
Abstract
Objective
To refine and adapt an existing surgeon's-view camera technique for application in intraoral and deep craniofacial surgical fields, providing a lightweight, low-cost, and educationally valuable visualization method.
Design
A technical innovation study evaluating a customized mounting and imaging system for surgeon's-view video recording in craniofacial surgery.
Patients/Participants
Representative craniofacial cases were recorded, including palatoplasty and pharyngeal flap surgery.
Interventions
A USB camera (IMX179 sensor, M12 mount) was mounted directly onto surgical loupes or a head-mount using a custom 3D-printed housing. The system incorporated an aperture-narrowing disc to increase the depth of field and utilized a smartphone as the recording and power source.
Results
The system successfully recorded clear, stable, surgeon-aligned videos of deep surgical fields without additional recording equipment. The aperture modification improved focus stability, though image brightness and sharpness were reduced. Lens interchangeability and smartphone mirroring enabled flexible field-of-view adjustment and real-time sharing with surgical staff.
Conclusions
This refined surgeon's-view camera system is a practical, adaptable, and affordable solution for recording deep craniofacial procedures. Despite minor image trade-offs, it enhances surgical education and may broaden accessibility to high-quality operative video recording.
Keywords
Introduction
Recording and sharing surgical experiences has long been an integral part of surgical education and skill dissemination. Video documentation not only enables trainees to observe complex procedures repeatedly but also facilitates peer review and academic presentation. Over the past decade, the evolution of compact action cameras has revolutionized surgical video recording. 1 Their small size, lightweight design, and wide-angle field of view have made them convenient tools for capturing operations, leading to numerous reports across various surgical specialties utilizing these devices for educational purposes.
However, craniofacial surgery—particularly intraoral procedures or surgeries performed in deep, narrow fields—poses unique challenges for video recording. These surgical fields are often dark, confined, and obstructed by instruments, making it difficult for conventional action cameras to provide clear and meaningful visualization. While alternative visualization systems exist, such as microscope-integrated recorders, laparoscopic or endoscopic cameras, and professional surgical recording systems integrated into commercial loupes, they have notable limitations.2,3 These include high costs, a steep learning curve, limited flexibility, and potential interference with the surgical workflow.
In 2022, Park et al introduced a novel approach using a miniature M12 mount USB camera, which is exceptionally lightweight, affordable, and flexible in software utilization through smartphone integration. 4 This approach demonstrated the feasibility of capturing the surgeon's point of view without additional staff or significant disruption to the operative field.
Building on this concept, we present the application of an M12 mount surgeon's-view camera specifically for intraoral and deep-field craniofacial procedures. This technique enables precise visualization of narrow operative corridors, overcomes many limitations of conventional systems, and provides highly practical and educational video material for craniofacial surgeons and trainees.
Methods
This study was conducted following the principles of the Declaration of Helsinki, and written informed consent for surgical recording and use of images for research and publication was obtained from all patients. The surgical video recording technique was adapted and refined from the method reported by Park et al, with several modifications to improve visualization in intraoral and deep surgical fields. 4 The device and cabling were managed in a manner similar to conventional wired headlight systems, with appropriate sterile draping and routing to avoid interference with the operative field.
Camera and Recording Setup
A M12 mount USB camera module equipped with a Sony IMX179 CMOS sensor was used for video capture (AliExpress, Shenzhen, China) (https://a.aliexpress.com/_oDqqRvf). The camera was connected via USB to a smartphone (Samsung Galaxy S22, Samsung Electronics, Suwon, Korea), which served as both the power supply and recording device. The recording application (USB Camera, Google Play Store, Google LLC, USA) was used to capture and store videos. The recording resolution was set to 1600 × 1200 pixels at a frame rate of 30 frames per second.
