
Abstract
Objective
Cleft spectrum anomalies are sometimes associated with airway obstruction at birth. Modified delivery may facilitate advanced treatment, but there is insufficient data examining its use in patients with isolated cleft lip (iCL), isolated cleft palate (iCP), or cleft lip and palate (CLP). This study aims to address this gap.
Design
Deidentified birth hospitalization data were extracted from the Healthcare Cost and Utilization Project Kids’ Inpatient Database (2000-2019). Patients were identified using ICD codes and categorized as iCL, iCP, and CLP. Incidence, demographics, airway procedures on day of life (DOL) 0 or 1, complications, and survival were examined. The Rao-Scott chi-square test was used for comparison between unaffected and cleft spectrum groups.
Participants
The sample included 26 943 508 individuals, excluding out-of-hospital births, transfers, and individuals with cleft in association with mandibular anomalies or syndromic disorders.
Results
The weighted incidence for isolated cleft spectrum was 1.3 per 1000 birth visits. Airway intervention on DOL 0 or 1 occurred in 5.0% of the cleft group compared to 1.7% in the unaffected group (P ≤ .01). Preterm delivery occurred more frequently among patients with cleft spectrum but did not account for the elevated rate of airway intervention. Among individuals who received an airway intervention, hypoxic complications or mortality were more frequent in patients with cleft spectrum.
Conclusions
Individuals with isolated cleft spectrum experience higher rates of perinatal airway interventions with poorer outcomes than unaffected individuals. These findings may affect delivery planning, especially regarding the location and availability of neonatal services at delivery.
Keywords
Introduction
Cleft spectrum anomalies, which include conditions like cleft lip and palate (CLP), are common congenital malformations.1‐3 The adjusted prevalence of isolated cleft lip (iCL) in the United States is 1 in 1563, isolated cleft palate (iCP) is 1 in 2807, and CLP is 1 in 1687. 1 Approximately 70% of cleft anomalies are nonsyndromic and occur in isolation.2,4,5 Their presence is associated with both genetic and environmental risk factors.2,4,5 Cleft spectrum anomalies also occur in association with various genetic syndromes; common syndromes include Stickler syndrome, CHARGE syndrome, velocardiofacial syndrome, and Apert syndrome.2,4,6
The presence of iCL, iCP, or CLP is associated with increased airway obstruction, feeding difficulties, sleep-disordered breathing, and failure to thrive. 7 Usually, airway obstruction is due to structural abnormalities in the infant's oral or nasal passage. This can manifest as aspiration of fluids, airway collapse during sleep, and possibly life-threatening airway compromise.4,7 Preparation for these complications can often begin prenatally, as cleft spectrum anomalies are able to be detected before delivery. Cleft lip is frequently diagnosed via prenatal ultrasound; cleft palate is also potentially detectable, although it is more difficult.2,8,9 Historically, the limited prenatal detection of cleft palate has posed challenges for postnatal resuscitation planning and preparation, as unanticipated airway complications at birth may delay critical interventions and compromise early stabilization efforts. Fetal magnetic resonance imaging, however, can easily detect a cleft palate.9‐11
Other craniofacial anomalies, particularly those affecting the mandible, are often considered for delivery modification: delivery at a more resourced facility, predelivery mobilization/attended delivery, and ex-utero intrapartum treatment to expedite treatment initiation or the duration of airway attempts prior to hypoxic injury.11‐17 However, these delivery modifications are uncommon among individuals with cleft spectrum anomalies in the absence of micrognathia or a syndrome. 17
There are no studies investigating the frequency or type of airway intervention in patients with cleft spectrum anomalies immediately after birth and no guidelines for recommending delivery modifications in patients prenatally diagnosed with cleft anomalies. This study aims to compare birth hospitalization data and performance/type of airway intervention between individuals with a birth hospitalization discharge diagnosis (BHDD) of cleft spectrum anomalies and the general population to better inform delivery planning.
Methods
Study Design
We conducted a retrospective cohort study utilizing data extracted from the Kids’ Inpatient Database (KID) developed by the Agency for Healthcare Research and Quality as a part of the Healthcare Cost and Utilization Project (HCUP). This database is the largest publicly available pediatric inpatient care database, including around 3 million pediatric discharges representing all payers. 18 Sampling weights are created in the database based on survey design to allow for the calculation of national estimates. Each discharge record captures diagnosis and procedure codes for a given inpatient admission as defined by the International Classification of Diseases, Ninth and Tenth Revisions (ICD-9 and ICD-10, respectively) as well as demographics, hospital characteristics, charges, and length of stay.
Deidentified data were extracted between 2000 and 2019. Selection criteria included all birth hospitalization encounters of live and stillbirths. Out-of-hospital births and transfers were excluded. Data were reported as ≤11 hospital encounters (or masked in a frequency range) for cells containing 10 or less individuals, consistent with HCUP privacy policies. A certified professional coder assisted with code selection and verified that the ICD-9 to ICD-10 transition for each diagnostic category was accurate. The professional coder also assisted with the design of coding algorithm for the capture of appropriate individuals. Due to the deidentified nature of the data in the KID, this study was exempt from institutional review board review.
