
Abstract
Objectives
(1) Assess caregiver-reported development in infants born with cleft lip ± alveolus (CL ± A) and cleft lip and palate (CLP); (2) determine factors associated with increased developmental risk; and (3) determine consistency of developmental risk before and after surgery for cleft lip.
Design
Prospective, longitudinal assessment of development. Time (T) 1, prior to lip closure; T2, 2 months post lip closure.
Setting
Three US craniofacial teams and online parent support groups.
Participants
123 total caregivers (96% mothers); 100 at T1, 92 at T2, and 69 at both T1 and T2.
Measure
Ages and Stages Questionnaire-3 (ASQ-3): Communication, Gross Motor, Fine Motor, Problem Solving, Personal Social Domains.
Results
At T1 47%; at T2 42% passed all 5 Domains; 36% of infants pass all 5 Domains at both T1 and T2. Infants with CLP were at greatest risk on Communication [B = 1.449 (CI = .149-20.079), p = .038; Odds Ratio (OR) = 4.3 (CI = .923-19.650)] and Gross Motor Domains [B = 1.753 (CI = .316-20.605), p = .034; OR = 5.8 (CI = 1.162-28.671)]. Male infants were at greatest risk on Fine Motor [B = 1.542 (CI = .495-20.005), p = .009; OR = 4.7 (CI = 1.278-17.101)] and Problem Solving Domains [B = 1.200 (CI = .118-19.708), p = .044; OR = 3.3 (CI = .896-12.285)].
Conclusions
Based on caregiver report, infants with CL ± A and CLP meet referral criteria at a high rate. Infants with CLP and male infants were at greatest risk. Regular developmental screening is recommended.
Introduction
Infancy is a time of rapid physical and cognitive development. Within the first month of life, infants typically learn to feed from a bottle or breast, sustain their focus on objects and recognize the voices of familiar caregivers. By three months of age, infants typically hold their heads up firmly, bring their hands to their mouths as well as demonstrate cooing and social smiles. Six-month milestones are characterized by rolling in both directions, learning to sit, using hands and mouths to explore the environment, communicating with different sounds, giggles, facial expressions, playing games such as peek-a-boo and recognizing their own name. As infants develop into toddlers at one year, they demonstrate an expanding vocabulary of simple words such as “mama,” “dada” or “uh-oh” and simple gestures such as clapping or waving. Many children start to walk by holding on to furniture and move towards independent walking. 1
Caregivers, pediatricians and other providers monitor the rate at which developmental milestones are achieved; this can vary widely, even among typically developing infants. However, the attainment of developmental achievements among children with medical conditions may be compromised due to their health status and related treatment. For children born with a cleft lip with or without cleft palate (CL ± P) developmental progress may be compromised due to speech and language delay or hearing concerns. Additionally, caregivers are often faced with challenges related to feeding, managing daily use of presurgical interventions such as taping or a nasoalveolar molding device, interruptions to daily routines as a result of frequent doctors’ appointments, surgeries, and post-surgery restrictions such as arm restraints. These interventions can impact the relationship between caregivers and their infant and may also affect infant development. 2
The Bayley Scales of Infant (and Toddler) Development (BSID) 3 has most often been used in research to investigate the development of infants with cleft lip and/or palate (CL/P).2,4–9 While these studies found little evidence of significant delays in the first year of life, there are documented declines in scores on the BSID when children were assessed after 12 months. Some authors postulated correlates of the decline in scores with history of middle ear problems 5 or quality of maternal interaction.2,7 Kapp-Simon & Krueckeberg 6 reported that poorly developed fine motor skills during the first year of life were associated with lower scores on the mental development scale of the BSID at age two. Additionally, sleep disordered breathing, with poor sleep quality, during the first year of life has been associated with diminished cognitive outcomes as measured by the BSID at age three. 9
Not only do treatments and complications related to a diagnosis of cleft have the potential to affect achievement of milestones, research suggests caregiver sensitivity to an infant's needs or their interactions with their child can influence later development.2,8,10 Murray and colleagues reported that timing of lip repair and early mother-infant interactions mediated cognitive development at 18 months and 7 years of age.2,10 Similarly, Collett, Leroux, & Speltz reported that a combination of maternal sensitivity during infant feeding, BSID cognitive scores at 24 months of age, and demographic variables were predictive of both language and reading scores at age 7 years. 8
The impact of early medical care on child development can have repercussions as children grow and enter school. Children born with CL/P can be at increased risk for learning challenges. 11 Interruptions in achievement may occur due to underlying changes in brain structure12,13 or to the effects of social-emotional and environmental challenges, such as caregiver stress and disruption from required medical interventions.14–16 For these reasons, it is important that providers and caregivers track how the infant or toddler, who has a diagnosis of CL/P, achieves milestones in order to identify developmental delays and implement remediation as soon as possible to improve outcomes as children transition into school.
Direct assessment with an instrument such as the BSID is the gold standard for assessing infant development; however, there are challenges. Direct assessment can be time consuming, especially within the context of a cleft team visit. Infants may be irritable or tired at time of assessment, decreasing reliability of the results; they may also be hesitant to interact with an unfamiliar adult and the cleft team visit may not allow sufficient time to allow the infant to become comfortable. While there is an opportunity for direct observation, examiners may only capture one snapshot of development and infants may not demonstrate newly emerging skills during the time of the assessment. In order to address these shortcomings, providers have looked to caregiver-report instruments as an alternate method of assessing development.
There are a number of caregiver report instruments in the literature intended to provide standardized assessment of early child development; however, to our knowledge, there are few studies that used caregiver input to measure development of infants with CL/P.15,17,18 Neiman and Savage17,18 reported cross sectional data on infants 5-36 months of age and found that 30 to 48% of 5-month-old infants, depending on cleft type and scale, scored in the at risk range in motor development, cognitive development, self-help, and global scores. While scores for the other children were generally in the expected range, the mean score on the expressive language scale for the three-year olds was in the at-risk/delayed range with children who had cleft palate only (CP) having the lowest scores.
Recently, Costa et al. 15 reported on the usefulness of the Ages and Stages Questionnaire-3 (ASQ-3) for 18-month-old toddlers diagnosed with CL/P who resided in the UK. The ASQ-3 is a parent-report screening measure used to assess infant and toddler development across multiple domains: Communication, Gross Motor, Fine Motor, Problem Solving, and Personal-Social. The instrument provides three different types of cutoff points: pass, monitor, and refer. While overall, the sample reportedly exhibited typical development, the authors reported that just over 31% of the 322 toddlers received a score in the referral range on at least one of the domains. This includes 17.7% of toddlers falling in the referral range on one domain, 7.8% of toddlers falling in the referral range on two domains, 3.4% falling in the referral range on three domains and 2.2% falling in the referral range on four or more domains. With regards to specific scales, the Communication Domain received the highest percent of toddlers in the monitor range (46.3%), followed by Problem Solving (14%). An additional 15.5% fell in the referral range on the Problem Solving Domain followed by 9.3% on the Communication Domain. The authors concluded that the ASQ-3 is a useful tool to help caregivers and providers identify children in need of additional evaluation to implement intervention services when appropriate.