Optics and Illumination
Interchangeable M12 lenses with focal lengths of 25 mm were used to adjust the field-of-view according to the surgical depth and working distance (Figure 1A). Illumination was provided by a SurgiTel HighIntensity headlight (SurgiTel, Ann Arbor, MI, USA), which ensured sufficient lighting in narrow intraoral and deep surgical fields. The light was set to maximum brightness, corresponding to approximately 80 000 lux according to the manufacturer's specifications.

Optical components and mounting configurations of the low-cost surgeon’s-view camera system. (A) Optical components, including an interchangeable M12-mount lens (25 mm focal length), a custom 3D-printed aperture-narrowing disc placed at the posterior outlet of the lens to increase the F-number and depth of field, and the compact USB camera module. (B) Direct loupe-mounted configuration using a custom 3D-printed housing that integrates the camera and headlight, aligned with the surgeon's visual axis. (C) Head-mounted configuration designed for surgeons who do not routinely use loupes, with the camera and light source integrated into a custom 3D-printed mount. (D) Examples of interchangeable M12-mount lenses with different focal lengths used to adjust the field-of-view according to surgical depth and working distance.
Mounting and Customization
The camera system was developed with 2 mounting configurations to accommodate different surgical preferences. The first was a direct-mount system in which the USB camera was attached to the surgical loupes and carefully aligned with the surgeon's visual axis (Figure 1B). The second was a head-mount configuration designed for surgeons who do not routinely use loupes, allowing the camera to be positioned securely while maintaining a surgeon's-eye perspective (Figure 1C). In both configurations, a custom 3D-printed housing integrated the camera, the light source, and the mounting structure into a single unit. This design provided stable fixation for prolonged procedures and coaxial alignment of the optical axis with the operative field. These features helped maintain a consistent view of the surgical field and minimized parallax throughout the operation.
Improving Focus Stability in Deep Fields With Aperture Modification
To further enhance the depth of field in deep and narrow surgical spaces, an aperture-narrowing disc was 3D-printed and placed at the posterior outlet of the lens (Figure 1A). Reducing the aperture size increases the effective F-number, thereby enhancing the depth of field and allowing structures at varying distances to remain in focus simultaneously. The disc was fabricated using a polycaprolactone filament. Its thickness was 0.8 mm, and the aperture diameter was set at 1 mm, corresponding to the smallest reproducible orifice achievable with the printer. The overall disc diameter was determined according to the inner diameter of the lens's posterior outlet to ensure stable fitting. This modification effectively increased the F-number, resulting in a greater depth of focus and more stable image capture during procedures. While this adjustment slightly reduced image brightness and sharpness, it provided a significant improvement in focus stability, which was particularly beneficial for intraoral and deep craniofacial procedures.
Real-Time Video Transmission Setup
The recorded surgical field was transmitted in real time to a tablet PC (Samsung Galaxy Tab S10 Ultra, Samsung Electronics) using the mirroring application (Samsung Flow, Samsung Electronics). The tablet output was then relayed through a wireless HDMI transmitter (Anytrox Wireless HDMI transmitter/receiver set, Top High Technology, Shenzhen, China) to an external monitor for simultaneous display.
Cases
This setup was used to record representative intraoral procedures, palatoplasty, and pharyngeal flap surgery. Each recording session successfully captured the deep and narrow operative fields without the need for additional staff or specialized equipment such as a surgical microscope or endoscope.
Pharyngeal Flap
Pharyngeal flap surgery involves one of the deepest operative fields in craniofacial surgery, characterized by a vertical and narrow intraoral corridor that is difficult to capture and share the surgical field.
In this study, the system was applied during pharyngeal flap surgery for velopharyngeal insufficiency, where the limited access and frequent instrument movement often obscure the view. The recording maintained a stable view across the entire surgical depth, enabling clear visualization of flap elevation, inset, and posterior pharyngeal wall suturing, with minimal obstruction by instruments. This provided a true surgeon's-eye perspective that is highly valuable for trainee education and sharing the visual field for the other medical staff (Figure 2; Supplemental Video 1).
