
Abstract
Background
The effectiveness of virtual-reality (VR) simulation-based training in cleft surgery has not been tested. The purpose of this study was to evaluate learners’ acceptance of VR simulation in airway management of a pediatric patient post-cleft palate repair.
Methods
This VR simulation was developed through collaboration between BioDigital and Smile Train. 26 medical students from a single institution completed 10 min of standardized VR training and 5 min of standardized discussion about airway management post-cleft palate repair. They spent 4-8 min in the VR simulation with guidance from a cleft surgery expert. Participants completed pre- and post-surveys evaluating confidence in using VR as an educational tool, understanding of airway management, and opinions on VR in surgical education. Satisfaction was evaluated using a modified Student Evaluation of Educational Quality questionnaire and scored on a 5-point Likert scale. Wilcoxon signed-rank tests were performed to evaluate responses.
Results
There was a significant increase in respondents’ confidence using VR as an educational tool and understanding of airway management post-cleft palate repair after the simulation (P < .001). Respondents’ opinions on incorporating VR in surgical education started high and did not change significantly post-simulation. Participants were satisfied with VR-based simulation and reported it was stimulating (4.31 ± 0.88), increased interest (3.77 ± 1.21), enhanced learning (4.12 ± 1.05), was clear (4.15 ± 0.97), was effective in teaching (4.08 ± 0.81), and would recommend the simulation (4.2 ± 1.04).
Conclusion
VR-based simulation can significantly increase learners’ confidence and skills in airway management post-cleft palate repair. Learners find VR to be effective and recommend its incorporation in surgical education.
Introduction
In the face of strict work hour limitations during residency training, surgical residents are experiencing less time in the roles of first assistant and primary surgeon.1,2 Reduced time exercising clinical decision-making in a leadership role, coupled with overall diminished resident autonomy can be detrimental, particularly as the complexity of operations increase. In response to the increased knowledge required of surgical residents, incorporation of multiple forms of simulation fills gaps in surgical education and has become a standard component of medical and surgical training in high-income countries.3–9
Virtual reality (VR) is being explored to enhance surgical education due to its unique ability to recreate clinical situations in an immersive fashion where procedural skills, anatomical knowledge, and clinical acumen can be practiced in real-time. 10 Moreover, VR technology allows for quantification of accuracy, precision, and error rates of performance. 11 Various studies in different surgical specialties contend that VR training improved operative performance in residents, and a systematic review assessing effectiveness in teaching medical content suggests beneficial outcomes with more research needed in low- and middle-income countries.11–14 Although VR has played a global role in craniofacial training since 2006, few studies have evaluated its effectiveness in plastic surgery, specifically in cleft care.15–18
High incidences of treatable cleft lip and palate anomalies bring the topic of VR simulation in surgical education to a global scale.19,20 Significant barriers to comprehensive cleft care exist in Latin America, Africa, and Asia due to lack of financial resources, technical expertise, and access to training. 21 Simulation-based training has been widely adopted in developed countries, and VR-based simulation may reduce logistical and financial barriers associated with in-person training in low-resource regions and promote equitable access to cleft care education.
In January 2023, Smile Train, Inc. (New York) and BioDigital, Inc. (New York) launched a novel multi-user cleft surgery VR platform that simulates cleft palate repair in a metaverse operating room. This platform may promote cost-effective education to healthcare professionals in regions that lack sufficient resources and training to perform high-quality, safe procedures on a broad scale. This study was conducted to evaluate learners’ acceptance of and procedural confidence in a VR simulation of upper airway management of pediatric patients following cleft palate reconstruction.
Methods
Development of the Metaverse Simulation
This simulation was developed through collaboration between BioDigital, Inc. and Smile Train, Inc. Smile Train, a large cleft-care charity, is a non-profit organization focused on providing global comprehensive cleft care through partnering with local in-country medical professionals. Smile Train's model provides training and financial resources to local healthcare providers to promote no-cost comprehensive cleft care to all patients. BioDigital is a New York-based biomedical software company. The BioDigital platform is an interactive 3D model of a medically accurate human body. It is a fully embeddable cloud-based software, accessible on mobile devices, desktop computers, or through virtual or augmented reality technology. The VR application used for this simulation workshop involved airway management of pediatric patients post-cleft palate repair.