Exposure
After inclusion criteria were applied, individuals were divided into groups utilizing their BHDDs: iCL, iCP, CLP, and unaffected individuals. To isolate cleft spectrum anomalies from other syndromic causes of cleft lip/palate, ICD-9/10 codes identifying these diagnoses were excluded from this initial data grouping, as shown in Supplemental Material (Table SI). In addition, individuals with codes for micrognathia, agnathia, microstomia, syndromic micrognathia, and retrognathia were excluded. A noncleft group composed of patients lacking the predetermined ICD-9/10 codes was utilized as the control group, referenced as “unaffected” above.
Outcomes
The primary outcome was the incidence of cleft spectrum anomalies. Other outcomes included demographic information (sex, race, hospital, region), length of stay, total charges, disposition, mortality, perinatal airway procedure performance by type of intervention, airway procedure performance according to gestational age, complications, and survival. Airway procedure performance/interventions were included only if they occurred on day of life (DOL) 0 or 1. Airway interventions included nasopharyngeal airway, laryngoscopy/bronchoscopy, intubation, tracheostomy, extracorporeal membrane oxygenation, or cardiopulmonary resuscitation (CPR) (Table SI). The Rao-Scott chi-square test was used for statistical comparison between patients with any cleft anomaly (combining iCL, iCP, and CLP) and the unaffected group. The risk difference was used to further confirm the data had meaningful differences.
In addition, 2 variables were created to evaluate the potential need for medical intervention and the sufficiency of interventions performed in patients with isolated cleft spectrum anomalies. The potential need for medical attention was defined as patients who either received an airway intervention or did not receive an airway intervention and had a hypoxic complication (cardiac arrest, birth asphyxia, hypoxic–ischemic encephalopathy, anoxic brain damage, intraventricular hemorrhage or cerebral infarction) or mortality event. Intervention insufficiency was defined as patients who received an airway intervention and had either a hypoxic complication or mortality on day DOL 0 or 1. For this analysis, patients who underwent airway interventions were further subdivided into those who experienced no complications or mortality and those who did. While the term “insufficiency” is commonly used in neonatology to describe clinical conditions such as respiratory or placental insufficiency, in this context, we use “insufficiency” to characterize whether patients who required intervention exhibited higher rates of complications. The investigation of these 2 variables further describes the requirement for consideration of healthcare presence and intervention at the time of birth. They also help to identify rates of neonates who would benefit from a modification to the healthcare attention they already received, either in the form of the addition of an intervention or increased/differing support than what was provided.
