
Abstract
Objective
No studies have examined the effectiveness of platelet-rich plasma (PRP) alone and platelet-rich fibrin (PRF) without alveolar bone grafting or other bone substitutes for alveolar cleft repair during infancy. This study evaluated the effectiveness of autologous PRP/PRF on alveolar regeneration in infantile unilateral cleft lip and alveolus.
Design
Retrospective study.
Setting
Patients, Participants: A total of 56 patients with alveolar clefts were classified into the no PRP/PRF (which received gingivoperiosteoplasty [GPP] without PRP/PRF), PRP (which received GPP with PRP), and PRF (which received GPP with PRF) groups.
Interventions
Regarding preparation, 5 mL of blood was withdrawn, and 1 mL each of PRP and PRF was prepared via centrifugal separation. PRP was implanted in the alveolar cleft after loading it into a commercially available gelatin sponge, while PRF was implanted directly.
Main Outcome Measures
Postoperative bone formation was assessed using computed tomography and radiography for qualitative analysis.
Results
The new alveolar bone volume was higher in the PRF group than in the other groups; however, no differences were observed between the PRP, PRF, and control groups.
Conclusion
This study was performed without complication. However, no significant difference in bone formation was found between the PRP, PRF, and control groups.
Keywords
Introduction
Clefts of the alveolar process of the maxilla inhibit the eruption and maintenance of permanent dentition in patients with cleft lip and alveolus. Alveolar bone grafting (ABG) in the mixed dentition phase allows canine teeth to migrate and erupt through the cancellous bone. 1 Although its use has become common, the invasive procedure of harvesting the iliac bone places some burdens on patients. 2
Gingivoperiosteoplasty (GPP) was introduced to close alveolar clefts directly without bone grafting during infancy while promoting alveolar bone formation.3–6
However, its success rate in patients with unilateral clefts is reportedly 50–73% for experienced surgeons,7–9 and a growing need exists for materials to promote bone formation in the alveolar cleft. Platelet-rich plasma (PRP) and platelet-rich fibrin (PRF) have been reported to promote bone regeneration.10–13
Specifically, PRP and PRF have different characteristics, including the release peaks of the growth factors they contain. PRP forms clots but is fragile and unstable. In contrast, PRF is a solid gelatinous body with a fibrin matrix that slowly and continuously releases growth factors.14–16
Several studies have validated the effectiveness of PRP and PRF in enhancing bone regeneration in ABG for patients with cleft lip and palate.17–21
However, to our knowledge, no studies have examined the effectiveness and safety of PRP alone and PRF without ABG or other bone substitutes for alveolar cleft repair during infancy.
This study aimed to assess the effect of PRP on human infant periosteal cells (hiPCs) in patients with cleft lip and palate in vitro and clinically evaluate the effect of PRP and PRF with GPP on alveolar cleft reconstruction in patients with unilateral cleft lip and alveolus (UCLA).
Patients and Methods
Preparation of PRP and PRF
Whole blood samples (5 mL) were collected in a 10-mL tube without an anticoagulant from patients with UCLA during surgery. PRP was prepared using a traditional two-step centrifugation procedure. 9 Briefly, the samples were initially centrifuged at 350 × g for 7 min (KUBOTA CORPORATION tabletop centrifuge 2420, Tokyo, Japan). The buffy coat, which is the intermediate layer with an increased platelet concentration, was transferred with a small amount of the supernatant to a new tube and centrifuged at 1500 × g for 5 min(Figure 1A). Next, the bottom layer (approximately 1 ml) was collected as the PRP, while the remaining supernatant was used as platelet-poor plasma (PPP) (approximately 1 mL) (Figure 1B, C). During the surgery, PRP was implanted after being impregnated into a commercially available gelatin sponge (Gelfoam®, Pfizer Inc, NY, USA) (Figure 1D).