BioDigital developed an interactive, multiuser simulation system using Autodesk Maya® (Autodesk, San Rafael, CA) for content creation and development of an intuitive user experience that minimizes onboarding time for inexperienced VR users. The development process began with designing a comprehensive storyboard, outlining every possible path within the decision tree to account for user interactions. The generated content was imported into the simulation environment, adding variables to relevant 3D tools and anatomical structures.
Each interaction was integrated into the decision tree system, providing users with real-time success or failure feedback. A physiology tracker algorithmically monitored and adjusted the simulated patient's vital signs based on user interactions. This dynamic aspect of the simulation facilitated more realistic and immersive training scenarios. To ensure optimal functionality in a multiuser context, there was real-time synchronization of decision trees and physiological responses across all user sessions.
Participants
A total of 26 medical students from a single institution completed the VR-based simulation workshop. 24 of the 26 students participated in this study prior to their clinical rotations in surgery and anesthesia. As learner understanding of airway procedures and techniques to manage surgical airways pre- and post-VR simulation was assessed, participants at the medical student level were selected as they are expected to have less familiarity with post-operative airway management prior to the workshop compared to trainees at the resident level. Informed consent was obtained from each participant prior to initiation of the workshop.
Virtual-Reality Simulation Workshop Organization and Design
After providing informed consent, participants completed a pre-intervention confidence survey (Supplemental Digital Content 1), followed by 10 min of standardized VR training by playing Beat Saber (Beat Games, Pod Klaudiankou, Prague) on VR headsets. The headset model used was Meta Quest 2 (Meta, Menlo Park, CA). Participants received a 5-min standardized discussion given by the cleft repair physician-trainer about general, pediatric, and post-cleft palate repair airway management. Participants were separately led to a different room with the same physician for the simulation. Participants were given a 2-attempt maximum for successful completion. Successful completion was defined by performing the necessary actions to re-establish a patent and functional airway in a patient after cleft palate surgery. The physician-trainer was present in the simulation to guide surgical tool manipulation and the decision-making process without explicitly providing correct next steps. All discrete steps of the procedures were tracked in the decision tree and were required to complete the procedure within the time allotted. If participants did not complete the actions in time, the virtual patient expired. Participants completed a post-intervention survey directly after the simulation (Supplemental Digital Content 2).
Simulation Decision Model
The simulation was held in a metaverse operating room (Figure 1), which could be accessed by multiple “players” at once and was recorded. Participants were instructed to enter the operating room with the cleft repair physician-trainer. Upon entering the metaverse OR, participants see simulation objectives, patient vitals, and a 4-min timer (Figure 1a). Participants were then oriented to the room, which contained a surgical table with a bag valve mask, laryngoscope, and orotracheal tube (Figure 1b). The patient was intubated and supine on the operating table. Upon participant confirmation of appropriate orientation to the environment, the simulation began.

Virtual operating room. (a) Learning objectives and vital signs. (b) Tray with instruments. (c) Manual ventilations with bag valve mask. (d) Placement of endotracheal tube.
The simulation utilized linear and parallel decision trees that together prevented participants from using tools that might break the simulation and allowed users to make instrument selections in any order at the appropriate time. Participants were expected to first extubate the patient by removing the orotracheal tube, beginning the 4-min countdown. Following extubation, oxygenation started to decline and heart rate increased. Moving from the least-invasive to most-invasive strategy, participants were expected to first attempt to properly position the patient using the head-tilt chin-lift method to restore upper airway patency from tongue occlusion of the glottis. When this failed and oxygen saturation dropped below 80%, the user could then perform 2 ventilations using a bag valve mask to provide non-invasive positive pressure ventilation or attempt re-intubation with laryngoscope and orotracheal tube. If a participant chose the bag valve mask first, the chest fails to rise on ventilation attempts (Figure 1c).