Results
In total, there were 34,084 weighted BHDD of cleft anomalies or 1.3 per 1000. A higher percentage of patients with cleft spectrum anomalies were male compared to the unaffected group (57.0% vs 51.1%, P ≤ .01). ICL and CLP were more common in males (63.3% and 63.2%, respectively) while females were more commonly diagnosed with iCP (55.3%). A higher percentage of the affected cleft spectrum population were white (58.1% affected vs 52.8% unaffected, P ≤ .01) and were delivered at an urban teaching hospital (53.0% vs 51.5%; P ≤ .01). The median hospital length of stay was 1.9 days for the cleft cohort, with iCP and CLP having the longest length of stay (1.9 days). For unaffected patients, the median length of stay was 1.6 days. The cleft cohort was more likely to discharge to a short-term hospital (10.7% vs 1.5%, P ≤ .01) or another facility (1.3% vs 0.2%, P ≤ .01). Survival occurred in 99.7% of unaffected individuals, 98.4% of individuals with iCL, 97.1% of patients with iCP, 95.8% with CLP, and 96.8% with any cleft spectrum anomaly (Table 1).
Weighted Frequencies and Median Values of Demographic Variables of Interest.
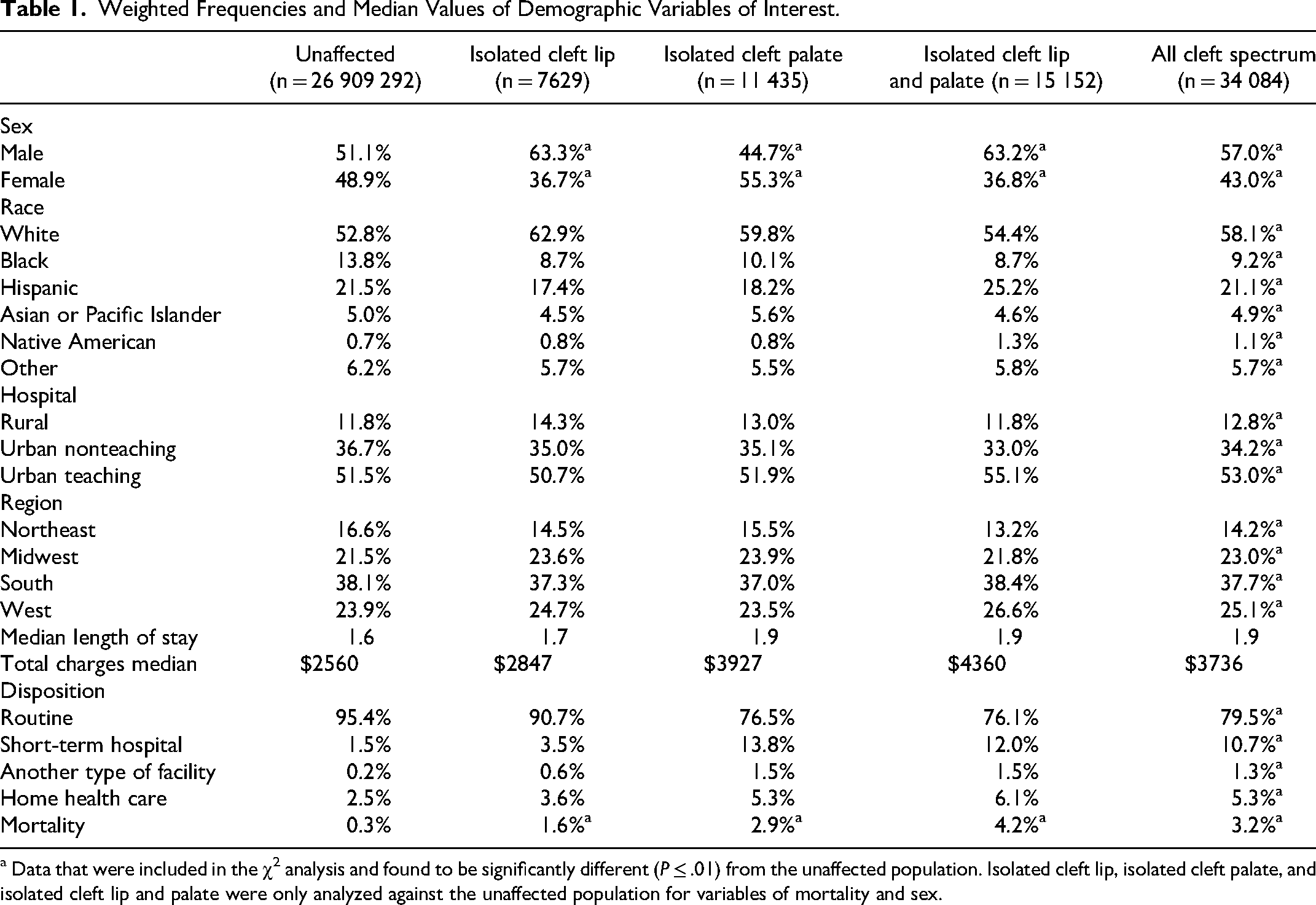
a Data that were included in the χ2 analysis and found to be significantly different (P ≤ .01) from the unaffected population. Isolated cleft lip, isolated cleft palate, and isolated cleft lip and palate were only analyzed against the unaffected population for variables of mortality and sex.
Airway intervention on DOL 0 or 1 occurred in 5.0% of the cleft cohort compared to 1.7% in the unaffected population (P ≤ .01). The iCP group had the highest rate of intervention (6.5%, P ≤ .01 relative to unaffected), followed by individuals with CLP (5.2%, P ≤ .01 relative to unaffected), and iCL (2.6%, P ≤ .01 relative to unaffected). Patients in the iCL group had the lowest intervention rate compared to patients with iCP or CLP. The most common intervention type among those with any cleft spectrum anomaly was intubation (4.8%) followed by laryngoscopy/bronchoscopy (0.3%). The highest rate of surgical airway performance occurred in individuals with iCP at 0.1%, while no tracheostomies were performed among individuals with iCL or CLP (Table 2). Cardiopulmonary resuscitation was also more frequent in the cleft cohort than in the unaffected population (0.2% vs 0.1%, P ≤ .01), with the highest rate of CPR in the iCP group (0.4%).
Weighted Intervention Rates.
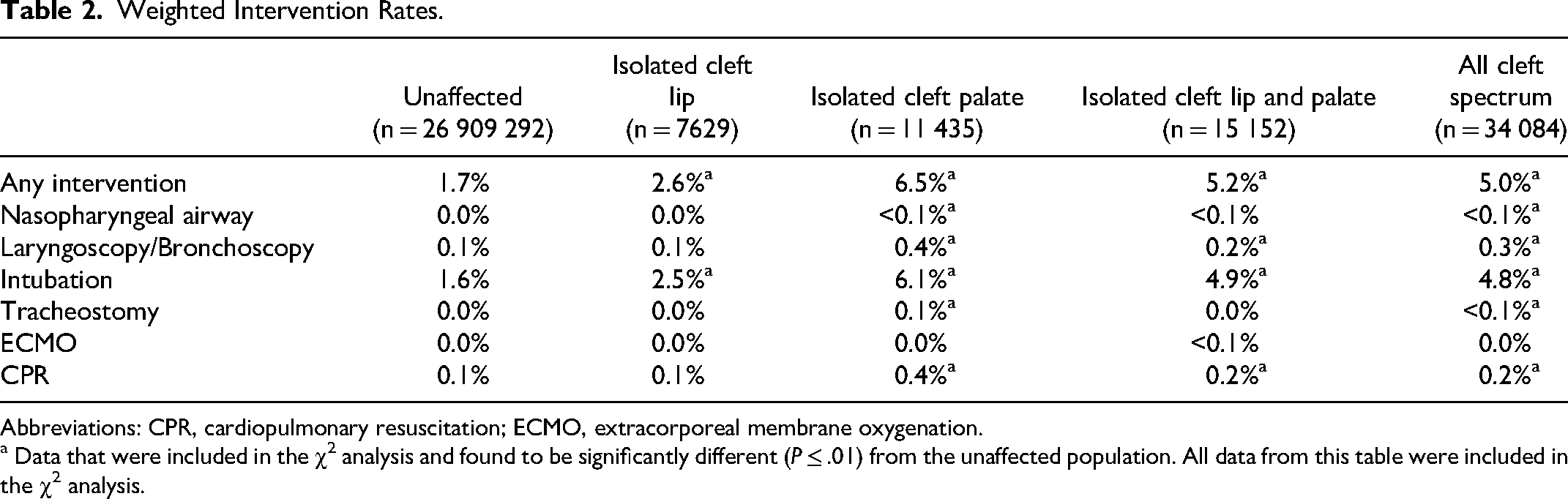
Abbreviations: CPR, cardiopulmonary resuscitation; ECMO, extracorporeal membrane oxygenation.
