
Abstract
Background
Rare craniofacial clefts are among the most complex anomalies encountered in reconstructive surgery. Although isolated Tessier clefts are well described, patients with multiple independent craniofacial cleft axes remain exceptionally rare, and their anatomical patterns, staged reconstructive burden, and early functional outcomes remain incompletely characterized.
Patients and Methods
A retrospective review was conducted of patients with combined craniofacial clefts treated at a tertiary craniofacial center between 2015 and 2024. Combined clefts were defined as 2 or more independent craniofacial cleft axes according to the Tessier classification.
Results
Thirteen patients met inclusion criteria. Ten (77%) underwent staged reconstruction at our institution, with a mean of 3.1 operative stages per treated patient. Orbital involvement was present in nine patients and palatal clefts in 6. Skeletal reconstruction was required in three patients. Early functional outcomes were generally acceptable during follow-up, although residual deformities and speech-related sequelae persisted in some referred revision cases. Minor wound infection occurred in three patients, and hypertrophic or widened scarring in 4.
Conclusions
Combined multi-axis craniofacial clefts represent a rare and surgically demanding subset of congenital anomalies requiring function-prioritized staged reconstruction and continued multidisciplinary follow-up throughout growth.
Keywords
Introduction
Rare craniofacial clefts are among the most complex congenital facial anomalies encountered in reconstructive surgery. Although cleft lip and palate are relatively common, atypical facial clefts are considerably less frequent and show marked anatomical variability. The classification proposed by Tessier in 1976 remains the standard framework for describing these deformities, defining 15 craniofacial cleft lines (0–14) according to their relationship to the orbit and allowing correlation of the associated soft-tissue and skeletal defects. 1
The reported incidence of rare craniofacial clefts ranges from approximately 1.4 to 4.8 per 100,000 live births, placing them among the least common congenital craniofacial anomalies seen in clinical practice.2,3 Within this already uncommon group, patients with multiple independent craniofacial cleft axes remain particularly poorly defined in the literature.4,5 Compared with isolated Tessier clefts, combined multi-axis deformities involve simultaneous disruption of multiple facial units and therefore present reconstructive challenges beyond those of a single-axis defect. Published evidence remains largely limited to isolated case reports and small institutional series, including combinations such as Tessier clefts 3 and 4 and associations involving clefts 3, 7, and 11.6,7
Management remains challenging because of marked anatomical variability and the lack of standardized treatment pathways.8,9 Reconstruction typically requires staged soft-tissue and skeletal correction throughout growth, with priority given to ocular protection, oral competence, feeding, speech, and dental occlusion. 2 Current literature provides limited guidance on the anatomical spectrum, operative burden, early functional outcomes, and the impact of prior intervention in combined multi-axis craniofacial clefts. In particular, it remains unclear how multiple independent cleft axes and previous surgery affect operative sequencing, reconstructive burden, and early functional recovery in the context of the existing literature on single-axis Tessier clefts. This study therefore examines the anatomical patterns, staged surgical management, and early functional outcomes of combined craniofacial clefts treated at a tertiary craniofacial center, with particular attention to revision complexity and the reconstructive principles that guide function-prioritized management during growth.
Patients and Methods
Study Design
A retrospective review was conducted of patients with combined craniofacial clefts treated at a tertiary craniofacial referral center between January 2015 and December 2024. Institutional review board approval for retrospective clinical analysis was obtained from the local Medical Research Ethics Committee before data collection.
Combined craniofacial clefts were defined as the presence of 2 or more independent Tessier cleft axes. Craniofacial extensions along a single developmental axis, such as Tessier 0–14 or 2–12, were considered components of the same cleft field unless accompanied by an additional independent axis. Bilateral symmetrical clefts were similarly excluded as bilateral variants of a single cleft pattern rather than true multi-axis deformities. Patients with recognized syndromic craniofacial anomalies, including Treacher Collins syndrome, were excluded because these conditions follow well-defined and extensively studied syndrome-specific craniofacial patterns that fall outside the scope of the present analysis.
Data Collection
Clinical records and photographic documentation were reviewed. Collected data included demographics, age at presentation, referral status, cleft pattern, orbital and palatal involvement, procedures performed, postoperative complications, and functional outcomes, including feeding, speech, and dental development.
