
Abstract
Background
This article investigates the prevalence of conditions that affect cognitive and/or psychosocial functioning in 10-year-old children born with a cleft lip and/or palate (CL/P) and explores how the presence of such additional difficulties may affect the reporting of outcomes in psychological research.
Design
Cross-sectional data derived from routine psychological assessments.
Setting
Centralized treatment, Norway.
Participants
Data on cleft type and additional conditions were collected for 754 children with CL/P from 11 consecutive birth cohorts. Data on psychological adjustment were collected for three consecutive birth cohorts (n = 169).
Main Outcome Measures
The Strengths and Difficulties Questionnaire (SDQ), completed by children and parents.
Results
A total of 240 children (32%) in the sample had an additional condition, such as developmental delay, attention deficit/hyperactivity disorder, or a specific language impairment or dyslexia. Analysis of SDQ scores using conventional exclusion criteria (approach 1) was compared with a second method (approach 2), which included all children and categorized them according to the presence or absence of additional conditions. Significant variation in profiles of psychosocial adjustment was found depending on the approach to exclusion.
Conclusions
The presence of additional conditions in a sample may affect results and subsequently the conclusions drawn in relation to the psychosocial adjustment of children born with CL/P. The present study emphasizes the importance of careful assessments and reporting of all associated conditions, in order to improve the understanding of the impact of a cleft and the consequences of associated conditions in this population.
A cleft in the lip and/or the palate (CL/P) may be associated with a number of additional conditions, including malformations and anomalies in the central nervous system, cardiovascular problems, and various syndromes (Milerad et al., 1997; Stoll et al., 2000; Sivertsen et al., 2008; Gorlin et al., 2009). Research has suggested that cognitive dysfunction may also occur in association with CL/P (Milerad et al., 1997), with degrees of impairment varying from mild to severe. Some studies have reported a higher-than-expected proportion of children with CL/P to be at risk for developmental problems and/or learning disabilities, particularly if there is palatal involvement (Neiman and Savage, 1997; Broder et al., 1998; Speltz et al., 2000; Millard and Richman, 2001; Christensen and Mortensen, 2002; Swanenburg et al., 2003). More recent studies have explored the neurobiological components of behavior and/or cognitive factors in this population (Nopoulos et al., 2005; Nopoulos et al., 2007) and found evidence for differing brain structures in children and adults with a cleft.
In previous and current psychological research, the selection of inclusion and exclusion criteria has been driven by biomedical parameters. Children with known syndromes and severe developmental and/or neurological difficulties are therefore normally excluded from studies investigating the impact of CL/P. While restrictive selection criteria should ensure homogeneity within samples, the results can become skewed if this process is not applied correctly (Schinka and Velicer, 2003). In addition, studies within the field of CL/P research have employed different approaches to their choice of exclusion criteria, creating large methodological variation across studies (Broen et al., 1998; Wyszynski et al., 2006). It is considered good practice for authors to specify their exclusion criteria; however, this information is still occasionally lacking or reported in insufficient detail. As understanding of associated conditions increases, there is a clear need in current research investigating the impact of CL/P to discuss the optimum inclusion and exclusion criteria for the variables under study and to achieve a greater consensus in the choice of criteria used.
A further unfortunate consequence of the biomedical approach to inclusion and exclusion is a lack of understanding about those subgroups that are usually excluded, despite the importance of this understanding for research and clinical practice. While some research has aimed to increase our knowledge about specific, diagnosed syndromic conditions associated with CL/P, others that manifest in less obvious ways or are not yet classified as part of a syndrome have received little attention.
Another important observation is that potentially important factors and interaction effects between variables are often overlooked or disregarded within analyses, and their potential impact is rarely discussed in relation to the results of studies investigating psychological functioning (Strauss and Broder, 1991). While many studies yield potentially interesting findings, the subsequent reporting and interpretation of these findings may be misleading if the impact of important included variables is not fully considered (Pope and Snyder, 2005; Wyszynski et al., 2006). One such variable could be the presence of an additional condition. It is likely that children with less severe forms of associated conditions (such as learning difficulties, language impairments, attention deficit/hyperactivity disorder [AD/HD] and dyslexia) will remain included in cleft samples, with the further problem that specific information about the presence of these conditions is likely to be missing. Although the prevalence of less severe conditions in relation to CL/P is currently unknown, such conditions are likely to affect psychosocial functioning significantly (Huntington and Bender, 1993; Svetaz et al., 2000; Pinquart and Shen, 2011). The impact of additional conditions such as these on research outcomes has already been demonstrated in the physical disabilities literature (Miyahara and Piek, 2006). If the existence of these and other mild impairments is not accurately reported or controlled for within statistical analyses, research in this area is unlikely to provide an accurate picture of adjustment in children born with CL/P.
