
Abstract
Objective
This review aims to summarize existing prospective registries for congenital craniofacial anomalies across the globe.
Design
We conducted a comprehensive review of Embase and the Google Search Engine for articles which gathered data from prospective craniofacial registries and registry websites, respectively. Registry details were verified by registry coordinators where email addresses were available.
Setting
Institutional or national cleft lip and/or palate (CLP) centers.
Main Outcomes
For each registry, we collected coordinating and contributing centers, registry goals, years of operation, number of patients, datapoints collected, funding, and quality assurance mechanisms.
Results
Nine registries were identified. Six focused on CLP, 1 on craniosynostosis, 1 on craniofacial microsomia, and 1 on a range of craniofacial abnormalities. Only European and U.S.-centered registries were identified. Every existing European CLP registry represents all government-supported cleft centers in its respective nation. The 3 U.S.-based registries are expansive, but do not capture a nationwide patient base.
Conclusions
This review characterizes the current global state of prospective registries for research on congenital craniofacial anomalies. The strength and organization of data collection varies greatly by registry and by country, though the present landscape exhibits potential for improvement of craniofacial research and patient outcomes. With this evidence, we advocate for a nationally coordinated registry to improve outcomes for children with craniofacial anomalies across the United States.
Introduction
Patients with congenital craniofacial anomalies face complex medical issues affecting various structures of the head essential for childhood health and development. Adding to anatomical complexity, craniofacial abnormalities are heterogeneous and overlapping. Management often depends on syndromic diagnosis, morphology, institution, age, and even socioeconomic factors.1-6
Further hindering management is the lack of consistent, quality research involving this patient population. Literature-supported guidance is limited by small sample sizes and inconsistent methods. 7 Prospective studies are necessary to obtain patient-reported outcomes, as patients cannot weigh in until well after the initiation of care in infancy. Additionally, it takes time for the effects of surgery to manifest; for example, the neurodevelopment of a patient with craniosynostosis may not become apparent until years after surgery. 8 One solution to this problem lies in prospective registries that track treatments and outcomes using a “standardized and complete dataset including associated follow-up.” 9
Over the past 3 decades, institutions within and outside of the United States have collaborated in research via multicenter studies and registries; however, there is little oversight to standardize these networks. The existing national U.S. registries include population-level data rather than clinical.10,11 It has been recognized in the pediatric craniofacial sphere that “a new era of collaborative craniofacial research” is needed.7,12 This would involve a comprehensive, prospective registry of patients, treatments, and outcomes. Such registries require formidable effort, but would provide invaluable insights to improve care.
Creating a novel international, or even national, craniofacial registry is a task fraught with obstacles. There must be a clearly defined purpose, leadership structure, funding source, legal basis, data storage plan, quality assurance mechanism, and data collection team. 13 Datapoints including patient history and clinical characteristics, treatments, and outcomes need to be collected longitudinally until at least skeletal maturity; all variables ought to be collected in a standardized manner and should expand as technology evolves. 7 Perhaps most importantly, infrastructure to sustain high-quality organization and data collection over time is required. Fortunately, there is a global network of existing registries upon which a larger, unified registry may be modeled. It would be advantageous to analyze current registries for similarities that should be incorporated in the larger registry, for 3 key reasons: to reduce the burden of feedback loops by using already tried-and-true methodologies, to provide an avenue for potential comparison of treatments and outcomes between centers, countries, and continents, and to lay the groundwork for future registry collaboration. However, no study has yet delineated the essential details of existing registries. The purpose of this review is to describe the current landscape of prospective, collaborative craniofacial research.
Methods
Following a predetermined review protocol, 14 all authors decided upon a primary study objective and key registry characteristics to collect based upon known requirements for a national registry.7,13 A plan for data collection was made in consultation with an experienced medical librarian (LHY). This study was determined by our institutional review board as nonhuman subjects research.
Eligibility Criteria
Two sets of eligibility criteria were followed: one for articles to capture multicenter research collaborations and registries, and another for registries, themselves. The former inclusion criteria included studies on congenital craniofacial anomalies with data from multiple sites. We excluded studies where craniofacial anomalies were not the focus, those with single-center data, articles not in English, and those with unclear data sources. The latter criteria included registries with prospectively collected, multicenter data on children with congenital craniofacial anomalies and excluded those that focused on national birth data, were not created for research, or were created for one specific study.
Search Strategy
The search strategy was created by author LHY using a combination of keywords and controlled vocabulary in Embase 1947 to present (for articles containing registries) and Google Search Engine (for registries, themselves). Search strategies were completed on November 4, 2024. Reproducible Embase search is available online (Supplemental Table S1).