In patients aged 2 years or more at follow-up, speech assessment was performed by the cleft speech-language pathologist within the multidisciplinary team using a structured CAPS-A–based perceptual protocol, including evaluation of resonance, hypernasality, nasal emission, articulation, intelligibility, and cleft speech characteristics where present. For descriptive subgroup reporting, perceptual findings at latest functional assessment were translated into a simple internal ordinal severity scale (0 = normal/absent, 1 = mild, 2 = moderate, 3 = marked, 4 = severe/profound). This scale was used for descriptive reporting only and was not intended for comparative statistical or inter-study analysis. Patients with suspected velopharyngeal insufficiency underwent instrumental assessment using nasoendoscopy and/or lateral videofluoroscopy according to multidisciplinary cleft-team protocol. Interpretation of speech and velopharyngeal findings was individualized because palatal morphology within this cohort was heterogeneous and included atypical transverse and oblique cleft extensions associated with multi-axis craniofacial clefts. Clinical status at the latest follow-up was summarized based on age-appropriate developmental milestones, perceptual speech findings, and instrumental assessment where indicated. Assessments were performed as part of routine clinical care and were not blinded.
Surgical Management
Nine patients presented primarily to our center, six of whom underwent operative reconstruction. In this group, age at first surgery ranged from 8 months to 6 years (mean, 14 months). Among the four referred patients, the age at first surgery at our institution ranged from 4 to 9 years (mean, 6.5 years).
All 10 surgically treated patients underwent staged reconstruction, with a total of 31 operative stages (mean, 3.1 per patient).
Skeletal reconstruction was undertaken on a functional rather than chronological basis when bony deficiency compromised globe support, ocular protection, occlusal development, facial symmetry, or tension-free soft-tissue closure.
Soft-tissue reconstruction consisted of staged restoration of the involved craniofacial units, including eyelid continuity, lip and commissural reconstruction when indicated, cleft palate repair where appropriate, and correction of associated deformities. In patients with orbital involvement, early procedures prioritized eyelid continuity and ocular protection, with simultaneous correction of associated soft-tissue deformities when feasible.
Follow-Up
The duration of institutional follow-up ranged from 1 to 9 years (mean, 4.1 years), measured from initial presentation to our center to latest assessment. Functional outcomes were assessed at a mean patient age of 4.8 years.
Results
Patient Characteristics