a Data that were included in the χ2 analysis and found to be significantly different (P ≤ .01) from the unaffected population. All data from this table were included in the χ2 analysis.
Patients with cleft spectrum anomalies had a higher complication rate than unaffected individuals (6.7% vs 2.4%, P ≤ .01). The 2 most common complications for all groups were acute respiratory distress/failure (10.1% in all cleft spectrum patients and 4.2% in unaffected patients, P ≤ .01), followed by cardiac arrest (4.8% vs 1.6%, P ≤ .01). All complications were more frequent in patients with cleft spectrum anomalies than unaffected individuals: hypoxic–ischemic encephalopathy (0.5% vs 0.3%, P ≤ .01), intraventricular hemorrhage or cerebral infarction (0.6% vs 0.3%, P ≤ .01), nervous system complication during/following procedures (<0.1% vs 0.0%, P ≤ .01), birth asphyxia (1.1% vs 0.4%, P ≤ .01), failure to thrive (0.3% vs <0.1%, P ≤ .01), surgical feeding access (<0.1% vs 0.0%, P ≤ .01), and pulmonary hypertension (0.2% vs < 0.1%, P ≤ .01). For the complications “anoxic brain damage” and “chronic respiratory distress,” we were unable to calculate statistical significance due to the affected patient sample size being too small. Within the cleft spectrum group, complications most frequently affected individuals with iCP, followed by CLP and iCL, respectively. When evaluating every complication, iCL had the lowest rates among the cleft groupings. Despite that, individuals with iCL still showed greater rates of acute respiratory distress/failure (5.8% vs 4.2% P ≤ .01 relative to unaffected) and cardiac arrest (4.3% vs 1.6%, P ≤ .01 relative to unaffected) than unaffected individuals (Table 3).
Weighted Complication Rates.
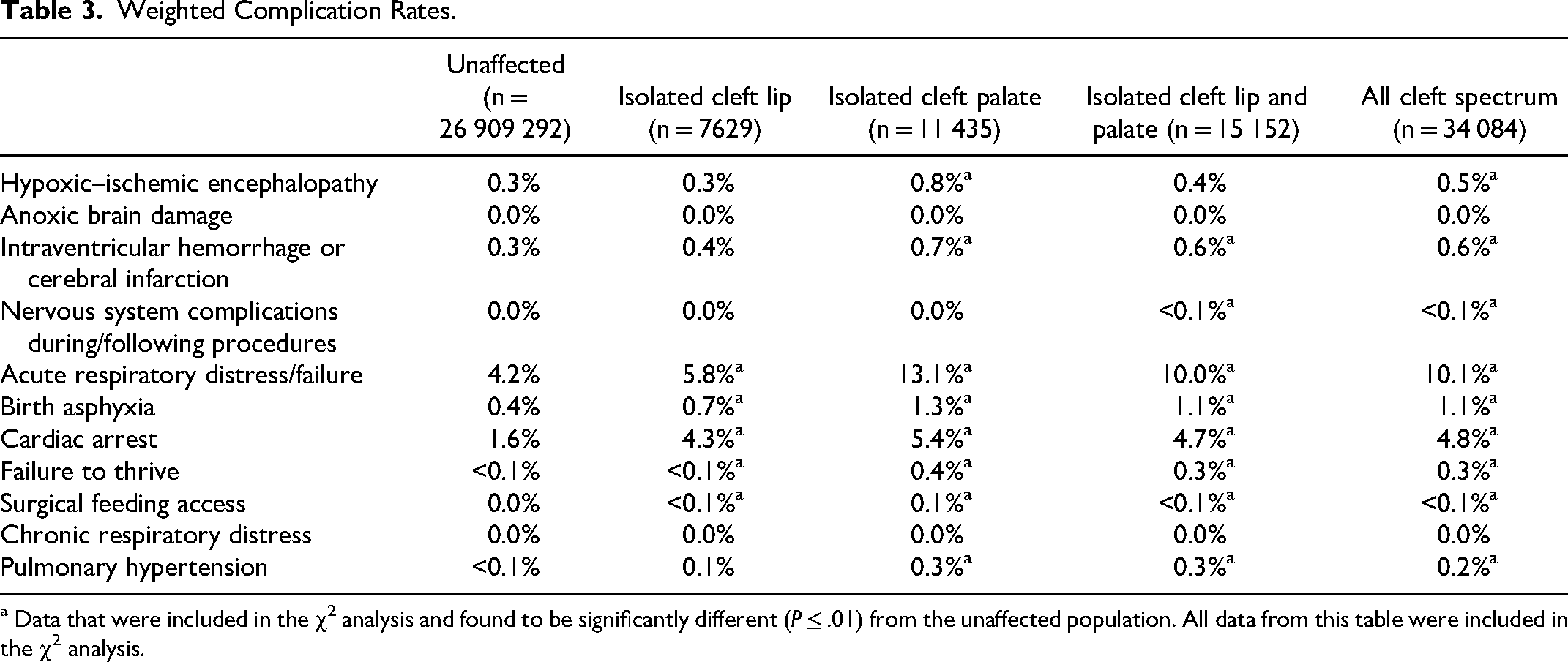
a Data that were included in the χ2 analysis and found to be significantly different (P ≤ .01) from the unaffected population. All data from this table were included in the χ2 analysis.
