
Abstract
Objective
To determine caregiver preferences for education modalities.
Design/Setting
A cross-sectional study of caregivers of patients with cleft lip and/or palate (CL/P) seen at this American Cleft Palate-Craniofacial Association–approved center in the Midwest between January 2017 and September 2022 was conducted.
Patients/Participants
The population included parents of patients undergoing primary or secondary revision surgeries after a diagnosis of CL/P.
Main Outcome Measures
A phone interview gathered demographics, education preferences, familial research, and resources.
Results
Of the 81 families of CL/P patients, 42 families consented for interviews. Patients first presented to the clinic at an average age of 2.3 years of age (range 0-17) and had a mean age of 10.1 years (range 1-23) at the time of parental interview. The majority of interviewees identified as the patient's mother (90.5%), Caucasian (78.6%), and had completed a college education (81%). The majority (85.7%) of caregivers reported completing research prior to the first appointment. Most participants preferred electronic resources (35.7%), support groups (29%), books or written material (29%), with fewer preferring videos (12%), social media (7%), or podcasts (2%).
Conclusion
The majority of families preferred having multiple resources available to learn about CL/P; however, the most common preferences were additional books, pamphlets, and online materials such as websites, videos, and audiobooks. With the multitude of options available for patient education materials, designing and providing high-quality materials that will be used by families and meet the health literacy of this diverse patient population is crucial.
Keywords
Introduction
Cleft lip and palate (CL/P) is one of the most common congenital diagnoses of the jaw and face, occurring in approximately 1 out of every 1000 live births. 1 This diagnosis often requires multiple surgical interventions over the patient's lifetime and involves the work of a multidisciplinary care team composed of specialists from plastic surgery, dentistry, otolaryngology, pediatrics, speech-language pathology, audiology, and social work, 2 and provision of educational resources and discussions regarding prognosis and treatment planning is best started at the time of initial diagnosis.
It is estimated that patients often retain less than 50% of what providers discuss during a clinic visit. 3 In addition to crucial face-to-face discussions, supplemental materials are often needed to ensure that patients and caregivers have a comprehensive understanding of their diagnosis and treatment plan. Providing patient education reduces anxiety about healthcare, promotes adherence to treatment, increases satisfaction with care, and improves overall health outcomes.4,5 Advances in technology have expanded the formats of educational materials to online videos, websites, eBooks, audiobooks, and phone applications, diversifying the ways in which patients can learn about their health, in addition to more traditional print-based health information resources.6–9
Thus, providing a diverse set of educational resources and understanding caregiver preferences are crucial. The aim of this study is to understand the preferences of caregivers of CL/P patients toward various education modalities at an American Cleft Palate-Craniofacial Association (ACPA)-approved center.
Methods
Study Population
A cross-sectional study of patients with CL/P seen at this ACPA-approved center between January 2017 and September 2022 was conducted. The population included patients undergoing primary or secondary revision surgeries after a diagnosis of isolated or syndromic CL/P. Exclusion criteria included families who had previously opted out of research participation at the institution and interviewees under the age of 18 years old. Phone interviews were conducted between March and April 2023. This study was reviewed and qualified as exempt by the Institutional Review Board.
Survey
A phone interview was offered to caregivers of patients with CL/P to elicit preferences for educational tools for both general CL/P-related information and secondary surgeries. Demographic information was collected including the interviewee relationship to the patient, highest education completed by the interviewee, ethnicity, primary language, and whether the interviewee's occupation was in the healthcare field. Clinical information, including patient age at initial visit, patient current age, patient sex, patient diagnosis (cleft lip, cleft palate, or both CL/P), and presence of a family member with a CL/P diagnosis was recorded.
