
Abstract
Objective
The coronavirus (COVID-19) pandemic presents an opportunity to study stress's effect on the development of non-syndromic orofacial clefts (NSOFCs). This study was aimed at assessing maternal stress exposure during the pregestational to first trimester pregnancy periods and the development of NSOFCs during a year of the COVID-19 pandemic.
Design
Cohort study of infants with NSOFCs and controls matched based on recruitment site and age.
Setting
Government hospitals in Saudi Arabia between November 2020 and November 2021.
Main Outcome Measures
Data collection included NSOFC clinical examination and maternal stress exposure assessment using the Modified Life Events Questionnaire, the Fear of COVID-19 Scale, and a focus on the lack of pregnancy planning and a threatened miscarriage.
Results
Of the 557 infants recruited, 191 had NSOFCs. Logistic regression analysis with adjusted odds ratios (AORs) that removed the effects of confounders showed that any of the seven stressful life events (AOR:3.78, P < .001) and the family histories of relatives with NSOFCs (AOR:9.73, P < .001) increased the AOR for NSOFC development. In contrast, maternal folic acid (AOR:0.56, P.010), threatened miscarriage (AOR:0.17, P = .001), fear of COVID-19 (AOR:0.83, P = .038), and suspected COVID-19 infection (AOR:0.43, P = .008) decreased the AOR for NSOFC development.
Conclusion
Along with an established risk associated with family history of birth defects, stressful life events may be a risk factor for NSOFC development. Beyond folic acid's known benefit, it may be that higher maternal health concerns contribute to increased protective health behaviors during pregnancy. Ongoing research is needed to specify the maternal risk factors for NSOFC.
Introduction
Non-syndromic orofacial clefts (NSOFCs) result in various functional and esthetic problems in children, such as higher morbidity rates, feeding difficulties, and speech difficulties, and require long-term treatment. These NSOFC life consequences can hinder children's social interactions, which can add to the financial and psychological burden that NSOFCs place on the family. 1
Genetics, the environment, and gene-environment interactions have been investigated to determine the causative factors for NSOFCs.2–5 Maternal stress has been suggested as a potential contributor to the etiology of NSOFCs6,7; however, the underlying mechanism is not fully understood. Some studies have linked maternal stress to the inflammatory activity attributed to elevated cortisol levels in the blood as reported in the literature, which is known to have a teratogenic effect.6–10 It has also been proposed that maternal stress may activate the fight-flight response that requires muscular blood profusion, leading to placenta hypoperfusion and fetal damage. 11
The World Health Organization announced the COVID-19 pandemic on March 11, 2020. 12 The pandemic posed many challenges to society, affecting many individuals’ mental health.3,13,14 Other risk factors known to be associated with the development of NSOFCs were amplified during the pandemic, such as smoking15,16 and various illnesses.17,18 Hence, the pandemic constitutes an ideal time to evaluate the effects of stress on NSOFC development. This study's aim was to assess maternal stress exposure during the pregestational period to first trimester of pregnancy and the development of NSOFCs during a year of the COVID-19 pandemic.
Materials and Methods
This cohort study was conducted at government hospitals in the Kingdom of Saudi Arabia between November 2020 and November 2021. In each region, we identified the main maternity and children's hospitals, as well as the main cleft referral centers using the Saudi Ministry of Health's list of hospitals 19 (Supplementary Table 1). The study received approval from the Research Ethics Committee of King Abdulaziz University (257-07-21), King Fahad Medical City (20-642), the Ministry of Health (H-02J-022), and King Abdullah International Medical City (H-01-R-005).
Subjects
All infants born with NSOFCs between November 2020 and November 2021 at the designated 23 maternal and referral governmental hospitals were included in this study (Supplementary Table 1). This period was selected to assure that the first trimester of pregnancy had occurred during the COVID-19 pandemic. 12 The controls were healthy infants recruited from the hospitals’ neonatal units or baby-well clinics, matched based on the recruitment site and the month of birth.