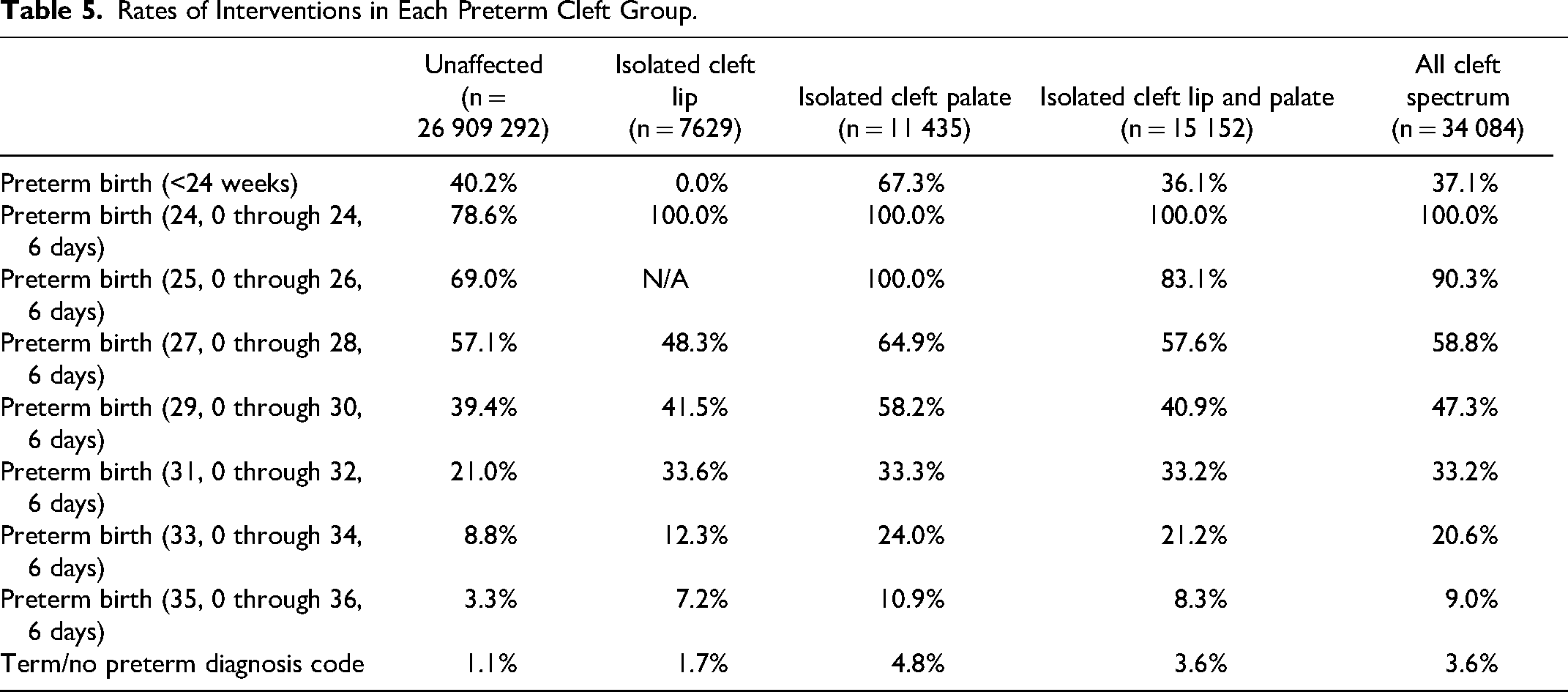
When assessing gestational age, 90.6% of the cleft cohort were born full term (greater than or equal to 37 weeks) compared to 94.3% of the unaffected population (P ≤ .01) (Table 4). When comparing full-term births only, 3.6% of the cleft cohort required an airway intervention, compared to 1.1% of the unaffected population. The higher rate of airway intervention among the cleft cohort was maintained at every assessed gestation age cohort other than <24 weeks gestation (Table 5). For example, intervention in preterm births (35, 0 through 36, 6) was 9.0% in patients with cleft spectrum compared to 3.3% in unaffected patients.
Weighted Incidence of Preterm Births by Gestational Age.
