
Abstract
Objective
To explore patient-reported outcomes using CLEFT-Q at a pilot adult cleft lip and palate (CLP) audit clinic.
Design
Cross-sectional study completed at two Dental Hospitals (Glasgow Dental Hospital and School and Dundee Dental Hospital and Research School) and coinciding with a National Cleft Surgical Service's pilot CLP audit clinic.
Participants
Adults who had primary surgery for orofacial cleft (OFC) performed in National Health Service Greater Glasgow and Clyde Health Board between 1990 and 2005.
Main Outcome Measure
Participants completed the validated CLEFT-Q scored 0–100, with higher scores reflecting better outcomes. Cleft lip (CL) and CLP scores were compared with Mann-Whitney U tests.
Results
The response rate was 33% with 21 participants (14 female, 7 male) and a mean age of 21.9 ± 3.2 years (range 17–31 years). The sample included adults born with unilateral cleft lip (CL; n = 6), cleft palate (CP; n = 2), unilateral cleft lip and palate (UCLP; n = 8), and bilateral cleft lip and palate (BCLP; n = 5). Across cleft types, CLEFT-Q scores ranged from 36.0 ± 23.3 (Lips) to 93.0 ± 22.6 (Speech Distress) for adults with CL; from 28.5 ± 22.4 (Nostrils) to 75.4 ± 21.0 (Speech Distress) for adults with UCLP; and from 31.8 ± 26.5 (Nostrils) to 76.4 ± 18.7 (School) for adults with BCLP. There were no significant differences between adults with CL and those with CLP across the 12 CLEFT-Q scales.
Conclusion
In this limited sample, scales of CLEFT-Q demonstrated a range of outcomes. The results provide baseline data for future research. Further work is needed to address residual concerns for adults with OFC.
Introduction
Orofacial clefting (OFC) is one of the most common congenital conditions worldwide 1 and the most common facial congenital diagnosis. 2 OFC is not evenly distributed universally with incidence rates varying by region and country. 3 The worldwide incidence is approximately one in 700 live births 3 and OFC affects around one in every 650 babies born in the United Kingdom (UK). 3 Worldwide, an estimated 4.6 million individuals are living with an orofacial cleft. 4 Recent global burden analyses indicate that the majority of this burden continues to fall on low and middle income countries. 5
Being born with an OFC can have a significant impact on function and aesthetics with potential speech, hearing, feeding, dental and psychological problems. 6 A key long term follow-up study of individuals with OFC between the ages of 18 and 55 in Denmark born between 1943 and 1987, found increased mortality with higher suicide risk in both males and females, despite OFC surgery having been completed in earlier years.7,8 Results of previous studies of adults with OFC vary from reporting a high degree of acceptability with their facial appearance 9 while others have reported substantial dissatisfaction, both in recent more cohorts 10 and in earlier work where 50%–60% of 68 adults reported being dissatisfied with their facial appearance compared to a control group. 11
Despite substantial progress in surgical techniques and the implementation of coordinated multidisciplinary (MDT) cleft care, evidence indicates that many individuals with OFC continue to experience residual functional, aesthetic, or psychosocial concerns into adulthood. 12 Further investigation is warranted to characterize the specific residual concerns that may persist and to determine the extent of ongoing care needs among adults with OFC.
Aims
This project aims to explore patient-reported outcomes (PROs) using the validated CLEFT-Q at a pilot adult cleft lip and palate (CLP) audit clinic.
Methods
Study Design
The design of this project was a pilot cross-sectional study of adults with OFC who had received surgical for their orofacial cleft in National Health Service (NHS) Greater Glasgow and Clyde (GGC) Health Board between 1990–2005. The timing of this project was planned to coincide with a National Cleft Surgical Service routine audit clinic scheduled to occur in NHS GGC Health Board. This involved pilot adult CLP audit clinics which were set-up to ascertain if and where any residual treatment needs exist in a cohort of people with OFC between the ages of 18 to 33. It allowed those participants who had a presenting complaint to be filtered into the National Cleft Surgical Service, in line with NHS protocol. This project was conducted jointly by two Dental Hospitals and Schools (Glasgow Dental Hospital and School and Dundee Dental Hospital and Research School).