Sample Size Calculation
The sample size was calculated using open-source epidemiological statistics for public health with a power of 80% and a confidence interval of 95%. Although a sample size of 87 patients and 174 controls was found to be sufficient for detecting statistical significance, 20 all patients diagnosed with NSOFCs between November 2020 and November 2021 were recruited and matched with the appropriate controls to improve the results’ statistical power. In addition, an increased control-to-case ratio was used to increase the power.
Methods
Throughout the study period, once the study coordinator identified a newborn with an NSOFC in any of the designated hospitals, the case was immediately examined, and a control was selected. During the first week after the child's birth, the parents of the NSOFC newborn and the controls were contacted. Some patients were recruited after they were referred to the tertiary center and examined in orthodontic or maxillofacial surgery clinics. The study design, methodology, and aims were explained to the parents, after which written informed consent was obtained and interviews completed.
Collaboration and ascertainment were conducted to ensure proper data collection. Once a hospital research coordinator was assigned to the study, the main researcher held a virtual meeting with them. The design and methodology were discussed in detail with examples and were standardized between the data collectors. In addition, during the study, the main researcher conducted monthly meetings with the research coordinators. Moreover, the main researcher periodically visited the included hospitals and reviewed patient records to match them with the included cases.
Clinical Examination
The clinical examinations of NSOFCs were performed in neonatal intensive care units (NICUs) using lights and mirrors. The principal investigator excluded syndromic orofacial clefts based on information that the patient's pediatrician and/or geneticist provided. NSOFCs were classified using the LASHAL classification system.21,22 The acronym LASHAL stands for lip (L), alveolus (A), hard palate (H), and soft palate (S). In this classification, lowercase letters indicate an incomplete cleft, whereas uppercase letters indicate a complete cleft. The location of the letter in the acronym indicates whether the cleft is on the right or left side of the mouth.21,22 NSOFCs were then grouped into the following categories for analysis: a cleft lip with or without a cleft palate (CL ± P) or a cleft palate (CP). Cleft lip (CL) and cleft lip with cleft palate (CLP) were grouped together under CL ± P in the analysis because they are known to have similar etiologies. 23
Measures
Parents were asked orally about their sociodemographic characteristics, including family income)low family income of <6000 Saudi Riyal (SR), moderate family income of 6000 to 16,000 SR, and high family income of >16000 SR), 24 parental education level, parental age, child's gender, and date of birth. A data collection tool was validated in English and Arabic for face validity with 20 parents to ensure the questions’ clarity. Six experts assessed content validity, and the content validity index was 0.9. The items included maternal exposure during the three-month pregestational period and first trimester, such as exposure to folic acid supplements, infections due to illnesses, and nicotine. A COVID-19 infection, the flu, a fever, and asthma during the pregestational period and first trimester were deemed illnesses. Parents were also asked about their family histories related to birth defects and consanguinity.
Maternal stress was subjectively evaluated using various methods. First, the modified Life Events Questionnaire, previously validated in Arabic and English,25,26 was used to evaluate exposure to different maternal stressors. It comprises yes/no questions about seven stressful life events (familial pressure, a marital status change, a change in family residency, a work state change or leave, familial problems, problems with friends or neighbors, and robbery). Second, as the lack of pregnancy planning has been suggested to influence maternal stress, 27 this variable was included to evaluate stress's effect on NSOFC development. Third, the Fear of COVID-19 Scale 28 validated in Arabic and English28,29 was used to assess maternal COVID fear and was conceptualized as a source of stress. It comprises seven yes/no questions: “I am most afraid of COVID-19”; “it makes me uncomfortable to think about COVID-19”; “my hands become clammy when I think about COVID-19”; “I am afraid of losing my life due to COVID-19”; “when watching news and stories about COVID-19 on social media, I become nervous or anxious”; “I cannot sleep because I am worrying about getting COVID-19”; “my heart races or palpitates when I think about getting COVID-19.” Mothers were asked to recall how they felt during the three months leading up to the pregnancy and during the first trimester when answering the Fear of COVID-19 Scale. The scale's total score was calculated. A reliability test for the Fear of COVID-19 Scale was performed, and Cronbach's alpha was 0.85. Fourth, a threatened miscarriage, explained as “the possibility of [a] spontaneous abortion,” was deemed a source of stress for pregnant mothers and was recorded using a yes/no question.