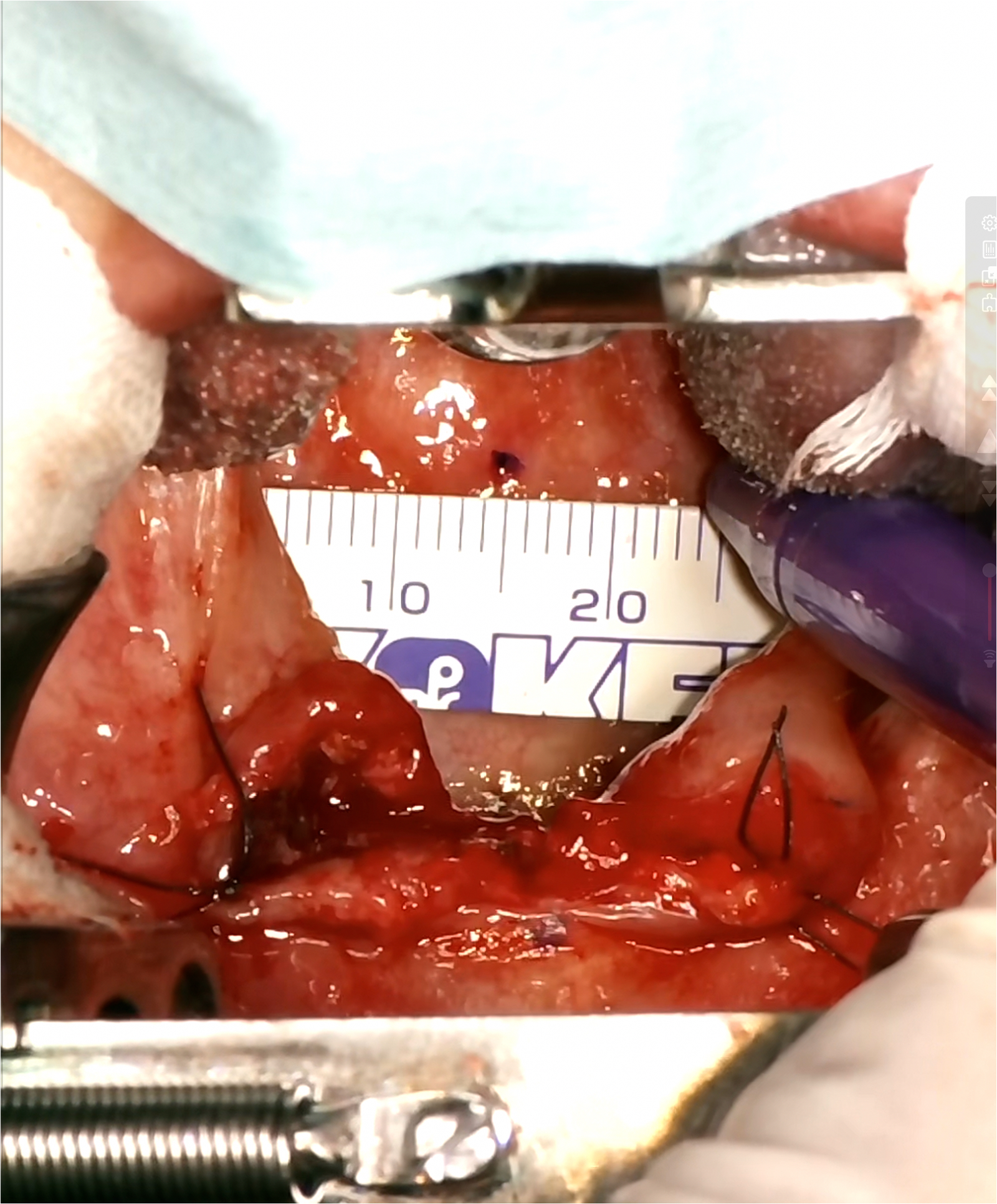
Intraoperative view during pharyngeal flap surgery captured by the surgeon-mounted camera system. The image shows the design stage of the pharyngeal flap, with the ruler and skin marker in place. The soft palate is divided along the midline, and the posterior pharyngeal wall is clearly visualized. Supplemental Video 1 demonstrates the sequence of flap design, local anesthesia administration, and flap elevation, recorded while the operator was wearing the system.