The ASQ-3 or earlier versions have been utilized in research in diverse populations. Researchers have found the ASQ to be a reliable and valid tool for identifying areas of developmental concern in infants and children across the globe,17,19–21 Similarly, the ASQ has been used to reliably identify risk in infants/toddlers with chronic illnesses including sickle cell disease, 22 congenital heart disease,23–25 and infant cancer 26 ; infants with low birth weight27–29 and Autism Spectrum Disorder.30,31 The ASQ-3 has also been used successfully to monitor development in clinical practice,22,32–34 though sensitivity to delay 34 and agreement with gold standard assessments such as the BSID were not always high. 35 ACPA parameters of care require ongoing monitoring of infant and child development to facilitate early referral to appropriate intervention programs as needed.36,37 The ASQ-3 may be an efficient tool that enables regular screening of developmental progress in the context of a cleft team visit; however, currently there is no information on how caregivers rate infants with CL ± P on the ASQ-3. Additionally, while there is some evidence in the literature that developmental risk increases across time for children with CL/P, there is no information on how children with CL/P perform across time on the ASQ-3.
The purpose of the current study was to (1) assess caregiver-reported development in infants born with cleft lip, with or without cleft palate (CL ± CP); (2) determine factors associated with increased developmental risk; and (3) determine consistency of developmental risk across two time points, before and after surgery for cleft lip.
Methods
Human Subjects Protection
All study procedures adhered to ethical standards of practice and were approved by each site's local Institutional Review Board.
Participants
Participants in the current study were caregivers of infants born with cleft lip, with or without cleft palate (CL ± CP). Caregivers completed the ASQ-3 as part of a larger study to develop a measure of health and well-being for children born with CL ± CP.38–40 The infant had to be under one year of age and have an unrepaired cleft lip with or without cleft palate at time of enrollment. They also had to be free of other major medical conditions that might significantly affect their health and well-being (eg, congenital heart defects, illnesses requiring prolonged hospitalization). Infants born prematurely were eligible to be included in this study. Gestation-adjusted ages were used for test administration as research has shown that evaluation of infants born prematurely with the ASQ-3 is valid when ages adjusted for prematurity are used. 27 Participants were recruited from three US based cleft-craniofacial teams and online parent support groups (ACPA, social media) with baseline data collected between Oct of 2017 and Feb of 2020. In order to participate in the study, caregivers had to speak either English or Spanish and be able to provide informed consent.
Measure
The Ages and Stages Questionnaire-3 (ASQ-3)
The ASQ-3 is a reliable and well-validated 30 item parent-report measure used to screen infant development across five domains: Communication (COM: listening, speaking, comprehension), Gross Motor (GM: sitting, walking), Fine Motor (FM: hand, finger skills), Problem Solving (PROBS: interaction with toys and learning), and Personal-Social (PERS: social interaction). 41 Each domain includes 6 items scored as ‘not yet’ (0), ‘sometimes’ (5) or ‘yes’ (10). Questionnaires are available for children ranging in age from 1 to 66 months. Total ASQ-3 scores range from 0 to 60 for each domain. Scores are classified as “pass” (above the cutoff), “at risk” or “monitor” (between 1 SD and 2 SDs below standardization mean) and “below cutoff” or refer (≥ 2SD below standardization mean). Cutoff scores vary by age and standardized scores are not available for this instrument. Test authors recommend that children who score “below the cutoff” should be referred for further assessment while children in the “at risk” range should receive close monitoring.
The ASQ-3 has demonstrated strong psychometric properties. Test-retest reliability was high with interclass correlations ranging from .75 to .82. Additionally, San Antonio et al. 42 explored the use of the ASQ under standardized versus nonstandardized conditions (pediatrician's waiting room) and concluded that it is a reliable measure to identify developmental concerns among both English and Spanish speaking families regardless of the conditions in which it was administered to the caregivers of young children. Concurrent validity was established as moderate to high on a subset of the standardization sample, comparing ASQ-3 classification scores with standardized measures. Classification agreement between a parent and trained observer was 93% while interclass correlations by domain ranged from .43 to .69. Chronbach Alphas ranged from .51 to .87 indicating moderate to strong internal consistency. Subsequent publications have resulted in sensitivity ranges from 66%-82% and specificity ranges from 78-86% when examining classification of developmental delay.33,43,44
Procedure
A primary caregiver (generally the mother) completed the ASQ-3 in their own home, either via paper-pencil (76%) or online (24%) at baseline and two months after surgery for lip closure. Paper-pencil ASQ-3 forms were returned by mail and entered into the database by the site research coordinator. Information on risk factors were obtained through interview and included: diagnosis, prematurity, birth weight, race/ethnicity, family socio-economic status (SES), medical treatments, and family history.
Risk variables were calculated for medical risk and SES. Since children with significant health conditions defects other than CL/P were excluded from participation, two conditions were considered for medical risk: 1) prematurity (0 = low risk, < 21 days premature; 1 = some risk, 22-42 days premature; 2 = high risk >42 days premature) and 2) birth weight (0 = low risk >2.8 kg; 2.3 to 2.8, 1 = some risk; 2 = high risk <2.3 kg,). 45 The two risks were combined and the Medical Risk Score was calculated as: 0-1 = low risk; 2-4 = moderate to high risk.
A SES risk score was calculated based on caregiver education and family income: four categories were created based on family income and caregiver education: 1 = < College Degree and Income < $ 35 000; 2 = Some College and Income between $ 35 000 and $ 74 999; 3 = Some College and Income between $ 75 000 and $ 114 999; 4 = minimum of Bachelor Degree and Income > $ 115 000).46–48
Data Analysis Plan
Statistical analysis was completed using SPSS 28.0. 49 Descriptive statistics (N's, means, standard deviations, and percentages) were used to identify sample characteristics and ASQ-3 subscale scores for the 192 administrations of the ASQ-3, which includes 69 subjects with two administrations approximately three months apart. ASQ-3 scores were summarized in three categories: pass, at-risk (monitor), or below the cutoff (refer). Cumulative risk was calculated for all T1 subjects and all T2 subjects as total number of referrals at each time point. For subjects with both T1 and T2 data, cumulative risk was also calculated as the higher number of referrals for either administration.