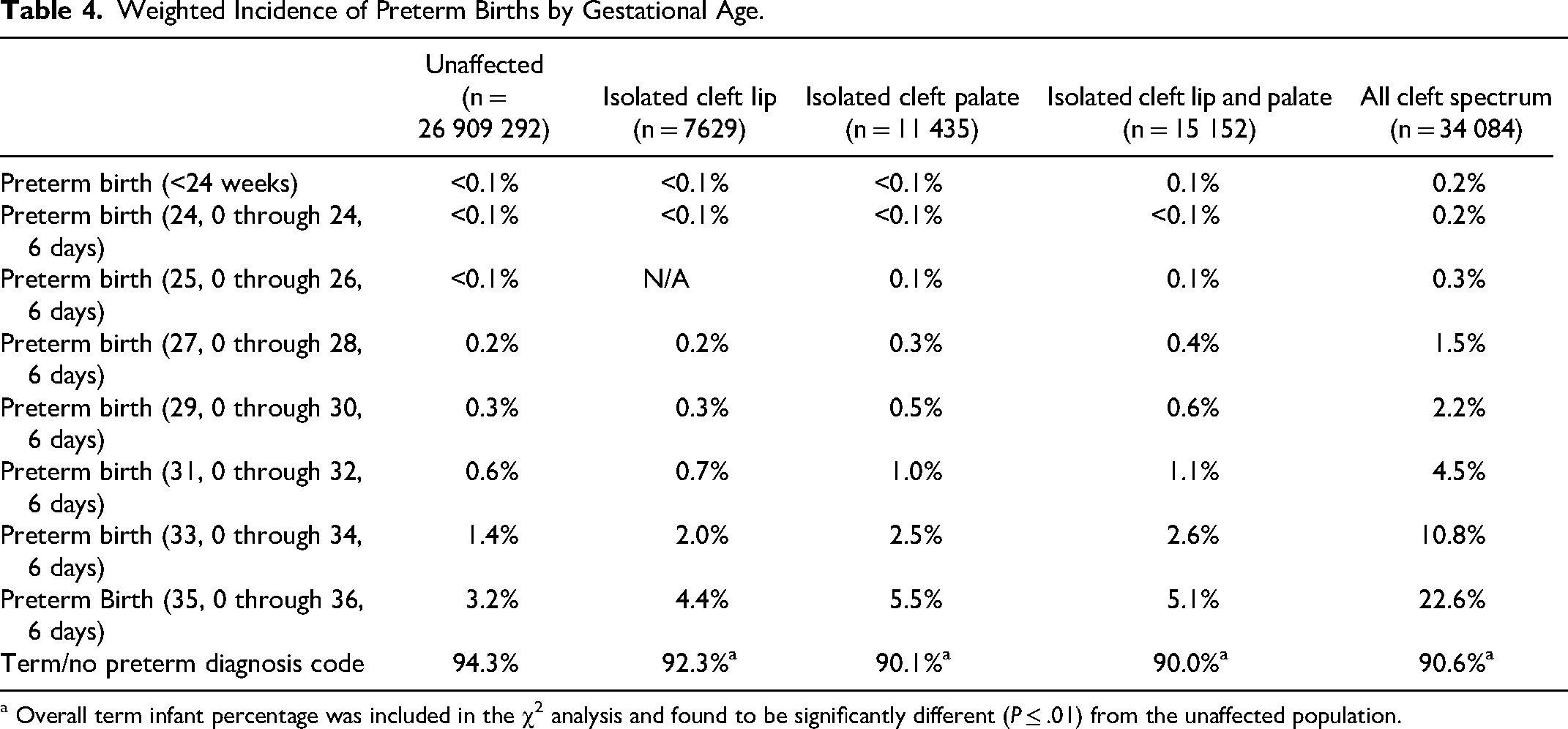
a Overall term infant percentage was included in the χ2 analysis and found to be significantly different (P ≤ .01) from the unaffected population.
Rates of Interventions in Each Preterm Cleft Group.
In patients with cleft spectrum anomalies, there was a greater potential need for medical attention, with 3.8% of unaffected individuals potentially needing medical attention, compared to 12.0% in all cleft patients (P ≤ .01). This was maintained across each phenotypic group with the lowest in individuals with iCL at 8.4% and 12.5% required among individuals with CLP and 13.6% among individuals with iCP (Table 6). The potential need for medical attention was greatest among individuals delivered at an urban teaching hospital (4.4% in unaffected and 13.8% in patients with cleft spectrum), followed by urban nonteaching hospital (3.3% in unaffected and 10.4% in patients with cleft spectrum) and lowest for rural hospital deliveries (2.5% in unaffected and 8.0% in patients with cleft spectrum). The trend of CLP and iCP having higher potential need for medical attention compared to iCL continued when looking at rural, urban nonteaching, and urban teaching hospitals.