This issue may, in part, explain why research investigating psychosocial outcomes in CL/P to date has produced conflicting and often confusing results (Rumsey and Stock, 2013). While some studies have identified increased levels of psychosocial difficulties in children with CL/P, others have found this group to have normal or higher levels of positive adjustment when compared with their nonaffected peers (Lockhart, 2003; Rumsey and Harcourt, 2004, Hunt et al., 2005; Collett and Speltz, 2007; Wehby and Cassell, 2010; Feragen, 2012). A better understanding of the relationship between CL/P and associated conditions, and the implications of this relationship for psychosocial adjustment, would have the potential to improve significantly the quality of information that is given to parents regarding their child's future development. Consequently, appropriate treatment and support could be offered on an individual patient basis, thus allowing a more targeted allocation of limited resources. A more detailed awareness of how additional conditions may covary with CL/P as a whole, or with different cleft types, may also lead to a better understanding of the embryonic phenomena underlying the development of CL/P.
In light of these considerations, the primary aim of the present study was to explore the prevalence of associated conditions known to affect psychological and/or cognitive functioning in a large Norwegian sample of 10-year-old children born with CL/P. Second, the available data were analyzed using two different approaches to exclusion, to illustrate the potential consequences of different exclusion criteria on the conclusions drawn about psychosocial functioning in individuals with CL/P.
Method
Design and Participants
The present study was based on retrospective cross-sectional clinical data from children born with CL/P, who were aged 10 years at the time of psychological assessment. All of the children in the sample were treated by one of the two cleft teams in Norway, a country that provides centralized treatment of CL/P. Consequently, 11 birth cohorts of children born from 1992 to 2002, in addition to half of the birth cohort of children born in 1991, were included in this study (n = 754). The total sample included 346 children (46.1%) with cleft lip and palate (CLP), 114 children (15.2%) with cleft lip alveolus (CLA), and 290 children (38.7%) with cleft palate (CP) or submucous cleft palate (SMCP), of whom 241 children had CP and 52 had an SMCP.
Children with CLA were not, until April 2007, routinely offered a psychological follow-up at age 10 years. Thus, data for children with CLA are lacking for the first five birth cohorts (1992 to 1996), affecting the prevalence of the different cleft types in the total sample. In those birth cohorts including children with CLA (1997 to 2002), the prevalence of cleft types was as follows: 180 children (39.0%) with CLP, 112 children (24.0%) with CLA, and 170 children (37.0%) with CP/SMCP. In the total sample, 68 of the children (9.4%) were of non-Caucasian origin; many of these children were adopted (n = 47, 6.8% of the total sample).
For some children, routine measures and questionnaires were not used because of severe developmental problems impeding the use of self-report (n = 36).
The study conformed to guidelines provided by the local ethics committee (Region Oslo - East). Information concerning cleft type, gender, and the presence of associated conditions (n = 754) was saved and analyzed anonymously in a separate data file, in accordance with guidelines produced by the Ministry of Health and Care Services (Helseregisterloven §2–3). Psychological data were considered to be sensitive, and thus parental consent was sought for its use. Information about the present study was sent to both parents and children from three consecutive birth cohorts (211 families in total). Only 2% actively declined participation, while 17.9% did not respond to the request, leaving a participation rate of 80.1 %.
Measures
Additional Conditions and Difficulties
Information about the presence of an associated condition was collected from the child's clinical treatment records and/or from information provided by the parents at the time of assessment.