CLEFT-Q
The CLEFT-Q was chosen to be used in this project as it is a rigorously designed PRO measure, which can be used to compare and collect evidence-based outcome data from people with OFC between 8 and 29 years of age on an international level. 13 The CLEFT Q contains 12 independently functioning scales, ranging from 6 to 12 items, with responses of frequency being ‘never, sometimes, often, always’ and endorsement being ‘not at all, a little, quite a bit, very much’) and 1 eating/drinking checklist. CLEFT-Q also includes 1 separate eating/drinking checklist. Raw scores are converted to 0 to 100 with higher scores reflecting better outcomes. The CLEFT-Q scales are made up of three domains: Appearance, Facial Function, and Health-Related Quality of Life. Participants with cleft palate (CP) were excluded from cleft lip scar scale as this scale was not relevant to them.
Participants
Potential participants were all adults who had received surgery for their OFC in NHS GGC Health Board between 1990–2005 and were identified from the board's patient database by the Lead Consultant Cleft Orthodontist. Individuals with syndromes or additional craniofacial anomalies were excluded. All 63 eligible individuals were invited. A Participant Information Sheet and the CLEFT-Q were posted prior to arranging appointments. Of those invited, 40% (n = 25) attended for interview, while 60% (n = 38) did not respond or declined. Overall, 33% participants (n = 21) attended their appointment, provided verbal consent, and completed the CLEFT-Q.
Data Collection
Data were collected using paper copies of CLEFT-Q between June 2022-June 2023. Verbal confirmation was obtained from all participants that they were willing to complete the CLEFT-Q, consent to anonymised data use and project participation, with a research investigator available to address any questions. All were asked to complete the questionnaire