Interviewees were asked to rate their preappointment understanding prior to the first visit on a scale of 0 to 5 with 0 indicating no understanding and 5 being extensive understanding of CL/P. Interviewees were asked to quantify how much research was performed prior to the first visit with five options: none, some (less than 1 h), moderate (1-3 h), and extensive (3 or more hours). Research sources and education preferences were listed, and interviewees were given the option to select more than one option. The list of resources including information provided by another health care provider, electronic materials (electronic materials may include resources such as websites, online videos, eBooks, or audiobooks), books/written materials, phone applications, videos, podcasts, talking with a friend or family member, social media, or support groups. For interviewees who had a primary language other than English, an option for educational tools in non-English was given, and the interviewee was asked which formats would be preferred in their native language. Bilingual participants were interviewed in English.
Statistical Analysis
A statistical analysis was performed using Microsoft Excel, Version 16.66.1 (Microsoft Corporation One Microsoft Way, Redmond, Washington). Results were summarized using descriptive statistics.
Results
Patient and Caregiver Characteristics
Patient and caregiver characteristics are summarized in Table 1. The majority (90.5%) of interviewees identified as the patient's mother. Most (81%) interviewees reported a college education level, and the majority (78.6%) were Caucasian. The primary language spoken was English (90.4%). Less than one-fourth of interviewees (21.4%) worked in the healthcare field. Interviewees reported an average of preappointment understanding of CL/P of 2.4 on a scale of 0 to 5. A portion of interviewees (16.7%) had an additional family member with CL/P. The average age of the patient at the initial appointment at this particular center was 2.3 years (range 0-17, median age 6 months). The age reported at the