
Abstract
Aims
To provide an overview of the Cleft Outcomes Research NETwork (CORNET) and the CORNET Speech and Surgery study. The study is (1) comparing speech outcomes and fistula rate between two common palate repair techniques, straight-line closure with intra-velar veloplasty (IVVP) and Furlow Double-Opposing Z-palatoplasty (Furlow Z-plasty); (2) summarizing practice variation in the utilization of early intervention speech-language (EI-SL) services; and (3) exploring the association between EI-SL services and speech outcomes.
Design
Prospective, longitudinal, observational, comparative effectiveness, multi-center.
Sites
Twenty sites across the United States.
Participants
One thousand two hundred forty-seven children with cleft palate with or without cleft lip (CP ± L). Children with submucous cleft palate or bilateral sensorineural severe to profound hearing loss were excluded from participation.
Interventions
Straight-line closure with IVVP or Furlow Z-plasty based on each surgeon's standard clinical protocol.
Main Outcome Measure(s)
The primary study outcome is perceptual ratings of hypernasality judged from speech samples collected at 3 years of age. Secondary outcomes are fistula rate, measures of speech production, and quality of life. The statistical analyses will include generalized estimating equations with propensity score weighting to address potential confounders.
Current Progress
Recruitment was completed in February 2023; 80% of children have been retained to date. Five hundred sixty two children have completed their final 3-year speech assessment. Final study activities will end in early 2025.
Conclusions
This study addresses long-standing questions related to the effectiveness of the two most common palatoplasty approaches and describes CORNET which provides an infrastructure that will streamline future studies in all areas of cleft care.
Introduction
Cleft palate, with or without cleft lip (CP ± L), is one of the most common birth defects, 1 impacting speech, hearing, dentition, health, and quality of life. Children with CP ± L undergo numerous surgical, orthodontic, and behavioral interventions; yet, due to the lack of a strong evidence-base, there is still much debate about which approaches are the most effective across the many domains of cleft care.2–5
Multi-site inter-center comparisons (eg, Eurocleft, 6 CSAG 7 ) and randomized controlled trials (RCTs) (Scandcleft, 8 TOPS 9 ) carried out primarily in Europe have provided valuable information resulting in changes in treatment of children with cleft palate. However, these types of research collaborations have been slower to develop in the United States (US). The Americleft Project was modeled after Eurocleft and included a group of clinical researchers from orthodontics, speech-language pathology, surgery, psychology, pediatrics, and social work, representing 30 cleft palate teams across North America. Building on the collaborations formed in Americleft, 10 a team of multidisciplinary researchers and clinicians began working together in 2016 to create a new national cleft outcomes research network and the comparative effectiveness study to be described here. This project was funded by the National Institutes of Health-National Institute of Dental and Craniofacial Research (NIH-NIDCR) in 2018. The Cleft Outcomes Research NETwork (CORNET) was created to streamline the design and implementation of outcome studies across all disciplines of cleft care while also creating a sustainable model for future research in cleft palate. This paper describes a study of speech and surgical outcomes that forms the basic infrastructure for CORNET. The study to be described here is the CORNET-Speech and Surgery Study (SSS).
Study Rationale
Comparison of Palatoplasty Approaches
Cleft palate repair (eg, palatoplasty) is performed to close the abnormal connection between the oral and nasal cavities and to enable normal speech development. Despite the common objectives agreed upon by all surgeons, there is variability in both the surgical procedure used and the outcomes achieved. The most commonly employed palatoplasty approaches are straight-line closure with intra-velar veloplasty (IVVP) and Furlow Double-Opposing Z-plasty (Furlow Z-plasty).11–14 While both approaches involve reconstruction of the levator muscle sling, it has been suggested that the Furlow technique “has the advantage of lengthening the velum, avoiding overlap between the oral and nasal mucosal incisions, optimizing the vascularity of both the mucosal and muscular layers and reconstruction of the functional levator veli palatini sling.” 13 (pp1014-1015) A systematic review conducted by Timbang and colleagues 13 comparing these two approaches concluded that children with unilateral cleft lip and palate had a greater chance of needing secondary surgery following a straight-line closure with IVVP compared to those treated with a Furlow Z-plasty. However, confidence in the findings of this review was substantially weakened by the lack of rigorous comparative studies; the literature on this topic consists of retrospective, single-center reports (see Timbang et al, 2014) 13 and a methodologically flawed Randomized Controlled Trial (RCT).14,15 The weak evidence suggesting better speech outcomes with Furlow palatoplasty is offset by a weak body of evidence suggesting that the Furlow technique is associated with a higher incidence of oronasal fistulae, especially for wider clefts.14,16–17 This finding was not supported by other investigations,18–21 including two meta-analyses performed as part of systematic reviews.13,22
Data collected on surgical practice patterns from various sources (see Katzel et al, 2009; Kearney et al, 2020)11,12 reflect equipoise among surgeons regarding the superiority of one surgical approach over another. Due to conflicting findings (summarized above) and the absence of standard practice guidelines, surgical decision making is driven by each surgeon's interpretation of the available evidence, their training, and their experience. In this context, an observational comparative effectiveness study can provide convincing evidence to resolve the uncertainty around this issue.
Randomized Controlled Trials and Comparative Effectiveness Research
Randomized controlled trials (RCTs) are thought to provide the highest level of evidence for determining best treatments. 23 RCTs, especially in surgery, are challenging to conduct because of issues related to cost, equipoise, blinding, the learning curve associated with replication of a specific technique across clinician-investigators, and lack of confidence in research findings by clinicians and patients.24–27 RCTs have also been criticized for problems with external validity, that is, can the findings be generalized to patients in clinical practice settings (see Rothwell, 2005). 28 More recent reports comparing RCTs and well-designed observational studies found no difference between the two designs in treatment effects for a variety of clinical conditions.29–33
As an alternative to RCTs, comparative effectiveness research (CER) designs have been proposed as a way to remove clinical uncertainty and achieve better clinical outcomes by comparing treatments in “real-world” settings as part of routine clinical care.34–37 The CER methodology described here was designed to counter bias and confounding factors associated with nonrandom assignment; a purported weakness of CER studies. 34 To this end, data are being collected on important variables that may impact outcomes such as (1) patient characteristics (eg, cleft type, measurements of cleft with and length, age at repair, syndrome status); (2) surgeon characteristics (eg, specialty training, years in practice, number of palate repairs in a one year period); and (3) variation in surgical technique (eg, soft palate nasal mucosal closure technique, soft palate oral mucosal closure technique, levator muscle repair technique). These and other variables will be accounted for with robust statistical methods (eg, propensity weighting and sensitivity analyses) as an alternative to randomization.
The Cornet-SSS methodology was designed to overcome the primary flaws of the only RCT comparing straight-line closure with IVVP and Furlow Z-plasty, 14 which included the use of an unvalidated non-speech task to assess speech, issues related to randomization and lack of fidelity of the surgical approaches by some surgeons, and lack of control of surgical skill and experience in the analyses. A valid and reliable measure of speech outcome, the Cleft Audit Protocol for Speech-Augmented-Americleft Modification (CAPS-A-AM) was adapted from the Cleft Audit Protocol for Speech-Augmented38,39 and tested in the Americleft Speech Project. 40 Instead of asking surgeons to adopt a specific or new palatoplasty approach that may or may not be part of their typical clinical practice/protocol, the CER design allows them to “do what they would typically do” for each patient. Finally, this study design attempts to address other weaknesses in the literature by (1) improving representativeness, external validity, and power by recruiting a large number of participants from geographically diverse centers across the US; (2) developing (together with the participating surgeons and speech-language pathologists) detailed and standardized forms to document interventions along with explicit training on the completion of these forms; and (3) employing extensive quality control measures to ensure the reliability and validity of the data.