themselves without assistance from family/friends or clinicians and were able to. The authors attest that neither ethical approval nor Caldicott approval were required, as the study was conducted as part of the NHS GGC Health Board Routine Cleft Audit Service and did not employ patient-identifiable data.
Data Analyses
Descriptive statistics were used to describe the characteristics of the recorded data set. Due to low numbers of participants with CP (n = 2) it was decided not to include them in Bonferroni-corrected Mann-Whitney U Tests conducted on each of the 12 scores to assess if CLP (unilateral and bilateral CLP combined) differed from CL. CLEFT-Q norms for the age ranges of the participants were included to provide context to interpret this sample. 14 IBM® SPSS® Statistics software platform Version # (IBM, 2023) 15 was used.
Results
Participant Demographics
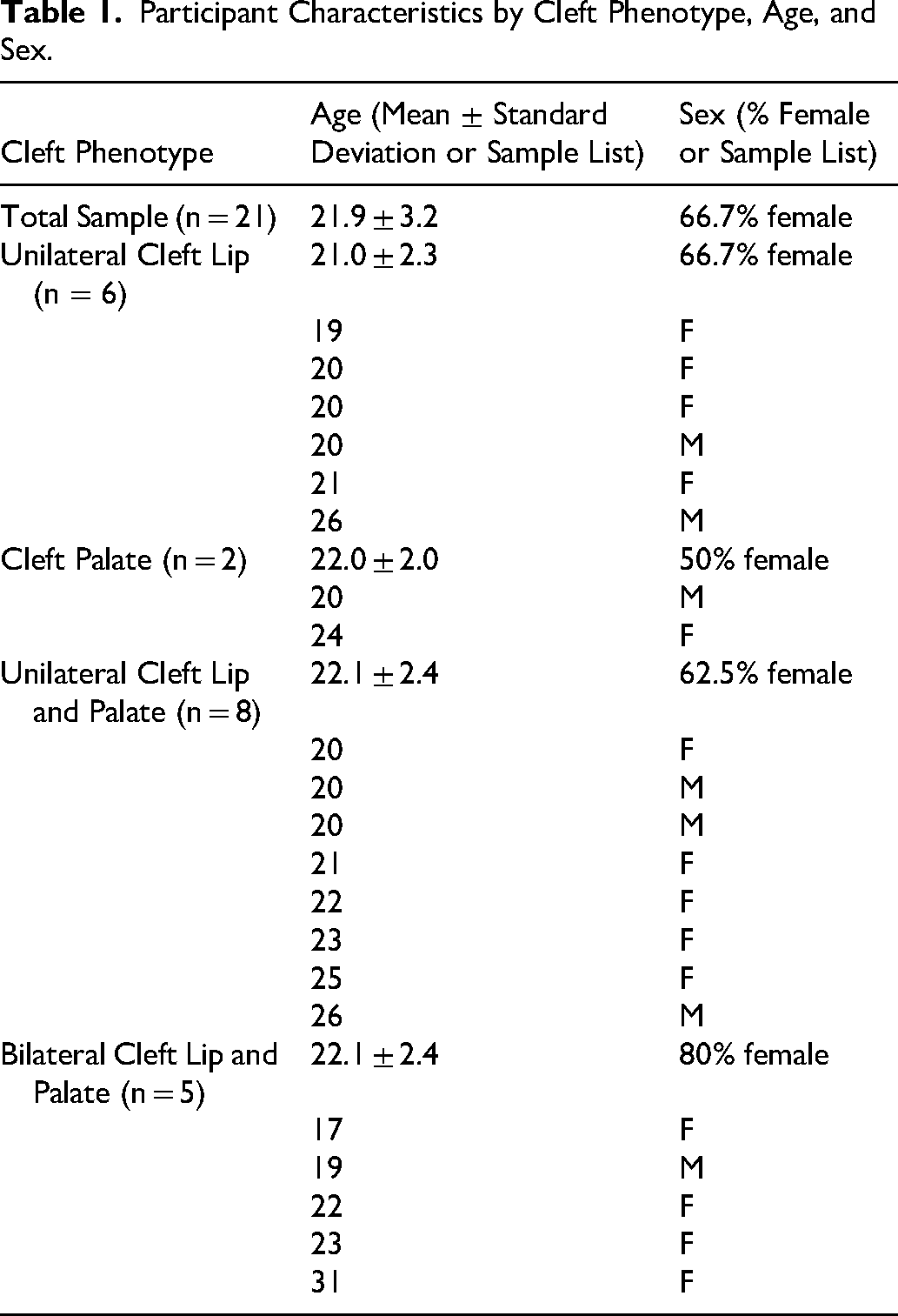
In total 21 participants were recruited to the study, all of whom had English as their first language. As shown in Table 1, 14 (67%) of the participants were female and 7 (33%) were male. The age range of participants was from 17 to 31 years of age, with about half (n = 11) who were younger than 21 and half (n = 10) who were 21 or older. The cleft phenotypes were: CL only (n = 6), CP (n = 2), unilateral CLP (n = 8), and bilateral CLP (n = 5).
Participant Characteristics by Cleft Phenotype, Age, and Sex.
CLEFT-Q Scales
As per the CLEFT-Q User Guide 13 the higher the scores for each of the CLEFT-Q scales, the better the outcome. Please note that the statistical analyses should be treated with caution due to the small sample sizes being compared in this project. A combined summary of CLEFT-Q Scores is in Table 2. The 12 Mann-Whitney U tests for all scales of the CLEFT-Q comparing participants with CL to those with CLP were not significant (p > 0.05).
Summary of CLEFT-Q Scores.