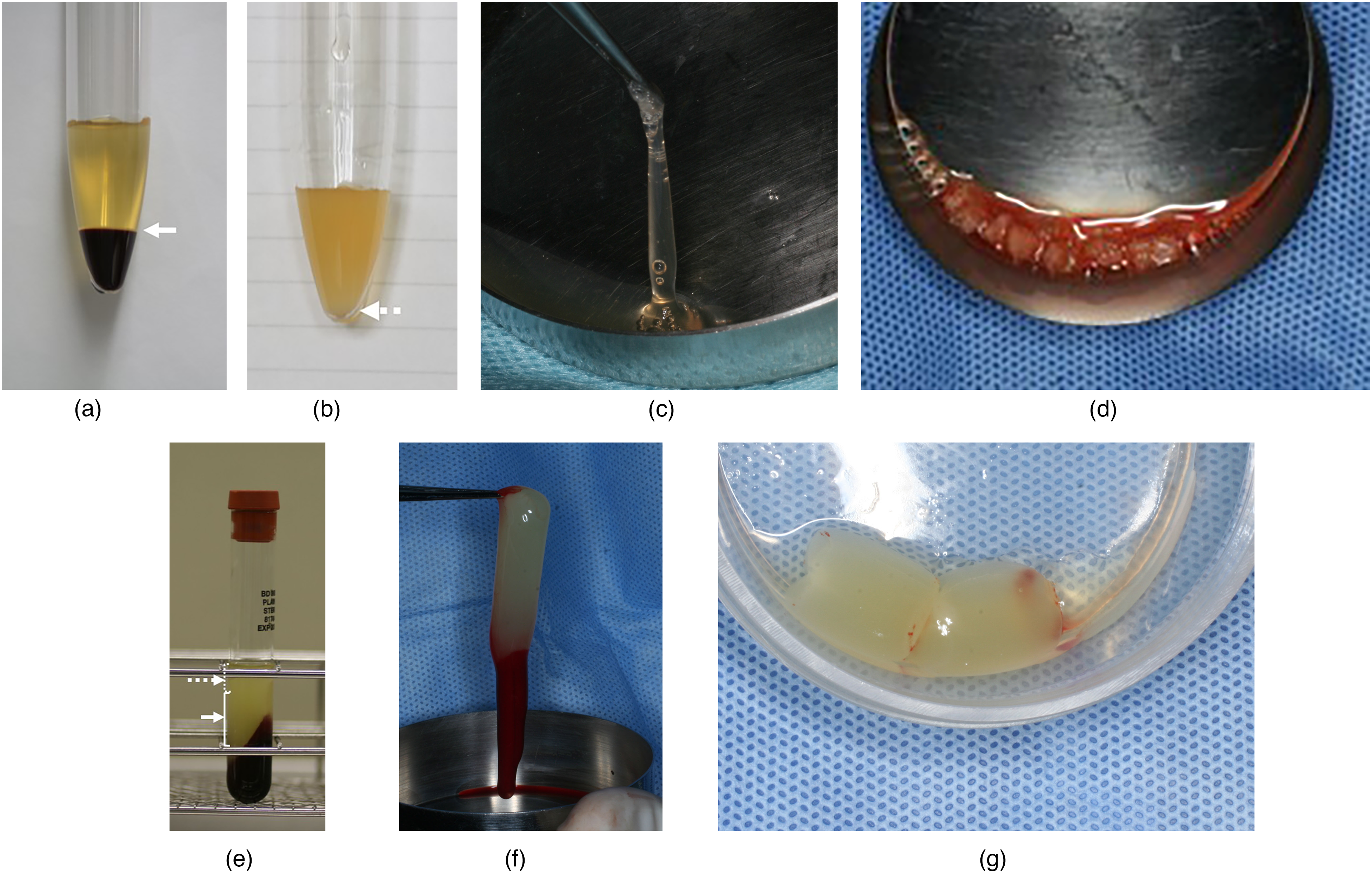
PRP and PRF. (A) The buffy coat which is the intermediate layer with an increased platelet concentration after the first centrifuge of whole blood (white arrow). The blood cell component of the lower layer was removed. (B) Subsequently, the buffy coat was transferred with a small amount of the supernatant to a new tube and centrifuged. After the second centrifuge, the bottom layer (approximately 1 ml) was collected as the PRP (white dotted arrow). (C) Collected PRP. (D) PRP was implanted after being impregnated into a commercially available gelatin sponge. (E) PRF (white arrow) under the upper layer of the PPP (white dotted arrow) after centrifugation. (F) PRF with blood cell components pinched with a forceps from inside a tube. (G) PRF obtained after removal of blood cell components. PRP, platelet-rich plasma; PRF, platelet-rich fibrin; PPP, platelet-poor plasma.
PRF was prepared by centrifugation at 400 × g for 10 min as previously described.22,23 After centrifugation, the tubes were stored at 4 °C until transplantation. The second layer, a non-transparent white clot under the upper layer of the PPP, was collected as the PRF gel immediately before transplantation (Figure 1E). PRF gel clumped under the upper layer of the PPP was picked up with forceps, and the lower portion attached to blood cell components was cut with scissors to obtain the PRF particles (Figure 1F, G). To verify the concentration rate of PRP used in this method, samples were obtained preoperatively under the same conditions, and the number of platelets and concentrations of cytokines in PRP and PPP were measured. The concentrations of each growth factor were determined using specific Quantikine enzyme-linked immunosorbent assay kits for platelet-derived growth factor (PDGF)-bb, vascular endothelial growth factor (VEGF), transforming growth factor (TGF)-β1, and TGF-β2 (R&D Systems, MN, USA). Standards and samples were accurately assayed in duplicates for each growth factor, and the mean values were calculated.