Impact of Speech/Language Intervention on Speech Outcome
Following palatoplasty, children with CP ± L often exhibit speech problems. Some of these are delays in the acquisition of speech sounds, whereas others reflect the early influence of clefting and/or velopharyngeal dysfunction. Children with CP ± L are also at risk for language delay,
41
especially those with associated syndromes.42–45 Because of the impact of poor speech and language skills on intelligibility, socialization, self-concept,46–48 and early reading success,
49
many have advocated for parent coaching and early intervention focused on speech-language skills to circumvent the development of atypical speech errors
50
and to ensure that age-appropriate speech-language skills are present when children enter kindergarten.46,51–54 The Americleft project found that normal speech by the start of kindergarten is not the norm for the majority of children with CP ± L, as 69% of 5- and 6-year-olds still exhibited speech sound disorders
55
based on the Goldman-Fristoe Test of Articulation-2.
56
This is considerably higher than what was reported for a comparison group without clefts (24% occurrence) or for the occurrence of hypernasality, which was only 22% in the same population of children with CP ± L.
55
While additional surgical intervention is needed to treat hypernasality, effective speech/language intervention has been shown to improve articulation and/or language abilities of children with5,57,58 and without cleft palate.
59
Although children with CP
Four systematic reviews examining speech/language intervention in children with cleft palate varied in the strength of their support for the overall benefits of intervention.5,57,58,61 However, they were unanimous in their call for more research, employing stronger methods and greater scientific rigor.5,57,58,61 While a number of intervention studies have been published recently,62–68 including several RCTs,63,65–67 there are still many unanswered questions related to which approach and/or service delivery model is most beneficial for which children, optimal age for initiation of services, and more.5,61 Finally, there is little or no data available about current speech/language intervention practice patterns for children with CP ± L, such as factors which may influence access, utilization, and type of services delivered, including socioeconomic status, race, and primary language spoken in the home, etc. These factors have recently been shown to significantly influence access to services, and potentially, outcomes for other populations of children with speech-language impairments 69 but have not yet been studied in children with CP ± L in the US.
Speech/language and surgical interventions contribute to the speech outcome of children with CP ± L. Therefore, the CORNET-SSS is also collecting data on the wide variety of speech/language interventions the children are receiving during the study period; specifically focused on early intervention services as the children are followed from pre-palatoplasty until 3 years of age. These preliminary data will direct us to the most important variables to investigate and/or provide pilot data for a large-scale study assessing the impact of early speech/language intervention on communication skills of young children with CP ± L in the future.
Study Aims
To compare the speech outcomes and fistula rate of two common palate repair techniques, straight-line closure with IVVP and Furlow Z-plasty.
To summarize current practice variation in the utilization and type of early intervention-speech/language (EI-SL) services accessed by children with repaired CP ± L and describe the association of EI-SL services with speech outcomes.
Table 1 shows the study aims, primary and secondary objectives, associated hypotheses, outcome measures, and covariates.
Primary and Secondary Study Objectives, Hypotheses, Outcome Measures, and Covariates.
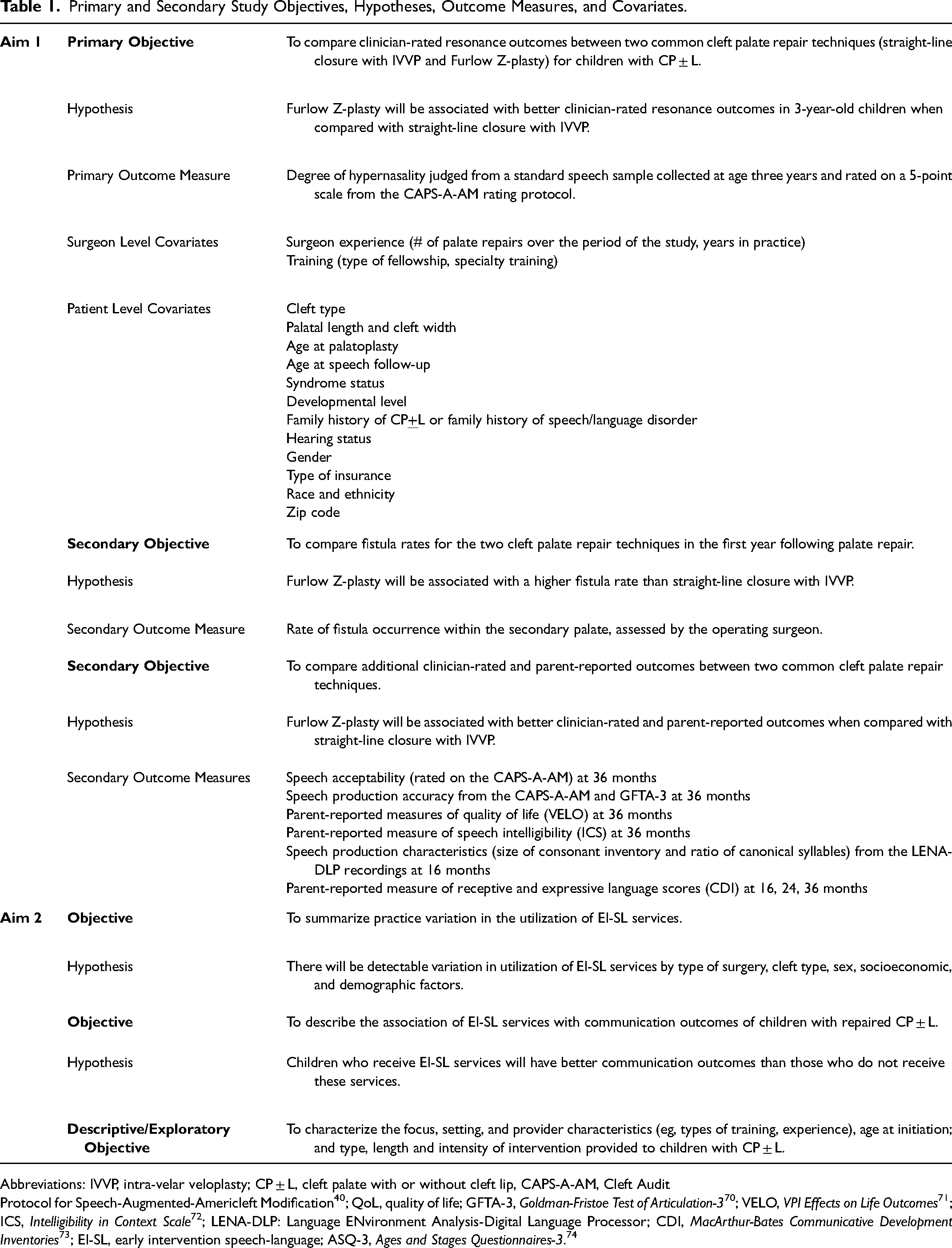
Abbreviations: IVVP, intra-velar veloplasty; CP ± L, cleft palate with or without cleft lip, CAPS-A-AM, Cleft Audit
Protocol for Speech-Augmented-Americleft Modification 40 ; QoL, quality of life; GFTA-3, Goldman-Fristoe Test of Articulation-3 70 ; VELO, VPI Effects on Life Outcomes 71 ; ICS, Intelligibility in Context Scale 72 ; LENA-DLP: Language ENvironment Analysis-Digital Language Processor; CDI, MacArthur-Bates Communicative Development Inventories 73 ; EI-SL, early intervention speech-language; ASQ-3, Ages and Stages Questionnaires-3. 74
Methods
Study Overview
This is a multi-center, prospective, longitudinal, observational comparative effectiveness study of speech and surgical outcomes. The study participants (target enrollment = 1231 children with CP ± L) are enrolled prior to primary palatal surgery (approximately 8 to less than 30 months) and followed until 3 years of age. The palate repair and surgical follow-up occur following each surgeon's standard clinical protocol. The surgical approach chosen by some surgeons is based on cleft severity/cleft type, while other surgeons employ the same approach (either straight-line/IVVP or Furlow Z-plasty) regardless of the type or severity of the cleft. Variability in treatments and participants are both anticipated and desirable and will be utilized as covariates in statistical analyses to determine their effects on outcomes. Data collection occurs at: enrollment, palatoplasty, post-palatoplasty follow-up, 16 months, 24 months, and 36 months of age. When possible, these data collection points coincide with regularly scheduled clinic visits. Study procedures are outlined in Figure 1.
