings and our own results question the appropriateness of using AHI values of 5 or even 10 events/hour as an indication for surgical airway intervention, as was most used by respondents to the survey performed by Fan and colleagues. 61
The current study has limitations. Due to its retrospective design, our findings are not as robust as those in a prospective RCT. Although all data are gathered prospectively, the authors have not adhered to a strict treatment protocol, as modifications are continuously made in an effort to improve patient outcomes. Other limitations included the relatively small study population and absence of polysomnographic data in all cases. Nonetheless, our sample size of 122 patients is the largest from a single institution to address this issue. In addition, our patient cohort, comprised of roughly 50% syndromic patients, represents a selection bias that must be acknowledged. The authors recognize that many, if not most, patients with nonsyndromic RS succeed with conservative airway management. Nevertheless, the goal of this study was to identify characteristics of patients with RS that ultimately fail conservative airway management, which may guide clinicians in the treatment of those who are not readily or obviously categorized into the conservative or surgical groups. The lack of PSG data in all patients may be viewed as a selection bias, as well. As noted in our Results, PSG data could not be obtained in patients who required prolonged intubation or supplemental O2, which precluded accurate investigations. Thus, the decision to perform a surgical airway procedure on these patients was less controversial. Similarly, those patients who clearly and quickly improved with conservative airway measures did not undergo PSG, which makes intuitive sense. Finally, one must acknowledge the reality in which care for neonates with RS is delivered. Providers are routinely stratifying patients using all available data, some of which have been validated in our analysis. An exhaustive RCT of conservative management vs. early surgical airway intervention for every patient is not realistic, nor is it always what is best for the patient, the family or the utilization of health care resources. Prolonged hospitalizations increase costs and are a source of stress for families. One study reported an average LOS of conservative management of 64 days, higher than our mean LOS for our surgical cohort (54 days) and well above our mean LOS for our conservative group (12 days). 33 Although these authors did not find a significant difference in cost between their surgical and conservative patients, differences between Canadian and American healthcare systems should be recognized. One must remember the purpose of intervention in RS: to reduce mortality and the negative physiologic impact of prolonged airway obstruction. Extended conservative management in the hospital may reduce the chance of a catastrophic event but may not mitigate the physiologic effects of long-term airway obstruction.
Conclusions
Identifying objective clinical parameters that may predict failed conservative airway management in infants with RS remains a challenge, given the realities of clinical medicine. The imperfection of each individual factor is illustrative of the heterogeneity of this patient population. As such, an objective approach that accounts for an array of predictors is more suitable to the disease process. Therefore, for patients who are not easily categorized into a conservative or surgical airway treatment protocol, we propose a set of contributing predictors of failure of conservative management: max
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231224194 - Supplemental material for Predicting Failure of Conservative Airway Management in Infants with Robin Sequence: The EARN Factors
Supplemental material, sj-docx-1-cpc-10.1177_10556656231224194 for Predicting Failure of Conservative Airway Management in Infants with Robin Sequence: The EARN Factors by Jennifer L. McGrath, Esperanza Mantilla-Rivas, Marudeen Aivaz, Monica Manrique, Md Sohel Rana, Hannah R. Crowder, Nathanael S. Oh, Gary F. Rogers and Albert K. Oh in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of institutional review board approval and/or statement of conforming to the Declaration of Helsinki
This study was approved by the Institutional Review Board for human research (Pro00014271) at the Children's National Hospital, Washington, DC.
Presentation
Presented, in part, at the 12th Congress of the Asian Pacific Craniofacial Association, December 2018; International Society of Craniofacial Surgery, Virtual Symposium, October 2021; 90th Annual Meeting of the American Society of Plastic Surgeons, October 2021.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.