Associated difficulties affecting cognitive and/or psychological functioning included a wide range of conditions, such as syndromes (with or without other associated conditions), developmental difficulties (such as a diagnosis within the autism spectrum disorder, a developmental delay, or nonspecific developmental difficulty affecting the child's cognitive capacities and learning), AD/HD, specific language impairment (SLI), dyslexia, or learning difficulties (such as difficulties in reading and language or mathematics). Additional medical conditions such as a heart defect or other birth anomalies were also registered, in addition to a diagnosis of Pierre Robin sequence.
Strengths and Difficulties Questionnaire
The Strengths and Difficulties Questionnaire (SDQ; www.sdqinfo.com; Goodman, 1997) is a screening tool for behavioral difficulties and strengths in children and adolescents, completed by one or both parents and the child in the current study. The SDQ has been used routinely as part of a psychological assessment at age 10 years in the Oslo team since the end of 2009. Data therefore exist for more than three consecutive birth cohorts, providing both self-reported and parent-reported data. The SDQ includes five subscales measuring emotional distress, conduct problems, hyperactivity/attention difficulties, peer relationship problems, and prosocial behavior. Each subscale includes five items that are positively or negatively worded. Each item is scored “not true,” “somewhat true,” or “certainly true” (0 to 2). The first four subscales are summarized into the Total Difficulties Score (including in total 20 items, with scores ranging from 0 to 40). Internal reliability (Cronbach's alpha) was “satisfactory” for the Total Difficulties Score for both the child and the parent version of the questionnaire (α = .77 and .84) but was modest for some of the subscales: emotional distress (α = .66 and .65), conduct problems (α = .48 and .58), hyperactivity/attention difficulties (α = .58 and .80), peer relationship problems (α = .51 and .64), and prosocial behavior (α = .65 and .62). Similar results have been reported in previous studies (Goodman, 2001; Van Roy et al., 2008) and indicate that scores for some of the subscales should be interpreted with caution.
Statistical Analysis
Analyses were performed using SPSS 19. Descriptive statistics were used to examine the frequency of the included variables. The SDQ reliabilities (Cronbach's α) were calculated for the Total Difficulties Score and each of the five subscales. Chi-square tests were performed when analyzing differences in frequency between dichotomous groups, while differences between groups on the continuous outcome measure were analyzed using independent sample t tests. Cohen's d effect sizes were calculated in cases of significant differences in means on the SDQ.
Results
In a sample of 754 children, 240 children (32%) had known or suspected additional conditions. The prevalence of such conditions across groups is described in more detail below.
Descriptive Statistics
Distribution of Cleft Types and Gender
The distribution of cleft types, gender, syndromes, and the presence of additional difficulties for the 11 consecutive birth cohorts (n = 754) is summarized in Table 1. The cleft type ratio (for birth cohorts 1997 to 2002) and the gender ratio presented in Table 1 are consistent with previous prevalence figures (Sivertsen et al., 2008).
Distribution of Cleft Type, Gender, and Additional Conditions Affecting Psychological and/or Cognitive Function (Including Children With a Syndrome and an Additional Difficulty) for the Study Sample (n = 754) *
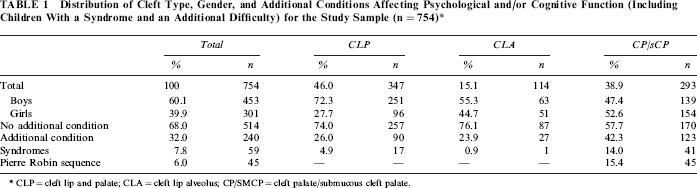
CLP = cleft lip and palate; CLA = cleft lip alveolus; CP/SMCP = cleft palate/submucous cleft palate.
Distribution of Syndromes Across Cleft Types
As can be seen in Table 1, a total of 59 children (7.8%) were diagnosed with a syndrome (such as Treacher Collins, 22q11, or Crouzon). As expected, the frequency of a diagnosed syndrome differed across cleft types: 17 of the children with CLP were diagnosed with a syndrome (4.9%), compared with 41 of the children with CP (14%). Only one child with CLA had been diagnosed with a syndrome (0.9%). Most of the children with a diagnosed syndrome also had other difficulties, such as a developmental disorder and/or learning difficulties (n = 57, 96.6%), while two children had a diagnosed syndrome without any additional difficulties (3.4%; χ2 = 123.09, P < .001).