Potential Need for Medical Attention and Insufficiency, Overall, and by Hospital Type.a
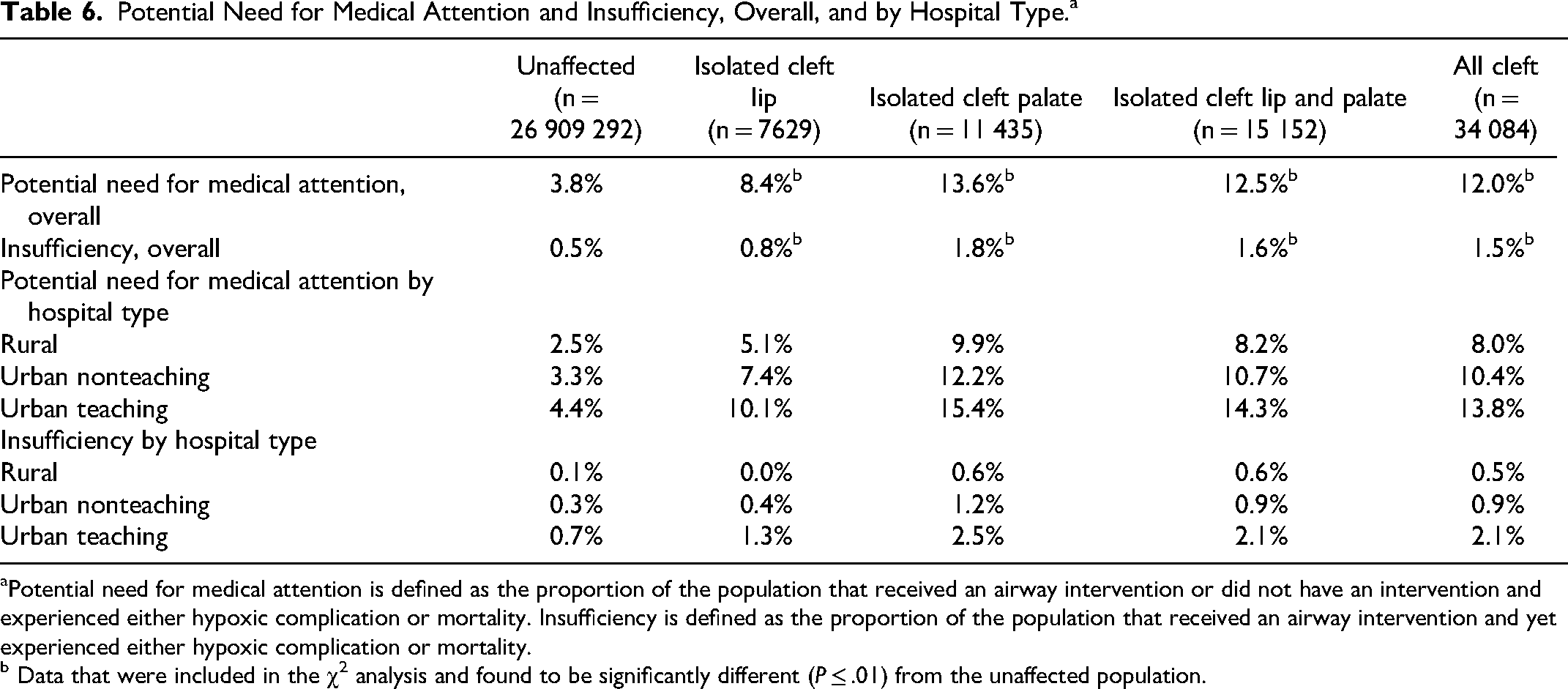
Potential need for medical attention is defined as the proportion of the population that received an airway intervention or did not have an intervention and experienced either hypoxic complication or mortality. Insufficiency is defined as the proportion of the population that received an airway intervention and yet experienced either hypoxic complication or mortality.
b Data that were included in the χ2 analysis and found to be significantly different (P ≤ .01) from the unaffected population.
Intervention insufficiency was also higher among patients with cleft spectrum changes (1.5% vs 0.5%, P ≤ .01). While the absolute rate of insufficient treatment to prevent hypoxic complications or mortality was greater at urban facilities, the odds ratio of intervention insufficiency was greater at rural hospital types (OR: 5 compared to unaffected) than at an urban nonteaching (OR: 3 compared to unaffected) and urban teaching (OR: 3 compared to unaffected) (Table 6).
Discussion
Our analysis identified 34 084 weighted individuals with cleft spectrum anomalies (1.3 per 1000 patients), which is lower than previously described data. 1 A contributing factor to this difference may be the exclusion of patients with micrognathia and other jaw and facial abnormalities from this study, as the purpose was to evaluate airway outcomes in individuals with isolated cleft spectrum anomalies. This was selected to inform delivery planning in a subset of the population suspected to be at lower risk than all individuals with cleft spectrum changes. Often, it is the association of cleft spectrum anomalies with other craniofacial anomalies such as micrognathia and glossoptosis that leads to concern for a reduction in airway size and acute requirement for intubation or tracheostomy at birth.6,7,10,11,17,19 Most other guidelines on the management of cleft spectrum anomalies emphasize a multidisciplinary approach in the weeks to months after delivery, with little guidance for the management of delivery itself and the immediate postpartum period.2,4,5,20,21
Other demographic data described in this study showed that neonates with cleft spectrum anomalies were more often male, apart from patients with iCP. This is consistent with other studies, which report that while infants with cleft palate are more often females, those affected by cleft spectrum as a whole (iCL and CLP) are predominantly male.4,22 Reasonings for this include a possible role of the female sex hormones and inheritance patterns.23,24 This study also found that patients with cleft spectrum anomalies were more often white, which also supports trends found in other studies.1,4 Additionally, patients with cleft spectrum were found to be more commonly delivered at an urban teaching hospital. Unfortunately, data on the pregnant person were not available in the KID database, so risk factors and genetic associations were unable to be evaluated. It is also notable in our data that the epidemiology varied according to the specific diagnosis (iCL vs iCP vs CLP).