The number of points needed for each domain category differs by age and standardized scores are not available on the ASQ-3. Therefore, nonparametric analysis was needed to compare groups. Using the first administration for each subject (N = 123) to avoid duplicate subjects, chi-square (X2) analysis was used to compare infants within the refer group (ie, > 2 standard deviations below the mean) to infants who scored within the monitor or pass range in each domain of the ASQ-3 by cleft type [cleft lip ± alveolus (CL ± A) and cleft lip and cleft palate (CLP)], medical risk (high, low based on prematurity and birth weight category), child sex, child age group [we used ≤5.5 months and >5.5 months to divide the subject cohort approximately in half since some research suggests greater risk for older subjects 22 ] race (white, nonwhite), marital status (married/partnered or single/divorced/widowed), and SES risk (four categories based on family income and caregiver education). Significant variables were retained for logistic regressions with bootstrapping using 1000 samples, to examine predictors for each domain. Two additional logistic regressions with bootstrapping were used to determine predictors of subjects who met criterion for referral in: 1) one or more domains and 2) in two or more domains.
Results
One hundred-twenty-three caregivers (96% mothers) completed the ASQ-3 with 69 of those caregivers providing reports at two time points for a total of 192 reports. Most caregivers (88%) reported they were married or residing in the same household with a committed partner. Six percent of caregivers had less than a high school education and 22% had a household income under $ 35 000. Mean infant age at T1 assessment was 4.9 months (SD = 1.8, range 1 to 11 months). Mean age at T2 assessment was 8.4 months (SD = 1.8, range 4.7 to 14.3 months). For the 69 infants with two assessments, T1 mean age was 5.3 months (SD = 1.6) and T2 mean age was 8.3 months (SD = 1.7). Most infants were diagnosed with CLP (72.4%) and were male (65.9%). Most infants were White (67.5%) with 17% identified as Hispanic/Latinx. Twenty-seven percent of infants met criteria for higher SES risk which is generally consistent with U.S. statistics 50 ,51 and 8.9% of the infants were considered at medical risk due to the combination of low birth weight and prematurity, which is lower than U.S. rates 52 which suggest an approximate 10.5% risk for prematurity (Table 1).
Infant and Primary Caregiver Characteristics by Assessment Time.
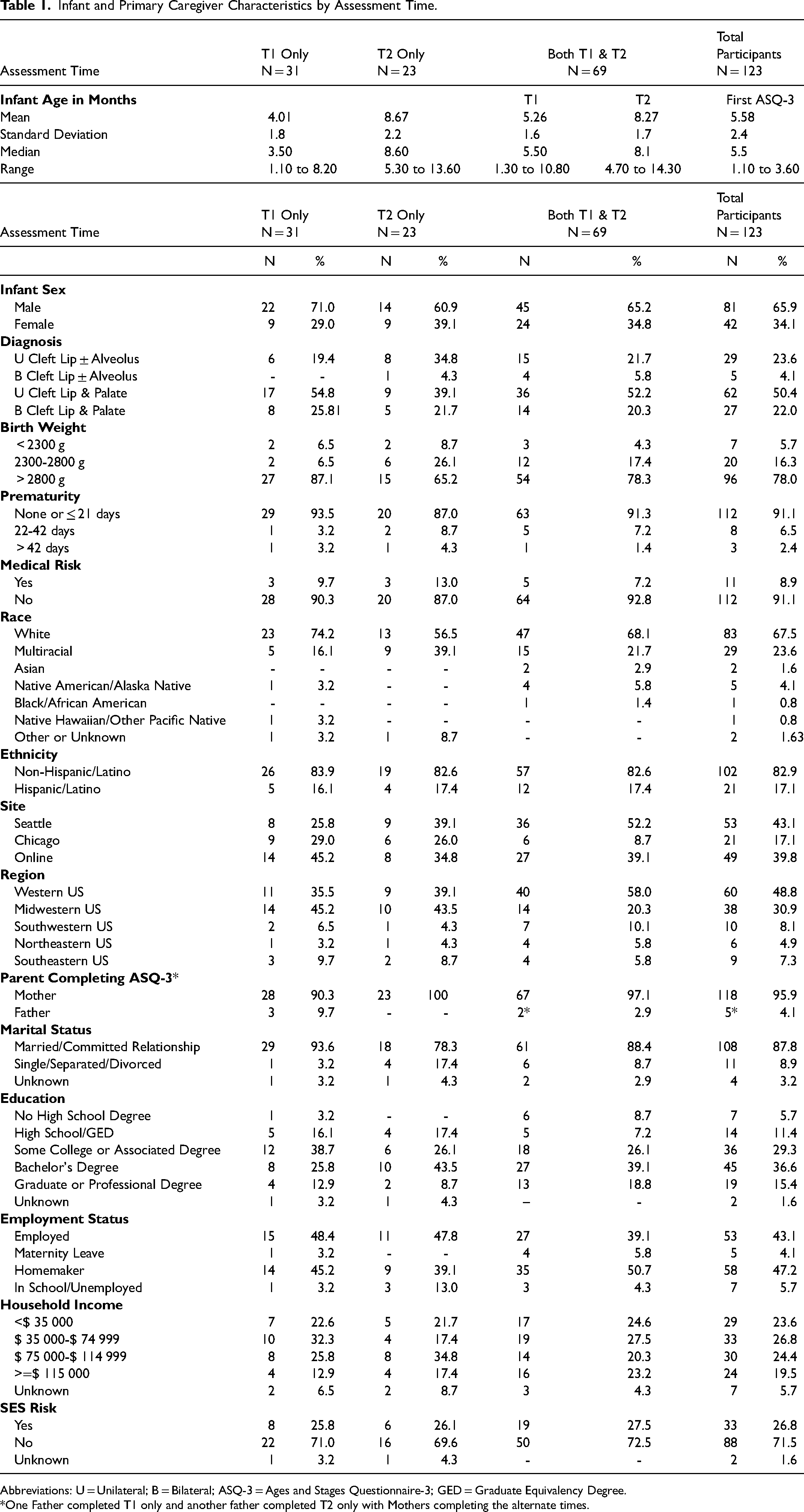
Abbreviations: U = Unilateral; B = Bilateral; ASQ-3 = Ages and Stages Questionnaire-3; GED = Graduate Equivalency Degree.
*One Father completed T1 only and another father completed T2 only with Mothers completing the alternate times.
ASQ-3 Scores
Table 2 presents cross sectional data for ASQ-3 raw scores and classifications (pass, monitor, refer) by test age for all forms completed (N = 192 forms). Overall, 70% of the completed ASQ-3's resulted in a passing score on the Problem Solving Domains, 69% were scored as passing on the Gross Motor Domain, 65% were scored as passing in the Communication Domain, 63% passed on the Personal Social Domain, and 60% passed on the Communication and Fine Motor Domains. Pass rates by age range from a low of 22% on the Communication Domain at 9-10 months of age and a high of 94% on the Gross Motor Domain at 2 months. Overall, the percentage of reports that met criterion for referral (≥2 SD below mean) in each domain were as follows: Communication, 16%; Gross Motor, 15%; Fine Motor, 20%; Problem Solving, 13.5%; and Personal Social, 17%. Finally, of the infants who scored within the monitor range 25% were on the Communication, 21% on Fine Motor, 20% the Personal Social, 16% on Gross Motor, and 16% on Problem Solving Domain.