Distribution of Pierre Robin Sequence
Forty-five children with CP/SMCP had a diagnosis of Pierre Robin sequence (PRS; 15.4%). There was a somewhat higher but nonsignificant distribution of boys with a diagnosed Pierre Robin sequence than girls (n = 26, 18.7%; n = 19, 12.3%; χ2 = 2.28, P = .089). The frequency of diagnosed syndromes did not differ in children with CP with or without PRS (n = 6, 13.3%; n = 35, 14.2%; χ2 = .02, P > .05). However, a significantly higher frequency of children with PRS had an additional diagnosis on the autism spectrum disorder: 11.1% (n = 5) compared with 1.6% (n = 4) in the group of children with CP (χ2 = 11.48, P < .01). All the children with a diagnosis on the autism spectrum disorder were boys. The prevalence of other additional difficulties did not vary significantly between the two samples of children with CP (48.9% of the children with PRS had some type of additional condition compared with 41.1% of the children with CP without PRS; χ2 = 0.96, P > .05).
Distribution of other Medical Conditions
Hearing difficulties were registered in 35 children (4.7%), including children with hearing aids and/or children with a history of hearing difficulties that the parents believed had an impact on the child's everyday life. Other conditions, such as a heart anomaly, syndactyly, or other medical anomalies, were recorded in 37 children (4.9%). For nine children, there was a diagnosis of epilepsy (1.2%).
Prevalence of Associated Conditions in Adopted Children
There were 47 adopted children in the sample (6.8%), most with a visible cleft (n = 39, 83%). Analyses showed that there were no significant differences in the presence of additional conditions between adopted and non-adopted children with CLP: while 26 of the adopted children with CLP did not have an additional condition (66.7%), this was the case for 297 of the remaining sample of children with CLP/CLA (76.3%; χ2= 1.80, P > .05).
Distribution of Conditions Affecting Psychological and/or Cognitive Function
Table 2 provides an overview of the distribution of conditions affecting psychological and/or cognitive functioning. Sixty-seven children (8.9%) in the present sample had AD/HD, 29 had a specific language disorder (3.9%), and 37 had dyslexia (4.9%). Two children had a diagnosis of Tourette syndrome (.03%). A total of 108 children (14.4%) had a condition likely to affect development. An important finding, both for clinical practice and research was that 69 children (9.2%) had indications that were characteristic of developmental difficulty or delay without a clear diagnosis. A remaining 25 children (3.3%) had been diagnosed with a developmental difficulty, while less than 2% of the children had a diagnosis on the autism spectrum disorder. Forty-two children had specific or more general learning difficulties, related to language, reading, and/or mathematics (5.6%). The number of children with a specific condition does not add up to the total number of children with an additional condition since some children had more than one additional condition (n = 120).
Frequency of Associated Conditions Across Cleft Type
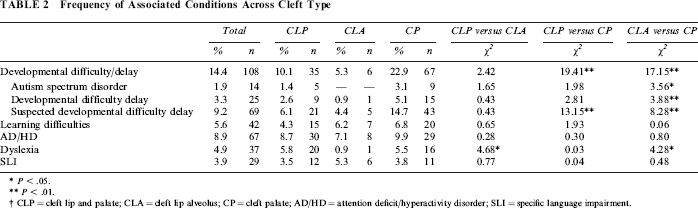
P < .05.
P < .01.
CLP = cleft lip and palate; CLA = cleft lip alveolus; CP = cleft palate; AD/HD = attention deficit/hyperactivity disorder; SLI = specific language impairment.
Prevalence of Associated Conditions Across Cleft Types
Table 2 also shows the breakdown of participants according to type of associated conditions. As can be seen, some conditions occur significantly more often in some cleft types than others, while other associated conditions do not seem to vary as a function of cleft type: while 4% to 6% of the children had learning difficulties irrespective of cleft type, the prevalence of developmental difficulties varied significantly across cleft type (CLP: n = 35, 10.1%; CLA: n = 6, 5.3%; CP: n = 67, 22.9%). Another significant difference was that the frequency of dyslexia was found to be 5% to 6% in children with CLP and CP, while less than 1 % of the children with CLA had this diagnosis.