The participants then encountered resistance attempting to insert the orotracheal tube due to swelling of the airway (Figure 1d). After failing to achieve an airway, a long tongue stitch could be visualized and utilized to further retract the tongue, assisting with intubation and completing the simulation. If a participant's first session was not successfully completed within the allotted time, a second and final attempt would begin.
Data Collection and Surveys
Each participant was assigned a randomized ID number used to complete online deidentified pre- and post-surveys. The pre-survey is a psychometrically validated tool originally developed to gauge resident self-confidence during their surgical training, which was modified and abbreviated for our study. 22 It evaluated the use of VR as an educational tool, understanding of airway management of patients post-cleft palate repair, understanding of techniques to manage surgical airways, and whether VR should be incorporated into medical and surgical education. The survey scores were based on a 5-point Likert scale, with 1 being “strongly disagree” and 5 being “strongly agree”.
The post-survey consisted of the same pre-survey questions, assessing post-intervention confidence in simulation tasks, along with a modified version of the Student Evaluation of Educational Quality (SEEQ) survey (Supplemental Digital Content 2). The SEEQ survey is a validated instrument to assess tools of higher education by learners.23,24 The SEEQ survey asked students whether the VR-simulation workshop was stimulating, increased interest, allowed for better learning, was clear, effective in teaching, and whether they would recommend it to others. This portion of the post-simulation survey was also scored on the same 5-point Likert scale.
Data Analysis
SEEQ scores were evaluated using descriptive statistics. Pre- and post-workshop confidence survey responses were evaluated using a Wilcoxon signed-rank test. Data is shown as means and standard deviations where appropriate. Data analysis was performed using Graphpad Prism (Graphpad Prism, version 9.5.0, Dotmatics).
Results
Prior VR Experience of Participants
The majority of participants (96.2%) reported having minimal prior exposure to VR headsets, defined as having used them once or twice prior to the simulation workshop, while one participant (3.85%) reported using VR headsets at least once a month.
Pre- and Post-Intervention Confidence with VR Simulation
Pre- and post-intervention survey responses were linked through the randomly assigned ID numbers. In assessing their confidence in VR as an educational tool, participants started with a confidence score of 3.00 (2.00-4.00) (Figure 2). After the simulation, there was a statistically significant increase in median confidence score to 4.00 (4.00-5.00) (Figure 2). There were statistically significant increases in scores for understanding airway procedures from 2.00 (1.00-3.00) to 5.00 (4.00-5.00) and understanding techniques to manage surgical airways from 2.00 (1.00-2.235) to 4.00 (4.00-5.00) (Figure 2). Participants’ opinion on incorporating VR in medical and surgical education started high (4.00) and did not experience a statistically significant change following the workshop (4.00) (Figure 2). The majority of respondents (84.6%) completed the simulation in 1 attempt, 16.4% of respondents within 2 attempts, and no respondents were unable to complete the simulation.