Summary of Cross Sectional ASQ-3 Scores and Classifications Across Ages.
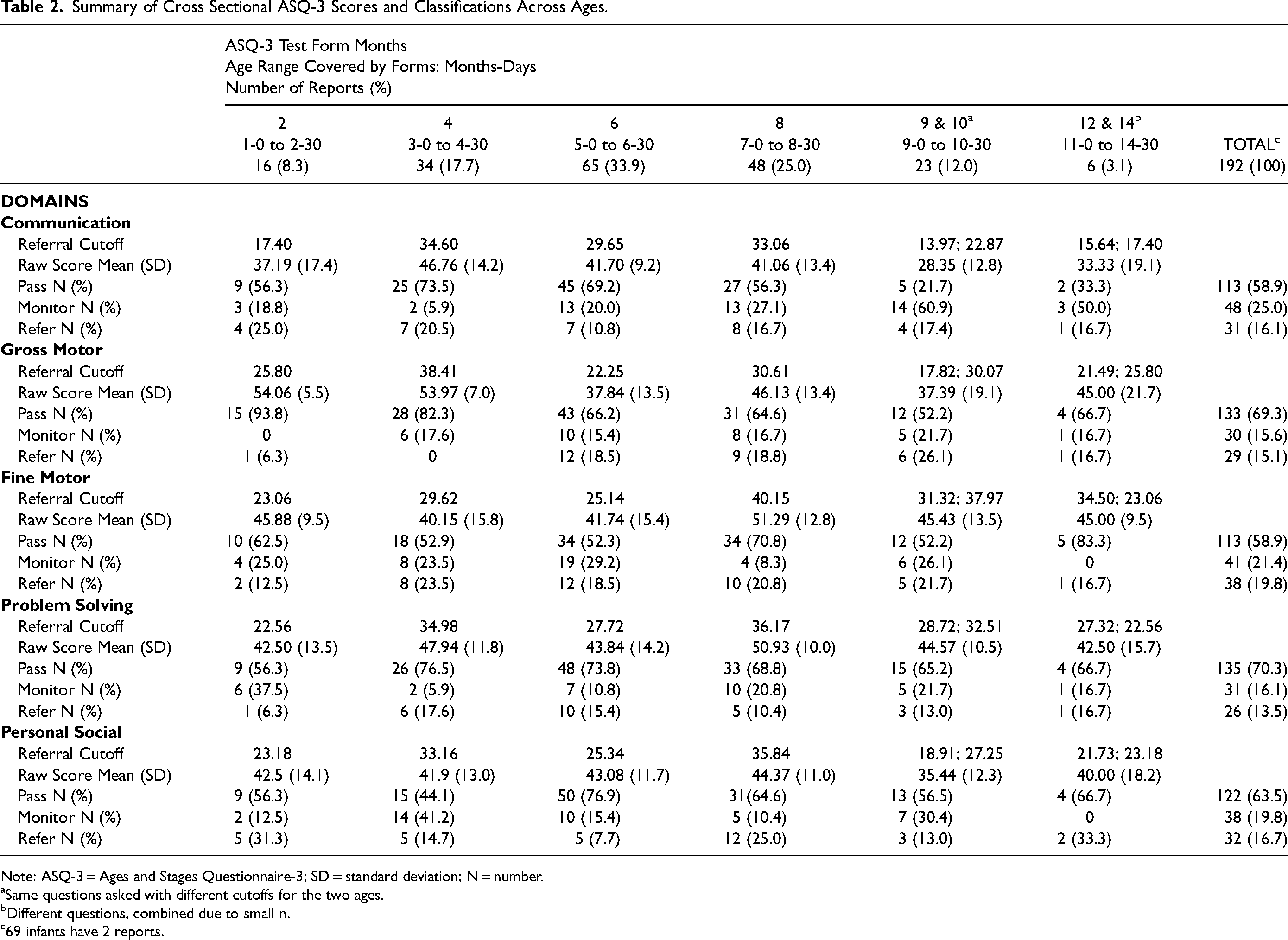
Note: ASQ-3 = Ages and Stages Questionnaire-3; SD = standard deviation; N = number.
aSame questions asked with different cutoffs for the two ages.
bDifferent questions, combined due to small n.
c69 infants have 2 reports.
Table 3 presents the cumulative number of ASQ-3 administrations that met criteria for referral classification across domains by age for all 192 reports. Slightly more than half of the reports resulted in no referrals (57%). Twenty-four percent of the reports resulted in one referral while 19% of the reports resulted in two or more referrals. Infants were least likely to receive a referral when caregivers completed the 6-month ASQ-3 form.
Cumulative Referrals by Age.
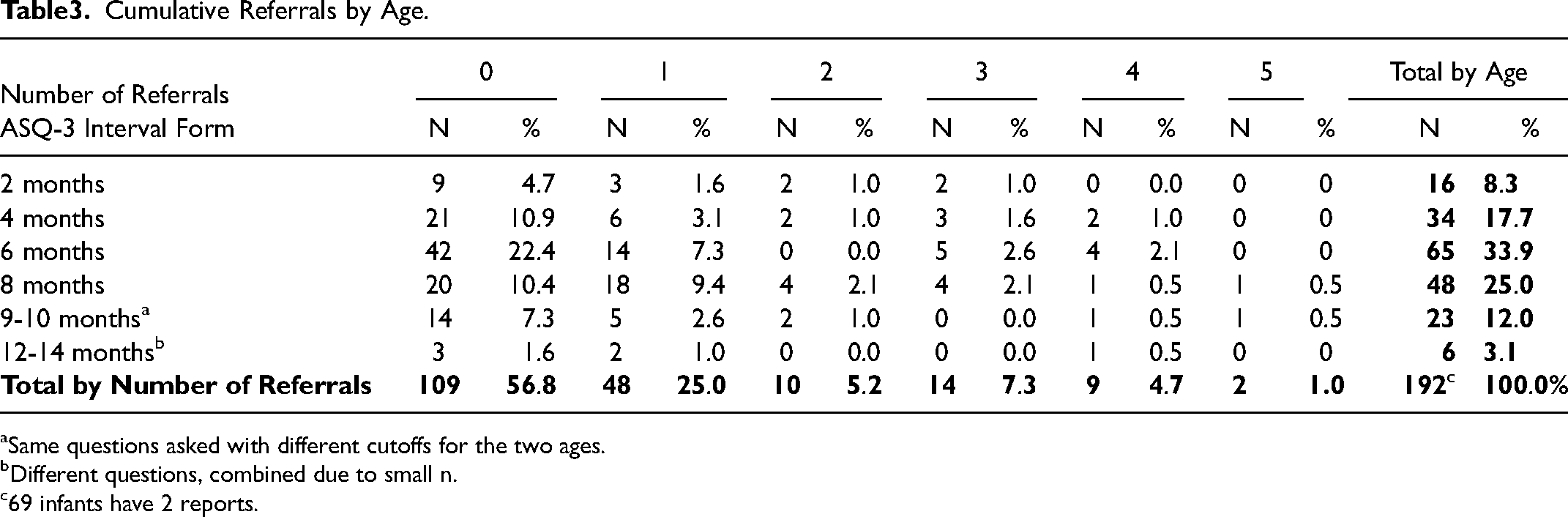
aSame questions asked with different cutoffs for the two ages.
bDifferent questions, combined due to small n.
c69 infants have 2 reports.