SPSS Statistics 19 was used for data entry and analysis. Nominal and ordinal data were described as frequencies and percentages. Groups were compared using the chi-square test, employing p-values and odds ratios. However, when the cell count was <5, Fisher's exact test was used. Descriptive data are described as means and medians. Differences between the groups were determined using an independent sample t-test. A binary logistic regression model incorporated factors previously determined to be risk factors for NSOFCs. NSOFC, CL ± P, and CP were deemed dependent factors. The following were deemed independent factors: maternal exposures (folic acid supplements, illnesses, a COVID-19 infection, a suspected COVID-19 infection, paternal nicotine use, any stressful life event, the mean score of the total Fear of COVID-19 Scale, pregnancy planning, a threatened miscarriage), family history, and parental consanguinity. Mothers were considered to be exposed to stress if they were exposed to any of the seven stressful life events. The p-value was set at 0.05.
Results
A total of 557 infants were recruited over 12 months after 140,380 living births were screened at the designated maternity hospitals, and 40 NSOFC cases were referred to the included referral centers (after cases born at the included hospitals were excluded). The NSOFC cases comprised 191 out of 217 eligible participants (88% response rate) who were grouped into 136 (71.2%) with CL ± P and 55 (28.8%) with CP. The participants were recruited from different regions: the central (120, 32.8%), western (144, 39.3%), eastern (54, 12.3%), southern (46, 12.6%), and northern (11, 3%) regions.
No significant differences were found between the participants with NSOFCs and the controls in terms of the participants’ sociodemographic characteristics. However, more mothers of NSOFC infants reported exposure to medications compared with the controls. This was significant among CP (P = .03). In contrast, the use of maternal folic acid was significantly less in the mothers of NSOFC infants compared with the controls (P < .001 for NSOFC). Maternal reports of the medications and supplementations used during the pregestational period and first trimester are listed in Table 1 and Supplementary Table 2.