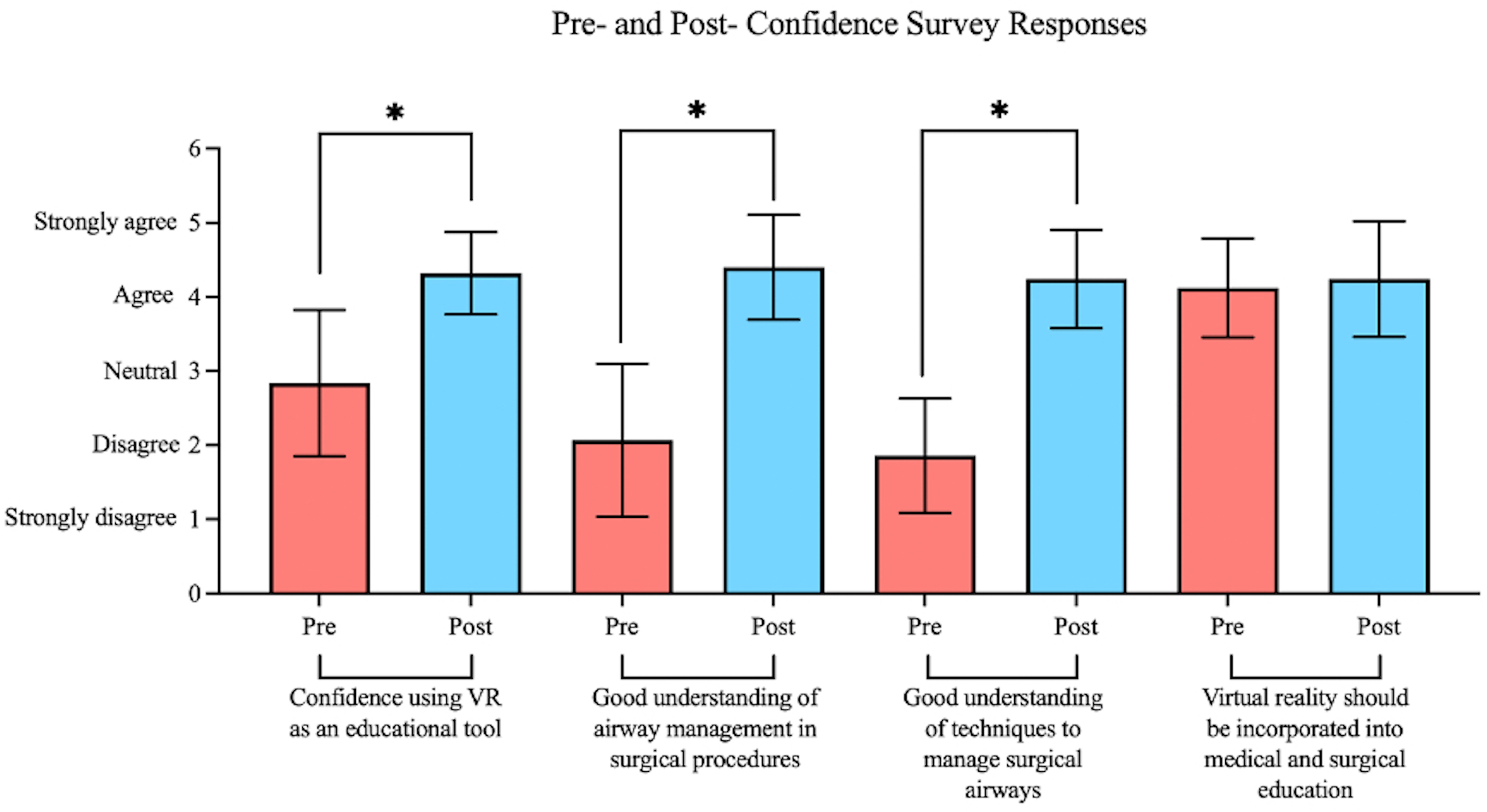
Pre- and post-confidence survey responses.
Evaluation of VR Educational Experience
In the SEEQ survey, participants demonstrated a high level of satisfaction with VR-based simulation as an educational tool for learning airway management of patients post-cleft palate repair. Participants agreed that the simulation was stimulating (4.31 ± 0.88), increased interest in the subject matter (3.77 ± 1.21), allowed for better learning (4.12 ± 1.05), was clear (4.15 ± 0.97), effective in teaching (4.08 ± 0.81), and they were likely to recommend it to others (4.2 ± 1.04) (Figure 3). Participants also largely agreed (4.27 ± 0.72) that they would feel comfortable doing the simulation again alone (Figure 3).