Children with More Than One Additional Condition
Within the total sample, 240 children (32.3%) had an additional difficulty. While 123 of the children (16.4% of the total sample; 51.3% of the children with an additional condition) had one extra diagnosed condition in addition to the cleft, 67 of the children had two additional diagnoses (8.9%; 27.9%), while the remaining 53 had three or more conditions in addition to the cleft (7%; 22.1%). As expected, the mean value of the number of additional conditions was lower for children with CLP/CLA (M = 0.46; SD = 0.95) than for children with CP (M = 0.78, SD = 1.11), reflecting a significant difference between these two cleft types in terms of risk of associated conditions (F[751] = 17.13, P < .01). Not surprisingly, children with a syndrome had a significantly higher frequency of co-occurring additional conditions compared with children without a diagnosed syndrome (cleft only: M = 0.42, SD = 0.83; cleft with diagnosed syndrome: M = 2.53, SD = 1.10; F[750] = 328.42, P < .001). There were no gender differences in the frequency of co-occurring conditions (boys: M = 0.59, SD = 1.05; girls: M = 0.58, SD = 1.00; F[751] = 0.05, P > .05).
Prevalence of Associated Conditions According to Gender
Analyses exploring possible gender differences in the prevalence of additional conditions showed that there were no significant differences between boys and girls within the different cleft types. The exception was a significantly higher frequency of diagnosed dyslexia in boys with CLP compared with girls with CLP (n = 18, 7.2% versus n = 2, 2.1%; χ2 = 3.33, P < .05), while the frequency was approximately 5% in both boys and girls with CP (χ2 = 0.04, P > .05). No other additional conditions varied significantly in frequency between boys and girls.
How Did the Presence of Associated Conditions Affect Psychosocial Measurement?
The second aim of the present article was to explore how the presence of additional conditions in a sample may affect the reporting of the results of psychological measurement. Data for the SDQ outcome measure were available for 211 children, for whom parental consent for inclusion in this study was given by 80.1% of parents. Hence, psychological data for a total of 169 parents and 164 children were included in the following analyses (data from the SDQ were lacking for five children of the consenting parents).
To test how the choice of different exclusion criteria affected the reporting of psychological outcomes, the present sample was categorized using two different approaches: the first used traditional exclusion criteria, reflecting those used by most studies in this area of research. This involves excluding children with a known syndrome and/or a diagnosed severe to moderate developmental disability (approach 1). In accordance with this approach, 21 children were excluded from analyses (10.4%). The second approach involved including all children, while registering all known additional difficulties and performing analyses to take account of these different conditions (approach 2). Using approach 2, a total of 68 children (32.0%) were registered as having a diagnosis in addition to the cleft and were thus categorized according to the type of condition.
To explore how the two different approaches affected psychological profiles, a split file analysis was performed on the data obtained from the SDQ (comparing excluded and included children from approach 1), followed by an independent two-sample t test comparing children with and without any additional conditions (approach 2). The analysis therefore tested whether scores on the outcome measure differed significantly between the two approaches.
Forty-seven children with some type of additional condition were still included in the main sample when using approach 1. The analyses revealed significant differences in psychosocial and/or cognitive functioning between the two approaches, highlighting more psychosocial difficulties in children with a cleft when using approach 1 than when using approach 2. As can be seen in Table 3, significant differences were present both in self-reports from the child and in parent reports.
Different Approaches to Exclusion Criteria and Their Effect on Psychological Measurement †
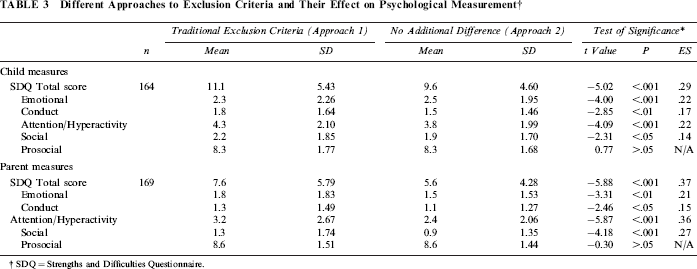
SDQ = Strengths and Difficulties Questionnaire.