Thirteen patients with combined craniofacial clefts met the inclusion criteria, including eight males and five females (Table 1). Age at presentation ranged from 1 day to 9 years. Nine patients presented primarily to our institution, whereas four were referred after undergoing 2–4 prior procedures elsewhere. Of the nine primary-presenting patients, six underwent staged reconstruction, and all four referred patients required revision surgery. Nonoperative management was selected in three patients without significant functional impairment or evidence of progressive deformity, with continued longitudinal follow-up during growth. Overall, ten patients underwent 31 operative stages at our center (mean, 3.1 per patient).
Individual Patient Characteristics and Management.
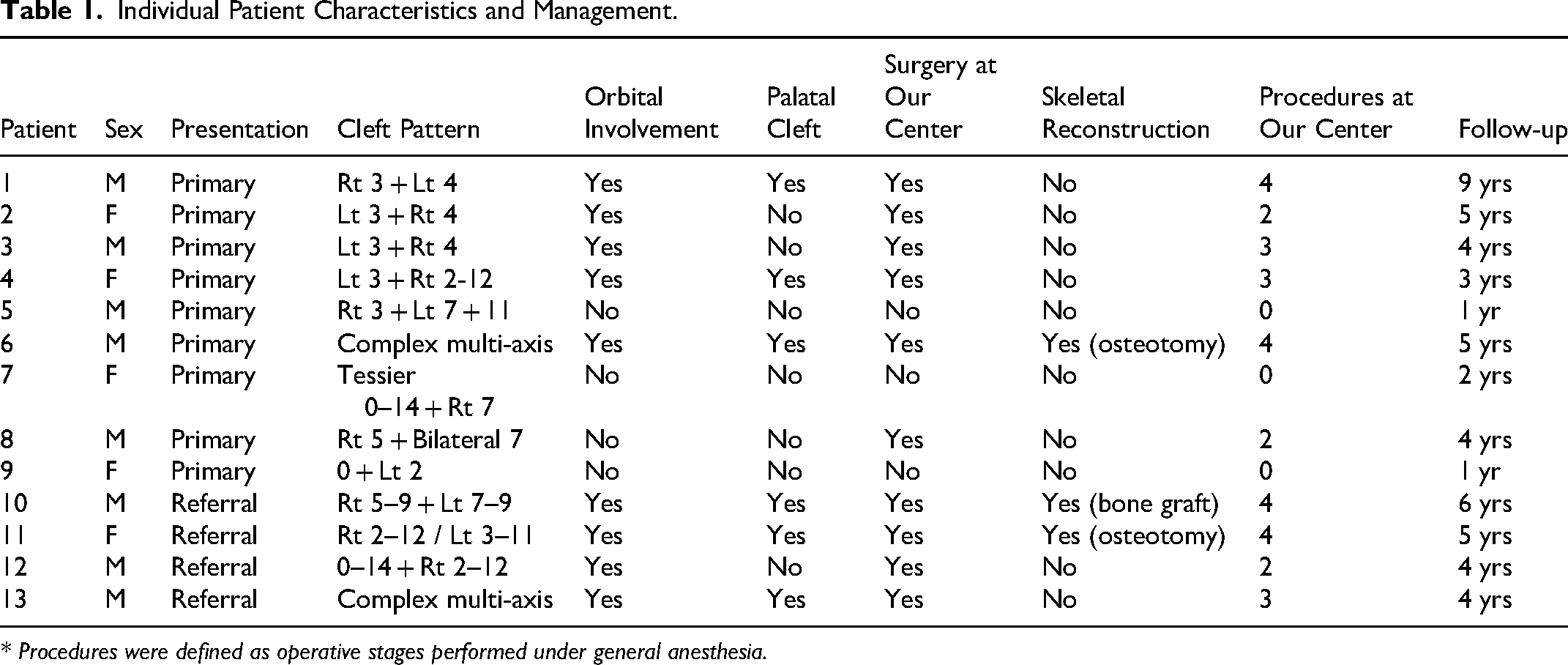
* Procedures were defined as operative stages performed under general anesthesia.
Anatomical Patterns
A broad spectrum of combined craniofacial cleft configurations was observed (Table 1; Supplementary Table 1). The most frequent pattern was Tessier clefts 3 and 4, identified in three patients. The remaining cases comprised less common multi-axis configurations, including one 3–7–11 cleft, one 3 plus 2–12 cleft, and two complex deformities not fully classifiable within the conventional Tessier system.
Orbital involvement was present in nine patients and included eyelid coloboma (n = 7), orbital floor defects (n = 4), and orbital dystopia (n = 4), with overlap among findings. Severe ocular abnormalities were identified in four patients, including anophthalmia or microphthalmia in two, extensive orbital wall deficiency with associated zygomatic-maxillary hypoplasia in one (Figure 2), and exposure-related corneal opacity in two (Supplementary Tables 2 and 3).
Palatal Involvement
Palatal clefts were present in six patients. One patient (Figure 1) demonstrated an additional transverse palatal extension aligned with the facial cleft axis. Five patients underwent palatal repair during the study period. In this patient, the conventional cleft palate was repaired, whereas the transverse component remained unrepaired. One additional patient had a very large unrepaired palatal cleft at latest follow-up.

Representative patient with combined craniofacial clefts involving the right Tessier 5–9 axis and left Tessier 7–9 axis with associated orbital deformity. (A) Preoperative frontal view demonstrating complex craniofacial clefts with periorbital soft-tissue deficiency and corneal opacity secondary to ocular exposure. (B, C) Right and left lateral views demonstrating the extent of the facial clefts and associated midfacial asymmetry. (D, E) Frontal and left lateral three-dimensional computed tomography reconstructions demonstrating the underlying cranial, orbital, and maxillofacial skeletal deformities. (F) Intraoral view demonstrating a transverse palatal cleft aligned with the facial cleft axis and a repaired right cleft palate. (G) Postoperative frontal view after staged reconstruction, including release of fibrous tethering and eyelid reconstruction with local flaps to restore eyelid continuity and reduce ocular exposure.