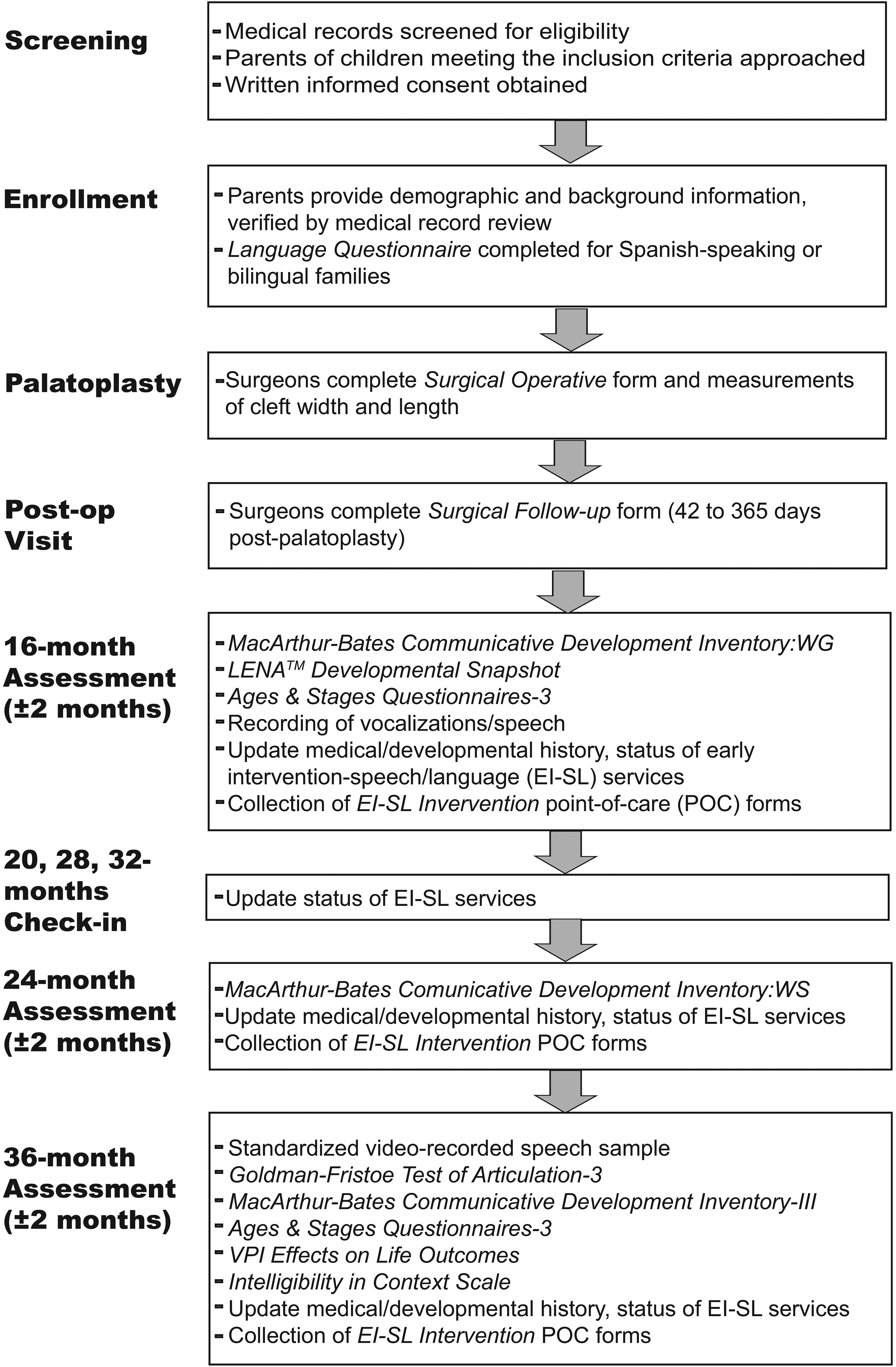
Flowchart of study procedures and data collected.
Development of Data Collection Instruments
Prior to the onset of study recruitment, the study surgeons and speech-language pathologists (SLPs) met in person and/or via multiple conference calls to develop the point-of-care (POC) data collection instruments. Surgeons created three surgical POC forms: the Standard Surgical Practice form, the Surgical Operative form, and the Surgical Follow-up form. The Standard Surgical Practice form obtains information about the surgeon's training and post-operative practices. The Surgical Operative form obtains information that will be used for classifying surgical technique including those elements that differentiate straight-line/IVVP and Furlow Z-plasty or that may contribute to the technique's effectiveness as well as other important aspects of the surgery:
Cleft type and cleft anthropometrics (eg, cleft width at the posterior edge of the hard palate shelves, width of the hard palate at the posterior edge, and palatal length);
75
Technique of mucosal incision, muscle dissection, and mucosal closure (eg, soft palate nasal mucosal closure technique, soft palate oral mucosal closure technique, levator muscle repair technique, use of myomucosal flaps or buccal fat pad flaps to augment closure, use of dermal or submucosal matrices to augment mucosal repair); Components that may contribute to the surgery's effectiveness (eg, length of muscle overlap, use of relaxing incisions); Details of antibiotic, corticosteroid, and local anesthesia use; length of surgery; estimated blood loss, etc.
A third form, Surgical Follow-up, documents postoperative complications (eg, presence of an oronasal fistula, prolonged hospitalization, or readmission). As a part of each site's launch, one of the surgeon co-investigators reviews the three surgical forms, including the cleft measurements and fistula documentation, with the site study team before the start of data collection. These forms are available from the first author upon request.
SLPs created two EI-SL forms: the EI & SLP Provider Characteristics form that records information about the providers’ discipline, education and work history, and language status; and the EI-SL Intervention form to document speech/language interventions that the children are receiving. These forms are available from the first author upon request.
The EI-SL Intervention POC form includes:
The profession of the specific provider (eg, speech-language pathology, physical therapy, occupational therapy); Where the intervention is carried out (eg, home, outpatient hospital/clinic, telehealth); Amount of intervention the child is receiving (frequency and duration of sessions); Level of parent involvement (eg, parent participated in the session, parent observed the session); Details about areas addressed in intervention (eg, communication precursors, expressive language, speech articulation); The specific goals targeted and the techniques used (eg, for children working on speech: specific sounds targeted and the therapy model being used).
The professionals involved in the development of these POC documentation forms used their clinical knowledge and the literature to provide a comprehensive list of data elements for all forms. The final list of data elements for all POC forms was reviewed by the study surgeons or SLPs, depending on the form. Paper versions of the forms were piloted at the two earliest launched sites prior to study-wide distribution, training on form completion, or development of the REDCap version of the forms. EI-SL forms were trialed by SLPs using de-identified data from early intervention providers and speech therapy notes before forms were used for prospective data entry. Revisions made prior to study-wide distribution included clarifications, qualifications, or reforming of questions, formatting issues, etc. rather than changes in the actual data elements. Trainings are provided to all study staff to promote valid and reliable form completion.