Self-reports
Results from the independent sample t tests, using mean scores for approach 1 (M1) and approach 2 (M2) were as follows: total score, M1 (SD) = 11.1 (5.43), M2 = 9.6 (4.60), t (139) = -5.02, P < .001, ES = .29; emotional problems, M1 (SD) = 3.0 (2.26), M2 = 2.5 (1.95), t (139) = -4.00, P < .001, ES = .22; conduct problems, M1 (SD) = 1.8 (1.64), M2= 1.5 (1.46), t (139) = -2.85, P < .01, ES = .17; attention problems, M1 (SD) = 4.3 (2.10), M2 = 3.8 (1.99), t (139) = -4.09, P < .001, ES = .22; peer problems, M1 (SD) = 2.2 (1.85), M2 = 1.9 (1.70), t (139) = -2.31, P < .05, ES = .14. The only nonsignificant subscale was the SDQ measurement of prosocial behavior (M1 = 8.3 [1.77], M2 = 8.3 [1.68], t [139] = .77, P > .05), which produced similar profiles irrespective of the chosen exclusion/inclusion approach.
Parent Reports
Results from the independent sample t tests, with mean scores for approach 1 (M1) and approach 2 (M2) were as follows: total score, M1 (SD) = 7.6 (5.79), M2 = 5.8 (4.28), t (146) = -5.88, P < .001, ES = .37; emotional problems, M1 (SD) = 1.8 (1.83), M2 = 1.5 (1.53), t (146) = -3.31, P < .01, ES = .21; conduct problems, M1 (SD) = 1.3 (1.49), M2= 1.1 (1.27), t (146) = -2.46, P < .05, ES = .15; attention problems, M1 (SD) = 3.2 (2.67), M2 = 2.4 (2.06), t (146) = -5.87, P < .001, ES = .36; peer problems, M1 (SD) = 1.3 (1.74), M2 = 0.92 (1.35), t (146) = -4.18, P < .001, ES = .27. In the parent-reports, the only nonsignificant subscale was the SDQ measurement of prosocial behavior (M1 = 8.6 [1.51], M2 = 8.6 [1.44], t [146] = –.30, P > .05), which produced similar profiles irrespective of the chosen exclusion/inclusion approach.
In summary, 32% of the children in the sample had an additional condition, such as developmental delay, AD/HD, a specific language impairment, or dyslexia. Analyses demonstrated that the two different approaches to inclusion and exclusion significantly affected the results of scores on the psychological outcome measure and hence possible conclusions about the psychological adjustment profiles of this sample.
Discussion
The results of this study confirmed the presence of associated conditions affecting cognitive and/or psychological functioning in a substantial proportion of 10-year-old children with CL/P. Significant differences were found between analyses based on two different approaches to exclusion criteria. When using the conventional approach of excluding those with identifiable syndromes and severe conditions, results were indicative of a higher level of psychosocial difficulties in children with CL/P. In contrast, when using an approach in which children were categorized according to whether or not an additional condition was present, children with a cleft alone produced scores that were within the normal range. The findings of this study therefore have important implications for the assessment and reporting of psychological adjustment in this group.
A total of 240 of the children in this sample (32.3%) had a syndrome or additional condition known to affect development and/or learning. The prevalence of some conditions was found to vary across cleft types, where cleft palate was associated with a higher risk for a diagnosed syndrome, developmental difficulties, and ASD and palatal involvement was associated with a higher risk for dyslexia. Only two significant gender differences were identified. First, there was a higher frequency of dyslexia in boys with CLP compared with girls with CLP. Second, children with PRS were found to have a significantly higher frequency of autism spectrum disorder, a diagnosis that was found only in boys within this sample. Hearing difficulties were registered in 35 children (4.7%). Although it is possible that hearing difficulties may affect psychosocial adjustment to CL/P, data were insufficient to conduct suitable analyses. Further research should seek to examine the relationships of this variable to psychological adjustment in the future.