Palatoplasty
Palatoplasty is among the most common intraoral procedures in craniofacial surgery, yet its deep and confined operative field limits direct observation to the primary surgeon and a single assistant. Other medical staff, including the anesthesiologist, scrub nurse, and trainees, typically cannot visualize the surgical site due to its restricted access and narrow line of sight. The application of this recording system enabled clear visualization of the intraoral field from the surgeon's perspective, allowing real-time sharing of the operative view with the entire operating team. This setup facilitated active communication and intraoperative discussion between the surgeon, trainees, and medical staff, providing both educational value and improved team situational awareness (Figure 3; Supplemental Video 2).
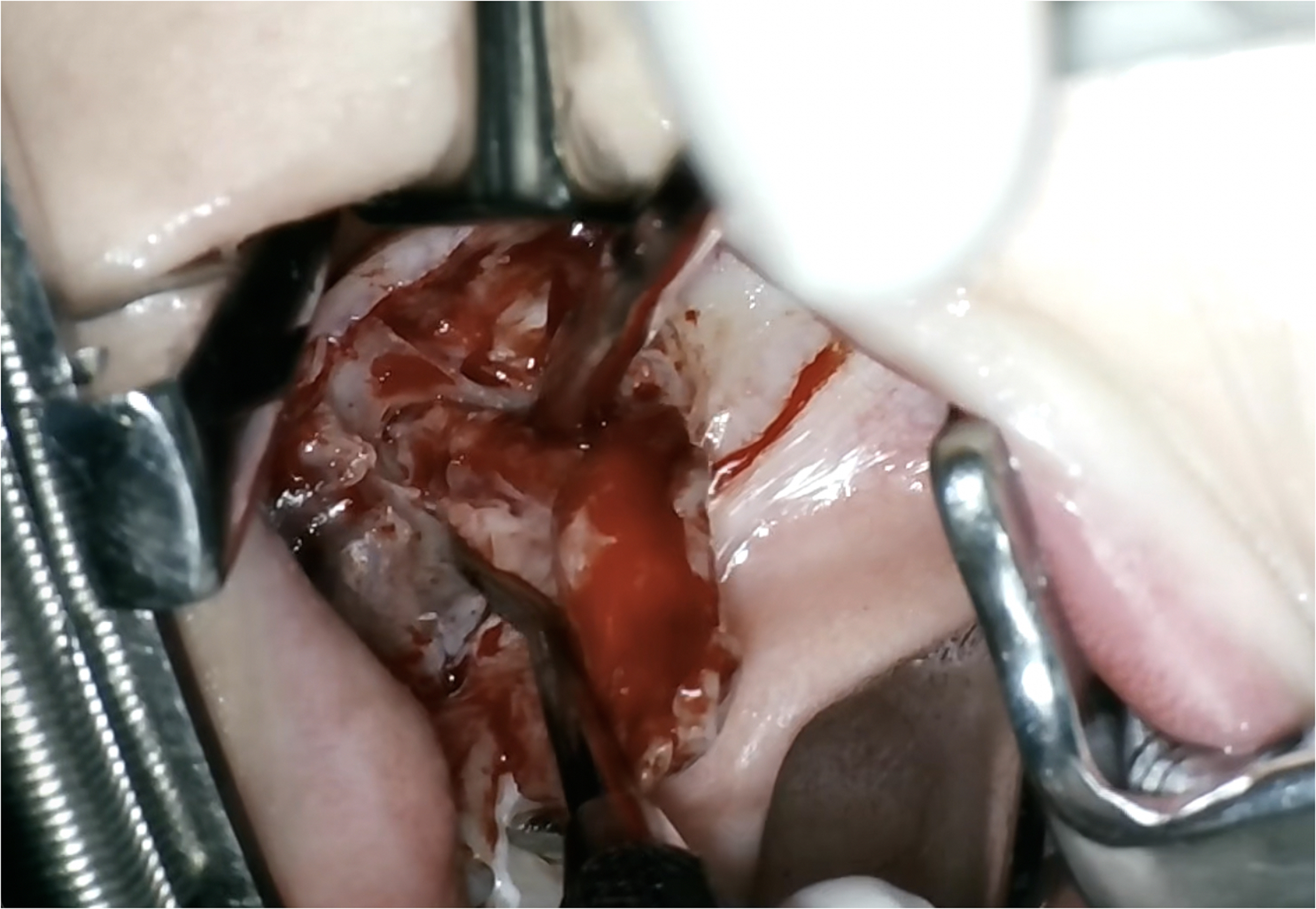
Intraoperative view during palatoplasty captured by the surgeon-mounted camera system. The neurovascular bundle and the posterior end of the right hard palate are clearly visualized. Supplemental Video 2 demonstrates the dissection process, including detachment of abnormally inserted palatal muscles from the posterior hard palate, isolation of the neurovascular bundle, and muscle dissection from the hamulus—steps that are typically difficult to observe directly.
Discussion
Recording surgical procedures from the surgeon's point of view has become increasingly valuable for education, skill assessment, and documentation. Various visualization systems have been used for this purpose, each with distinct advantages and limitations. Endoscopic systems provide excellent illumination and image clarity in narrow or deep operative fields; however, they require specialized equipment, are costly, and can interfere with the surgical workflow, as instruments may collide with or obstruct the endoscope during complex procedures. 3 Operating microscopes also deliver superior image quality, but they are not routinely used in craniofacial or intraoral surgery. 2 Using them solely for recording is impractical, as the microscopic field-of-view is unfamiliar to most surgeons in this field and does not reflect the natural operative perspective.