first visit did not differentiate patients treated at a separate center prior to transferring their care for this initial appointment. The average patient age at the time of the interviews was 10.1 years. Of the patients included in this study, 57.1% were male. Over half of the patients included in the study had a diagnosis of CLP (57.1%).
Characteristics of Caregivers Surveyed Regarding Preferences on Educational Materials.
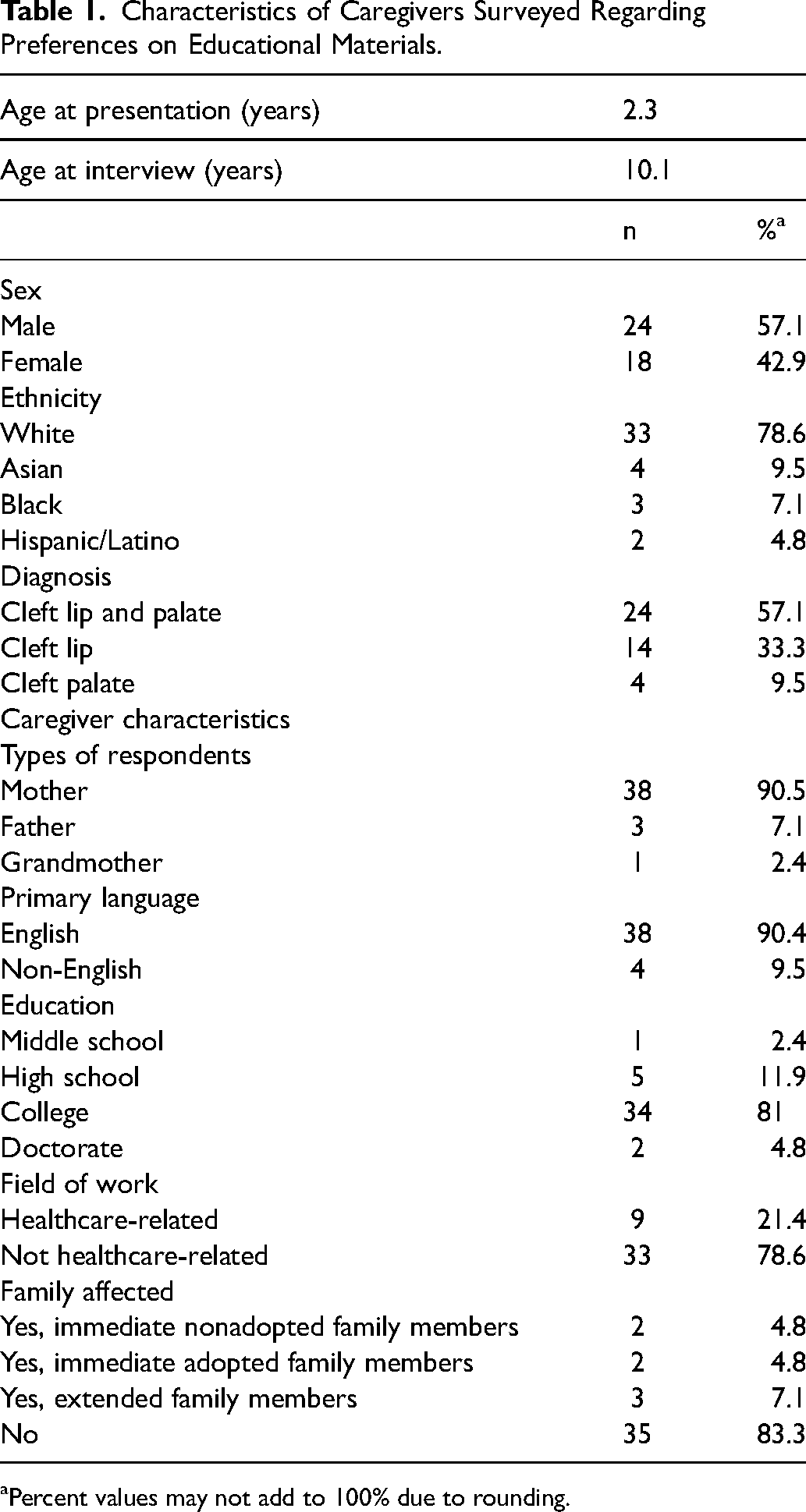
Percent values may not add to 100% due to rounding.
Research Sources Used by Caregivers
Most caregivers engaged in preappointment research (85.7%, n = 36). The most common preappointment research time spent was greater than 3 h (38%), which was defined as an extensive amount of research. The most common sources of preappointment information were electronic materials (62%), followed by another physician (40%), and talking with friends or family (14%). Less common sources of preappointment information were social media (7%), books and written materials (7%), adoption agencies (5%), and support groups (5%). A summary of the preappointment research sources used by interviewees is reported in Table 2.
Preappointment Research and Preferred Educational Modalities.
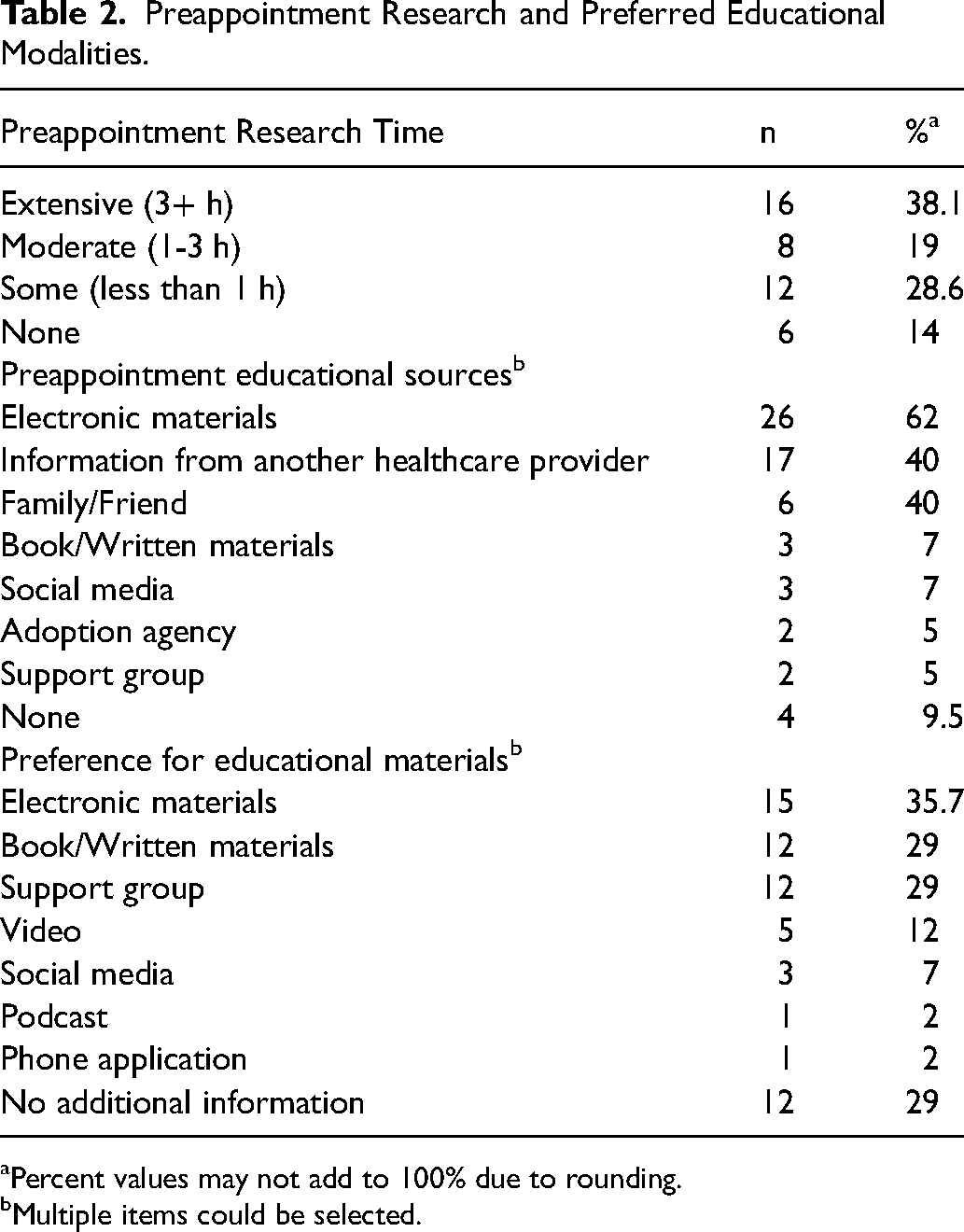
Percent values may not add to 100% due to rounding.
Multiple items could be selected.
Preferred Patient Education Tools
While many families described the value and importance of the clinic visits and education provided during these appointments, commonly preferred supplemental materials included electronic materials (35.7%), support groups (29%), and a book or written material (29%). Less commonly preferred supplemental materials included videos (12%), social media (7%), podcasts (2%), and iOS or Android apps (2%). Approximately one-third of respondents (29%) did not feel any further tools were needed outside of what was provided at appointments. Four interviewees identified a primary language other than English. Supplemental education materials in non-English languages were requested, specifically in video format (75%), books or written material in their native language (25%), and electronic material in their native language (25%). Family and caregiver preferences for patient education materials are summarized in Table 2.
Discussion
Patients with CL/P and caregivers are faced with numerous decisions that can greatly impact their health and quality of life. Studies have shown that patients often forget information discussed during visits which may lead to gaps in knowledge about the diagnosis and treatment options. 10 As such, patient education materials are important adjunctive educational tools apart from office visits. While patient preferences for educational materials have been studied in other fields,7,11–15 few studies have evaluated the educational preferences among caregivers of patients with CL/P palate. By gaining a better understanding of preferences for educational information, educational teams can develop materials that are most suitably tailored to their patient populations.
The most preferred methods of patient education material delivery in this study were electronic materials (such as websites, online videos, eBooks, or audiobooks), books or written materials, and support groups, while lesser preferred materials include videos, social media, podcasts, and iOS or Android apps. Utilization of electronic platforms for accessing health information has experienced a notable surge in recent years. 16 However, these can also serve as a barrier when electronic platforms restrict access for groups unable to afford costly devices or unable to easily gain internet access and should be taken into account when designing patient educational materials. Books or written materials were the second most preferred format. Prior research has highlighted the preference for written materials across a variety of patient populations.13,17,18 The findings of this study underscores the ongoing relevance of written materials as a means of delivering patient education across a variety of age groups even in the midst of a rising digital age.