Cell Isolation and Culture
Alveolar periosteum samples were obtained from excess mucoperiosteum discarded during lip repair and GPP in patients with UCLA (Supplementary Digital Content 1A) and harvested microscopically (Supplementary Digital Content 1B, C). Next, hiPCs were isolated after fine mincing and cultured in Dulbecco's Modified Eagle's Media (DMEM; Sigma-Aldrich, MO, USA) supplemented with 10% fetal bovine serum (FBS; Gibco Life Technologies Co., NY, USA), 100 μM ascorbic acid, and 1% antibiotic antimycotic solution (AMS; Fujifilm Wako Pure Chemical Corp, Tokyo, Japan) in 5% CO2 at 37 °C. They were routinely passaged when the culture reached confluency. The expansion culture medium was changed every 3 days, and hiPCs were passaged up to 3 times. Specifically, the total cell volume for storage was 5 × 105 to 1 × 106/mL.
Proliferation and Mineralization Assay
The hiPCs were seeded into 24-well plates (Iwaki Japan, Shizuoka, Japan) at 3 × 104 cells/well and cultured in DMEM without FBS, supplemented with 100 μM ascorbic acid and 1% AMS, in 5% CO2 at 37 °C. Five different treatments were administered as follows: 1% PRP, 5% PRP, 1% PPP, 5% PPP, and a negative control. The media containing different percentages of PRP were replaced every 3 days. To evaluate cell proliferation, cell counting was performed using the IN Cell Analyzer 2000 (GE Healthcare, NJ, USA) every 1–6 weeks after seeding. Mineralization was assessed every 1–4 weeks—for which cells were fixed with cold acetone/methanol fixation solution—using alizarin red S (Sigma-Aldrich, Castle Hill, Australia) staining to visualize extracellular calcium deposition. After fixation in 100% ethanol and treatment with 1% alizarin red S, the alizarin red-mineralized nodules were dissolved by incubating the samples in 1 mL of 10% cetypyridinium chloride (Sigma-Aldrich, Castle Hill, NSW, Australia) buffer for 30 min. Subsequently, the solution was removed, and 100 µL aliquots in triplicate were transferred to a 96-well plate before measuring absorbance at 550 nm using a microplate reader (Tecan Group Ltd, Zürich, Switzerland).
Immunohistochemical Analysis of PRP and PPP Supernatant Liquids
After fixation in 10% buffered formalin, the collected supernatant liquid samples from the cells treated with PRP and PPP were decalcified and sectioned in paraffin blocks for hematoxylin and eosin (H&E) staining. Type I collagen was stained with primary rabbit polyclonal anti-collagen I antibodies (Bioss, MA, USA).
Patients
Between 2003 and 2014, patients with UCLA and alveolar clefts extending over the incisive foramen underwent cheiloplasty and GPP with or without PRP/PRF during their primary surgery, which was performed by a single surgeon.
Patients are divided into three groups. Group 1 (GPP without PRP/PRF) did not receive transplantation of PRP/PRF from 2003 to 2008; Group 2(GPP with PRP) received transplantation of PRP from 2009 to 2012; and Group 3 (GPP with PRF) received transplantation of PRF from 2013 to 2014 (Figure 2).

(A) GPP without PRP/PRF (Group 1). (B) GPP with PRP and gelatin sponge (Group 2) loaded with PRP (white arrow). (C) GPP with PRF (Group 3) (white arrow). PRP, platelet-rich plasma; PRF, platelet-rich fibrin; UCLA, unilateral cleft lip and alveolus; GPP, gingivoperiosteoplasty.
GPP was performed in cases alveolar gaps was 2 mm or less. The alveolar gap was defined as the distance between the alveolar crests on the cleft and non-cleft sides. Nasoalveolar molding (NAM) was performed when the pre-op gap was greater than 2 mm. However, if the gap was greater than 2 mm after NAM, the patient did not undergo GPP and was excluded from the study. GPP with cheiloplasty was performed under general anesthesia. An incision was made, and the gingival mucoperiosteal flap was elevated using the standard procedure. 3 During the surgery, PRP was implanted after loading it onto a commercially available gelatin sponge (Gelfoam®) (Figure 1D), while PRF was implanted directly, which were closed using gingival mucoperiosteal flaps.