Head- or chest-mounted action cameras are widely adopted because of their affordable price and ease of use, allowing surgeons to record procedures without a complex setup. 1 However, these cameras typically provide a wide field-of-view, which is not ideal for deep and narrow operative fields such as those encountered in oral and craniofacial surgery. Capturing specific and detailed views of the target anatomy is challenging, and cropping to narrow the field often leads to loss of resolution and image clarity. Some surgeons attempt to customize action cameras with modified lenses or mounts to achieve a narrower field-of-view, but such systems become heavier and require technical expertise to operate, limiting their practicality in daily clinical use. 5
Several professional surgical recording systems have been developed specifically for operative video capture and can be mounted on loupes or surgical headlights to provide a stable, centered field-of-view. While these systems are capable of high-quality imaging, they are often bulky and rigid, making it difficult to flexibly align the camera to the surgeon's exact visual axis during dynamic craniofacial procedures. In addition, they are extremely expensive, with costs that are prohibitive for routine educational use or daily clinical practice. 6 As a result, despite their technical capabilities, such systems are not widely adopted for intraoral or deep craniofacial surgery, where cost-effectiveness and flexibility are critical.
The customized surgeon's-view USB camera system developed in this study provides a lightweight and compact solution that can be precisely aligned with the surgeon's visual axis, producing a true surgeon's-eye perspective. Its low cost makes it practical for routine recording and educational use, in contrast to professional surgical recording systems that are bulky and prohibitively expensive.
This M12-mount and smartphone-hosted system offers unique flexibility. The lens is fully interchangeable, and a variety of focal length lenses typically around 1 to several dollars each with low price allow the surgeon to select the optimal field-of-view for each procedure, from narrow deep intraoral fields to wider orbital or facial exposures (Figure 1D). The custom 3D-printed housing ensures stable optical alignment, and the aperture-narrowing disc increases depth of field and focus stability, which is particularly useful for deep and narrow craniofacial procedures.