Study Selection and Data Extraction
Study selection and data extraction were performed by 4 independent reviewers (SC, AM, KH, and TK). Initial evaluation included title and abstract screening followed by article review. Each article was assessed by 2 reviewers; disagreements were resolved by a third author. After full-text selection, registries were collected from relevant articles. An additional registry search was conducted via Google Search Engine. Registry characteristics including location, number of patients, funding, quality monitoring, and datapoints were extracted (authors SC, AM, KH, and TK). Details were emailed to the respective registry coordinator for verification wherever email addresses were available.
Analysis
After discussion between authors SC, KBP, and GBS a standard scheme for presentation of data was planned and implemented for each registry to allow for easier comparison of datapoints, including: country of data collection, coordinating site, aim(s), funding source, and quality assurance mechanism. 13 Geographical details were to be portrayed visually and other data was to be both described and tabulated.
Results
The Embase search yielded 812 articles. Seventy-seven of these drew data from 13 distinct registries. Nine registries that did not meet inclusion criteria were excluded (Supplemental Figure S1). Registries collected from Embase include the Synostosis Research Group (SynRG), Cleft Outcomes Registry/Research Network (CORNET), Cleft Collective Cohort, and Allied Cleft & Craniofacial Quality-Improvement and Research Network (ACCQUIREnet).
A Google search yielded 6 registries. One was excluded for lack of information available. The remaining 5 included the Swedish Cleft Lip and Palate (CLP) Registry, Norwegian Registry for CLP, Cleft Registry and Audit Network (CRANE), European Reference Network-Cranio (ERN-Cranio) registry, and the Craniofacial Microsomia: Accelerating Research and Education (CARE) Registry.
Registry administrators for SynRG, CORNET, Cleft Collective Cohort, ACCQUIREnet, the Swedish CLP Registry, CRANE, and the Norwegian Registry of CLP were available to verify data. Distinct registry datapoints are available online (Supplemental Table S2).
CLP registries are mapped in Figure 1, non-CLP registries in Figure 2, and multianomaly registries in Figure 3.
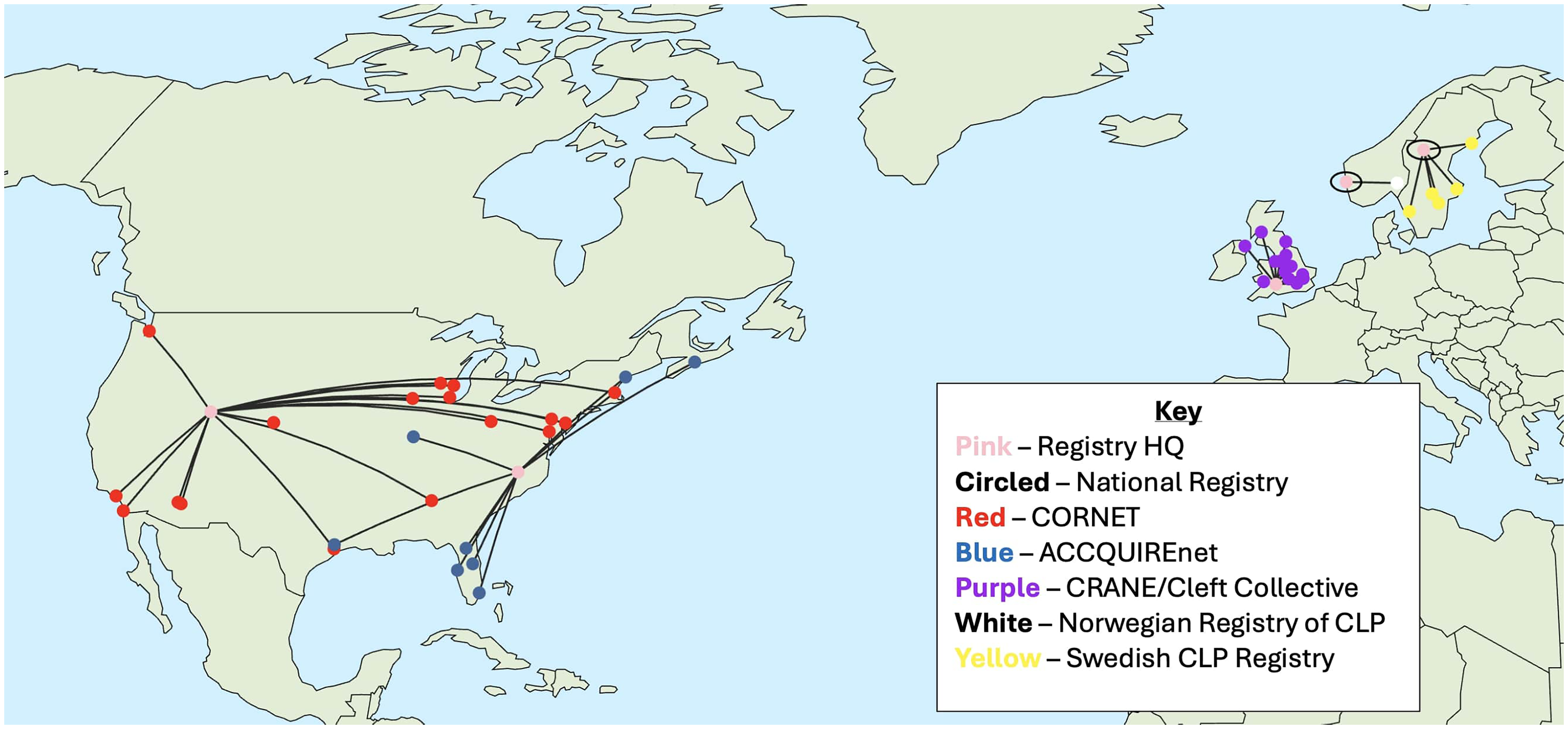
Sky Map of Data Collection Sites for Cleft-lip and Palate Registries.