Major Reconstructive Procedures
Six primary-presenting patients underwent staged reconstruction of their craniofacial clefts, with a mean age at first surgery of 14 months (range, 8 months to 6 years). Among the four referred patients, the age at first surgery at our institution ranged from 4 to 9 years (mean, 6.5 years). Skeletal reconstruction was required in three patients. In one patient, a segmental maxillary osteotomy was performed during mixed dentition to align the displaced lesser maxillary segment and close a residual alveolar bony gap. In another patient, the abnormally cranially attached right alveolar segment was osteotomized and medially translocated while preserving the internal mucosal-soft tissue attachment to restore alveolar arch continuity and facilitate facial cleft closure (Figure 2). One additional patient underwent calvarial bone graft reconstruction of the orbital floor to improve globe support in the setting of progressive globe descent.

Representative 5-year-old boy with complex multi-axis craniofacial clefts and associated craniofacial skeletal deformity treated with staged reconstruction. (A) Preoperative frontal view demonstrating severe facial cleft deformity with marked orbital and midfacial deficiency. (B) Immediate postoperative appearance following first-stage reconstruction, including osteotomy and medial translocation of the cranially displaced right alveolar segment to restore alveolar continuity and facilitate facial cleft closure. (C) Follow-up 1 year after the first reconstructive stage, before second stage revision surgery. (D) Immediate postoperative appearance following second-stage revision for further refinement of the facial cleft reconstruction and improvement of oral competence using preserved trimmed lip tissue as a temporary right alar substitute, with definitive nasal reconstruction deferred until later growth. (E) 18 months follow-up after second surgery demonstrating maintained soft-tissue coverage and preserved prepubertal facial contour during growth. (F) Preoperative intraoral view demonstrating severe displacement of the alveolar segments and marked disruption of maxillary arch continuity. (G) Postoperative view demonstrating restoration of alveolar continuity following segmental osteotomy and medial translocation of the displaced alveolar segment. (H) Intraoral view demonstrating the associated wide unrepaired cleft palate. (I) Preoperative three-dimensional computed tomography reconstruction demonstrating extensive orbital and maxillary skeletal deficiency with cranial displacement of the right alveolar segment. (J) Postoperative three-dimensional computed tomography reconstruction demonstrating restoration of alveolar arch continuity following first stage reconstruction.
Functional Outcomes
Functional outcomes were assessed at the most recent follow-up at a mean patient age of 4.8 years. Persistent feeding difficulty was reported in two patients, one associated with developmental delay and the other with a very wide cleft palate (Figure 2).
Structured CAPS-A–based speech assessment was available in 11 patients aged ≥2 years at latest follow-up; the remaining 2 patients aged <2 years were reported separately as non-assessable. At latest follow-up, the primary group without palatal cleft (n = 4) had normal speech and resonance. In the primary group with palatal cleft (n = 3), 2 patients had normal resonance and intelligibility after palatal repair, whereas 1 patient with a very large unrepaired cleft palate remained non-assessable because of absent sound production. In the referred group with palatal cleft (n = 3), all patients had velopharyngeal insufficiency at initial assessment; secondary speech procedures included Furlow palatoplasty revision, palatal re-repair with levator reconstruction, or buccinator flap reconstruction with or without palatal muscle re-repair, selected according to residual palatal anatomy, velopharyngeal dysfunction pattern, and the degree of palatal lengthening required. Following secondary speech surgery, 1 patient demonstrated marked clinical improvement, whereas residual VPI with hypernasality and cleft speech characteristics persisted in 2 at the latest follow-up. At latest follow-up, the single referred patient without palatal cleft had normal speech and resonance. Speech outcomes are summarized in Supplementary Table 5.
Orthodontic treatment was initiated in one patient. Five patients had age-appropriate dental arch development, whereas seven were considered likely to require orthodontic treatment with further growth. Severe visual impairment was present in four patients and was associated with major structural ocular abnormalities, including anophthalmia or microphthalmia, severe orbital dysplasia, and corneal opacity.
Complications
Postoperative complications were analyzed in the 10 surgically treated patients who underwent a total of 31 operative stages and were reported separately for primary cases (n = 6, 18 procedures) and referred revision cases (n = 4, 13 procedures).