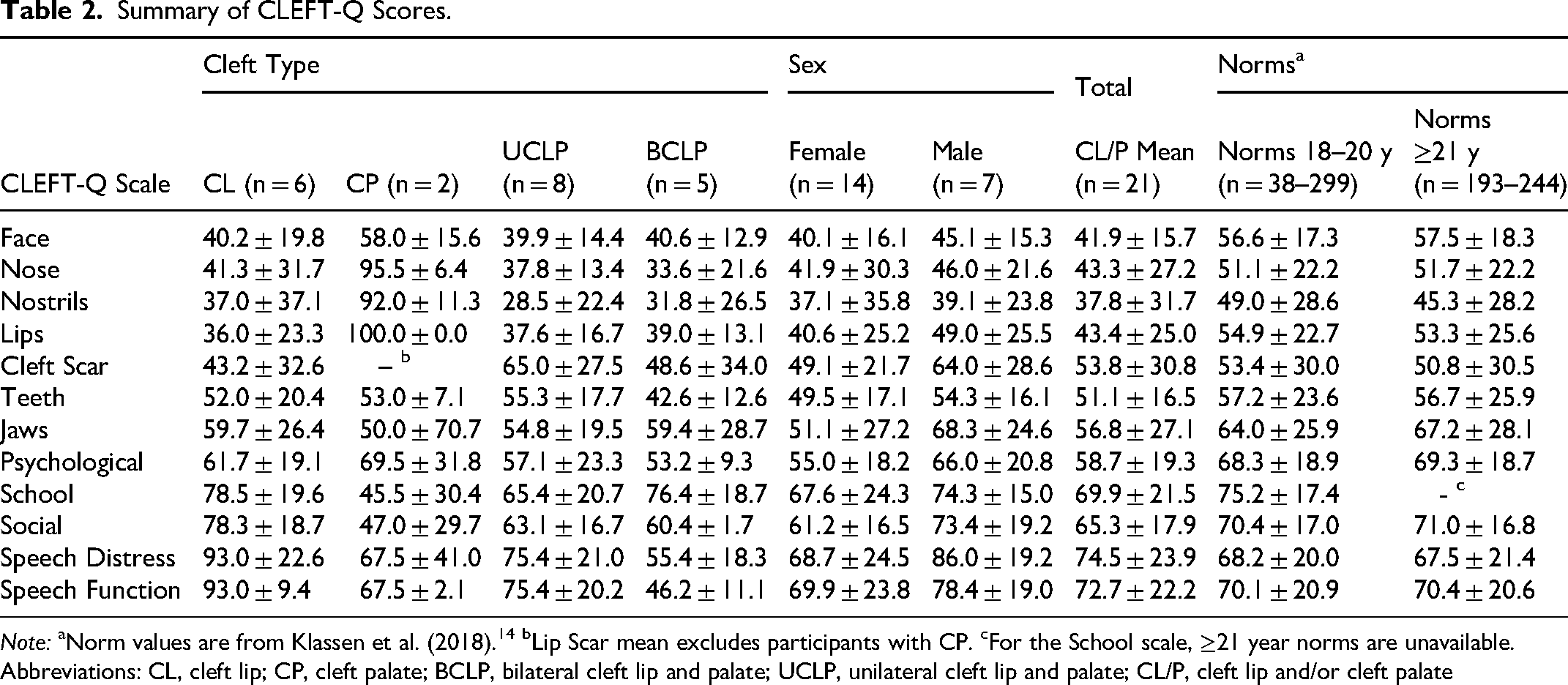
Note: aNorm values are from Klassen et al. (2018). 14 bLip Scar mean excludes participants with CP. cFor the School scale, ≥21 year norms are unavailable.
Abbreviations: CL, cleft lip; CP, cleft palate; BCLP, bilateral cleft lip and palate; UCLP, unilateral cleft lip and palate; CL/P, cleft lip and/or cleft palate
The CLEFT-Q normative values were derived from an international cohort aged 8–29 years, 14 whereas this sample was 17–31 years old in a homogeneous UK population. The single 17-year-old was nearly 18 and one participant (5%) was older than 29. The norms for ages 18–20 and older than 21 are included in Table 2 provide context to interpret this sample's results. Although female participants tended to be lower than males, there was an overall higher representation of females both within the sample and based on prevalence rates of OFC that may reflect a selection bias and should be interpreted with caution.