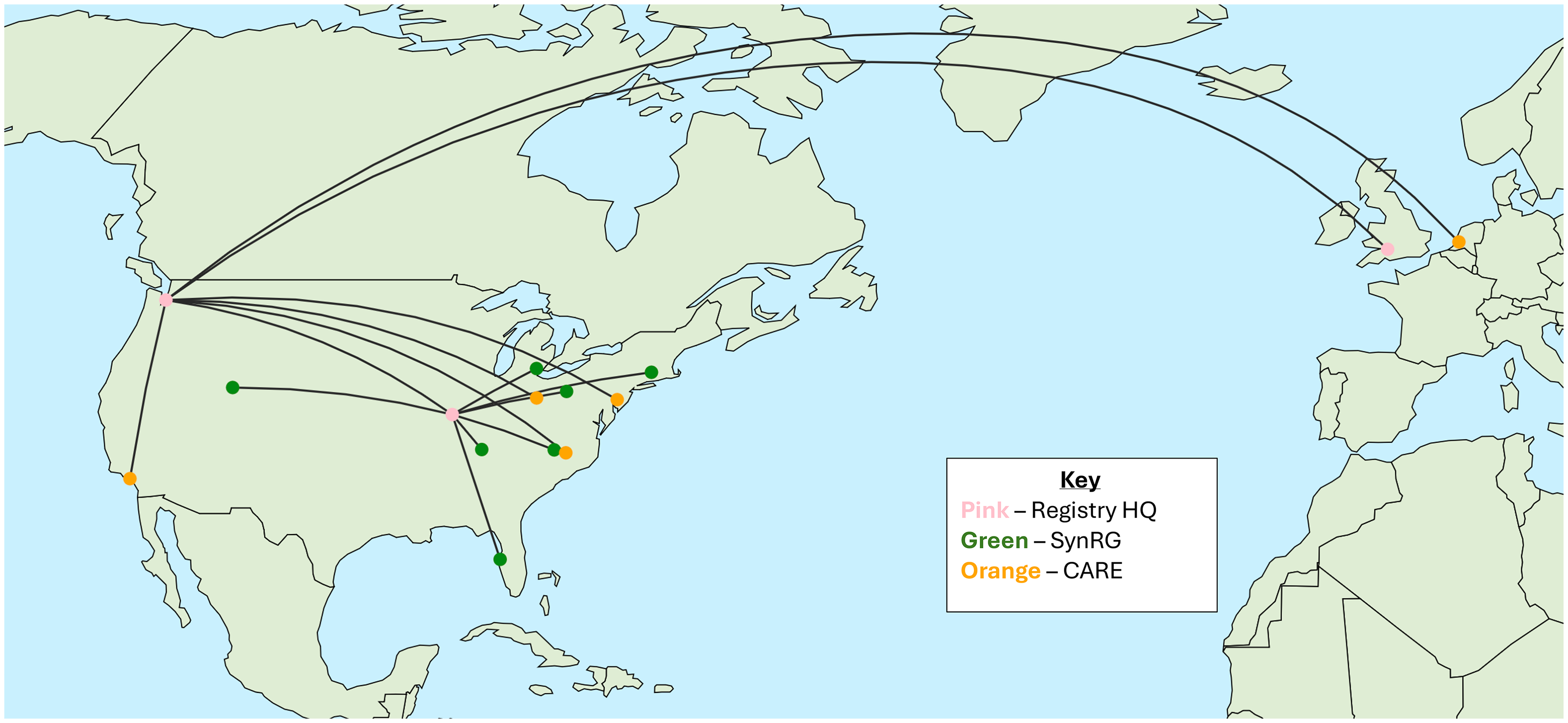
Sky Map of Data Collection Sites for Noncleft-lip and Palate Registries.