In the primary group, one superficial wound infection resolved with conservative management, and one hypertrophic scar matured acceptably during follow-up; no wound dehiscence occurred. In the referred revision group, two superficial wound infections, one partial wound dehiscence requiring revision, and three hypertrophic or widened scars were observed. Overall, wound-related complications occurred in 3 of 10 patients and scar-related complications in 4 of 10, with partial overlap. No major adverse events, including postoperative hemorrhage, vision loss beyond baseline, skeletal failure, or airway compromise, were observed. Several deformities in referred patients, including residual asymmetry, exposure-related corneal opacity, nostril stenosis, and hypertrophic scarring, were already present at referral and were considered baseline findings rather than sequelae of procedures performed at our institution. Detailed complication data are summarized in Supplementary Table 4.
Residual Deformities at Latest Follow-up
Residual facial asymmetry of varying degrees persisted in all patients, most commonly involving the periorbital and midfacial subunits. Serial standardized clinical photographs obtained during routine follow-up were additionally reviewed to assess interval changes in eyelid continuity, ocular protection, oral competence, and gross facial symmetry following staged reconstruction. When available, follow-up imaging studies, including computed tomography, were reviewed to assess maintenance of orbital support, alignment of displaced alveolar segments, and restoration of maxillary arch continuity following staged reconstruction. In the primary-operated group, no interval worsening of clinically significant ectropion, eyelid coloboma, or ocular exposure was observed after reconstruction. In referred revision cases, residual eyelid deformity persisted in three patients despite substantial improvement in eyelid position and ocular protection, and residual VPI persisted in two despite secondary speech surgery. Pre-existing corneal opacity remained unchanged. Given the marked anatomical heterogeneity and retrospective design, objective anthropometric symmetry analysis was not feasible; therefore, longitudinal assessment focused on clinically observable restoration of structural continuity, ocular protection, oral competence, and maintenance of skeletal alignment.
Discussion
Rarity and Clinical Significance
Even in specialized craniofacial practice, combined multi-axis craniofacial clefts are encountered only rarely, underscoring the exceptional infrequency of these deformities in routine practice.10,11 Despite the modest cohort size, this single-center series provides practical insight into the anatomical heterogeneity, staged reconstructive burden, and early functional course of combined multi-axis craniofacial clefts. The marked variability in cleft combinations observed in this cohort further supports the concept that these deformities comprise a highly heterogeneous and clinically challenging subset within the Tessier spectrum.
Anatomical Diversity and Classification
Although the Tessier classification remains the standard framework for describing craniofacial clefts,1,12 some deformities do not conform readily to a single numbered cleft line. Oblique and multi-axis patterns may span several facial regions and are more consistent with overlapping developmental disturbances than with strictly discrete anatomical entities.4,9,13 Similar patterns were observed in the present series.
Notably, two patients demonstrated complex multi-axis deformities that could not be reliably categorized within the conventional Tessier framework. These involved multiple facial and cranial subunits, including the orbit, midface, alveolus, and cranial base, extending beyond a reproducible cleft axis (Figure 2; Table 1). Rather than corresponding to recognized syndromic patterns, these cases represented non-syndromic multi-field clefting that could not be reliably accommodated within the conventional numbering system and therefore highlight an important limitation of the Tessier framework in highly complex deformities.
Embryologic Considerations
The embryologic basis of craniofacial clefts remains incompletely understood and is likely multifactorial. Disturbances in neural crest cell migration, fusion of the facial processes, and regional craniofacial growth during early development have all been implicated.8,9 Paramedian clefts, such as Tessier clefts 3 and 4, are generally attributed to failed fusion between the maxillary and medial nasal processes, whereas lateral clefts, such as Tessier cleft 7, are associated with first branchial arch abnormalities. 9 In the present series, the more complex multi-axis patterns are better understood within a developmental field framework, in which abnormalities within and between adjacent craniofacial fields may produce clefts that extend beyond a single conventional Tessier axis. 14
Reconstructive Strategy
Reconstruction of craniofacial clefts typically requires multiple operative stages over several years of growth, with timing guided by functional priorities and facial development.10,14 In combined multi-axis deformities, the reconstructive burden is often greater than in single-axis clefts because multiple functional units—most commonly the orbit, palate, and midface—require coordinated restoration within the same patient. This burden may be further underestimated in referred patients who had already undergone prior procedures before presentation. In our series, early priority was consistently given to ocular protection and restoration of eyelid continuity, followed by skeletal support and contour refinement during growth. These findings support a function-prioritized staged framework in which restoration of essential functional units precedes secondary skeletal and contour refinement. Accordingly, Table 3 is presented as a descriptive clinical guide rather than a validated treatment algorithm.