Modern smartphones further enhance the system's utility. In this study, the screen-mirroring function enabled the live operative view to be shared not only with trainees but also with scrub nurses and anesthesiologists, improving team situational awareness and intraoperative communication. These combined features may provide educational and clinical benefits that surpass what most commercial recording platforms can offer, while maintaining simplicity, flexibility, and cost-effectiveness.
Several practical considerations related to ergonomics and workflow should be acknowledged. The system requires a brief setup prior to hand sterilization to initiate recording and wireless mirroring; however, once established, it did not interfere with intraoperative workflow. The addition of the camera system increases the weight of the loupe or head-mounted setup by several grams, which may contribute to surgeon fatigue, particularly during prolonged procedures. In the present study, the system was primarily applied to relatively short operations, such as palatoplasty and pharyngeal flap procedures (typically less than 2 h), and no substantial increase in operative time or fatigue was observed.
The presence of the device within the peripheral, nonloupe visual field may introduce potential distraction. Nevertheless, sufficient visual space remained between the loupe lenses and the mounted device, allowing rapid adaptation during surgery. These ergonomic effects may vary depending on individual surgeon preference and should be considered when adopting the system.
A more precise evaluation of operative time and surgeon fatigue, particularly in prolonged procedures, is warranted in future studies. The system may increase fatigue due to the added weight and partial occupation of the peripheral visual field; however, it may also improve workflow efficiency by enabling real-time sharing of the surgical field with the operative team. The overall impact of these opposing factors remains unclear and requires systematic investigation.
Despite its benefits, this system has notable limitations related to the aperture-adjustment disc. To achieve a greater depth of field, the disc was designed with an extremely narrow aperture, which reduces image quality. Because this modification is not part of the original camera design, it is inevitably compromised compared to standard lens use. This trade-off represents the primary drawback of the system, but it remains acceptable in routine practice given the system's overall flexibility and educational utility.
Looking forward, this system holds promise for expanded applications in craniofacial surgical education and related fields. Integration with live streaming could enable real-time remote teaching, while the addition of stereoscopic or 3D recording may enhance spatial understanding of deep operative fields. The use of cameras integrated in smartphones with optical and digital zoom modules could further improve adaptability by allowing intraoperative transitions between wide and narrow fields of view. Another limitation involves the camera being directly attached to the surgeon, meaning minor body movements or oscillations may affect recording stability—especially when using tele-zoom lenses. As demonstrated in Supplemental Videos 1 and 2, overall image stability was acceptable under routine conditions; however, minor improvements may be achieved with the addition of digital image stabilization. This issue could be further mitigated through mechanical stabilization or software-based image stabilization integrated into the smartphone or camera sensor system.
Finally, this study was designed as a technical note focusing on system development and feasibility rather than comprehensive validation. Accordingly, objective evaluation, including quantitative imaging metrics, direct comparison with existing recording systems, and structured assessment of educational impact, was not performed. These elements represent important next steps and will be addressed in future studies to further establish the clinical and educational utility of this system.
Conclusion
We refined an existing surgeon's-view camera technique and adapted it for intraoral and deep craniofacial surgery. This lightweight, low-cost, and flexible system provides a true surgeon's-eye perspective suitable for routine educational and clinical use. While the aperture-adjustment disc reduces image quality, this trade-off is acceptable, and the system has the potential to enhance craniofacial surgical training and documentation.
Supplemental Material
Supplemental Material
Footnotes
Consent to Participate
The authors confirm that written informed consent was obtained from all patients for the publication of their photographs, videos, and research data.
Author Contributions
DS: conceptualization, methodology, investigation, writing—original draft, and writing—review and editing.
HI: methodology and validation.
AK: data curation and formal analysis.
TM: investigation and resources.
YS: software and visualization.
EF: validation and supervision.
IT: project administration and resources.
AW: supervision, funding acquisition, and writing—review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The longer shots of the surgical video are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.