When examining the frequencies of additional conditions in this sample in relation to national samples, a number of interesting issues were raised. Prevalence can be compared only approximately, since a variety of criteria and measures have been used to identify developmental difficulties/delay. Nonetheless, the frequencies reported in the present article confirm that children with CL/P are at a higher risk for such difficulties than the general population. In regard to developmental difficulties/delay, findings are difficult to compare since children with a cleft do not typically undergo standardized cognitive testing as part of the routine assessments in Norway. However, the results of the present study seem to indicate a higher prevalence of diagnosed developmental difficulties/delay in children with a cleft (3.3%) when compared with the prevalence worldwide (0.55% to 3%) or in national samples (0.77%; Strømme, 2000; Boyle et al., 2011). This finding is especially relevant in cases of CP, where a developmental delay had been diagnosed in more than 5% of the children. In addition, a significant number of children had a suspected but undiagnosed developmental delay, with as many as 15% of the children with a cleft palate in this category, pointing to a likely total number of children with a developmental delay that seems considerably higher than in national comparison samples. A similar picture can be seen when examining the prevalence of autism spectrum disorder in a normative sample (0.6%; Fombonne, 2009; Boyle et al., 2011) compared with the present sample overall (1.9%) and those with CP (3.1%). For AD/HD, the frequency was higher in children with a cleft (8.9%) when compared with national (3% to 5%; Suren et al., 2012), European (4% to 5.5%; Polanczyk et al., 2007), and American (6.7%; Boyle et al., 2011) samples, with few variations across cleft types. General prevalence indicates that 6% to 8% of children have an SLI (Tomblin et al., 1995), while the present sample included approximately only 4%. Finally, varying frequencies of dyslexia have been reported nationally (5% to 10%; Høien and Lundberg, 2012), with approximately 5% of the current sample having this diagnosis. In summary, the findings from the current study indicate that children with a cleft could be at higher risk for developmental difficulties or developmental delay, in line with previous research (Millard and Richman, 2001; Christensen and Mortensen, 2002; Swanenburg et al., 2003; Conrad et al., 2009). Children with CL/P may also be at higher risk for conditions such as AD/HD, while the prevalence of SLI and dyslexia seem to be comparable to rates in the general population.
As hypothesized, the results of this study indicated that the choice of exclusion criteria affects the results obtained and thus may affect the conclusions drawn regarding this population. To our knowledge, this is the first study to compare different approaches to exclusion and to test their effect on the reporting of outcomes. Specifically, more psychosocial difficulties were identified for this population when using the traditional approach to exclusion. In addition, this approach results in an inadequate consideration of the presence and the impact of additional conditions in a sample and affects mean outcome measures as a result. On the other hand, results indicated that when scores for children with associated conditions were analyzed separately, those without additional conditions showed similar levels of psychosocial adjustment as national comparison samples, using the SDQ (e.g., Van Roy et al., 2006; Van Roy et al., 2010).
It is clear that efforts should be made to achieve a consensus about how to deal with the presence of associated conditions in research relating to children with CL/P, in order to facilitate comparisons across samples and studies. The adoption of a new approach to research in this area is therefore suggested, in which inclusion is favored over exclusion and in which additional conditions are carefully recorded and separately analyzed in relation to psychologically relevant variables. This approach would create a large total data pool, from which subsamples could be isolated and studied.
The results of the present study strongly illustrate the need to achieve large samples in research of this kind: despite a sample of more than 750 children, data sets became relatively small when exploring subgroups. Some results seemed clinically interesting yet did not achieve statistical significance. For example, in the present study, a higher-than-expected frequency of boys with CLP had been diagnosed with dyslexia, while lower-than-expected numbers were the case for boys with CLA. Also of clinical interest was a higher frequency of learning difficulties in girls with CLA than boys; again, this was not found to be statistically significant and may have been due to the small subsamples. Collecting large data sets is possible in countries where CL/P services are centralized and where large-scale collaborative studies across teams and countries are achievable, although consensus on methodology and measures is crucial (Rumsey and Stock, 2013). Where large data sets are not available, the implications of this study's findings should nonetheless be taken into consideration when selecting appropriate exclusion criteria.
Further analysis of this data set is presented in a second article by the current authors (Feragen and Stock, in press). This article proposes categorization according to two main groups: cleft only and cleft with an additional condition(s), since differences between conditions were found to be small. Nonetheless, the type of condition in the latter group should always be stated for children with additional conditions when reporting sample characteristics, and tests to examine any differences between the different conditions should be conducted where possible. This approach will allow researchers to check whether the presence of an additional condition is potentially a confounding variable in psychological adjustment and hence distinguish which psychosocial outcomes are related to the cleft and which outcomes are associated with having an additional condition(s).