Functional Outcomes
Restoration of function remains a primary objective in the management of craniofacial clefts, encompassing feeding, speech, ocular protection, and dental occlusion. Within the palatal cleft subgroup, structured CAPS-A–based assessment demonstrated a clear disparity between primary and referred revision cases. Favorable speech outcomes were observed in 2 of 3 primary-presenting patients, whereas all 3 referred patients with palatal involvement demonstrated velopharyngeal insufficiency at initial assessment. Following secondary speech surgery, one showed marked clinical improvement, while residual VPI persisted in 2 at the latest follow-up. Although these findings suggest a greater residual functional burden in previously operated multi-axis clefts, interpretation should remain cautious because baseline palatal anatomy was highly heterogeneous and included atypical oblique and transverse cleft extensions that differ substantially from conventional cleft palate morphology. In addition, variability in prior outside surgical technique, extent of repair, residual tissue quality, and age at revision further limited direct comparison with isolated cleft-palate cohorts. Previous reports have similarly emphasized the influence of palatal involvement on speech development in craniofacial clefts. 2 The frequent maxillary and alveolar involvement observed in this cohort also underscores the importance of longitudinal orthodontic follow-up, as growth-related arch and occlusal disturbances often require intervention during development.
Complications and Referral Patterns
Postoperative complications were predominantly minor and consisted mainly of superficial wound infection and scar hypertrophy, with no major surgical complications. Within this cohort, referred revision cases required more procedures at our institution and experienced more wound- and scar-related events than the primary-operated group (Table 2). This observation should be interpreted cautiously, given the heterogeneity of the referred subgroup with respect to age, growth phase, prior operative technique, tissue quality, and baseline deformity severity. Revision surgery in previously operated tissues was frequently challenged by pre-existing fibrosis, scar contracture, altered vascularity, and residual skeletal deficiency related to prior interventions and baseline