Radiographical Evaluation
Radiological evaluations were performed 5 years postoperatively. Bone quantity and quality were evaluated radiographically via bone volume assessment using computed tomography (CT) (Aquilion One TSX-301C; Canon Medical Systems Co., Tochigi, Japan).24–26
CT was performed 2 times, immediately after GPP with cheiloplasty and when the patient was 5 years of age. CT was limited to beneath the level of the floor of the orbit to minimize radiation exposure. Data from the axial plane of the CT were used to generate three-dimensional images facilitated by CT imaging software (Ziostation2, version 2.4.3.4 Ziosoft Inc., Tokyo, Japan) to visualize the configuration and anatomy of the alveolar cleft defect, with the following technical parameters: SD 10 HU, 80 kVp, 160–270 mA, a field of 16 × 6 cm, and a voxel size of 0.25 mm. The areas of bone and defects on the cleft side were traced on each axial plane. While the superior limit of the CT slice was set at the same level as the nasal floor on the opposite side, the inferior limit was set at the crest of the alveolar bone (Figure 3A). In slices where the alveolar shape was visible or could be estimated based on the remaining alveolus on the opposite side, the following three lines were selected based on anatomic landmarks to broadly delineate the alveolar cleft and define the area of interest (Figure 3B): (1) a midsagittal line; (2) an anterior line drawn perpendicular to the midsagittal line at the most anterior point of the alveolus; and (3) a posterior line drawn perpendicular to the midsagittal line at the most posterior end of the alveolar defect.25,26
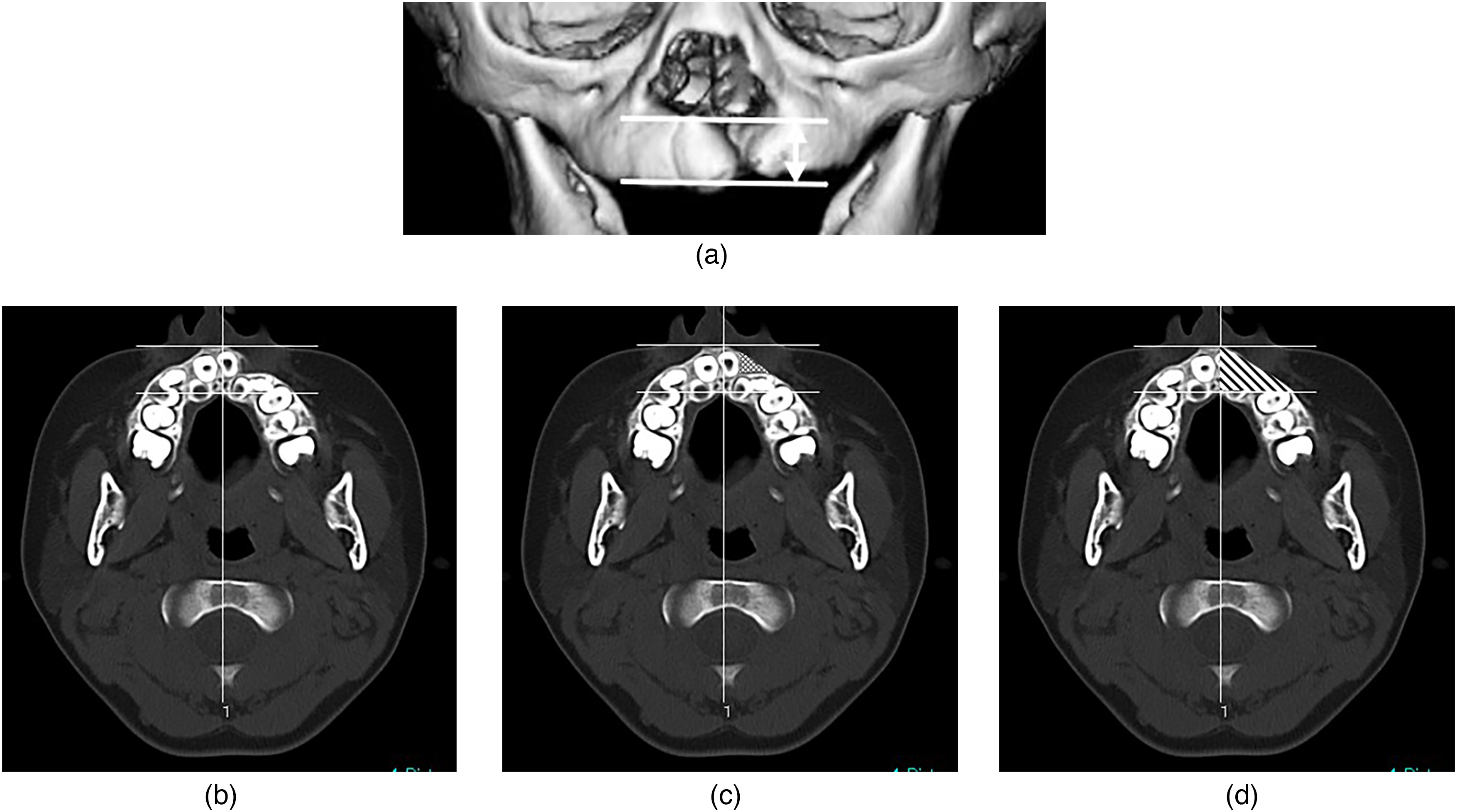
Radiographical evaluation. (A) Superior and inferior limits of the measurement area of the defect volume and scan area on computed tomography. For volume measurement, the superior limit was set at the same level as the nasal floor on the opposite side, while the inferior limit was set at the crest of the alveolar bone (a double-headed white arrow). (B) Landmarks on the x- and y-planes used to define the alveolar cleft. (C) Determination of the actual defect area on the cleft side (dotted area). (D) Determination of the virtual total bone volume on the cleft side (shaded area). X, midsagittal line; Y, anterior line; and Z, posterior line.