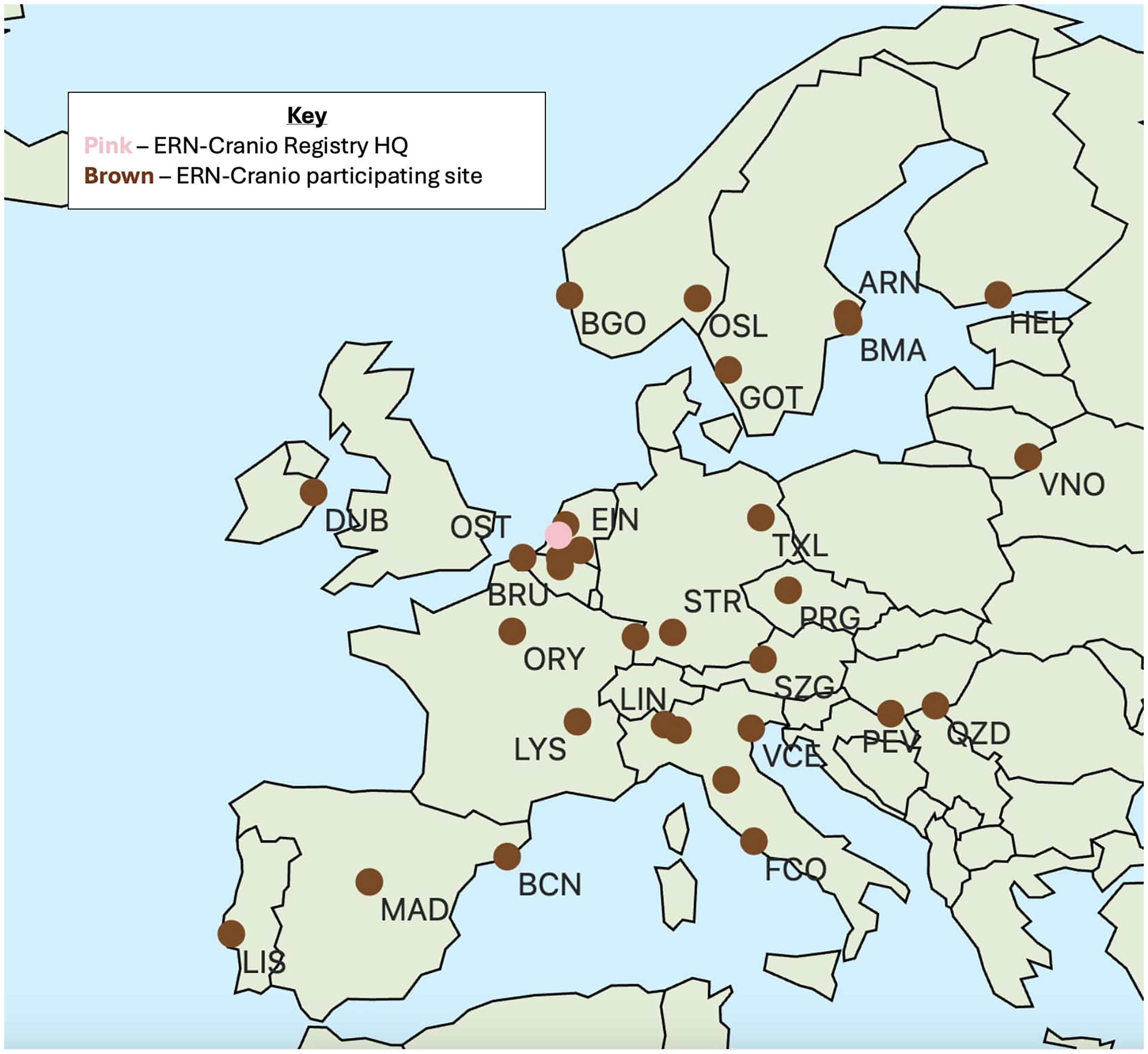
Sky Map of Data Collection Sites for ERN-Cranio Sites.
CLP Registries
The
General Characteristics of Prospective Registries for Congenital Craniofacial Anomalies.
