
Abstract
Background
Syndromic midface hypoplasia often includes a high or fragile palate that is vulnerable during midfacial disimpaction.
Solution
We created a patient-specific palatal protection plate produced through a fully digital workflow to stabilize and protect the palate.
What we did
After using conventional plates from 2022 to 2024, we implemented a digital design and printing workflow in 2025 and added suction-catheter sleeves to the Rowe forceps branches to improve retention.
Keywords
What We Do
Syndromic craniosynostosis conditions such as Crouzon, Pfeiffer, and Apert syndromes typically present with midface hypoplasia and characteristic palatal features. These include a high or narrow palatal vault, clefts, and postoperative scarring, all of which reduce the structural resistance of the palate. 1 During Le Fort III osteotomy or Wassmund III osteotomy and midfacial distraction, the nasomaxillary complex is mobilized using Rowe disimpaction forceps, a manoeuvre that can exert considerable pressure on the palatal vault. 2 In children with reduced palatal thickness or increased vault height, this may result in mucosal tears or perforation. Prior to the use of any palatal protection plate, 3 patients in our department sustained palatal injuries during midfacial disimpaction. Two patients developed mucosal damage, while in one patient, a previously repaired palatal cleft dehisced intraoperatively. These events highlighted the vulnerability of the palatal vault in syndromic patients and prompted the development of a protective strategy.
Similar concepts for patient-specific intraoral protection have been described previously for Le Fort I osteotomies in patients with cleft lip and palate. Between 2020 and 2023, reports of custom-made maxillary disimpaction splints, including the technique described by Jolly et al, 3 demonstrated the usefulness of impression-based protective plates for Le Fort I mobilization. These earlier techniques resemble our initial conventional approach were primarily designed for Le Fort I procedures and did not incorporate a digital workflow.
Our clinical need arose between 2022 and 2026, when we treated 9 children with syndromic midface hypoplasia, due to Crouzon syndrome, Pfeiffer syndrome, or Apert syndrome, requiring Le Fort III osteotomy or Wassmund III osteotomy and midfacial distraction. All presented with palatal anatomy that offered limited resistance to disimpaction forces. The combination of tall palatal vaults, narrow transverse dimensions, and previous palatal surgery made these children particularly vulnerable to injury. 4 To reduce this risk, we developed a rigid palatal protection plate that engages the dentition, distributes mechanical forces, and incorporates lateral guiding grooves for controlled seating of the Rowe forceps.
From 2022 to 2024, conventionally fabricated palatal protection plates based on alginate impressions were introduced (Figure 1).

Conventionally fabricated palatal protection plates created from alginate impressions.
However, impression taking was often uncomfortable in pediatric patients, especially in children with limited oral aperture or strong gag reflexes. Manual fabrication also resulted in variability in plate thickness and rigidity. These challenges prompted us to seek a more reproducible and patient-friendly approach.
In early 2025, we transitioned to a fully digital workflow. Intraoral scanning replaced impression taking, and virtual modeling was performed in Blender (Blender Foundation; available at: https://www.blender.org), an open-source 3D modeling and mesh-editing software widely used for medical and engineering applications.
The scanned anatomy was used to create a precisely fitting palatal baseplate, and rigid extensions around the dentition ensured stable positioning. The palatal section was selectively thickened to provide sufficient rigidity. Two parallel grooves were designed along with the lateral aspects of the plate to guide the Rowe forceps. Once the virtual model was finalized, it was exported as an STL file (Figure 2).
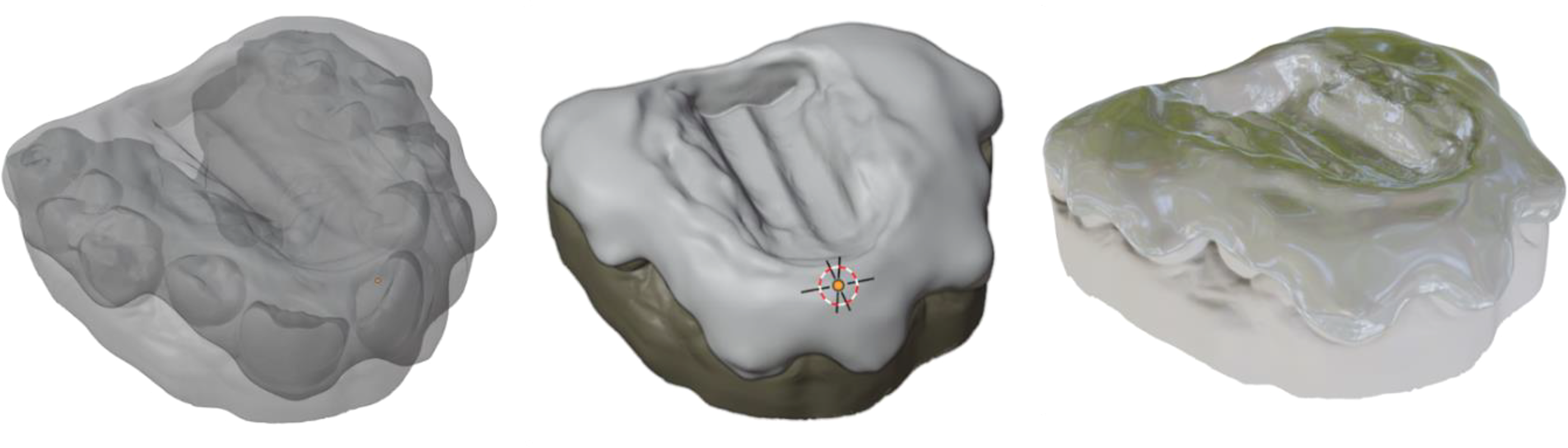
Digital design process and 3D printed palatal protection plates made from rigid biocompatible resin.