While within a standard deviation of the norm groups, facial appearance scores were lower than norms by both males and females. Individuals with CL ± P reported the lowest satisfaction, whereas those with CP reported scores in the range of the norms. This pattern was seen for specific facial features measured with the CLEFT-Q. In particular, nasal appearance was a prominent area of concern with the lowest scores among all the scales for participants with CL ± P. Mean scores for nose, nostrils, and lips were lower than norms, although were within a standard deviation of the norm groups. Cleft scar scores for CL ± P participants had a wide range within the norm group standard deviation with higher satisfaction among the unilateral CLP in this sample. In contrast and consistent with typical anatomy of their cleft type, individuals with CP reported high satisfaction with nose, nostrils, and lips. Teeth satisfaction scores were similar to norms, with those with BCLP reporting the lowest scores. Results for jaw satisfaction were similar to the norm values for males and relatively lower than the norm values for female participants, although remained within the norm standard deviation.
All participants were within a standard deviation of the norm group for psychological functioning, with relatively lower scores for adults with CLP. School functioning should be interpreted with caution as it was reported based on recall and within the norm group was also based on a small sample of 38 participants 18–20. Overall school means were similar to norms, with the most concerns reflected in the scores of the two CP participants. Similarly, social function scores were similar to norms for CL, with lower scores within a standard deviation for CLP and the most concerns seen in the two adults with CP. Speech function and speech distress scores followed the pattern of individuals with CL reported the highest satisfaction given typical anatomy, while those with unilateral CLP and CP had similar scores to the norms. BCLP reported the lowest scores that were below the norm groups’ standard deviations.
Discussion
Despite the limited sample size, our findings largely align with previous research and indicate ongoing treatment needs amongst adults with OFC, with perinasal aesthetics identified as a main area of concern. As has been reported, there can be persistent concerns regarding nasal and lip symmetry, lip fullness, and lip movement among adults with OFC.11,16–18 A focused clinical assessment of lip and cleft lip scar outcomes with longitudinal follow-up, examined alongside CLEFT-Q scores, is needed to determine how well objective ratings align with patient-reported satisfaction. This sample's scores were consistent with the high prevalence of severe malocclusion, 19 dental anomalies, and enamel defects 20 in OFC populations and highlight the ongoing importance of orthodontic and restorative treatment in people with OFC.
Psychological Function outcomes in individuals with OFC vary widely, and prior studies have highlighted that although concerns relating to appearance, anxiety, depression, or social acceptance may arise, many do not experience any major difficulties.9,21–24 School satisfaction was varied and aligned with some previous reports in individuals with OFC 12 ; however, these findings need to be interpreted cautiously given participants were recalling past experiences. Social concerns were most noted by the two adults with CP with largely similar scores to norms among CL ± P participants. Previous research indicates that adults with OFC often rely on close family networks and smaller social circles12,25 which may apply to some adults in this participant cohort. Results align with established associations between palatal involvement and speech difficulties, including hypernasality, resonance and articulation difficulties.26,27 Speech was of particular concern for participants with bilateral CLP.
This study also supports the use and inclusion of the CLEFT-Q as a suitable PROM for this population. The results provide a useful baseline for future work; however, further research is needed to better understand and address the remaining challenges faced by adults with OFC, with the aim of improving a better quality of life and ensuring that they get the holistic treatment that their condition demands.