In such slices, the anterior margin on the cleft side was created by connecting the most anterior portions of the remaining alveolus or by setting the margin as the line tangential to the outer surface of the remaining lateral alveolus from the most anterior portion of the remaining medial alveolus. 2
Subsequently, the actual bone defect and virtual total bone areas on the cleft side were determined as dotted and shaded areas, respectively (Figure 3C, D). The actual bone defect and virtual total bone volumes on the cleft side were calculated by summing all areas multiplied by 0.2 mm slice thickness. Specifically, the ratio of bone formation on the cleft side was defined as follows:

Data of all patients were obtained and analyzed by two researchers who were blinded to the treatment received by the patients. The mean of two sets of measurements for each patient was used to compare the three groups.
Statistical Analysis
Radiological evaluations of the three groups were compared using the Kruskal–Wallis test, while the Mann–Whitney U-test with Bonferroni correction was used to compare their characteristics. All analyses were performed using IBM SPSS Statistics for Windows, version 22 (IBM Corp., Armonk, NY, USA). Statistical significance was set at P < 0.05.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki. Permission for this study was granted by the IRB (Specified Nonprofit Corporation Advanced Medical Promotion Organization, Certified Committee for Regenerative Medicine, etc, in Nagoya No.: PC3150413). All samples were obtained from patients with UCLA according to the approved guidelines of the Ethics Committee of our institution (Approval No.: 11-126). Written consent was obtained from the parents of all patients.
Results
Measurement of Platelet and Cytokines in the Whole Blood, PRP, and PPP
Ten PRP samples were obtained from the whole blood. The mean concentrations of platelets, PDGF-bb, VEGF, TGF-β1, and TGF-β2 were 108.4 ± 15.2 × 104 cells/μL, 12709 ± 2476.2 pg/mL, 1362.1 ± 764.4 pg/mL, 68.5 ± 5.5 ng/mL, and 903.7 ± 275.5 pg/mL, respectively, in PRP and 39.1 ± 10.7 × 104 cells/μL, 7803.8 ± 1809.0 pg/mL, 497.6 ± 151.7 pg/mL, 26.3 ± 7.7 ng/mL, and 389.3 ± 53.3 pg/mL, respectively, in the whole blood. Specifically, the values were approximately 2–3-fold higher in PRP than in the whole blood. Meanwhile, the mean concentrations of platelets, PDGF-bb, VEGF, TGFβ1, and TGFβ2 in PPP were 0.2 ± 0.0 × 104 cells/μL, 975.3 ± 493.5 pg/mL, 151.5 ± 139.1 pg/mL, 14.5 ± 139.1 ng/mL, and <224.0 pg/mL, respectively (Figure 4).