To streamline the process of data collection for surgeons and EI-SL providers, the forms were designed so they could be completed in under five minutes and are available electronically (via REDCap,76,77 see description in
Study Sites
The study data collection sites are 18 diverse (geographically, ethnically, racially, linguistically) children's hospitals/cleft palate teams across the US. One site was unable to continue participation due to complications related to the COVID pandemic, leaving 17 sites contributing data for the primary study outcome at 3 years of age. All teams are approved by the Commission on the Approval of Teams of the American Cleft Palate-Craniofacial Association and affiliated with academic institutions. The hospitals/teams chosen represent diversity in the characteristics described above, vary with regard to surgeon practice patterns for straight-line closure with IVVP vs. Furlow Z-plasty and volume of patients seen, and have a research infrastructure. The University of Utah (UU) is the lead coordinating site for collection, aggregation, and analysis of data from all sites. The University of Wyoming (UWY), Nationwide Children's Hospital (NCH) and Phoenix Children's Hospital (PCH) are data analysis sites. The list of study sites can be found in Table 2.
CORNET Sites.
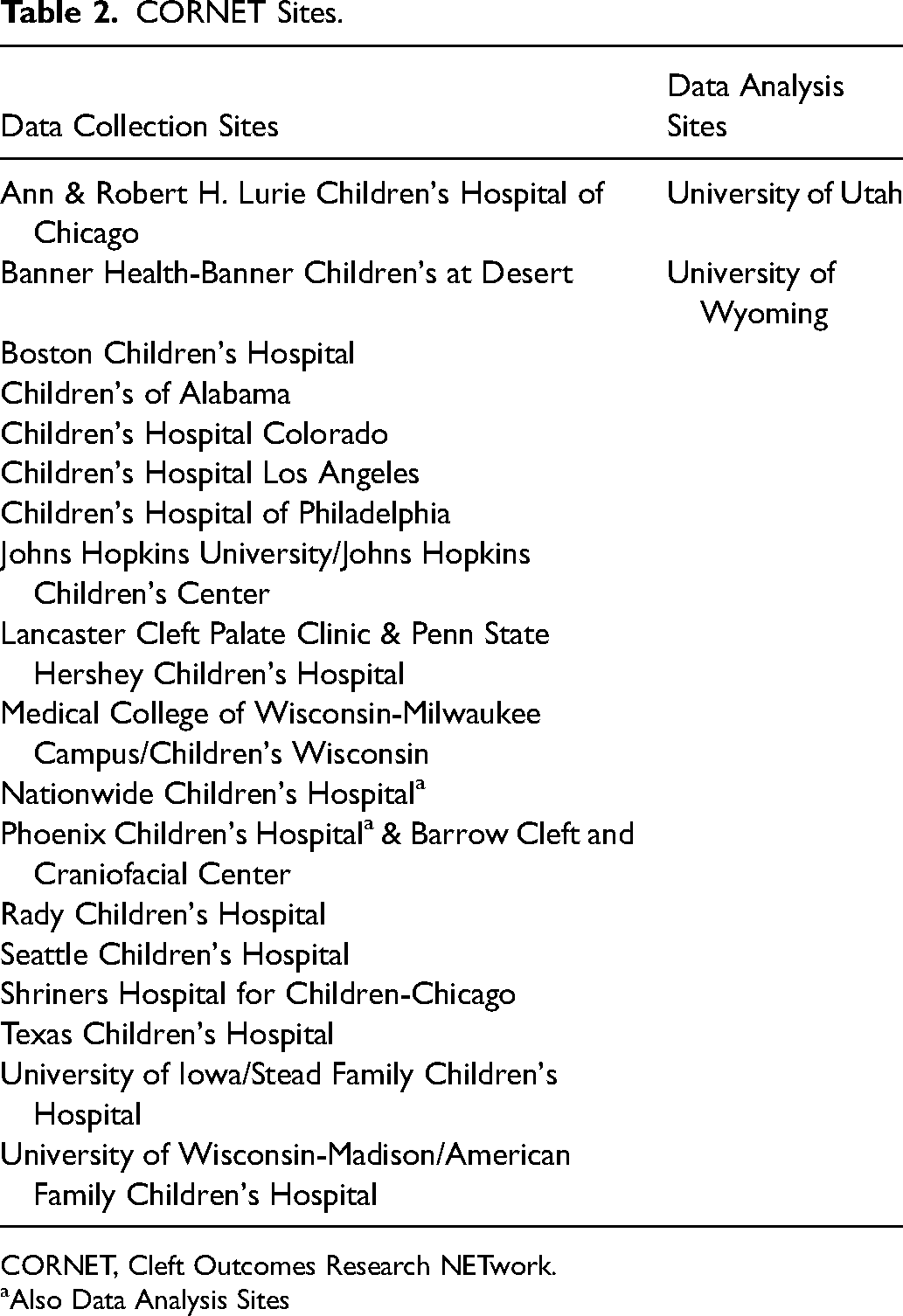
CORNET, Cleft Outcomes Research NETwork.
Also Data Analysis Sites
Recruitment and Study Participants
The study was reviewed and approved using a Single Institutional Review Board (SIRB) model with the UU as the Institutional Review Board of record (IRB#00105205). In-line with federal laws and regulations and NIH policies, written informed consent is carried out prior to the start of any study procedures. Children are recruited from the hospitals/cleft palate teams listed in Table 2. Potential participants are identified by the study staff from team records, clinic schedules, and surgical schedules. All parents of children who meet the inclusion criteria but not the exclusion criteria, as shown in Table 3, are invited to participate. Recruitment is typically carried out at a regularly scheduled clinical visit at the enrolling sites; since the COVID-19 pandemic, recruitment and consenting can be conducted remotely (telephone, Skype, Zoom).
Inclusion and Exclusion Criteria.
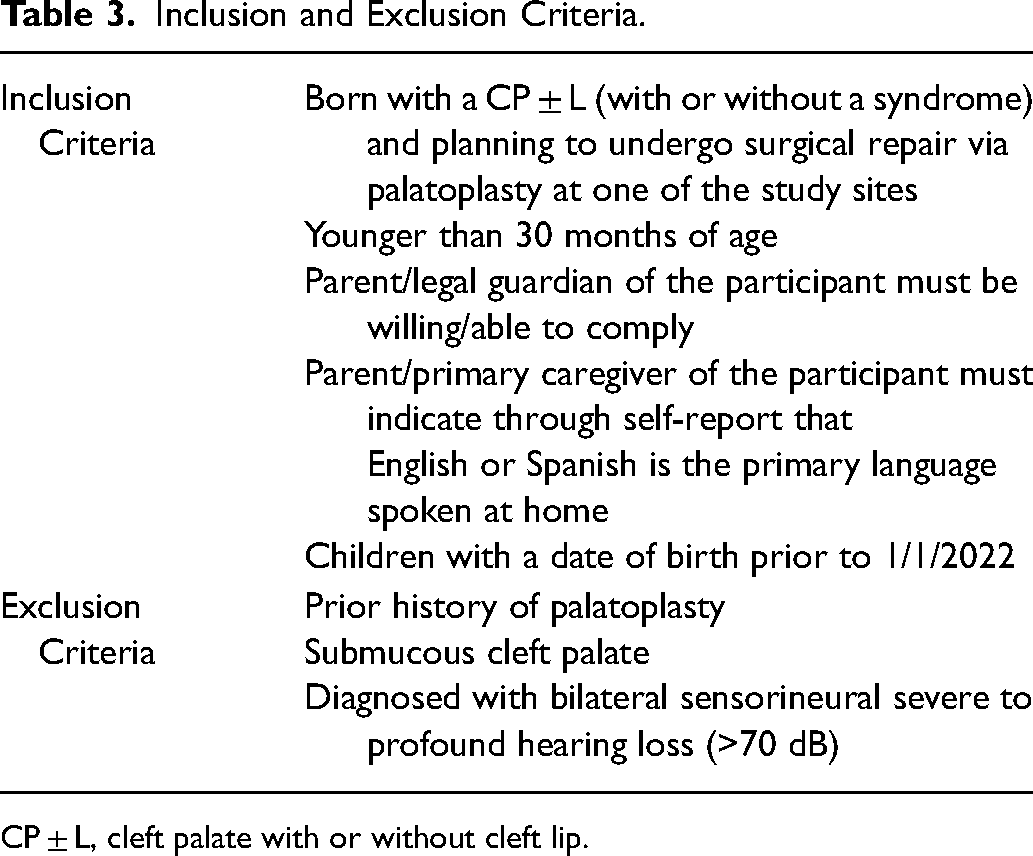
CP ± L, cleft palate with or without cleft lip.