The Distribution of Participant Sociodemographic Information, Maternal Exposures During the Pregestation or 1st Trimester and Family History.
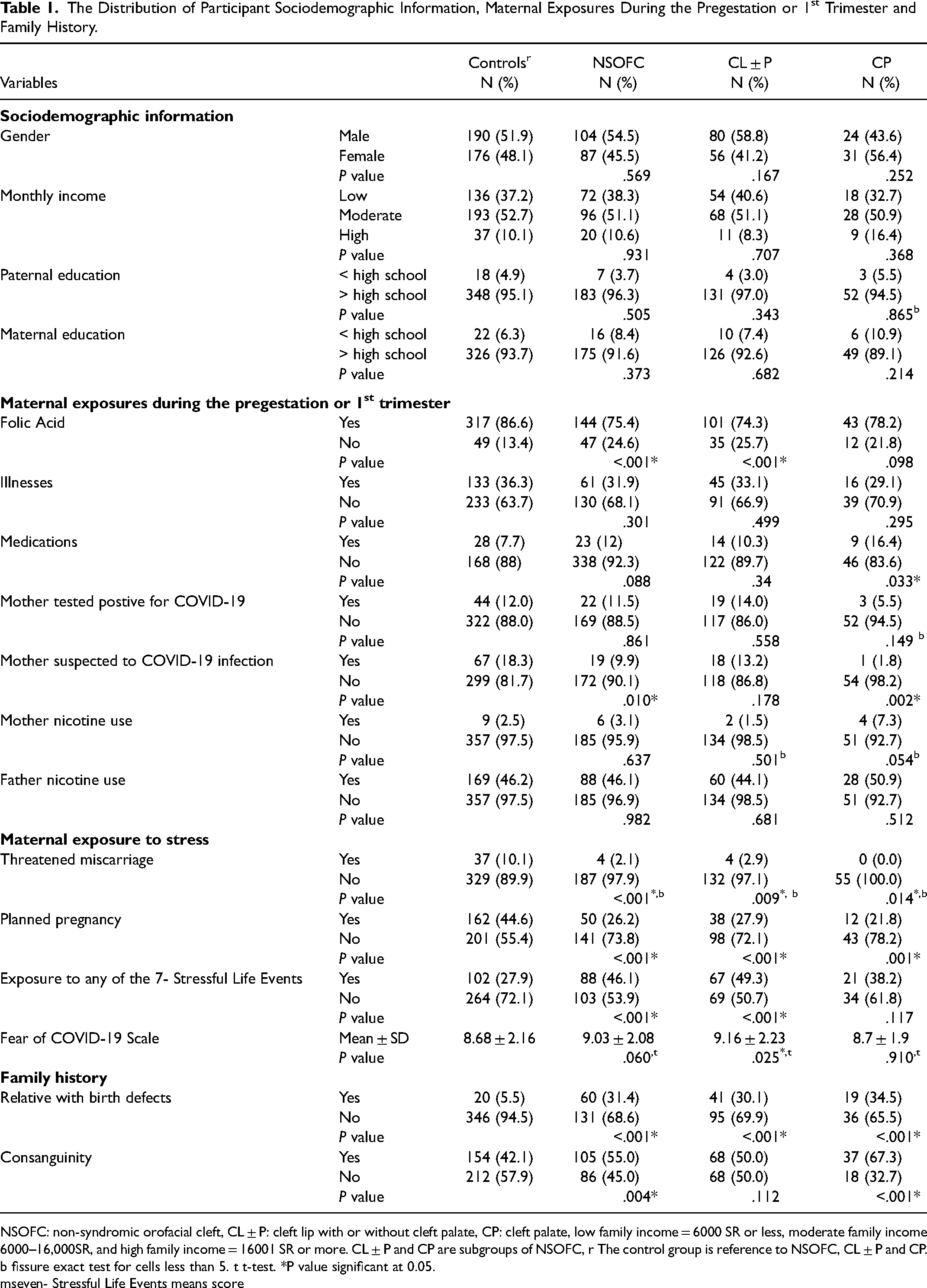
NSOFC: non-syndromic orofacial cleft, CL ± P: cleft lip with or without cleft palate, CP: cleft palate, low family income = 6000 SR or less, moderate family income 6000–16,000SR, and high family income = 16001 SR or more. CL ± P and CP are subgroups of NSOFC, r The control group is reference to NSOFC, CL ± P and CP. b fissure exact test for cells less than 5. t t-test. *P value significant at 0.05.
mseven- Stressful Life Events means score
Although no significant differences were found between the frequency of mothers reporting being infected with COVID-19 among the NSOFC cases and the controls, significantly fewer mothers suspected they were infected with COVID-19 among the NSOFC cases than among the controls (P = .010) (Table 1).
Mothers with NSOFC infants reported maternal exposure to stress, threatened miscarriages, and planned pregnancies significantly less frequently compared with the controls (P < .001). However, maternal exposure to any of the seven listed stress events was significantly higher in NOSFC mothers (P < .001) than in controls. The significant stressful life events that NSOFC mothers reported more compared with the controls were a family under pressure (P = .045), a work state leave or change (P < .001), and a family being robbed (P = .016) (Supplementary Table 3).
Although not significant, the mean total score of the Fear of COVID-19 Scale was higher among mothers of NSOFC patients than the controls (P = .060). The responses to the Fear of COVID-19 Scale items are detailed in Supplementary Table 4. NSOFC infants had significantly more relatives with birth defects and consanguineous parents than the controls (P < .001 and P = .004, respectively) (Table 1).