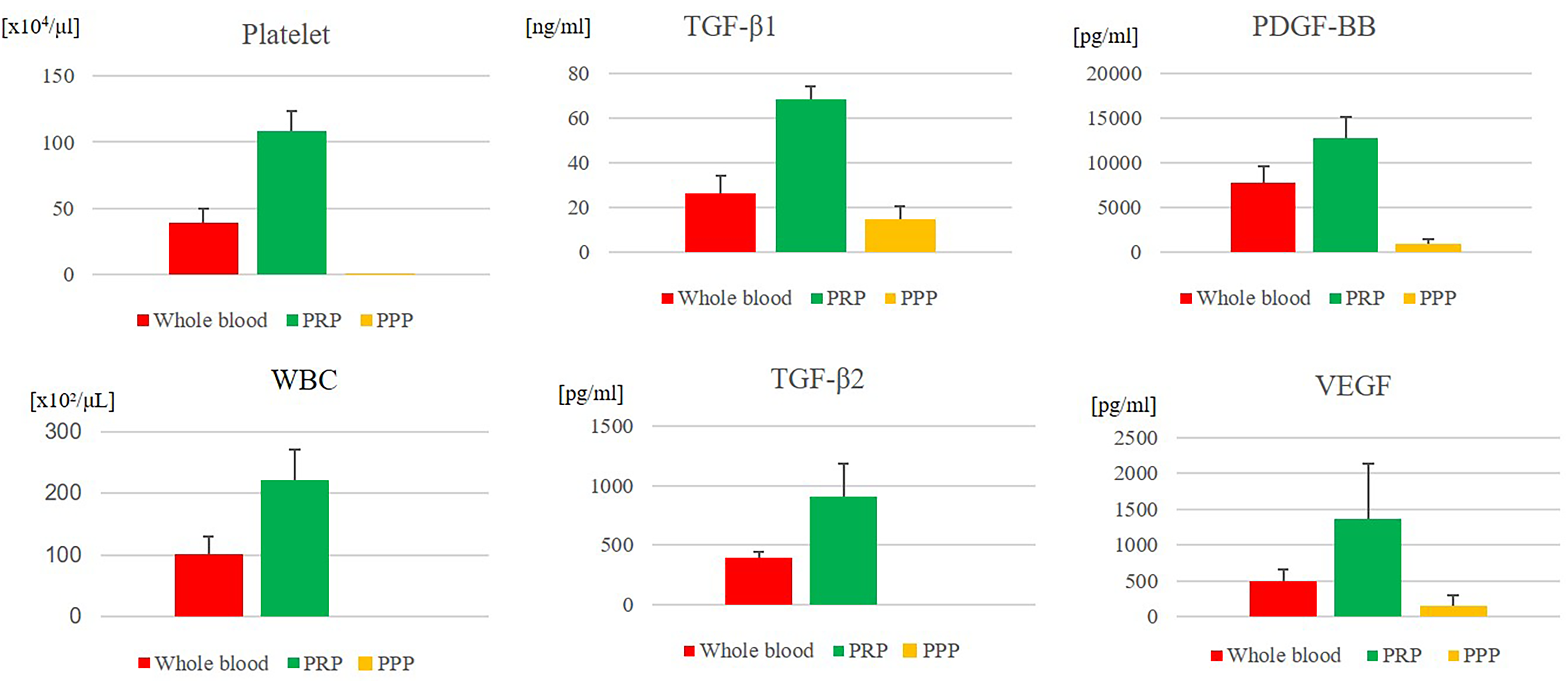
Platelet, white blood cell, and cytokines concentrations on the whole blood, PRP, and PPP (N = 10). PRP, platelet-rich plasma; PPP, platelet-poor plasma.
Proliferation and Mineralization Assay
The effects of PRP and PPP on hiPC proliferation are shown as growth curves measured every 1–6 weeks (Figure 5A, Supplementary Digital Content 2). Higher proliferation of hiPCs was observed when the culture medium contained 5% PRP than with the other treatments. Cells treated with 5% PRP showed relatively higher mineralization than those with the other treatments. Specifically, cells treated with 5% PRP and cultured for 4 weeks reached higher maximum mineralization than those cultured for other periods (Figure 5B, Supplementary Digital Content 3A).