Data Collection
Enrollment Visit
The study procedures and data collected at each of the study timepoints are outlined in Figure 1. At the enrollment visit (carried out at the time of recruitment and prior to palate repair), parents/primary caregivers provide demographic information as well as details of their child's medical (eg, pregnancy and birth, surgeries, ears and hearing) and developmental histories (eg, motor and speech-language milestones), and all therapies received. Site study coordinators verify and supplement parent-reported information based on review of each child's electronic medical record. For children exposed to both English and Spanish, the parents/primary caregivers are asked to complete a Language Questionnaire (LQ). 78 The LQ is a non-standardized instrument that was developed based on research and current best-practices to determine the child's language exposure and language proficiency (at 3 years only) in English and Spanish. The LQ includes a grid that parents/primary caregivers are asked to complete indicating how many hours a day their child is exposed to or uses Spanish and English and collects information on language history for both the parents/primary caregivers and the child. 78 The responses from the LQ are used to determine if testing should be carried out in English only, Spanish only, or both languages.
Palatoplasty and Surgical Follow-up
On the day of surgery, the surgeon is asked to perform the cleft width and length measurements and complete the Surgical Operative form in its entirety. The data from this form are used to assign type of surgery performed (IVVP vs Furlow Z-plasty). The Surgical Follow-up form is completed at the post-op surgery visit (anywhere from 42 to 365 days post-palatoplasty). If fistula status changes during this time period, the Surgical Follow-up short form is completed a second time, documenting the change.
16-, 24-, and 36-Month Assessments
The child's speech, language, and developmental skills are assessed at the target ages of 16-, 24-, and 36-months, as described below and in Figure 1. If possible, these assessments are coordinated with a clinical visit. However, the 16- and 24-month visits can be completed over the phone, on paper forms mailed to families, or via REDCap surveys.
At all three assessment points, parents/primary caregivers are asked to provide updated information on demographics, medical and developmental histories, therapies received, and changes in language exposure (see description of the LQ above); additional information is collected from the child's medical records by the study coordinator. Additional data collected at each of the assessment points are described below.
16-Month Assessment (14-18 Months)
Parents/primary caregivers are asked to complete questionnaires about their child's language and developmental functioning, including the MacArthur Bates Communicative Development Inventory: Words and Gestures (CDI:WG); an inventory of early receptive and expressive vocabulary and gestures), 73 the LENATM Developmental Snapshot (LENA TM ; an assessment of early language skills), 79 and the Ages and Stages Questionnaires-3 (ASQ-3; a developmental screening checklist across motor, cognitive, social, and communication domains). 74
During the first two years of the study, we also collected information about the child's speech sound production using a Language ENvironment Analysis-Digital Language Processor (LENA-DLP), which is an audio-recording device that the child wears in a vest. These 2-4 hour recordings were collected as part of a team visit or the LENA-DLPs were sent home with families and mailed back upon completion. During the COVID-19 pandemic, we suspended collection of the LENA speech recordings temporarily; however, even after data collection resumed, families were less willing to complete the recordings. As a result, we discontinued this study procedure and began asking families to report the sounds they heard their babies produce.
24-Month Assessment (22-26 Months)
Parents/primary caregivers are asked to complete the MacArthur Bates Communicative Development Inventory: Words and Sentences (CDI:WS), 73 which assesses expressive vocabulary and early grammatical skills.
36-month Assessment: Final Speech Outcome (34-48 Months)
The 36-month assessment is carried out in person and includes collection of a videorecording of a standard speech sample: three-minutes of spontaneous speech, counting from 1 to 10, repetition of the American-English Phrase Sample (AEPS; for assessment of speech and resonance), 80 and administration of the Goldman Fristoe Test of Articulation-3 (GFTA-3; a measure of speech sound development). 70 Parents complete the MacArthur Bates Communicative Development Inventory-III (CDI-III; a measure of vocabulary, sentence complexity, and language use), 73 the ASQ-3, 74 the VPI Effects on Life Outcomes (VELO; a measure of quality of life), 71 the Intelligibility in Context Scale (ICS; a measure of speech intelligibility), 72 and a new LQ to document not only language exposure but also language use. For more specific details about: (1) the speech sample elicitation, videorecording protocol, and the specific microphone and video camera used; (2) the training program; and (3) quality assurance procedures, see Baylis et al. 81 Children who are unable to complete the 36-month speech assessment described above due to low language skills can participate in a “limited visit” (remotely or in person). This limited visit includes administration of the ASQ-3 only.
Interim Contact Points
Parents/primary caregivers are contacted when their child is 20, 28, and 32 months of age to obtain updates regarding enrollment in EI-SL services (See Figure 1). Procedures for collection of the EI-SL data are described in more detail below. At the 32-month check-in, parents/primary caregivers are also asked a series of questions about their child's verbal skills to assist in planning for the 36-month visit.
Early Intervention–Speech/Language Services Documentation
If the parents/primary caregivers report that the child is receiving EI-SL services at any of the assessment or interim contact points, they are asked to sign an Authorization to Release Information form. Next, the study coordinator or site SLP contacts the service provider to describe the study and request their participation. They are next sent a letter including contact information for the study coordinator or site SLP, and intervention session forms with instructions on how to complete them (ie, the EI-SL Intervention form). 82 The provider is asked to complete a new form each time they provide speech/language services to the child. If a provider cannot be reached or fails to provide the requested information, copies of the current treatment plan, progress notes, Individualized Family Service Plan (IFSP), or other relevant documentation is requested; and trained study staff complete the POC documentation forms using a short form version of the EI-SL Intervention form. 82 Finally, if the two options above do not provide the data needed, parents are interviewed to obtain information on the provider and the frequency and type of therapy their child is receiving.
Data Management and Analysis
The UU is the main coordinating site for collection, analysis, and storage of data from all the participating sites; UWY, NCH, and PCH serve as data analysis sites. Study data are collected and stored using REDCap (Research Electronic Data Capture), an electronic data capture tool hosted by the Center for Clinical and Translational Research–Biomedical Informatics Core at the University of Utah. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources.76,77
All data collected on paper forms at the sites are entered into REDCap by the site study coordinators, and all entries are double-checked at the time of data entry. Automated data checks based on field constraints and range checks are carried out, with alerts sent to sites when problems are identified. Manual checks are also made by the UU research staff to identify missing, incomplete, or questionable data entries at the sites. If issues are identified, the site study coordinators are notified, and corrections are made and documented as is appropriate.