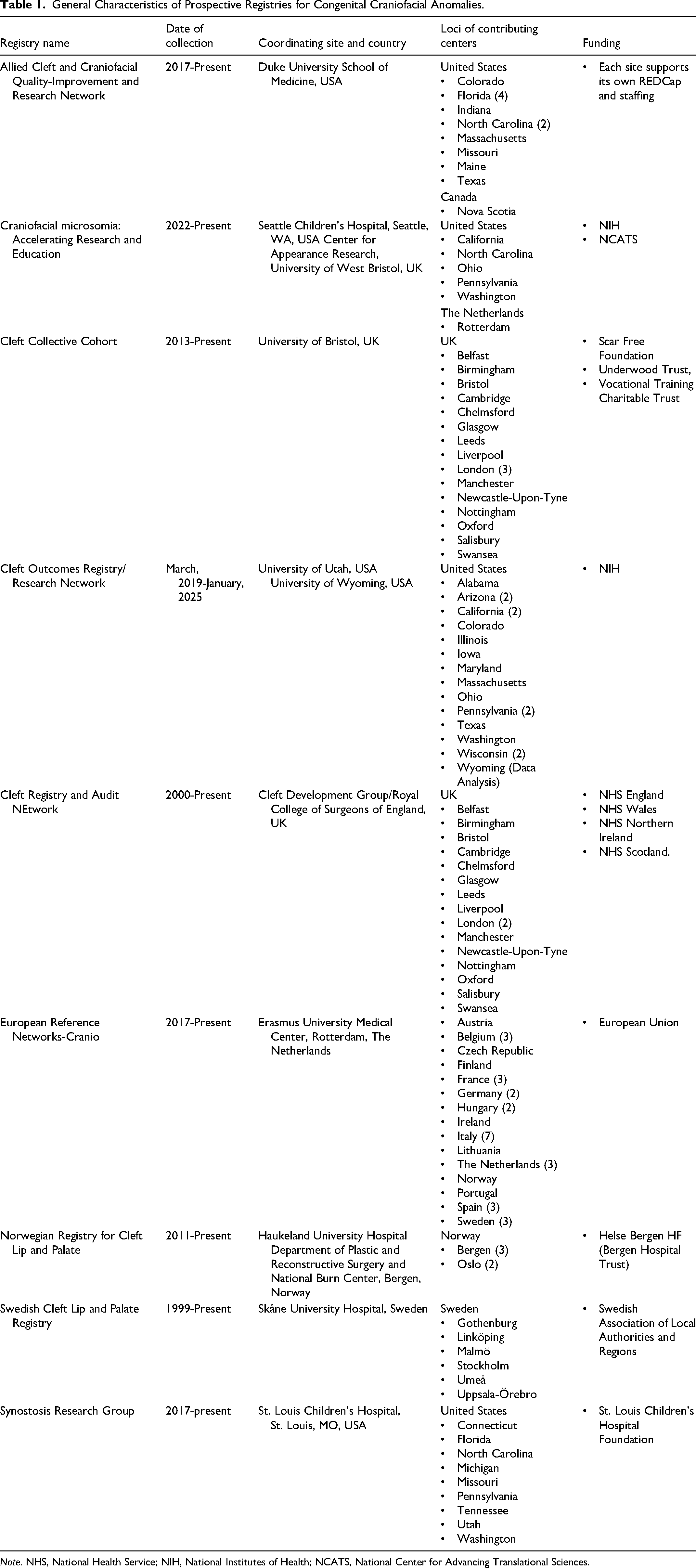
Note. NHS, National Health Service; NIH, National Institutes of Health; NCATS, National Center for Advancing Translational Sciences.
CRANE is a registry including over 25 000 patients with CLP in the United Kingdom.18,19 Its aims are to collect birth, demographic, and epidemiological information for all children born in the United Kingdom with CLP and to collect information on and audit cleft-related outcomes. Similarly to the Cleft Collective Cohort, all U.K.-based CLP centers participate (Table 1). Its funding is coordinated by the National Specialised Commissioning Group for England, the Welsh Health Specialised Service, and the Northern Ireland Specialist Services Commissioning Team; funding is raised via a levy calculated on a weighted per capita basis from the commissioning bodies in England, Wales, and Northern Ireland. Data is overseen by an independent Cleft Development Group comprised of patient representative groups, clinicians, and commissioners. This body ensures that CRANE is appropriately housed and funded. Quality is assured by a formal outlier process to manage any service that falls outside the expected performance range.
ACCQUIREnet consists of over 1000 patients with CLP. It aims to standardize outcomes assessment in cleft care by performing benchmarking for outcomes comparisons for 12 multidisciplinary teams across the United States and 1 in Canada (Table 1, Supplemental Table S2). 20 follow the International Consortium for Health Outcomes Measurement (ICHOM) Standard Set for the Comprehensive Appraisal of Cleft Care. Each data collection site financially supports its own REDCap and staffing. In terms of quality assurance, he coordinating team is focusing on reviewing data completeness, accuracy, and sustainability; participating teams receive annual performance reports. Eventually, the study will have an interventional arm, but as of September, 2024 it is purely observational; accordingly, it is registered as a prospective cohort with clinicaltrials.gov.
The CORNET registry is another CLP registry that has collected data on 1962 patients. 21 This registry is founded upon 2 goals: to help investigators understand the variability, progression, and current treatment practices for CLP, and to provide pilot and descriptive data necessary for hypothesis generation and study design for studies under development by CORNET. All 17 data collection sites are within the United States. CORNET is funded by the NIH. The registry's quality assurance mechanism was not available. The team behind CORNET has also undertaken a prospective outcomes study that includes additional data from 1189 of the 1962 participants.