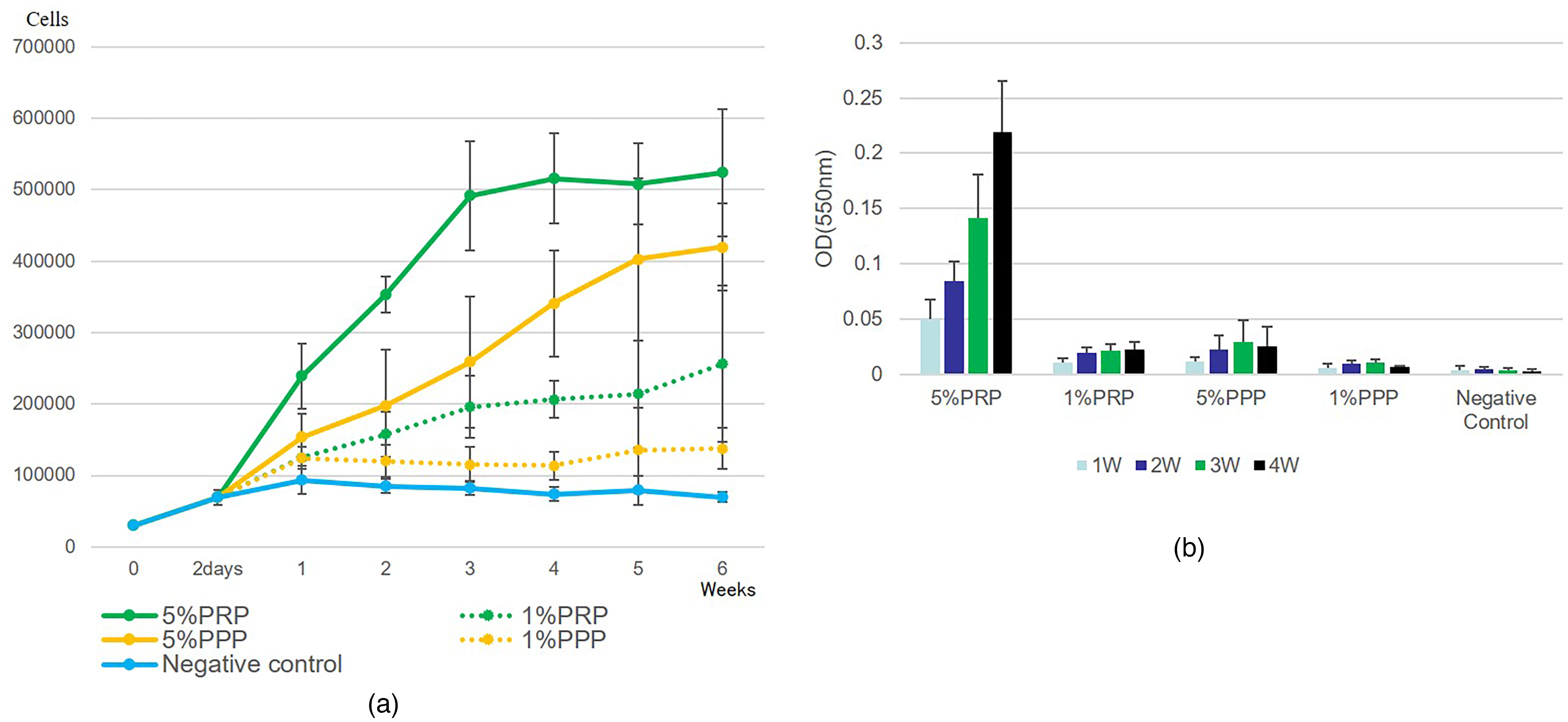
Proliferation and mineralization assay of hiPCs. (A) Proliferation and (B) mineralization assays of hiPCs cultured without FBS. hiPC, human infant periosteal cells; FBS, fetal bovine serum.
Immunohistochemistry Analysis of the Supernatant Liquid in PRP and PPP
The supernatant of 5% PRP was stained with type I collagen, while that of 5% PPP was not stained (Supplementary Digital Content 3B).
Patients
A total of 56 patients (male/female: 33/23) with UCLA were included in this study: group 1, 17 patients (8/9); group 2, 23 patients (16/7); and group 3, 16 patients (9/7).
The median (interquartile range) age of all patients at primary operation was 5.0 (5.0–6.75) months. Specifically, the median (interquartile range) ages of patients in groups 1, 2, and 3 were 5.0 (5.0–6.0), 6.0 (6.0–6.0), and 6.0 (6.0–7.0) months, respectively (Table 1). All patients had an uneventful postoperative course.
Evaluation of Bone Formation.

*P = .00.
Radiographical Evaluation
Median preoperative/postoperative virtual total bone volumes on the cleft side in groups 1, 2, and 3 were 880.9/2033.6, 958.5/2086.7, and 1079.3/2094.25 mm3, respectively. In contrast, median preoperative/postoperative actual bone defect volumes on the cleft side in groups 1, 2, and 3 were 341.9/306.6, 317.3/317.2, and 325.2/226.3 mm3, respectively. The preoperative/postoperative ratios of bone formation on the cleft side in groups 1, 2, and 3 were 61.0/84.5%, 65.8/83.9%, and 69.1/89.6%, respectively. No significant difference in the ratio of bone volume on the cleft side was found between the three groups (Table 1, Supplementary Digital Content 4).