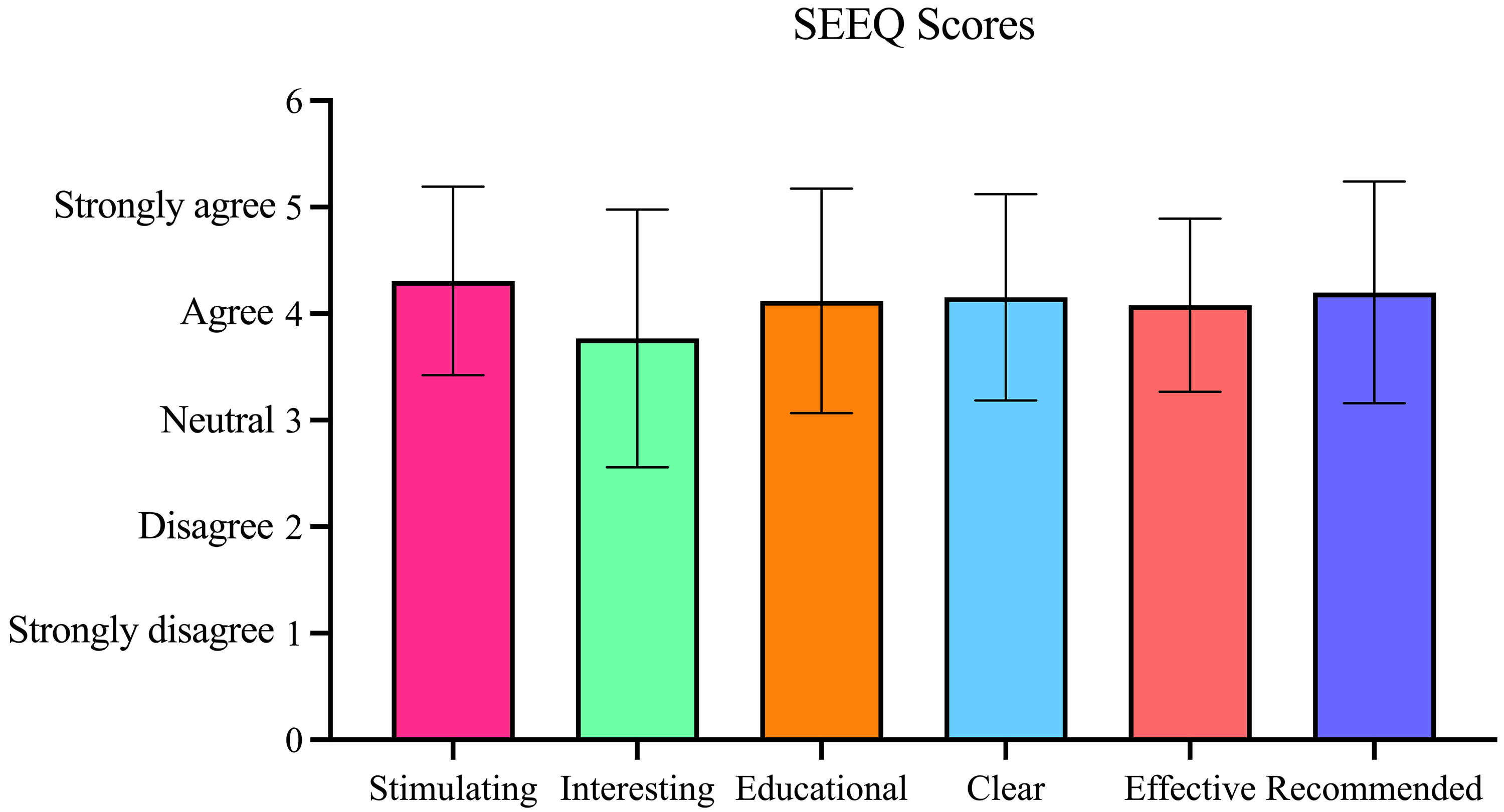
Student evaluation of educational quality (SEEQ) survey responses post-VR simulation.
Simulation Feedback
The majority of respondents (80.8%) reported no discomfort during the VR simulation. There were 2 (7.7%) reports of sweating, 1 (3.8%) report of nausea, and 1 (3.8%) report of “other” not further specified by the respondent. There was positive feedback on the VR technology itself, as respondents reported feeling “much more comfortable with the virtual reality” modality after the simulation and expressed excitement to “see how the technology gets implemented in the future for more complicated maneuvers/procedures.” Constructive feedback from participants included increasing the challenge level of the simulation, as well as the functionality of the technology to better “feel the supplies.” One respondent reported that the simulation did not offer additional educational value after the standardized talk with the cleft repair surgeon.