The
The
Craniosynostosis Registries
The
Microsomia Registries
The
Multifocused Registries
European Reference Networks (ERNs) are a series of collaborations between European hospitals Europe which excel in managing rare diseases.13,26 ERN-Cranio is the specific ERN for disorders of the ear, neck, and throat, craniosynostosis, CLP, microsomia, and other rare congenital craniofacial anomalies. ERN-Cranio's goal is to centralize expertise about congenital craniofacial anomalies and improve health by leveraging multinational data. Patient data is collected from sites in the Netherlands, France, the United Kingdom, Spain, Sweden, Italy, Germany, Finland, Portugal, Austria, the Czech Republic, Hungary, Norway, Finland, and Lithuania. It is funded by the European Union. Information regarding the number of participants and quality assurance plan was unavailable.
Discussion
Craniofacial anomalies are relatively prevalent birth defects, yet treatment strategies remain difficult to optimize. 27 Prospective registries address gaps in outcomes research by tracking and refining therapeutic results; when assembled with robust methodology, registries may produce results superior to many observational studies, including chart reviews and low-powered RCTs. 28 This review illustrates the similarities and differences between prospective registries for congenital craniofacial anomalies worldwide.
Of 9 identified registries, 6 focused on CLP, 1 on craniosynostosis, 1 on craniofacial microsomia, and 1 on a range of craniofacial anomalies. Only European and U.S.-based registries were identified, with some participation from Canada, Australia, and New Zealand. 25 European CLP registries are the most organized; 4 of 6 identified CLP databases represent all government-supported cleft centers in their respective nation. Meanwhile, none of the 3 U.S. registries are nationally inclusive; though notably, ACCQUIREnet includes multinational data (United States and Canada).
The fact that most European registries began almost a decade earlier than U.S. registries likely traces to earlier efforts to coordinate cleft care. The centralization of CLP care in the United Kingdom began in 1998 with the Clinical Standards Advisory Group Cleft Lip and Palate Study. 29 Since this report, the number of cleft teams in the United Kingdom has consolidated from 57 to 17, making it easier to streamline the flow of information. 30 Many European countries facilitate consistent referral of patients with craniofacial anomalies to treatment by integrating treatment teams with national welfare systems. 31 In contrast, U.S. registries rely on research groups with widespread centers that report to a leading institution.
The most striking gap is the lack of representation of patients outside of North America and Europe. This is not to say that the majority of the world lacks craniofacial care entirely—there are dedicated cleft centers in Australia, Brazil, Canada, and New Zealand, but without large, prospective reporting schemas.32,33 Global nonprofit organizations like SmileTrain and Operation Smile are established in every continent except Antarctica, and the Noordhoff Craniofacial Foundation and the Chang Gung Craniofacial Center have done outstanding work to bolster cleft care throughout Asia, though their databases are internal and were not built for research (Smile Train Research and Innovation, personal communication, Sept. 9, 2024).34,35 Inclusion of all racial, ethnic, and geographical populations in research is paramount to equitable care, especially considering the ethnic disparities in CLP outcomes that already exist in the United States, alone. 36
We excluded a number of registries from analysis. The Pediatric Craniofacial Surgery Perioperative Registry was excluded because data was collected only at the time of hospitalization for surgery. However, data was gathered from 33 centers in the United States and Canada. The registry was formed by a group within the Society for Pediatric Anesthesia and holds data from 8794 patients predominately with craniosynostosis. 37 Also excluded were national nonprospective CLP registries; these included the Danish Facial Cleft Register and the database of the Dutch Association for Cleft Palate and Craniofacial Anomalies. Since Denmark and the Netherlands have organized their countries’ cleft care into 2 and 15 centers, respectively, they enroll virtually every individual with CLP. Lastly, we excluded registries built upon national birth data. This category included the National Birth Defect Prevention Study (NBDPS), European network of population-based registries for the epidemiological surveillance of congenital anomalies (EUROCAT), and Latin-American collaborative study of congenital malformations (ELCAMC), as well as craniofacial databases like the International Perinatal Database of Typical Oral Clefts, which pulls data from EUROCAT and NBDPS. These databases track prevalence patterns and risk factors for congenital anomalies such as maternal health, prenatal exposures, and genetics.38,39 Though they provide pools of participants for potential prospective study, 40 they are not designed to analyze outcomes.
There have also been massive, national and international studies on CLP patients and outcomes. Although they did not produce prospective registries, these investigations were instrumental in advancing patient care. The Eurocleft study, a 6-center retrospective review of patients with complete unilateral-CLP (UCLP), was a landmark work that inspired the creation of multiple studies with similar aims since its publication in the early 1990s. 41 The 2011 Americleft study was modeled after Eurocleft. 42 Similarly, the cross-sectional New Zealand Cleft Outcomes Study investigated surgical outcomes of children with CLP who underwent primary surgery at 1 of the 5 centers repairing clefts in New Zealand. 33 The Scandcleft group went a step further with a series of 3 RCTs spanning Denmark, Finland, Norway, Sweden, and the United Kingdom that compared 4 surgical protocols for UCLP. 43 All of these efforts have identified gaps in care that necessitate the creation of larger, ongoing registries—or, at least, defined guidelines for auditable data (L. Ayrey, personal communication, September 12, 2024).