Parent-reported questionnaires and video-recordings are uploaded to a secure, password protected, HIPAA/PHI-compliant online cloud storage platform (Ubox). All questionnaires are scored (and double-checked) and video-recordings quality-checked by the trained research assistants at the UU. A video sample is determined to be “ratable” for the primary study outcome (perceptual rating of hypernasality), if the child produces an adequate sample of connected speech with good audio-quality. If the child only produces single words or does not produce an acceptable number of multi-word utterances, the sample is considered unratable; and the child is re-scheduled for a new recording at a later date.
The LENA-DLP recordings are converted to waveform audio files (.wav) using the LENA software at the UWY or NCH. Quality review and perceptual speech analysis of the recordings are conducted at the UWY. The samples are analyzed to characterize the child's speech production skills using a modified TimeStamper methodology, which is described in a series of articles by Hardin-Jones et al 2023a, 83 2023b, 84 and 2024, 85 prior to uploading to the Ubox.
Classification of Palatoplasty Type
The Surgical Technique Review Panel, consisting of four surgeons (two study Co-Is and two site PIs), met prior to study launch and developed criteria for classifying each palate repair as a straight-line closure with IVVP or a Furlow Double-Opposing Z-plasty using the surgeons’ responses on the Surgical Operative form. Straight-line closure with IVVP requires straight-line closure of the soft palate nasal mucosa, circumferential muscle dissection with independent muscle repair, and straight-line closure of the soft palate oral mucosa. Furlow Double-Opposing Z-plasty requires Z-plasty closure of the soft palate nasal mucosa, leaving the muscle attached to the posteriorly based mucosal flaps, and Z-plasty closure of the soft palate oral mucosa. Other techniques, such as those using a hybrid of these maneuvers and/or techniques using a buccal myomucosal flap in the mucosal closure, will be excluded from the two primary technique types and categorized as “Other”.
Fistula Determination
The presence of a fistula within the secondary palate is defined as any oral-nasal communication between the incisive foramen and base of the uvula14,86 as assessed by the surgeon between 42 and 365 days post-surgery and documented on the Surgical Follow-up form. If fistula status changes over the study period, a shortened version of the Surgical Follow-up form is completed, and data from the last evaluation are used in the analysis.
Rating of the 36-Month Videorecorded Speech Samples
The primary aim of the study is to compare hypernasality rating from the videorecorded speech samples at 36- months of age for the two palatoplasty groups. The ratings are carried out by trained CORNET SLPs. Prior to rating the samples, the SLP raters participate in a multi-day training session and complete refresher trainings at regular intervals over the study period. Samples are rated remotely in groups of four using a modified version of the CAPS-A-AM rating form. 40 Each sample is assigned a primary and secondary rater. The primary rater evaluates all four samples for speech acceptability, voice, hypernasality, hyponasality, and audible nasal emission (ie, CAPS-A-AM speech parameters) and phonetically transcribes the AEPS and GFTA-3 using the International Phonetic Alphabet (IPA) 87 and the extIPA for disordered speech. 88 One randomly chosen sample is re-rated for intra-rater reliability (25% of the samples) approximately two weeks after the initial rating. The secondary rater evaluates the same four samples for the speech parameters described above but only phonetically transcribes the AEPS and GFTA-3 for one randomly chosen sample for the purposes of inter-rater reliability (25% of the samples).
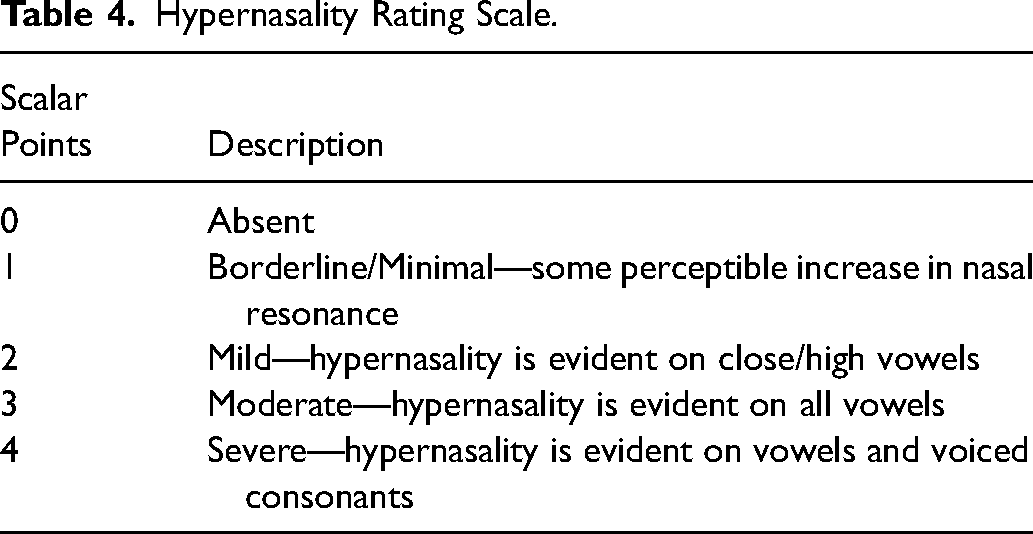
As the primary study outcome is degree of hypernasality based on a perceptual speech rating, a consensus rating protocol is used for ratings of hypernasality. To re-calibrate the raters prior to the start of each rating session, the raters listen to anchor samples of varying degrees of hypernasality from a rating of “0” or absent to “4” or severe (see Table 4 for a description of the scalar points). The raters make independent ratings of the speech parameters and phonetic transcriptions on paper forms and enter their ratings into REDCap. When performing the ratings, the SLP raters are not aware of the child's surgery type and are not assigned samples of children from their own sites.
Hypernasality Rating Scale.
The ratings are reviewed at the UU, which includes comparing the paper forms with the data entered into REDCap. Following the consensus rating protocol for hypernasality, if a disagreement occurs between the primary and secondary raters on the score assigned, the two raters re-listen to the sample(s) together on a later date and reach consensus on the final rating to be assigned for that sample.
Statistical Analysis
Power Analysis/Sample Size Calculation for the Primary Study Outcome
The sample size and power calculations were based on a comparison between straight-line closure with IVVP and Furlow Z-plasty for the primary outcome of degree of hypernasality at 36-months.
The initial sample size calculation was conducted using the number of palate repairs performed historically at anticipated sites. This calculation, details of which are available from the authors upon request, estimated that enrolling 1514 participants would provide 80% power to detect a small effect size (Cohen's D = 0.30) 89 with a two-sided significance level of 0.05.
In June of 2022, during the conduct of the study, the target sample size was recalculated. For this recalculation, patient outcomes were assumed to cluster by surgeon rather than sites,14,90 with an intraclass correlation (ICC) of 0.05. The number of surgeon clusters was estimated at 67 based on the number of surgeons performing palate repairs at participating sites. Using information available at that time on actual enrollment, including the distribution of participants into the straight-line closure with IVVP and Furlow Z-plasty cohorts, it was estimated that a sample of 454 participants with 36-month speech samples would be needed to provide at least 80% power to detect a small Cohen's D 89 effect size (0.30) with a two-sided significance level of 0.05. Assuming 10% loss due to lack of suitable matches and using information available at that time from enrolled participants on observed loss to follow-up, prevalence of language delays limiting speech sample collection at 36-months, and use of alternative palate repair techniques, it was estimated that 1231 participants would need to be enrolled to achieve the revised target of 454 participants with ratable 36-month speech samples.