In addition to electronic and written materials, a large portion of respondents both utilized friends and family as a preappointment resource and preferred support groups for patient education, highlighting the importance of a strong social support system. Previous studies have shown that consistent support from parents, friends, and health professionals is associated with improved patient and family quality of life, lower psychological distress, and better adjustment to raising a child with CL/P.19,20 Thus, craniofacial centers may opt to organize support groups on behalf of patients and caregivers or be able to provide resources for which support groups, both in-person and online, can be found.
Despite 62% of respondents using the internet as a preappointment source of information, only 35.7% of respondents in this study preferred online materials as a supplemental educational tool. Prior studies on health information–seeking behavior have found the internet to be one of the most common sources of information for parents to learn about their child's condition.21–23 The low preference for this format of patient education materials may be due to concerns about the trustworthiness, reliability of information obtained through the internet, and the overwhelming amount of information available.13,22 Additionally, prior studies have found that many online websites are written at a higher reading level than recommended by the National Institutes of Health, which may hinder caregiver and patient understanding and expectations of CL/P care.24–26 This highlights the need for healthcare providers to be aware of reliable and regulated online sources of information in order to guide patients to effective and appropriate websites.
The findings of this study emphasize the diversity of patient preferences, and the importance of multimodal patient education tailored to individual preferences and experiences. Research demonstrates that making use of multiple strategies when educating patients may be more effective than using single modes, such as verbal or written. 27 Regardless of the format in which patient education materials are delivered, evaluating the health literacy level of the patient and ensuring appropriate readability of the materials provided are of utmost importance. 28 It is estimated that approximately 80 million adults in the United States have limited or low health literacy.29–31 The readability of written or online resources can be assessed by various readability measures, each of which uses various indices for scoring, such as words per sentence, word and sentence count, and syllables per word.32,33 Analyzing the readability of patient education materials is an important tool in which providers can customize health-related education material to the individual patient. Additionally, it is notable that for patients with primary languages other than English, the majority (75%) preferred a video available in their native language. While caregivers are provided with interpreters during the appointments, this reflects the desire and the need for reliable, additional resources outside of appointments to reference and learn more about diagnosis and treatment.
This study is not without limitations. As with all single-institution studies, results may be limited in their generalizability. Only families opting in for research were included in the study, limiting the sample size. Additionally, the majority of respondents are college-educated and Caucasian. While this reflects the population in the area where the study was conducted, it is not reflective of the United States population as a whole. Future research on this topic should be conducted in a multicentered fashion to better capture different demographic regions within the country. Interestingly, the average age of the patient at the initial CL/P appointment at this particular center was 2.3 years, which is older than expected for primary CL/P surgery as this would be expected to start in infancy. This number may be high because this study also included patients undergoing secondary revision of CL/P who presented to this particular center for the first time. Additionally, difficulties with recall may have also impacted responses about previsit information seeking, particularly for those who were interviewed years after their initial evaluation. After using the information gleaned from this study to create and revise patient education materials, future work should focus on assessing patient satisfaction with the materials created.
Conclusion
The majority of families preferred having multiple resources available to learn about CL/P with the most common preferences being electronic materials, written materials and books, and videos. With the multitude of options available for patient education materials, designing and providing high-quality materials that will be used by families of this diverse patient population is crucial.
Footnotes
Acknowledgments
The authors would like to acknowledge Tonye Sylvanus for his assistance in the successful execution of this study and Todd Warner for his assistance in experimental design and statistical analysis.
Data Availability Statement
Data are available upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was reviewed and determined to be Exempt by our institution's Institutional Review Board (IRB ID STUDY00018204).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.