deformity, increasing the complexity of operative planning and potentially necessitating additional staged procedures. Taken together, these findings underscore the value of early multidisciplinary management in specialized craniofacial centers, while recognizing that long-term skeletal symmetry and reconstructive durability remain to be defined after pubertal growth.
Comparison of Surgically Treated Primary-Presenting and Referred Revision Subgroups at our Center (n = 10).
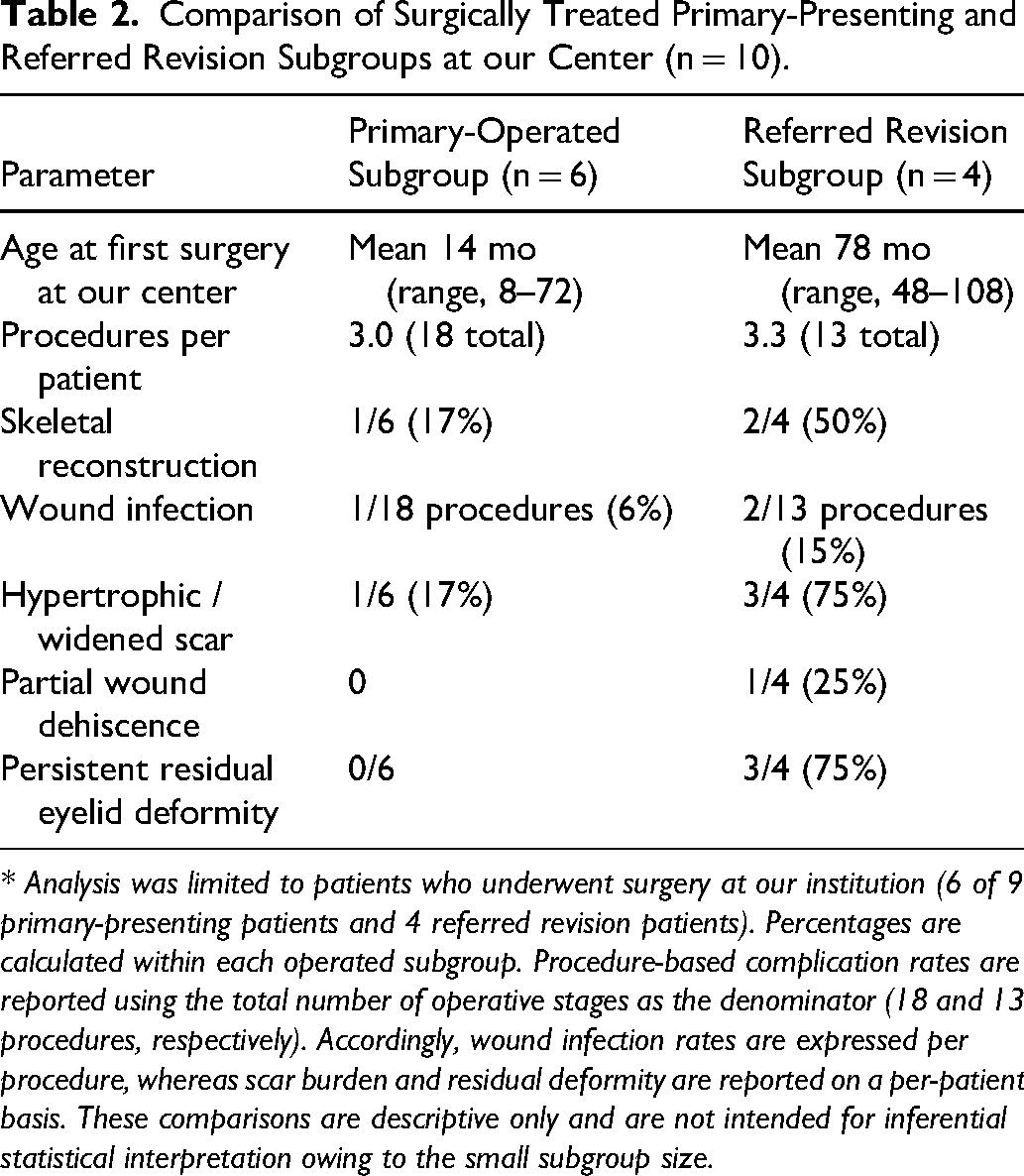
* Analysis was limited to patients who underwent surgery at our institution (6 of 9 primary-presenting patients and 4 referred revision patients). Percentages are calculated within each operated subgroup. Procedure-based complication rates are reported using the total number of operative stages as the denominator (18 and 13 procedures, respectively). Accordingly, wound infection rates are expressed per procedure, whereas scar burden and residual deformity are reported on a per-patient basis. These comparisons are descriptive only and are not intended for inferential statistical interpretation owing to the small subgroup size.
Descriptive Function-Guided Reconstructive Sequence for Combined Multi-Axis Tessier Clefts Based on Institutional Operative Experience.
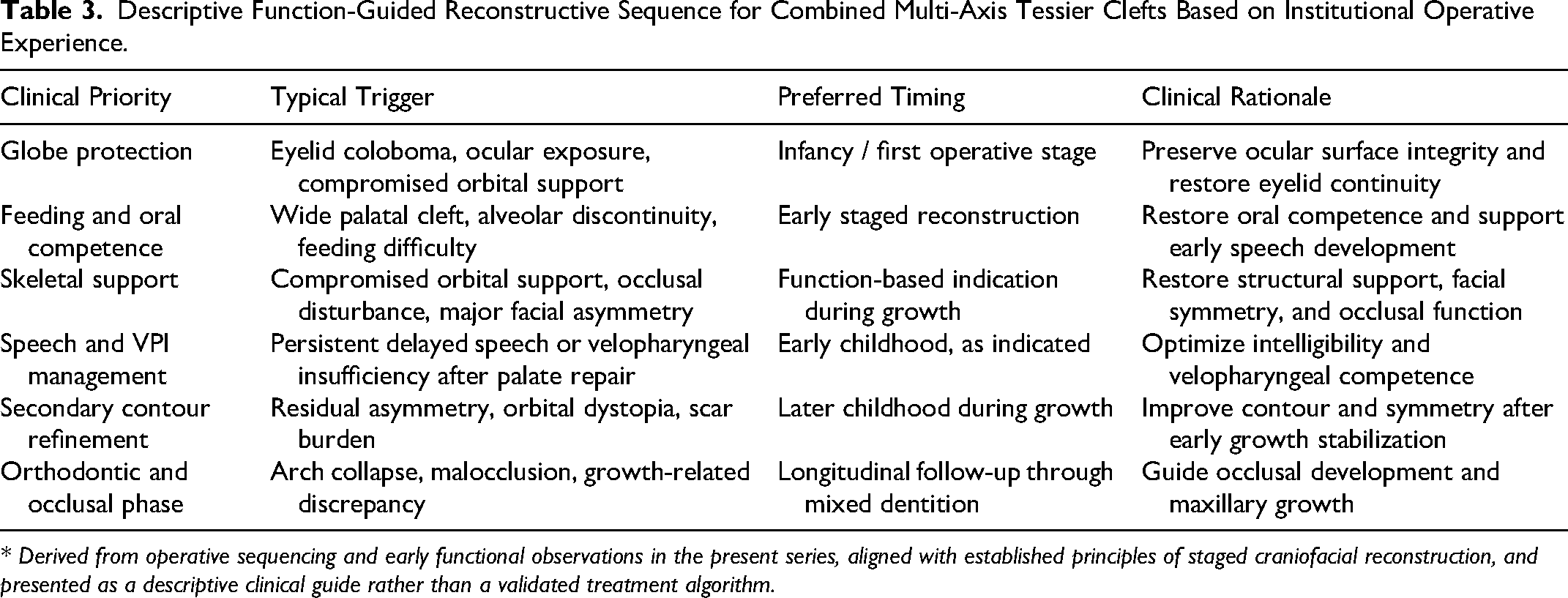
* Derived from operative sequencing and early functional observations in the present series, aligned with established principles of staged craniofacial reconstruction, and presented as a descriptive clinical guide rather than a validated treatment algorithm.
Limitations
The limited cohort size reflects the rarity of combined multi-axis craniofacial clefts. The small sample and marked phenotypic heterogeneity precluded formal comparative analysis and do not permit the development of a uniform treatment algorithm. In addition, the retrospective design limited the availability of uniform blinded longitudinal outcome assessment across this heterogeneous cohort; accordingly, feeding and speech findings should be interpreted as descriptive early clinical observations rather than comparative outcome measures. Interpretation of speech outcomes warrants particular caution because baseline palatal morphology was inherently heterogeneous, ranging from conventional cleft palate patterns to wide atypical or transverse extensions aligned with the facial