This analysis identified higher rates of full-term births in the unaffected cohort compared to individuals with cleft spectrum anomalies. This aligns with previous research, and although the underlying reasons have not been fully explored, it is hypothesized that maternal factors and other genetic abnormalities may contribute.25,26 The analysis further revealed that, although patients within the cleft spectrum exhibited higher overall rates of preterm delivery, their intervention rates remained elevated across all gestational age cohorts when compared to the unaffected group. This suggests that earlier gestational ages do not entirely account for the increase in airway intervention. As discussed above, the KID database lacks information on the pregnant person and their prenatal course. Since preterm birth usually results from a combination of factors, such as preeclampsia, polyhydramnios, placental problems, and cervical insufficiency, we are unable to determine the exact reason for the preterm deliveries.
Airway interventions on DOL 0 or 1 were shown to occur more often in the cleft cohort, especially among patients with iCP and CLP, compared to unaffected individuals. Further analysis of the cleft spectrum group showed that those individuals also required overall higher rates of medical attention (those who either received an airway intervention or did not receive an airway intervention and had a hypoxic complication or mortality event) compared to unaffected individuals. Interestingly, these differences were found despite our exclusion of those with associated syndromes or micrognathia. This was lower, however, than the rates of performance of airway interventions and rates of requiring medical attention among individuals with cleft spectrum changes in association with micrognathia. 17 This would also be supported by previous studies that have focused solely on airway management in patients with cleft spectrum anomalies in association with other craniofacial anomalies.6,11,17,19
In addition, complications were more frequent among individuals with cleft spectrum changes than unaffected individuals. The data show that the complication rate remains higher for the group affected by cleft spectrum changes despite more frequent airway interventions. This suggests a potential opportunity to optimize delivery planning in cases of isolated cleft spectrum by considering delivery at hospitals equipped with appropriate neonatal services to manage potential birth complications. The most common complications were acute respiratory distress/failure and cardiac arrest, which occurred at the highest frequency in every group, including unaffected patients. However, cleft spectrum anomalies involving the palate (CLP and iCP) had complications occurring at an even higher frequency, suggesting that this population may require delivery in a setting with equipment and personnel to perform resuscitation in response to these complications. Notably, iCL has lower rates of both complications and interventions when compared to CLP and iCP, which indicates these patients may benefit from a shared decision-making model when considering where to deliver and with which modifications.
This study also examined the rates of medical attention and interventions based on hospital type (urban, urban nonteaching, and rural). The highest rates of medical attention and interventions were observed among individuals delivered at urban teaching hospitals. These centers often have multidisciplinary teams and specialized resources, which likely contribute to the increased use of interventions. Urban hospitals also tend to handle a higher volume of complex births and may receive referrals from rural hospitals. Furthermore, the study found that rural hospitals had higher odds of intervention insufficiency compared to both urban nonteaching and urban teaching hospitals, which is also likely related to resources and personnel availability. Rural prenatal outcomes may also be affected by access to prenatal care in rural communities and perinatal health behaviors related to social determinants of health. 27
This study has many limitations, one of which being the lack of information on patients delivered outside the hospital. There is no data included in the KID database that would allow easy comparison between outcomes in those who sought medical attention and those who did not. Furthermore, our study lacked access to individual patient charts, which impedes our understanding of healthcare decision-making. Similarly, there is no information available about the pregnant person, which prevents us from making meaningful connections between maternal comorbidities and other health/social factors that could change our understanding of intervention utilization.
Since this study is a retrospective database review, it also requires careful interpretation. Notably, not all hospitals provide complete data, and individual state processes for discharge reports vary, involving ICD codes for diagnoses and procedures. The lack of granularity with regard to coding procedures also limits this study's ability to report on the type of cleft. Finally, when evaluating significance levels for the χ2 test, it is notable that our sample size among the unaffected population was extremely large, which can result in statistically significant differences between groups even when these differences are minimal. This can complicate the interpretation of results, as small effects may appear significant due to the increased precision afforded by a large sample size.
Conclusion
Cleft spectrum anomalies are common congenital anomalies that were previously known to increase neonatal risk for many complications. This study has highlighted both the risk for hypoxic complications and increased utilization of airway interventions. These findings suggest there is potential benefit in consideration of airway management and delivery at a location with access to appropriate neonatal services. While modified delivery may not be right for every case of isolated cleft spectrum, it is useful to have an open-ended discussion to consider risks and benefits and may be helpful when deciding on a recommendation as a provider.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656251350597 - Supplemental material for Perinatal Airway Risk for Individuals With Isolated Cleft Spectrum
Supplemental material, sj-docx-1-cpc-10.1177_10556656251350597 for Perinatal Airway Risk for Individuals With Isolated Cleft Spectrum by Johanna L Ellefson, Samantha J Barr, Maya N Matabele, Sabrina X Huang, Gisselle A Garcia, Elle C Nuttall, Manasa Venkatesh, Inna M Lobeck, Deborah Kacmarynski and Michael D Puricelli in The Cleft Palate Craniofacial Journal
Footnotes
Ethical Approval and Informed Consent Statements
An ethics statement was not required for this study as it is based exclusively on data extracted from the Healthcare Cost and Utilization Project Kids Inpatient Database.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the NIH-funded T32 Voice Research Training Grant (T32DC009401, 5 T32 DC 9401-15).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available upon reasonable request from the corresponding author. The data are available for purchase from the United States Department of Health and Human Services’ Healthcare Cost and Utilization Project, Kid's Inpatient Database.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.