Discussion
This study shows that the VR simulation workshop was well-received as an educational tool by participants and was effective in increasing their confidence and improving skills in airway management of pediatric patients post-cleft palate repair. SEEQ survey mean scores demonstrated that participants somewhat to strongly agreed that the virtual-reality simulation model was stimulating, facilitated learning, was clear, was an effective means of teaching, and that they would recommend the model to others. Participants felt that they were neutral or somewhat agreed with the virtual learning model increasing interest in post-cleft palate repair airway management. Of note, participants somewhat to strongly agreed that they would feel comfortable doing the simulation alone following the guided learning. This efficient learning curve is an important benefit of this technology in medical and surgical education.
Following the completion of the virtual-reality simulation workshop, participants were significantly more confident using VR as an educational tool, had a significantly better understanding of airway management following surgical procedures, and had a significantly better understanding of techniques to manage airways of patients post-cleft palate surgery. Participants’ opinion that VR should be incorporated in medical and surgical education started high in the pre-survey and did not significantly increase after the simulation. These results demonstrate the broad acceptance of using virtual simulation models to supplement in-person learning. While this scenario of postoperative airway management may often be handled by the anesthesiology team, we feel that the emergent nature of this clinical situation warrants that surgical providers have an understanding of these skills. As our main objective was assessing trainee confidence with VR, our findings can be applied to developing future procedure-specific VR simulations targeted to surgical trainees.
The sphere of simulation-based training encompasses many modalities, including synthetic, animal models, cadavers, and the recent addition of virtual and augmented reality. As compared to other static learning models, virtual and augmented reality allows for complete user immersion in a complex clinical scenario where learners can practice real-time clinical decision-making. 10 Additionally, VR provides training with real-time exposure and peer feedback regardless of geographic location. This feature has particular relevance in remote and low-resource areas where educational and training resources, skills, and facilities may be limited.
Considering the technical difficulties innate to cleft repair operations, VR could increase resident surgical exposure in a safe and sustainable fashion, promoting patient safety. 25 This concept has been investigated in previous literature where VR implementation in surgical education was found to decrease the number of medical errors committed by residents, allowing for improved patient safety and surgical outcomes. 11 Ideally, VR simulations would be integrated early and throughout residency training, allowing for proficiency assessment when coupled with performance metrics and self-directed remote learning. This affords supervising surgeons increased confidence when delegating greater clinical responsibility to trainees. As the scope of surgical education is diminished by limited work hours, decreased trainee operative exposure and fewer opportunities to exercise autonomy in the operating room, comprehensive simulation modalities are vital to the state of surgical education. 26
From a global health perspective, the increase in morbidity and mortality risk in untreated cleft patients, 27 of which annual incidence exceeds 100 000 in low-resource regions, 28 highlights the importance of disseminating comprehensive cleft care education globally. It has been shown that one of the most pertinent barriers to cleft care education in low-resource regions is a limited number of practitioners with cleft care expertise. 21 Moreover, regions that experience cleft incidence as high as 9.31 per 10 000 births may be served by a single plastic surgeon.29,30 Importantly, these surgeons may not have undergone subspecialized training in cleft care.
Such discrepancies between incidences of oral clefts and specialized providers is exacerbated by limited financial resources. 31 Therefore, VR may present advantages to training in regions with a backlog of patients with clefts and limited cleft care education. 32 Multiple users from any region can interact in the metaverse, including leaders of cleft care education. This can significantly reduce the logistical and financial barriers associated with the traditional mission trip model and in-person simulation workshops in these regions. 24 Moreover, advancements in best clinical practices and/or guidelines can be provided as real-time updates to the simulations. As cleft care progresses, both high- and low-income countries can be privy to the same advances. Thus, VR simulations have the potential to become an integral component in cost-effective and equitable cleft education worldwide.