cleft axis. In referred revision cases, variability in prior operative technique, extent of repair, residual tissue quality, and incomplete availability of outside operative records may have further influenced velopharyngeal function and speech outcomes. The small cohort size, heterogeneous palatal anatomy, and variability in prior outside palatal repair additionally precluded formal inferential comparison of speech outcomes with conventional cleft-palate populations. Future prospective studies incorporating standardized speech and velopharyngeal assessment instruments are needed to better define long-term functional outcomes. Continued follow-up through adolescence and beyond the pubertal growth spurt will be required to define long-term skeletal stability, occlusal development, facial symmetry, aesthetic outcomes, and reconstructive durability, as the current findings remain early growth-phase observations.
Conclusions
Combined multi-axis craniofacial clefts represent a rare and surgically demanding subset of congenital facial anomalies. Management requires individualized, function-prioritized staged reconstruction and sustained multidisciplinary follow-up throughout growth, with strategy guided by cleft distribution, functional priorities, and evolving craniofacial development.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261460777 - Supplemental material for Combined Multi-Axis Tessier Clefts: Surgical Management and Early Functional Outcomes From a Tertiary Center
Supplemental material, sj-docx-1-cpc-10.1177_10556656261460777 for Combined Multi-Axis Tessier Clefts: Surgical Management and Early Functional Outcomes From a Tertiary Center by Karam Allam, Shenouda Gameel and Sherif Bakri in The Cleft Palate Craniofacial Journal
Footnotes
Ethical Approval and Consent
Institutional review board approval for retrospective clinical analysis was obtained from the Medical Research Ethics Committee (MREC), Faculty of Medicine, Sohag University (IRB No. Soh-Med-26-3-10PD) before data collection. Written informed consent for treatment and publication of clinical photographs was obtained from the patients’ guardians.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. Data are not publicly available because of patient privacy considerations and the identifiable nature of clinical imaging.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.