Additional bone grafting was performed in 5/17 (29.4%), 9/23 (39.1%), and 3/16 (18.8%) cases in groups 1, 2, and 3, respectively.
Discussion
PRP has been suggested to increase osteogenic differentiation during hiPC proliferation in vitro. However, no significant effect of PRP or PRF with GPP in alveolar cleft reconstruction was observed in patients with UCLA in our clinical evaluation.
PRP contains many platelet growth factors that play important roles in bone regeneration. Previous in vitro studies have shown a release of growth factors, including TGF-β, PDGF, VEGF, bone morphogenetic protein 2, and abundant insulin-like growth factor 1 in PRP, indicating osteogenic potential.23,27–30 These cytokines play a fundamental role in the initial mechanisms due to their capacity to stimulate cell migration, proliferation, and bone tissue formation. 14 Here, PRP, which included these cytokines, induced high proliferation and mineralization of hiPCs. Additionally, hiPCs treated with 5% PRP showed relatively higher proliferation and mineralization than those with different treatments. The supernatant of hiPCs treated with 5% PRP was stained with type I collagen, while that of those treated with 5% PPP was not stained. Since collagen I is one of the major structural components of bone and is widely accepted as a marker for osteogenic differentiation, the cells treated with 5% PRP demonstrated higher proliferation and mineralization than others. Determining the optimal PRP concentration is important as the concentration to be added during surgery depends on this factor.
However, the actual implantation of PRP requires a material to hold it for some period. Considering this, using PRF, which has a performance similar to PRP and slowly releases growth factors, might be desirable. The fibrin networks of PRF might support an increase in postoperative bone formation as an osteoconductive scaffold, inducing fibrin matrix remodeling and promoting the secretion of a collagen matrix. 23 Several studies have validated the effectiveness of PRF in enhancing bone regeneration in autologous bone grafts and other bone substitutes,17–21 while some reports have shown negative results.31,32
PRF exhibits high reproducibility and does not require expensive equipment or advanced skills. It is also an autologous, safe, and cost-effective source of growth factors. However, accurately measuring cytokine concentrations in PRF is unfeasible because the fibrin networks of PRF cannot be completely removed.
Clinically, this study showed the production of infant PRP/PRF and the implantation of only PRP/PRF for cleft alveoli for the first time. However, no statistically significant difference in alveolar bone formation for cleft alveolus was found between the non-PRP/PRF, PRP, and PRF groups. The simple release of growth factors along with PRF and PRP into the alveoli may be insufficient to promote long-term bone regeneration. Therefore, materials for sustained growth factor release are required in the future. 33
Regarding additional bone grafting, group 3 had less surgery than the other groups. The bone formation rate may have been influenced by the fact that group 3 had a higher rate than the other groups, although no statistical advantage was found.
This study has some limitations. First, the sample size is small. Second, accurately measuring cytokine concentrations in PRF is impossible because the fibrin network of PRF cannot be completely removed. Third, the experimental system was limited by the small volume of whole blood and the total amount of PRP.
In conclusion, hiPCs treated with 5% PRP had a significantly higher proliferative capacity and osteogenic activity than those subjected to other treatments in a culture environment without FBS. However, no significant difference in bone formation was found between the PRP, PRF, and control groups.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261417033 - Supplemental material for Implantation of Infant Platelet-Rich Plasma/Fibrin with Gingivoperiosteoplasty in Patients with Unilateral Cleft Lip and Alveolus
Supplemental material, sj-docx-1-cpc-10.1177_10556656261417033 for Implantation of Infant Platelet-Rich Plasma/Fibrin with Gingivoperiosteoplasty in Patients with Unilateral Cleft Lip and Alveolus by Shinji Kobayashi, Yuichiro Yabuki, Madoka Sugiyama, Atuko Fukui and Takashi Hirakawa in The Cleft Palate Craniofacial Journal
Footnotes
Ethical Approval
Data from all patients who underwent the aforementioned treatment at the Kanagawa Children's Medical Center were retrospectively reviewed. This study was conducted in accordance with the Declaration of Helsinki. Permission for this study was granted by the Japanese Association for the Promotion of State-of-the-Art in Medicine (Institutional Review Board No.: PC3150413). All samples were obtained from patients with unilateral cleft lip and alveolus according to the approved guidelines of the Ethics Committee of our institution (Approval No.: 11-126). Written consent was obtained from the parents of all patients.
Consent to Participate
The need for informed consent was waived by the review board because of the retrospective study design.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Japan society for the promotion of science Grants-in-Aid for Scientific Research Grant Numbers JP17K11561 and JP20K09857.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.