A binary logistic regression analysis was conducted for NSOFCs and their main phenotypes (CL ± P and CP). Maternal exposures (folic acid supplements, illnesses, a COVID-19 infection, a suspected COVID-19 infection, paternal nicotine use, exposure to any of the stressful life events, the mean score of the total Fear of COVID-19 Scale, pregnancy planning, a threatened miscarriage), a family history of NSOFC relatives, and parental consanguinity deemed independent factors. Maternal exposure to nicotine was excluded from the regression analysis because only six (3.1%) mothers reported smoking. Maternal exposure to medications was removed to avoid collinearity. After the effect of confounders was removed, maternal exposure to any of the seven stressful life events (AOR: 3.78, 95% CI: 1.95 to 7.32; P < .001) and a family history of relatives with NSOFCs (AOR: 9.73, 95% CI: 5.36 to 17.66; P < .001) increased the AOR for NSOFC development, and the parental consanguinity approached significance (AOR: 1.47, 95% CI: 0.99 to 2.20; P = .057). On the other hand, maternal folic acid (AOR: 0.56, 95% CI: 0.36 to 0.87; P = .010), a threatened miscarriage (AOR: 0.17, 95% CI: 0.05 to 0.50; P = .001), the fear of a COVID-19 infection (AOR: 0.83, 95% CI: 0.69 to 0.99; P = .038), and a suspected COVID-19 infection (AOR: 0.43, 95% CI: 0.23 to 0.80 and P = .008) decreased the AOR for NSOFC development (see Table 2).
Binary Logistic Regression Analysis for the Relationship Between NSOFC, CL ± P and CP (Dependent Factors) and Maternal Exposures in Pregestation Period/1st Trimester and Family History (Independent Factors).
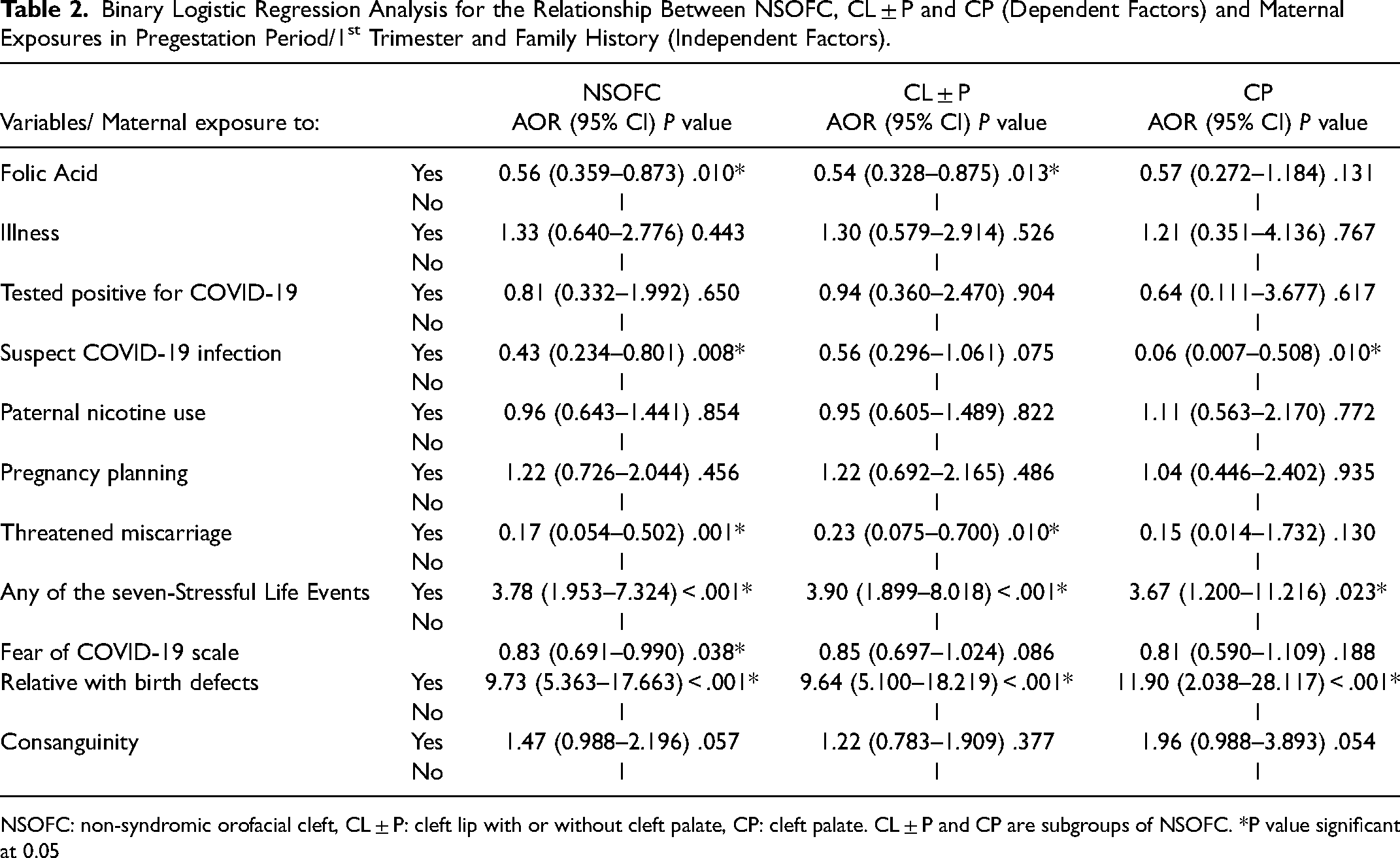
NSOFC: non-syndromic orofacial cleft, CL ± P: cleft lip with or without cleft palate, CP: cleft palate. CL ± P and CP are subgroups of NSOFC. *P value significant at 0.05
Moreover, any of the seven stressful life events (AOR: 3.90, 95% CI: 1.89 to 8.02 and P < .001) and a family history of NSOFCs (AOR: 9.64, 95% CI: 5.10 to 18.22 and P < .001) increased the AOR for CL ± P development (see Table 2). In contrast, folic acid (AOR: 0.54, 95% CI: 0.33 to 0.88 and P = .013) and a threatened miscarriage (AOR 0.23, 95% CI: 0.08 to 0.70 and P = .010) decreased the AOR for CL ± P development. Furthermore, a family history of NSOFCs (AOR: 11.90, 95% CI: 2.04 to 28.12 and P < .001) increased the AOR for CP development, and the parental consanguinity (AOR: 1.96, 95% CI: 0.99 to 3.89; P = .054) approached significance. In contrast, a suspected COVID-19 infection (AOR: 0.06, 95% CI: 0.01 to 0.51 and P = .010) decreased the AOR for CP development.