These efforts may underlie our finding that two-thirds of identified registries were dedicated to CLP. While this statistic may be due in part to the higher prevalence of CLP (1:1000 live births)38,44 is compared with other craniofacial anomalies (craniosynostosis at 1:1700 and hemifacial microsomia at 1:3000-1:5600),45,46 landmark trials and the aforementioned centralization of cleft care in Europe laid the first stones for subsequent cleft registries. We speculate that registries for other craniofacial anomalies are less common because fewer foundations are already in place.
Our findings uncover several areas for improvement. First, expanding geographic representation within craniofacial registries is essential. Currently, the greater picture of global outcomes is obscured by geographic limitation. This imbalance precludes insights into the diversity of patient experiences; studies have shown that healthcare outcomes can vary based on geographic and cultural differences, making it imperative to include data from low- and middle-income countries in a comprehensive dataset.47,48 Participation from underrepresented countries will reduce biases, enhance understanding of outcomes, and allow more targeted resource allocation. It was difficult to obtain information regarding reporting rates and patient coverage during our search. National registries such the Swedish CLP Registry boast reporting rates of up to 97.5%, a figure presumably underpinned by its designation as a national quality registry that is overseen by the Swedish Association of Local Authorities and Regions. 49 Coverage and reporting rates for other registries were not collected as part of this study but should be noted in future registries to identify gaps in care.
Second, promoting national coordination in the United States is crucial for improving data quality and ensuring equitable care. Support from the American Academy of Pediatrics, the American Cleft Palate Association, and other organizations will be key to mobilizing task forces for this aim. The lack of a centralized, national registry hinders systematic tracking of outcomes and identification of best practices.27,50 A national coordination strategy would involve establishing a unified registry system with participation from all cleft and craniofacial centers, similar to European approaches. 27 This would facilitate data sharing, improve intracenter communication, and provide a standardized framework for outcome measurement, all leading to actionable insights for patients from all corners of our country.7,29 We believe this lofty goal is achievable under the paramount condition that all participating institutions approach the endeavor with a spirit of camaraderie. The fragmented nature of the American healthcare system makes organizing care and research for children with craniofacial anomalies challenging, so it is understandable that the leadership behind feats as massive and impressive as the described registries may be protective of their work. Indeed, one author of this publication is closely familiar with such ethical issues, as a co-principal investigator of SynRG (as disclosed). We encourage a united stance to elicit federal support for a U.S. registry for craniofacial anomalies. The sum of data from every state will enable a never-before-seen level of care for these children across our country.
Third, the similarities that do exist between active registries provide an avenue for creating a global, prospective pediatric craniofacial registry. This notion is not new; the WHO has been calling for international collaboration since the 1990s with their “International Collaboration on Oral Health,” and in 2000 with their proposal, “International Collaborative Research on Craniofacial Anomalies.” 12 This has been echoed by other leaders in the craniofacial world. 7 This work clarifies similarities between existing registries, which can and should be “harmonized,” as put by Shaw (2005), into one registry, diminishing the need to start from scratch. Each registry detailed above brings unique and vital data to the table—ranging from surgical outcomes to genetic analyses to psychosocial impacts—that will contribute to an overarching picture.
Combining and expanding these registries will yield challenges. There must be agreement upon organization, leadership, data collection, quality checks, and recruitment strategies. 13 Ideally, the leadership structure should stem from national organizations such Clinical Effectiveness Unit of the Royal College of Surgeons of England, as is the case for CRANE. Recruitment strategies should aim to include a diverse patient population from craniofacial centers of various sizes, geographic locations, and resources. Additionally, efforts to streamline recruitment should be made to avoid large lags in study timelines. 51 To accommodate settings where resources are limited, it may be prudent to follow ERN-Cranio's example and create 2 sets of outcomes measures: 1 with a minimum set of datapoints that is feasibly implemented in various settings, and a second optional set of additional assessments for centers able to complete them. 26 In time, as processes are streamlined and more support becomes available, smaller centers can “level up” to include the more advanced metrics. In the meantime, they are still able to contribute feedback to the registry system. Such a system is critical to ensure reliable data and high reporting degrees from all participating centers. The ICHOM standard sets for CLP and Craniofacial Microsomia were designed to be feasible in low-income countries, and may be an excellent place to start. 52 However, implementing the Standard Set carries its own challenges that need to be worked out over time, like deciding upon the best mode of survey delivery, mitigating the time burden of completing surveys, earning support from hospital leadership, fitting data collection into clinic workflow, etc. 53 Close international collaboration will also be required to come to a consensus on the mandatory categories and metrics that are satisfactory to participants of different cultures and languages.