Statistical Methods: Aim 1 - Comparison of Straight-Line Closure with IVVP and Furlow Z-Plasty
The primary study objective is to compare the degree of hypernasality at 36-months of age between straight-line closure with VVP and Furlow Z-plasty. To address potential confounding from non-random assignment to procedure groups, the analysis will employ generalized estimating equations (GEE) with propensity score weighting. Briefly, a multivariable logistic regression model will be developed (ie, a propensity score) to estimate the conditional probability of receiving a Furlow Z-plasty given known patient (eg, cleft type, palate length, cleft width, cleft-related syndrome diagnosis, age at palatoplasty) and surgeon factors (eg, surgeon training and experience). See Table 1 for a list of covariates. Missing covariates will be addressed using multiple imputation. Observations will then be weighted, 91 and balance of covariates between weighted groups will be evaluated using standardized mean differences. Weighted GEE will then be applied to compare the degree of hypernasality at 36-months of age between the two surgical groups. The weighted GEE analysis will use robust standard errors and account for clustering of participants by surgeon.
The secondary study objective is to compare the incidence of fistula between straight-line closure with IVVP and Furlow Z-plasty. This analysis will be performed using logistic regression with propensity score weighting. The propensity score weighting approach will be identical to that described for the primary study outcome. The weighted logistic regression analysis will use robust standard errors and account for clustering of participants by surgeon.
Statistical Methods: Aim 2 - EI-SL Service Delivery: Characteristics and Associations
The proportions of participants receiving any type of EI-SL services, and the proportions receiving specific types of EI-SL interventions (eg, oral-motor exercises, speech production/articulation, language/vocabulary) will be summarized by type of surgery, cleft type, sex, and other socioeconomic and demographic factors. In addition, provider characteristics, therapy setting, number of sessions, and participant age at time of services will also be described.
Generalized logistic mixed effects models (GLMMs) will be used to characterize variation across sites in the proportions of participants who receive 1) any type of EI-SL services, and 2) each specific type of EI-SL service. These models will adjust for patient characteristics: sex, race, ethnicity, cleft type, cleft-related syndromic diagnosis, family history of speech-language disorder, age at time of EI-SL service delivery, and insurance status.
GEE analyses will be performed to describe the association of EI-SL service delivery with each of the following outcomes at 36 months of age: degree of hypernasality, consonants correctly produced on the GFTA-3 and AEPS, and ICS total score. These analyses will adjust for the same patient characteristics as described in the paragraph on GLMMs above.
Study Oversight and Monitoring
The study has an Executive Committee (EC) and an NIH-NIDCR appointed Clinical Study Oversight Committee (CSOC). The EC consists of the study principal invesigator and co-investigators who are responsible for 1) study design and management, 2) review of the study timeline and implementation of steps to ensure that study goals are met, 3) review and implementation of recommendations from the NIH program officer and oversight bodies, and 4) interpretation and dissemination of study findings. The EC also provides guidance and approval of other investigators interested in using the CORNET data set for new study ideas or grant applications. Data are only shared the if the parents/primary caregivers provide consent for their child's data to be used for future studies.
The CSOC is a monitoring board appointed by the NIDCR with expertise relevant to the study protocol (ie, plastic surgery, speech-language pathology, and statistics). They provide oversight and advise NIDCR and the EC on multiple aspects of the study such as safety of human subjects, participant recruitment and demographics of the study population, progress with data collection, and overall study administration. They make recommendations to the NIDCR and EC annually regarding changes to the study protocol and continuation of the study.
Current Progress
Participant recruitment started at the first site in March of 2019. Sites launched on a rolling basis, with the last site launched in March of 2020. Recruitment was completed as of February 2023; we have retained 80% of children enrolled. We expect to complete the final 36-month assessments in 2024; however, rating of samples, manuscript preparation, and dissemination of study findings will continue into 2025. Figure 2 shows the number of children who have reached the specific study milestones.
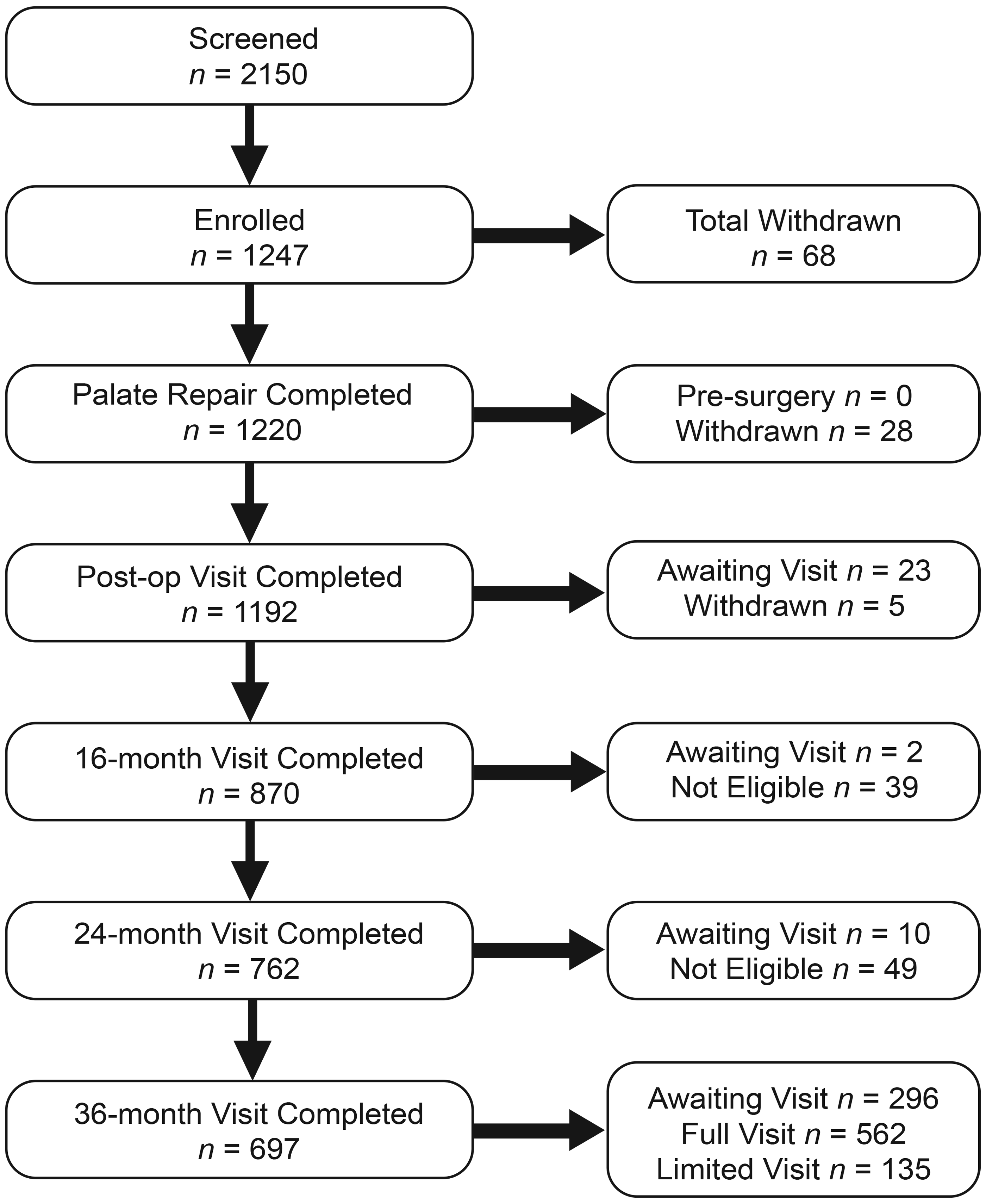
Study milestones.