Discussion
Our data suggest that a SARS-CoV-2 infection is not associated with an increased risk of NSOFCs or any sub-phenotypes. This finding is supported by a previous study that reported no evidence of a large teratogenic effect associated with a maternal SARS-CoV-2 infection during the first months of pregnancy. 30 Although a maternal COVID-19 infection did not show a relationship with NSOFCs, maternal exposure to life events, which were mainly a family being under pressure, a change in working status, and having been robbed, significantly increased the possibility of having a child with an NSOFC. Maternal stress during pregnancy, one of the environmental risk factors for NSOFCs, has not been fully understood. The COVID-19 pandemic has led to stress that affects individuals’ lives and mental health.31,32 Thus, this pandemic presents an opportunity to study stress's effects on NSOFC development. Furthermore, apart from causing an infection and stress, COVID-19 has influenced many other aspects of an individual's life, such as nicotine use16,33 and health care.16,34
In this cohort, exposure to any of the seven stressful life events resulted in a significantly increased odds of NSOFC compared with the controls. A significant relationship was evident when mothers were asked about their families being under pressure or changes in their working statuses. Although these stressors can take place at any time, research has documented the COVID-19 pandemic's negative effects on the economy, job opportunities, and job losses.35–37 Stress's effect on the development of NSOFCs is consistent with that reported in the previous literature. 38
In contrast, the fear of COVID-19, the suspicion of a COVID-19 infection, and a threatened miscarriage showed protective effects in children with NSOFCs. This was counter to the expectation of stressors contributing to NSOFCs and might indicate that mothers who were worried about losing their babies or getting infected with COVID-19 tended to take greater care of their health, which was partially seen in the higher rates of folic acid use as recommended.39–43 This is supported by previous studies that reported maternal supplementation's protective effect and having a child with an NSOFC.3,44 A familial history of birth defects is associated with an increased risk of NSOFCs as reported in previous studies.3,45–48 These findings are consistent with the results of the present study and confirm that genetic diseases affect NSOFCs.