The plates were printed on an SLA 3D printer using a rigid biocompatible resin. After printing, they were washed, post-cured, and manually smoothed to eliminate sharp edges. The workflow provided consistent results and produced plates with uniform rigidity and reproducible geometry. In all patients treated with both conventional and digital plates, no palatal perforations or mucosal tears occurred. Surgeons noted improved intraoperative handling, more stable forceps guidance, and more controlled force transmission with the digitally designed plates.
An additional improvement was the placement of short segments of suction catheters over the branches of the Rowe forceps. This step required only minimal preparation but greatly increased the friction between the instrument and the grooves of the plate. Without the catheter sleeves, the smooth metal surface of the forceps sometimes slid against the resin, particularly in cases with steep palatal vaults. The catheter segments allowed the forceps to seat more securely, improved tactile control, and reduced the risk of sudden displacement during disimpaction (Figure 3).
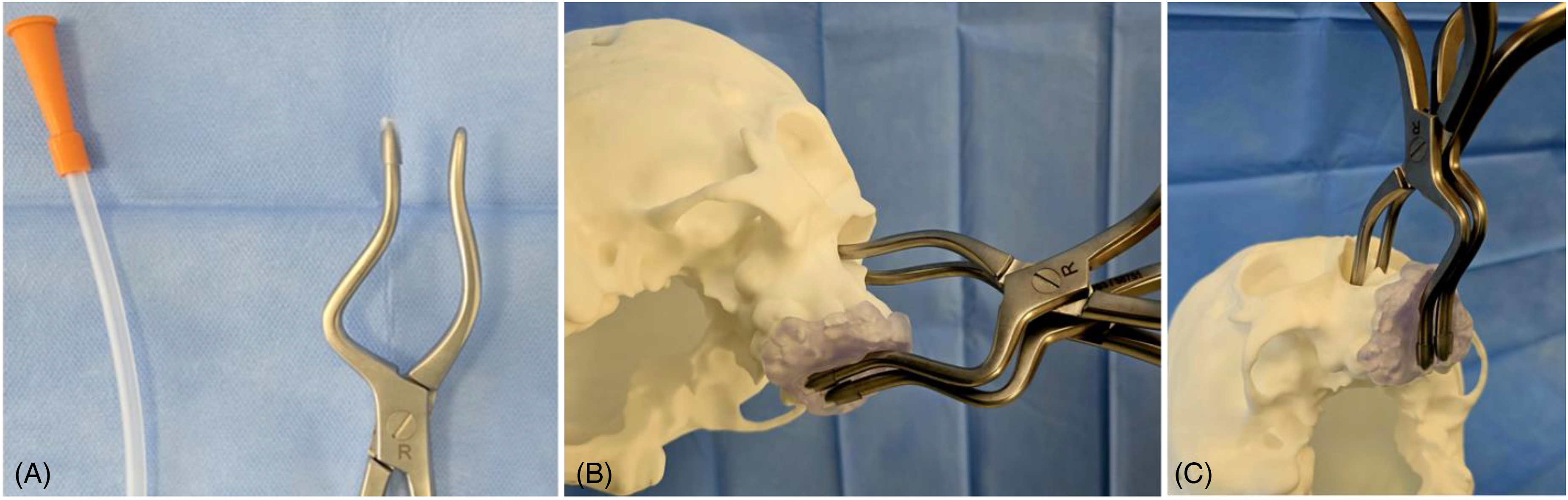
(A) Improvement of holding force by means of suction catheter pieces on the forceps breaks, (B and C) Demonstration of midfacial mobilization with Rowe forceps on an 3D printed anatomical model with the 3D printed plate.
Intraoperatively, the plate was inserted and seated securely through dental engagement. The catheter-sleeved forceps branches were then placed into the guiding grooves, and midface disimpaction was performed in a controlled manner. The plate was removed once mobilization was completed. In all 9 patients treated during both the conventional and digital phases, no palatal perforations or mucosal tears occurred. Surgeons noted that digital plates provided a more consistent fit, greater rigidity, and improved handling. The digital workflow has several advantages. Eliminating impression taking improves patient comfort and avoids airway concerns. Digital models can be stored, modified, or reprinted if needed. The workflow is cost-effective after initial equipment acquisition, and design adjustments can be made quickly. The 3D printed plates were reliable, durable, and anatomically accurate.
There are limitations. Intraoral scanning can remain challenging in very young children or those with limited mouth opening. The rigidity of the final device depends on the resin material, and centres must ensure sterilization compatibility. Virtual design requires basic familiarity with modeling software, although this can be learned with practice. Despite these limitations, the digital workflow combined with the simple catheter-sleeve modification provides a practical and effective method for protecting the palate during Le Fort III procedures in children with syndromic midface hypoplasia. The approach is easy to adopt in craniofacial centres with basic scanning and 3D printing resources and addresses a recognized but often underreported surgical challenge.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.