Prior to surgery (T1) 47% of the infants did not receive a referral on the ASQ-3 (Table 4). Post surgery, the percent without a referral was 42%. However, when two reports were available (N = 69), 36% of the infants did not receive a referral at either time point, 38% received at least one referral at one of the two time points, and 26% received two or more referrals at one of the two time points.
Cumulative Referrals Across ASQ-3 Domains for All Infants who Have Reports at T1 or T2 and Higher Referral Rate for Those with Reports at Both T1 and T2.
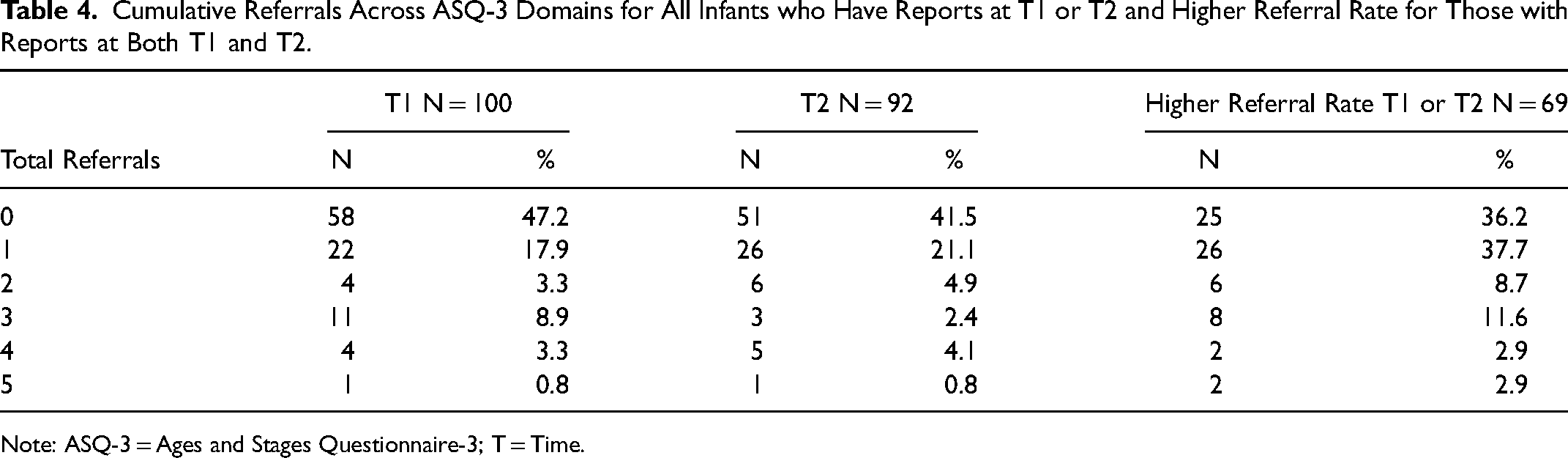
Note: ASQ-3 = Ages and Stages Questionnaire-3; T = Time.
ASQ-3 Consistency Between T1 and T2
Table 5 shows the Pass, Monitor, and Refer rates by domain for T1 and T2 for the 69 infants with two reports. Consistent pass rate was lowest for the Fine Motor Domain (25/69, 36%) and highest for the Gross Motor and Problem Solving Domains (39/69, 56.5% for each). For the Communication Domain, 27 of the 49 infants (55%) who passed at T1 also passed at T2. For Problem solving the rate was 31/69 (45%). Figure 1 provides a visual schema of change from T1 to T2.
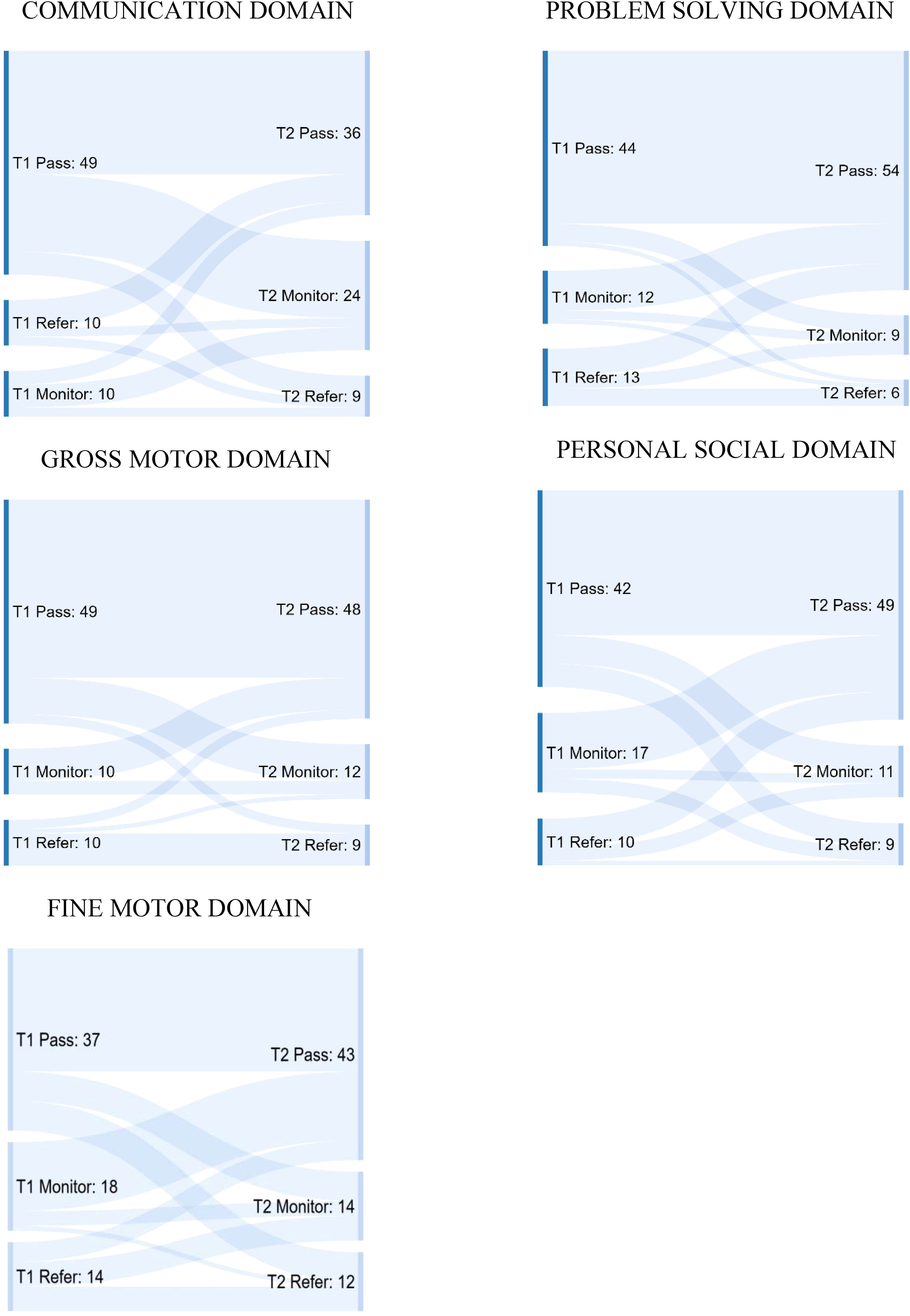
Ages and Stages-3: Domain Classification Changes Between T1 and T2.