This is an early study investigating the environmental risk factors for NSOFCs while taking into consideration all of the areas and tertiary medical centers of the Kingdom of Saudi Arabia. In addition, because our sample distribution closely resembles Saudi Arabia's population distribution, the results can be generalized to the Saudi population. 49 Furthermore, to assure generalizability, we compared the total number of NSOFCs we encountered, born at or referred to the included centers (177 born + 40 referred = 217 NSOFC), with the total number of births reported by the Saudi Ministry of Health in 2020 (188,773 living births), 50 which yielded a frequency of 1.15 NSOFCs per 1000 living births. This frequency is similar to the global NSOFC prevalence reported in a meta-analysis published in 2022. 51 Adding to the value of this study is the unique ethnic variation in the Saudi population. Although Saudis are generally deemed Caucasian, they comprise a mixed ethnicity resulting from decades of people traveling from all over the world and settling in Mecca and Medina, then mixing in marriage. Additionally, Saudi Arabia has a unique geographic location between the three continents of Asia, Africa, and Europe, which makes it difficult to group people under one ethnic group.52,53
Nevertheless, this study has some limitations. The first is the recall bias associated with case-control studies, which is inevitable in this study design. To limit this type of bias, we interviewed both the patients and the controls as soon as the infant was delivered. Second, reports of family problems, divorce, and certain behaviors, such as smoking, could be subject to bias due to social stigmas.
Conclusion
Our study adds to the existing body of evidence regarding the etiology of NSOFCs. This study confirmed that maternal stress exposure due to cumulative life events is a risk factor for NSOFC development. The fear of and perception of a COVID-19 infection along with the threat of a miscarriage might be related to better self-care during pregnancy among participating mothers, which led to a lower risk of NSOFC occurrence. Nevertheless, a prospective cohort study is key to obtaining more objective findings. Additionally, stress's epigenetic effects should be investigated to fully determine the cause-effect role. Finally, to fully assess stress's role, understanding the disease's genetic background is crucial.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231224198 - Supplemental material for Maternal Exposure to Stress During Covid-19 and Non-Syndromic Orofacial Clefts: A Cohort Retrospective Study
Supplemental material, sj-docx-1-cpc-10.1177_10556656231224198 for Maternal Exposure to Stress During Covid-19 and Non-Syndromic Orofacial Clefts: A Cohort Retrospective Study by Heba Jafar Sabbagh, Mona Talal AlSharif, Fatma Dawood Abdulhameed, Aziza Johar Aljohar, Reema Mahdi Alhussain, Sultan Musaad Alghamdi, Najla Sulaiman Alrejaye, Latifa Yousef AlGudaibi, Bahauddin Ibraheem Sallout, Badi Shoaib Albaqawi, Eman Abdulbaset Alnamnakani, Lougin Khalid Brekeit, Osama Adel Basri, Manal Ibrahim Almalik, Norah Suliman Al Soqih, Ali Bakr Alshaikh, Abdullah Jameel Aburiziza, Faisal Ali Al Qahtani, Bushra Musaad Alghamdi, Asalah Khalid Alraddadi, Hadeel Hamza Khaja and Rana Abdullah Alamoudi in The Cleft Palate Craniofacial Journal
Footnotes
Data Availability
The data used in this study is available upon reasonable request from the corresponding author.
Author Contributions
HJS: Conceptualization, Methodology, Study Design, Data analysis, Writing and editing of final draft; MTA: Conceptualization, Methodology, Study Design, Data analysis, Writing and editing of final draft; FDA, AJA, RMA, SMA, NSA, LYA, BIS, BSA, EAA, LKB, OAB, MIA, NSA, ABA, AJA, FAA, BMA, AKA, HHK: Methodology, Data collection; RAA: Conceptualization, Methodology, Study design, Writing and editing of final draft. All authors read and approved the final draft of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.