Our study demonstrated that even without significant prior experience, VR technology was easily learned and well-regarded by participants, suggesting that VR can be translated to low-resource settings with a high potential for user satisfaction. 33 Criticisms of the equitability of VR simulations include lack of financial resources and internet access for metaverse-based simulation models. However, traditional educational resources such as textbooks, peer-reviewed articles, and in-person lectures are often cost-prohibitive. The average price of a VR headset is $430, 34 which is more affordable than some smartphones. Additionally, recent United Nations reports have demonstrated an upward trend in internet accessibility among low- to middle-income countries. 35 Notably, all headsets in our study ran from a single smartphone hotspot, indicating that high-speed internet is not necessary for uninterrupted usage and sustained collaboration with other metaverse users.
This study has limitations. Data reported in this study are subjective, and future studies would benefit from objective measurements. While order and type of airway intervention in this operative scenario may vary across practitioners and institutions, simulations can be adjusted to suit local care protocols. Participants reported the simulation could be improved by increasing the difficulty level and enhancing the tactile functionality of the technology. Some participants felt they spent more time manipulating the instruments in the VR space than making clinical decisions. Unlike airway management in a real clinical setting, the decision tree in the model was linear. If participants made a wrong choice, they could not continue the specific task to see the repercussions. Furthermore, certain functions such as the visualization of the tongue stitch were only available after other steps had been taken with the purpose of placing emphasis on the utilization of the tongue stitch for completion of the simulation. It is important to note that given the complexity of this specific clinical situation, the study endpoints regarding learner understanding and techniques to manage surgical airways pre- and post-VR simulation should be interpreted as preliminary findings. BioDigital and Smile Train staff are actively collaborating to improve the decision-branching, difficulty, and tactile feedback. As study design was limited by a small sample size and being performed at a single institution, this report should be considered a feasibility study at this time. Limited prior VR exposure could have resulted in an inflated favorable participant opinion of VR as an educational tool. Additionally, the study consisted of a self-selecting non-randomized population who may have chosen to participate in a VR-specific intervention due to prior positive experience with VR. Furthermore, as this study was conducted in medical students, findings may not be generalizable to trainees at the resident or attending level. Therefore, in the future, we aim to assess the effectiveness of VR simulation for trainee learning through a randomized, multicenter-based study at various levels of medical training.
Conclusion
Virtual reality-based simulation workshops for surgical airway management can significantly increase a learner's confidence and skills in managing the airway of a pediatric patient post-cleft palate repair. Learners find VR training to be effective and recommend incorporating this type of educational tool in medical and surgical education. VR offers healthcare providers digital tools that have the potential to yield more equitable care, sustainable training practices, and high-quality training regardless of geographic location and access to resources. The platform provides a cost-effective, sustainable solution to enhance access to surgical training.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656241241128 - Supplemental material for Virtual Reality Simulation of Airway Management Post-Cleft Palate Surgery: A Model for Sustainable and Equitable Education
Supplemental material, sj-docx-1-cpc-10.1177_10556656241241128 for Virtual Reality Simulation of Airway Management Post-Cleft Palate Surgery: A Model for Sustainable and Equitable Education by Alexandra N. Verzella, Allison L. Diaz, Matteo Laspro, Andre Alcon, Jill Schechter, Aaron Oliker, Anne Arnold and Roberto L. Flores in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656241241128 - Supplemental material for Virtual Reality Simulation of Airway Management Post-Cleft Palate Surgery: A Model for Sustainable and Equitable Education
Supplemental material, sj-docx-2-cpc-10.1177_10556656241241128 for Virtual Reality Simulation of Airway Management Post-Cleft Palate Surgery: A Model for Sustainable and Equitable Education by Alexandra N. Verzella, Allison L. Diaz, Matteo Laspro, Andre Alcon, Jill Schechter, Aaron Oliker, Anne Arnold and Roberto L. Flores in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.