Crosstabs of ASQ-3 Categories at T1 and T2.
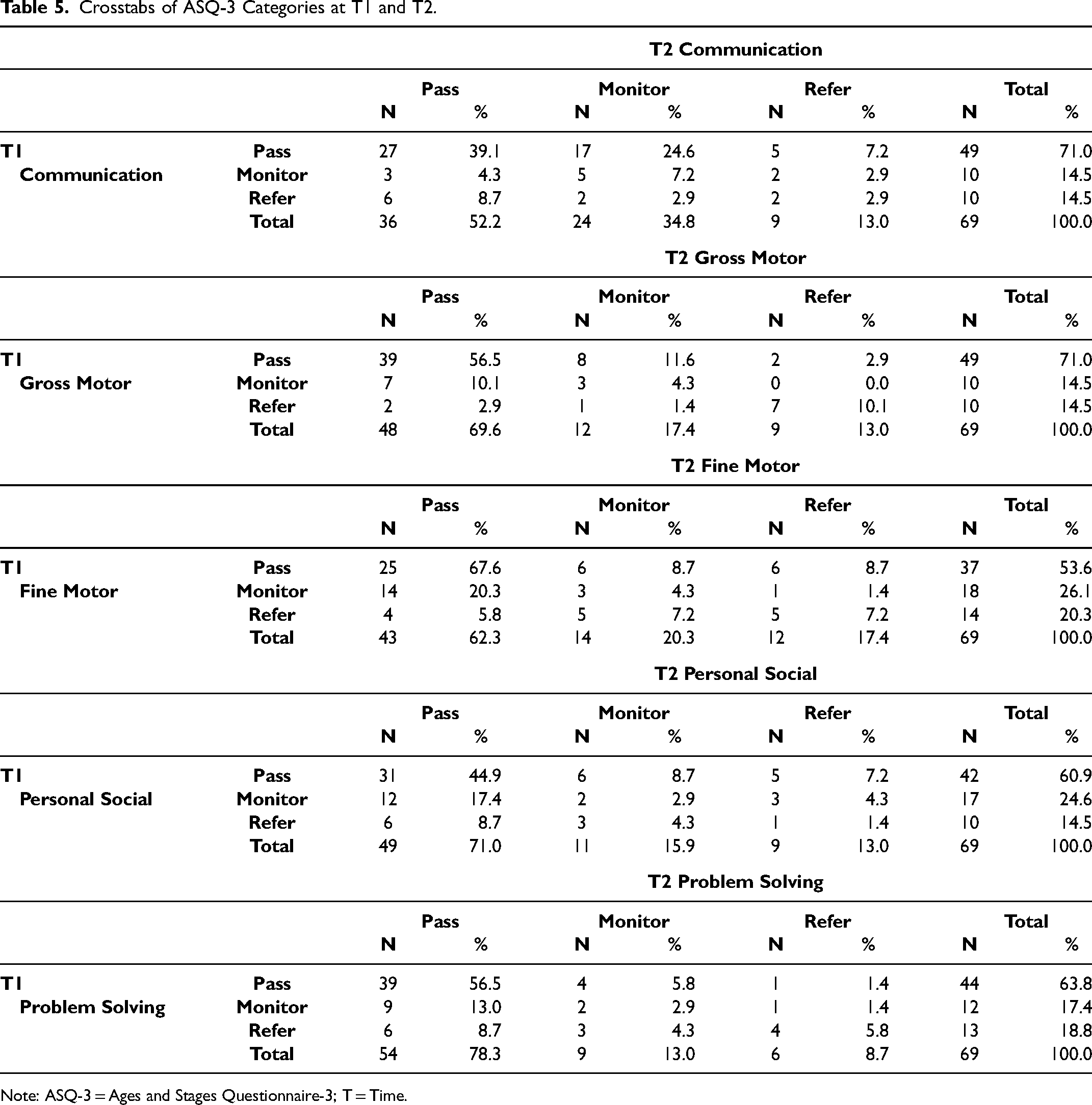
Note: ASQ-3 = Ages and Stages Questionnaire-3; T = Time.
Variables Associated with Domain Risk
SES, and ASQ-3 Domain Scores. There were no significant associations of SES and domain risks based on the four categories of risk (See Supplemental Table 1). Children who were referred were as likely to reside in families with higher SES as in families with lower SES.
Medical Risk, Race, Marital Status. Infants at higher medical risk due to prematurity and low birth weight were not more likely to meet criterion for referral on any of the domains than infants who were not categorized as high medical risk. Similarly, race and marital status were not associated with higher referral rates on any of the ASQ-3 domains.
Diagnosis and ASQ-3 Domain Scores. Chi-square analyses revealed that the infants with CLP were significantly more likely to meet referral criterion on the Communication Domain, X2 (1) = 4.610, p = .032), and Fine Motor Domain, X2 (1) = 3.838, p = .050), with a trend on the Gross Motor Domain, X2 (1) = 3.717, p = .054, than infants with CL. While significant differences were not detected between infants diagnosed with CL ± A versus CLP on the remaining two domains, more infants diagnosed with CLP met criteria for referral on the Problem Solving (17/20) and Personal Social Domains (20/24) than infants with CL.
Sex and ASQ-3 Domain Scores, Males were referred at a significantly higher rate than females on the Fine Motor Domain (22/25), X2 (1) = 6.844, p = .009, and the Problem Solving Domain (17/20), X2 (1) = 3.894, p = .048. Although not statistically significant, male infants also were found to score in the referral range more frequently than females on the Communication Domain (17/22) and the Personal Social Domain (15/24). Risk was more evenly distributed by sex on the Gross Motor Domain (12 of 20 in refer group were males)
Age and ASQ-3 Domain Scores. Infants older than 5.5 months were more likely to meet the criterion for referral on the Gross Motor domain than infants under 5.5 months of age, X2 (1) = 7.485, p = .006. Infant age was not significantly associated with any other domain.