Another possible issue in cleft research is the broader ramifications of adopting differing paradigms of inclusion and exclusion. In line with biomedical parameters, the tendency to refer to pathological findings in cleft research has dominated for many decades (Strauss, 2001). More recently, however, research has begun to highlight more positive findings (Baker et al., 2009; Berger and Dalton, 2009; Feragen et al., 2010). Similarly, reviews have suggested that the cleft may become the focus for distress, which actually results from other sources (Rumsey and Stock, 2013). While the potential psychosocial challenges surrounding CL/P are considerable, a clinical approach based on the identification of deficits may not be the most helpful. Equally, researchers have a responsibility in relation to the focus of the literature they are presenting. Rather than referring in the main to past research that has highlighted difficulties and challenges and that may be outdated because of changes in social settings and treatment, researchers should consider providing a more balanced view and to also consider variables that may play a part in positive adjustment to a condition such as CL/P. Authors of review articles should be particularly careful with their choice of references, since these reviews will often be used as templates for ongoing research and as an evidence base for clinical practice.
The results of the present study underline the crucial role of psychology within cleft care. The search for well-defined subtypes in children with CL/P would lead to better prognostic information, enabling early identification of children at risk for psychosocial and/or cognitive difficulties. Such information would also be of value in predicting and understanding longer-term clinical outcomes, such as psychological and social well-being, educational outcomes, and quality of life. Psychologists would thus possess the more detailed clinical knowledge needed to differentiate between the various challenges a family or individual might face and to be able to provide support accordingly. In addition, this study has demonstrated the need to formally assess and accurately document the child's progress at key developmental milestones. However, given the variation in levels of psychological care provided within cleft teams across and within countries, the accurate identification of additional conditions is in itself likely to be a challenge. Although some teams are able to employ full-time clinical psychologists, others can offer only a limited service, while some are not resourced to provide any psychological input. In addition, the way in which conditions are diagnosed will undoubtedly vary between sites and countries. In the present study, several children (n = 69) had a suspected but undiagnosed condition in addition to the cleft. This factor alone may affect the findings of a study if not appropriately documented and discussed. Nonetheless, the aim of the present study was not to provide a solution to such important methodological challenges but to raise awareness of the potential consequences on psychological measurement and practice and to encourage professionals to consider an alternative approach to the analysis of their data.
The current study has a number of strengths. First, a large sample size and high participation rate were obtained. The data were collected within a centralized treatment setting, and this suggests the sample is likely to be highly representative. Another strength was the use of a well-known, widely used, and valid questionnaire. Finally, the main measure was completed by both parents and children. The sample also included a high participation rate from fathers, who are not often well represented in this area of research (Nelson et al., 2012; Stock and Rumsey, in preparation). Nonetheless, some caution is required when interpreting the results. A key limitation of this study was the lack of a control group. This limitation was addressed by comparing this study's findings with results from national samples and scale norms. Another limitation could be that the self-report version of the SDQ is recommended for use from the age of 11 years, while the children in the present study were aged 10 years at the time of data collection. However, children of the same age have been included in large national studies and audits in the past (e.g., Van Roy et al., 2010), and results can be compared accordingly. In addition, statistical analyses demonstrated relatively low reliability for some of the subscales of the SDQ. However, reliability scores were comparable to those reported by Goodman (2001).
The current study provides a detailed description of 11 consecutive birth cohorts of children born with a cleft and treated by the Oslo team, Norway, including information about cleft type, gender, and associated conditions affecting psychological and/or cognitive function. The high frequency of additional difficulties in samples of children with CL/P indicates a need to develop a consensus about how to manage their presence in research, in order to facilitate comparisons across samples and studies and in order to distinguish between the effects of having a cleft and the effects of having an additional condition. Future research should seek to further develop the results found in the present study as well as to examine previously excluded groups in more detail to ensure they are no longer neglected in research and that their needs are met in practice.
Footnotes
Acknowledgments
The work of this article was financed by funds from the Norwegian ExtraFoundation for Health and Rehabilitation, project 2011/0198.