Limitations
This study has several limitations. The sample was small, self-selected, and drawn from a single UK cleft service, limiting generalisability. There may have been a bias toward adults experiencing more concerns who were motivated to attend a pilot adult clinic compared to those who were satisfied with their treatment outcomes. Participants all had English as their first language, and individuals with syndromes or additional craniofacial anomalies were excluded. Attendance and response rates were low (33% of everyone invited completed the Cleft-Q), and CP participants were underrepresented. The ratio of male to female participants did not represent prevalence rates of OFC. The age range (17–31 years) may not fully reflect the experiences of older adults with OFC. The school scale was largely based on recall rather than concurrent experiences, introducing additional bias. There was no data gathered on socioeconomic status of the participants or their families nor their educational attainment or employment status. After initial cleft surgeries identified to meet inclusion criteria, their further medical and surgical history is unknown, which makes it difficult to interpret their outcomes. For example, it could be some participants had not completed available revisions, orthodontics, orthognathic surgery, and speech therapies across their development. However, this project can be considered as a feasibility study.
Implications for Future Research and Work
Larger, multi-centre studies are needed to better characterize adult CLEFT-Q outcomes and identify subgroups at risk of poorer satisfaction. Similar work carried out internationally would allow comparisons across countries and highlight differences in OFC care and outcomes. Close collaboration between MDT cleft teams and psychologists is important to ensure adequate psychological assessment, support, and realistic expectation-setting for patients with OFC so that care is responsive to their specific needs with particular attention to females, who may be at higher risk for later concerns. Larger, longitudinal studies following individuals from adolescence into adulthood would help clarify when these gender differences first emerge and how they develop over time. Further work comparing adults with isolated OFC to those with syndromes or other craniofacial conditions could clarify how these factors independently influence PROs in these cohorts. Incorporating open-ended questions into future studies may also yield deeper qualitative insights, clarifying where residual challenges persist, how they affect individuals, and how they may be best supported.
Clinically, attention should be directed towards where the key issues of dissatisfaction reside. In this small sample, concerns highlighted perinasal aesthetics. At discharge, clinicians could explicitly confirm whether individuals are satisfied with this region or would prefer referral for further discussion and management. Previous studies show similar dissatisfaction amongst adolescents and teenagers, 2 suggesting that earlier identification and intervention may help individuals achieve greater long-term satisfaction with these aesthetic outcomes.
Footnotes
Acknowledgments
Sincere thanks to Dr. Toby Gillgrass, Dr. Rebecca Crawford, Mr. Gavin Revie, Mr. Scott McGregor, and all of the administrative staff of the National Cleft Surgical Service for Scotland, without whom this project would not have been possible. Please note that Tables 12,3 were generated with the use of AI and modified as necessary by Jill Anne O’Driscoll.
Ethical Statement
The Ethics Committee of NHS Tayside and NHS Greater Glasgow and Clyde (GGC) waived the need for ethics approval and patient consent for the collection, analysis, and publication of anonymized data for this non-interventional study. Neither ethical approval nor Caldicott approval were required, as the study was conducted as part of the Routine Cleft Care Scotland Audit Service scheduled to occur in NHS GGC and did not employ patient-identifiable data.
Informed Consent
As this project was run as part of the GGC Routine Cleft Audit Service, written consent was not needed prior to data collection as consent had been obtained at birth. However, it was confirmed verbally with the participants and/or their parents/carers that they were willing to partake in the project, to complete the CLEFT-Q, and to have their data anonymized and analyzed. As this study used fully anonymized data collected as part of the Routine Cleft Care Scotland Audit Service, individual informed consent was not required.
Author Contributions
Jill O’Driscoll: Conceptualization (lead); Methodology (lead); Writing – original draft (lead); Formal analysis (lead); Writing – review and editing. Grant McIntyre: Conceptualization (supporting); Methodology (supporting); Supervision; Writing – review and editing. Peter Mossey: Conceptualization (supporting); Methodology (supporting); Supervision; Writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. All data were anonymized prior to analysis. Due to ethical and patient confidentiality considerations, the data are not publicly available.
Anonymized Locations/Services
Dental Hospital and School A: Glasgow Dental Hospital and School
Dental Hospital and School A: Dundee Dental Hospital and School
National Health Service (NHS) Health board XXX: NHS Greater Glasgow and Clyde
National Cleft Surgical Service: Cleft Care Scotland
Other Identifying Information
Not applicable