Logistic Regressions
Infant age group, sex, and diagnosis were significantly associated with one or more of the domain scores and were retained for analysis within the logistic regressions. All Beta's are based on 1000 bootstrap samples.
Communication Domain. Infants with CLP were more likely to meet referral criterion on the Communication Domain than infants with CL ± A only [B = 1.449 (CI = .149-20.079), p = .038; Odds Ratio = 4.3 (CI = .923-19.650)]. Infant sex and age group were not significant contributors.
Gross Motor Domain. Infants with CLP [B = 1.753 (CI = .316-20.605), p = .034; Odds Ratio = 5.8 (CI = 1.162-28.671)] and infants over the age of 5.5 months [B = 1.706 (CI = .636-19.216), p = .003; Odds Ratio = 5.5 (CI = 1.651-18.351)] were more likely to meet referral criterion on the Gross Motor Domain. Infant sex was not a significant contributor.
Fine Motor and Problem Solving Domains. Male infants were more likely to meet referral criteria on the Fine Motor Domain [B = 1.542 (CI = .495-20.005), p = .009; Odds Ratio = 4.7 (CI = 1.278-17.101)], and the Problem Solving Domain [B = 1.200 (CI = .118-19.708), p = .044; Odds Ratio = 3.3 (CI = .896-12.285)]. Cleft diagnosis and age were not significant contributors.
Personal Social and Referral on One or More Domains. There were no significant associations of age, sex, or diagnosis with infant referral on the Personal Social Domain or referral on one or more domain scores.
Referral on Two or More Domains. Children with CLP were more likely to meet referral criteria on two or more domains than infants with CL ± A, [B = 1.804 (CI = .625-20.464), p = .010; Odds Ratio = 6.1 (CI = 1.338-20.464)]. Age and sex were not significant contributors.
Discussion
The primary purpose of this investigation was to determine the utility of the ASQ-3 in identifying infants with CL ± CP at risk for developmental delay. The achievement of developmental milestones generally follows a predicted timeline for infants, though some variability is expected. Caregivers and medical providers typically monitor the attainment of developmental milestones; however, tracking is often informal and as a result, infants that could benefit from specific interventions might be overlooked. 44 Identification of infants with CL ± CP who are at risk is critical because early developmental risk can be associated with later disruptions in learning and early intervention services can mitigate some of these risks.2,6,8,10
Caregivers completed a total of 192 ASQ-3 evaluations for this study. While 57% of those reports did not result in a referral, 43% of the reports resulted in a referral in at least one domain. For the infants whose caregiver completed two ASQ-3 reports, 64% (44/69) received at least one referral at either the first or second assessment. Referrals in the current study occurred in each of the domains and across all ages assessed. Based on all of the ASQ-3's administered (n = 192), referrals were highest for the Fine Motor and Personal Social domains (20%) although the other three domains were not much lower ranging from 14% for Problem Solving to 16% for Communication. These referral rates are higher than those reported by Costa et al., 15 for 18-month-old toddlers which were below 10% for Fine Motor, Personal Social, and Communication. The highest referral rate in the Costa et al. study was due to difficulty in the Problem-Solving domain at 16%, which is consistent with the rate for the younger children in the current study. The reasons for the slightly lower rates of referral for the older infants is unclear since we don’t have longitudinal data in the Costa et al. study; however, it is possible that the toddlers in the Costa et al. received early intervention services at a younger age. Researchers estimate that as many as 15% of children in the United States experience a delay in at least one area of development. 53 The rate is much higher for the younger children in this sample. More extensive, individualized assessment is needed to determine which of these children is actually in need of more intensive treatment, such as early intervention services; however, the concerns raised by the parent-reported evaluation should not be ignored.
It is striking that these infants, all of whom were under 15 months of age and most of whom were under a year of age, were more likely to fall in the ‘refer’ range for fine motor and personal social concerns than communication. It is possible that the early delays in fine motor skills are a precursor of later speech and language and cognitive delays. There is some precedence for this hypothesis. In their review, Gonzalez et al. 54 found some support for a relationship between fine motor skills in infancy and later language development. Other studies of the general population have shown that deficits in manual dexterity are related to speech impairments.55–57 The relationship between articulation and fine motor skills is not surprising, given speech production is also a very complex task that requires significant oral motor coordination.
Previous research on children with CL/P has documented poorer non-verbal development including motor skills, especially at younger ages. As noted previously, Neiman and Savage 18 identified lower motor and self-help skills in 5-month-old infants. Compared to normative data, 13-month-old infants also demonstrated poorer motor development. Kapp-Simon and Krueckeberg 6 found that eye-hand coordination and manipulative skills of children with CL/P, 8-15 months of age, were associated with cognitive development at two years of age. Speltz et al. 7 found that at 12 months of age infants with CL/P scored significantly poorer than control infants on nonverbal items of the Bayley than the verbal items. In the current study, the Fine Motor pass rate was 59% with 21% of the children falling into the monitor range and 20% in the refer range with only the oldest group (11-0 to 14-30 months) having no reported risk. The Communication pass rate ranged from 56% to 69% prior to 9 months but fell to 22% at the 9-10-month evaluation. The majority of the children fell into the monitor (61%) rather than refer (17%) category at that stage, but this increased monitor rate may be indicative of later problems with communication. Longer follow-up would be needed to determine if the early risks for fine motor difficulties in children with CL/P identified by the ASQ-3 are associated with later concerns for communication and cognitive functioning.
In an effort to determine which characteristics would better identify infants who meet referral criteria, we examined outcomes by cleft type, infant sex, prematurity, race, SES, and parental marital status. Surprisingly, prematurity, low birth weight, SES, and ethnicity were not significantly associated with developmental outcomes. It is possible that infants at risk due to prematurity or low birth weight in addition to CL ± P are more closely monitored by caregivers and providers, with implementation of remediation services at an earlier age. However, information about participation in early intervention was not available for this study so we cannot confirm this hypothesis.