Outcome metrics should be agreed upon for each craniofacial anomaly. When deciding upon key datapoints to collect, representatives from all stakeholder groups should be present. Cleft care teams are typically comprised of plastic surgeons, dentists, orthodontists, otolaryngologists, psychologists, audiologists, speech-language pathologists, geneticists, social workers, nurses, and advanced practice providers. For craniosynostosis teams, neurosurgeons and opthalmologists are also present. All of these providers, in addition to patient and family representatives, need to be involved in creating meaningful sets of datapoints and outcomes measures that are realistic and practical for long-term collection.
There must also be infrastructure for long-term support of study personnel, resource availability, and legal permissions. 13 Garnering financial support is perhaps the largest barrier to national and international registry creation. Our results have shown that the nationally organized registries in Europe are more frequently federally funded than U.S.-based registries. In the United States, individual institutions apply for grant funding through the NIH or their own hospital systems. This system does not support the inclusion of smaller cleft centers. The lack of a universal public healthcare system in America poses a challenge to widespread funding. While support from the American Academy of Pediatrics would be a coup, additional bolstering from the national government would likely be necessary. To this end, any research stemming from craniofacial registry data that has decreased the cost of care can be used to lobby for governmental support for stronger registries that might reduce costs even further.
A single registry will be a Herculean effort, but already there are votes of confidence in its conception.7,54 Our hope is that the evidence provided here may constitute a springboard for international unity in enhancing and advancing the care of all patients with craniofacial anomalies.
Our study has limitations. One is that the search strategy used to identify registries may not have been entirely comprehensive, as we did not search any databases aside from Embase and Google, and our search was conducted only in English and may not have captured registries published in other languages. Although a great strength of this work was the verification of data by registry coordinators, not all coordinators were able to be reached. In these cases, results were included as they appeared in the literature and online.
Conclusion
This review characterizes the global state of prospective registries for research on congenital craniofacial abnormalities. Our findings argue that the strength and organization of data vary by registry and country, though the present landscape exhibits potential for improvement of craniofacial research and patient outcomes. With this evidence, we advocate for nationally coordinated research to improve outcomes for children with craniofacial anomalies.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656251349881 - Supplemental material for The Current State of Prospective Registries for Congenital Craniofacial Anomalies: A Review
Supplemental material, sj-docx-1-cpc-10.1177_10556656251349881 for The Current State of Prospective Registries for Congenital Craniofacial Anomalies: A Review by Sophia Z Chryssofos, Arjun Mehendale, Kevin He and Tinna Kosoko-Thoroddsen, Gary B Skolnick, Lauren H Yaeger, Sybill D Naidoo, Kamlesh B Patel in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656251349881 - Supplemental material for The Current State of Prospective Registries for Congenital Craniofacial Anomalies: A Review
Supplemental material, sj-docx-2-cpc-10.1177_10556656251349881 for The Current State of Prospective Registries for Congenital Craniofacial Anomalies: A Review by Sophia Z Chryssofos, Arjun Mehendale, Kevin He and Tinna Kosoko-Thoroddsen, Gary B Skolnick, Lauren H Yaeger, Sybill D Naidoo, Kamlesh B Patel in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656251349881 - Supplemental material for The Current State of Prospective Registries for Congenital Craniofacial Anomalies: A Review
Supplemental material, sj-docx-3-cpc-10.1177_10556656251349881 for The Current State of Prospective Registries for Congenital Craniofacial Anomalies: A Review by Sophia Z Chryssofos, Arjun Mehendale, Kevin He and Tinna Kosoko-Thoroddsen, Gary B Skolnick, Lauren H Yaeger, Sybill D Naidoo, Kamlesh B Patel in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-4-cpc-10.1177_10556656251349881 - Supplemental material for The Current State of Prospective Registries for Congenital Craniofacial Anomalies: A Review
Supplemental material, sj-docx-4-cpc-10.1177_10556656251349881 for The Current State of Prospective Registries for Congenital Craniofacial Anomalies: A Review by Sophia Z Chryssofos, Arjun Mehendale, Kevin He and Tinna Kosoko-Thoroddsen, Gary B Skolnick, Lauren H Yaeger, Sybill D Naidoo, Kamlesh B Patel in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
Authors would like to acknowledge all who assisted in validating our data, including Dr Alexander Allori, Louise Ayrey, Dr Magnus Becker, Dr Kathy Chapman, Sarah Pollard, Amy Davies, Dr Kate Fitzsimons, Sissel Laastad Gavle, Dr Christer Kubon, Dr Craig Russell, Dr Åse Sivertsen, and Dr Paul Stricker.
Ethical Considerations
There are no human participants in this article and informed consent is not required.
Author Contributions
SC contributed to study design, data collection and verification, manuscript writing, and revision; AM, KH, and TKT contributed to data collection, manuscript writing, and revision. GBS and KBP contributed to study design, data verification, and manuscript writing and revision. LHY and SDN contributed to data collection and manuscript revision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Patel has been a consultant for Stryker CMF, and is a founding member and coprimary investigator of the Synostosis Research Group. All other authors have no conflicts of interest, financial or otherwise.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.