To date, data collected for the CORNET-SSS have supported investigations of stop production post-palate repair, 84 postoperative management protocols, 90 predictors of delayed palate repair during the COVID-19 pandemic, 92 feeding management and impact on palatoplasty for babies with Pierre Robin Sequence, 93 a tutorial on collecting standard speech samples for research and clinical purposes, 81 and validation of a methodology documenting consonant production in toddlers with cleft palate.83,85 Our team has presented 21 papers at national and international conferences, with an additional seven manuscripts in various stages of completion. An ancillary study has also been launched in direct collaboration with the CORNET-SSS (Health and Psychosocial Outcome Study in Young Children with Cleft Palate [HAPY]). HAPY is a prospective, observational study evaluating demographic, medical, and contextual factors associated with psychosocial and health outcomes over time in children born with CP ± L. CORNET is sharing background data already collected on the children and working with sites to facilitate recruitment across all CORNET sites.
Discussion
The CORNET-SSS is a prospective, longitudinal, comparative effectiveness study evaluating surgical outcomes from primary palate repair, EI-SL service delivery, and a broad set of clinician-rated and parent-reported speech and language outcomes in a large and diverse group of children with CP ± L. The CORNET-SSS has enrolled 1247 participants, from 18 sites, with engagement from approximately 60 surgeons and 100 SLPs. The study attempts to balance scientific rigor with clinical feasibility; we have testable hypotheses, standardized data collection protocols, and a statistical analysis plan that minimizes bias and confounding by employing propensity score matching. We are not constraining surgeons’ decision-making regarding type of surgery but allowing them to “do what they would typically do” based on each child's individual characteristics.
Our study is innovative in a number of ways. First, we have created common data elements that can be shared across studies and integrated into clinical practice. Some sites have incorporated the Surgical Operative form into their standard documentation for palatoplasty, and the Americleft speech data collection procedures and rating protocol have been adopted at many sites for both research and clinical purposes. These practices facilitate data sharing and the comparison of results across different studies and clinical sites, while also reducing the cost and time for development of data collection and analysis tools. Second, the CORNET-SSS is a “biopsy” of current clinical practice for children with CP ± L in the US. In addition to details regarding each surgeon's specific surgical technique, we are collecting data on pre- and post-operative care, practice patterns, and access to EI-SL intervention services. Third, we are increasing generalizability of research findings by including Spanish-speaking children and children with syndromes. We are following best practices for assessment of children who are bilingual which include: (1) utilizing non-biased assessment protocols; (2) assessing children in one or both languages depending on the amount of language exposure in the two languages; and (3) employing SLP raters who are bilingual English/Spanish speakers. Children with syndromes made up approximately 24% of the total population of participants in the multi-site Americleft speech study. 94 Yet, these children have been excluded in previous speech/surgical outcome studies until now, even though they represent a significant portion of cleft teams’ clinical populations.9,52,55,95–99 Finally, the approach we have taken, using real world evidence and working with clinician-researchers to develop the questions and provide the study data, should facilitate acceptance and implementation of the study findings.
Study Challenges
A study of this magnitude is not without challenges. Our most significant challenge was the COVID-19 pandemic; the impact of the pandemic on research has been documented in the literature. 100 The start of the pandemic corresponded to the start of recruitment at two of our later launching sites. Early in the pandemic, many study staff were unable to conduct in-person visits, impacting recruitment, enrollment, and data collection. The research team revised the study protocol and procedures to allow remote consenting and data collection (if appropriate). For example, we converted all questionnaires to REDCap forms and purchased fillable forms for the standardized parent-reported questionnaires. Consenting and other enrollment activities can be completed with families by phone or video calls. Families can be sent the parent-reported questionnaires and REDCap version of forms that are completed at the 16- and 24-month visits. They also receive written instructions and follow-up by phone with the study coordinators. Because the 36-month visit must be conducted in person, site SLPs are also testing children outside of regularly scheduled team visits if necessary.
In spite of these changes, families were often unable to complete study procedures due to COVID-related barriers. As a result, we eliminated some procedures so as not to overly burden families. Sites also reported difficulty hiring study staff during the pandemic and increases in the number of children lost-to-follow-up which has impacted collection of study data. Unfortunately, some of these challenges have continued into the post-pandemic period. Cleft teams are continuing to report higher lost-to-follow-up rates compared to pre-pandemic. Some sites are reporting a back-log in scheduling, giving priority to older children who missed visits during the pandemic. Although we expected that there would be children lost-to-follow-up based on prior studies that relied on assessments being carried out as part of team visits, 94 our attrition rate is higher than anticipated.
The inclusion of children with syndromes, many with developmental delays, revealed more children than expected who are unable to provide a robust speech sample at age 3. Thus, a “limited” 36-month visit protocol was developed to collect at least minimum indices of the speech-language skills of this subgroup of children. As we had not enrolled Spanish-speaking children in our research studies previously, we had to develop an instrument to document language exposure and proficiency for children speaking both Spanish and English and create different rater training and calibration sessions for bilingual SLPs who are rating the Spanish monolingual and bilingual samples.
Conclusions
The CORNET-SSS is addressing longstanding questions related to the effectiveness of the two primary palate repair approaches by comparing hypernasality outcomes and fistula occurrence as well as speech/language intervention practices and their potential impact on speech outcomes. The findings of this study will provide new knowledge that will guide surgical decision making and assure the best speech-language outcomes for children born with CP ± L.
The research network described here also fills a critical gap by providing clinician-researchers with an innovative tool for multidisciplinary, multi-center outcomes data collection and dissemination by creating a consortium of cleft teams across the US (ie, CORNET). However, the potential for CORNET goes beyond speech and surgical outcome studies. The CORNET infrastructure will streamline future design and implementation of studies in other cleft care specialties (eg, dental, orthodontic, genetics), create a sustainable model for large scale multidisciplinary CP
Footnotes
Acknowledgements
The authors would like to acknowledge the clinical sites participating in the Cleft Outcomes Research NETwork (CORNET) Consortium in alphabetical order: Ann & Robert H. Lurie Children's Hospital of Chicago; Banner Health—Banner Children's at Desert; Children's of Alabama; Children's Hospital Colorado; Children's Hospital Los Angeles; Children's Hospital of Philadelphia; Johns Hopkins University/Johns Hopkins Children's Center; Lancaster Cleft Palate Clinic & Penn State Hershey Children's Hospital; Medical College of Wisconsin-Milwaukee Campus/Children's Wisconsin; Nationwide Children's Hospital; Phoenix Children's Hospital & Barrow Cleft and Craniofacial Center; Rady Children's Hospital; Seattle Children's Hospital; Shriners Hospital for Children—Chicago; Texas Children's Hospital; University of Iowa/Stead Family Children's Hospital; University of Wisconsin/American Family Children's Hospital.
We also acknowledge the contributions of Jacob Kean, PhD, Susan D. Horn, PhD, and Thomas Greene, PhD for developing the study methodology and Sarah Hatch Pollard, MPH, and Amy Wilder, PhD for assistance with manuscript preparation.
The authors would like to acknowledge the University of Liverpool CTRC for development of the TimeStamper software.
Parts of this manuscript was presented at the 80th Annual Meeting of the American Cleft Palate Craniofacial Association, May 2-6, 2023, Raleigh, NC and at the 14th International Cleft Congress, July11-15, 2022, Edinburgh, Scotland.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: the National Institute of Dental & Craniofacial Research of the National Institutes of Health under Award Number R01DE027493.The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.