Depending on the ASQ-3 domain assessed, males regardless of diagnosis, infants with a diagnosis of CLP, and infants with CL ± P over 5.5 months of age were more likely to meet criterion for referral. Caregivers reported increased risk for male infants compared to female infants across most domains, achieving statistical significance in the area of Fine Motor skills with a trend observed on the Problem Solving Domain of the ASQ-3. These results are consistent with what is known about sex differences and developmental risk in children without a medical condition. Research supports differences in developmental trajectories for boys and girls, which slightly favor the girls during the earliest years.56,57 However, variations may differ by domain, with girls showing stronger language and fine motor development and boys having a visual-spatial advantage. 58 Other research specifically on motor development suggests that the caregivers of boys tend to focus more on gross motor development while girls’ caregivers demonstrate a tendency to encourage skills that fall under the fine motor domain. 59
Consistent with several investigations in the limited infant literature,4,6 as well as research examining older children (see Richman et al. 11 for a review) infants with CL ± A were less likely to meet referral criterion on any of the individual domains as well as on two or more domains of the ASQ-3 compared to infants with CLP. In the current study, infants with CLP showed the greatest vulnerability on the Communication and Gross Motor domains. The Cleft Collective Study, which evaluated 18-month-old children with CL/P, also found that the toddlers with CL ± A were at the lowest risk for referral, with children with CLP falling between children with CL ± A and cleft palate only (CP). 15
Infants with CLP were significantly more likely to meet referral criterion on the Communication, Fine Motor, and the Gross Motor domains and were more likely to meet referral criterion on two or more domains. Speech and language delays do occur more frequently in children who have a cleft palate in addition to cleft lip. As noted above, motor delay has been shown to be associated with speech articulation, language, and cognitive development in children both with and without CL/P.6,17,18,60 Due to the nature of the longitudinal study during which the current ASQ-3 data was collected (validation of the iCOO pre-post cleft lip surgery), children with isolated cleft palate were excluded, so we do not have information on how young infants with isolated CP perform on the ASQ-3.
Infant Age was only associated with increased risk on the Gross Motor domain. Only 1 of the 29 infants who met criterion for referral was under 6 months of age. Older infants are expected to master important motor milestones such as rolling in both directions, sitting up, crawling and independent walking. Caregivers are typically very focused on these skills and may be more sensitive to delays. However, there is some support in the literature for increased motor delays with increasing age for children with CL/P. Three studies using the BSID reported lower scores on the motor scale for infants over 12 months of age relative to either standardized data or controls.4,5,7
The ASQ-3 has been used to assess risk for infants/children with other medical conditions.22–26 We used the more stringent criteria of ‘below the cutoff’ or ‘refer’ (≥ 2 SD below the mean) for our analyses; however, studies investigating risk in children with medical conditions frequently combine the ‘monitor’ and ‘refer’ categories to define their referral population (ie, children who score 1 standard deviation below the mean). A recent study investigating risk for infants/toddlers with sickle cell disease, at a median age of 8.7 months (range 3.7 to 50.1), reported that from 4 to 10%, depending on domains, fell in the monitor or referral range. Risk increased with age such that by a median age of 20.9 months (range 11-62), the combined rates ranged from 11 to 27%. 22 Noeder et al. 24 examined the concurrent validity between the ASQ-3 and the BSID. They also recommended use of a more conservative number, > 1 SD below the normative mean, to identify children in need of referral to increase the predictive value of the ASQ-3 for children with cardiac problems.
When the children with CL ± P who scored in the monitor range are added to the referral numbers, 75% (75/100) of infants met criteria for monitor/refer on at least one domain and 51% (51/100) on two or more at T1; 78% met criteria for one and 47% (43/92) for two or more at T2. Of the 69 infants with two data points, 90% (N = 62) met criteria for monitor/refer on at least one domain and 85% (78/92) for two or more domains across the two assessments. The percentage of combined monitor/refer risk was distributed fairly equally across each of the domains ranging from 30% on Problem Solving to 41% on Communication. For Toddlers in the Costa et al. 15 study, the highest combined (monitor and refer) risk was found in the Communication Domain (56%) and lowest was Fine Motor (11%). These results suggest that children with CL ± P should receive regular developmental screenings to ensure that those children in need of early intervention services are identified.
Limitations/Future Directions
When compared to the population of infants diagnosed with CL/P, the current sample was fairly representative of factors such as sex, diagnosis, socioeconomic risk,50,51 Hispanic/LatinX population 61 and rates of prematurity52,53; however, a larger proportion of our population was White and as group was better educated compared to US Census data.50,51,61
Subjects for this study were recruited from three cleft clinics and online support groups for families whose children were born with CL/P. Despite the large recruiting pool, we recognize generalizability could be affected due to the limited geographical locations from which subjects were recruited. Additionally, it is likely that caregivers who responded to requests from online support groups might differ from others on factors such as motivation or access to social media and/or technology. The generalizability of findings is also limited to infants with CL ± P as our study did not include infants with CP due to the fact that data was collected pre and two-months post lip repair in the parent study. As noted above, children with CP are often found to have higher rates of developmental delay and cognitive challenges, even in infancy.17,18 This population of children may have been found to be at greater risk as measured on the ASQ-3.
Finally, it is possible that infants born prematurely or with other complications were more closely monitored than the other infants with cleft and received intervention services when appropriate. We did not collect information on intervention services received, which is a significant weakness of this study and did not allow us to determine if there were associations between factors such as SES and medical risk that influenced provision of services. Information about early intervention services, either past or ongoing, would be important to gather in future research to better assess the achievement of milestones as reported by caregivers.
While caregiver observation may be a useful tool to identify infants at risk, as with any self or proxy-report, inherent bias can affect responses. This may lead to an over reporting or conversely an under reporting of behaviors. Additionally, while caregivers are most familiar with their infants and toddlers, caregiver reports continue to offer only a snapshot of behaviors or patterns at intervals rather than a daily recording of observations. Future research might benefit from collecting data across multiple, consistent time points. Not only can more data points inform conclusions regarding patterns of development, but the achievement of milestones can be explored across different age groups.
Conclusions
Infants with CL ± P demonstrate high rates of developmental risk based on parent-report using the ASQ-3. Infants with CLP and male infants were at greatest risk. Infants screened in the monitor and referral ranges of the ASQ-3 require close ongoing monitoring by cleft-team members. Caregivers can be given strategies for home interventions across identified risk areas. Infants who meet the refer criteria on two or more domains should have a more in-depth evaluation with possible referral to an infant intervention program. Future research can include infants and toddlers with a more comprehensive range of diagnoses, increase time points to better understand development over the first several years of life and integrate information from both caregivers and providers.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231225304 - Supplemental material for Developmental Risk for Infants with Cleft Lip with or Without Cleft Palate Based on Caregiver-Proxy Reports
Supplemental material, sj-docx-1-cpc-10.1177_10556656231225304 for Developmental Risk for Infants with Cleft Lip with or Without Cleft Palate Based on Caregiver-Proxy Reports by Kathleen A. Kapp-Simon, Meredith Albert, Todd C. Edwards, Salene M. Jones, Claudia Crilly Bellucci, Janine Rosenberg, Donald L. Patrick and Carrie L. Heike in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
We extend our appreciation to the caregivers who took part in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the National Institute of Dental and Craniofacial Research (grant number: R01DE024986).
Human Subjects Protection
All study procedures adhered to ethical standards of practice. Informed consent was required of all participants. This study received ethical approval from the University of Washington IRB (Approval # J - IRB00005647) on September 18, 2015, The University of Illinois at Chicago (Approval # 2015-0913) on Dec 2, 2015, and The Western Institutional Review Board (Approval # 20160692) on March 20, 2016.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.