
Abstract
Nasopalatine duct cysts may present with atypical radiographic features when arising in grafted alveolar cleft regions. A patient with cleft lip and palate presented with a well-defined radiolucent lesion in the anterior maxilla following alveolar bone grafting. Imaging demonstrated a unilocular lesion associated with displacement of the incisive canal, mimicking other odontogenic and nonodontogenic cysts. The unusual location and surgical history posed diagnostic challenges. Local trauma related to grafting may have contributed to cyst development. Careful radiographic assessment is essential for accurate differential diagnosis and appropriate management.
Introduction
The World Health Organization 1 classifies the nasopalatine duct cysts (NDCs) as the most common developmental nonodontogenic cyst of the jaws, typically occurring in the fourth to sixth decades of life with a slight male predilection. 2 The NDCs arise in the midline of the anterior maxilla from epithelial remnants of the nasopalatine duct within the incisive canal. 3 Although their pathogenesis has been associated with local stimulation, including trauma and surgical intervention, their occurrence in alveolar cleft regions following secondary bone grafting (SBG) remains rare. 4
In patients with cleft lip and palate, anatomical variations of the nasopalatine canal may alter the radiographic presentation of lesions in this region, potentially mimicking other odontogenic and nonodontogenic cysts. 5 This diagnostic overlap is particularly challenging in grafted areas, where postsurgical changes and graft-related conditions must also be considered.6,7
This report presents a rare case of NDC arising in a grafted alveolar cleft site and emphasizes the importance of detailed radiographic assessment for accurate differential diagnosis among cystic lesions in this complex anatomical context.
Case Report
An 18-year-old female patient with a history of left complete cleft lip and alveolar cleft underwent an SBG using recombinant human bone morphogenetic protein-2 (rhBMP-2; INFUSE® Bone Graft) 8 years prior. The patient presented with a complaint of pressure in the anterior maxillary region.
A periapical radiograph of the maxillary incisors revealed a well-circumscribed, corticated, unilocular radiolucency located adjacent to the grafted alveolar site, involving the region of the left lateral incisor (Figure 1). Despite the radiographic features suggestive of a radicular cyst, the lamina dura appeared intact. Pulp sensibility tests from canine to canine showed normal responses, ruling out an inflammatory periapical lesion.

Periapical radiograph showing a well-defined radiolucent lesion at the periapical region of the left lateral incisor, adjacent to the alveolar bone graft.
Cone-beam computed tomography (CBCT) was performed to further assess lesion extent and its relationship with adjacent structures. The exam was acquired using a Dentsply Sirona Axeos unit (FOV: 5 × 5.5 cm; voxel size: 0.08 mm). Imaging demonstrated a well-defined, homogeneous, unilocular hypodense lesion extending toward the palatal aspect, measuring approximately 13 mm in height, 10 mm in width, and 11 mm in depth (Figure 2). The lesion was located in close proximity to the incisive canal region, without evidence of root resorption or cortical perforation (Figure 3).

Cone-beam computed tomography (CBCT) multiplanar reconstructions demonstrating lesion extent: (A) axial view (mesiodistal dimension); (B, C) sagittal views (buccopalatal and superoinferior dimensions).

Cone-beam computed tomography (CBCT) images showing the relationship between the lesion and adjacent structures: (A) axial view demonstrating communication with the incisive canal (arrow); (B) coronal view showing deviation of the incisive canal in the grafted cleft area; (C) sagittal view demonstrating cortical thinning and preservation of adjacent tooth roots.
Based on imaging findings and clinical history, the differential diagnosis included developmental cysts such as the NDC and odontogenic keratocyst, as well as a surgical ciliated cyst due to the history of prior surgical intervention in the region.
Surgical enucleation was performed. Histopathological analysis revealed a cystic cavity lined by fibrous connective tissue containing vascular structures, mucous cells, and small glandular ducts (Figure 4), consistent with a diagnosis of NDC.
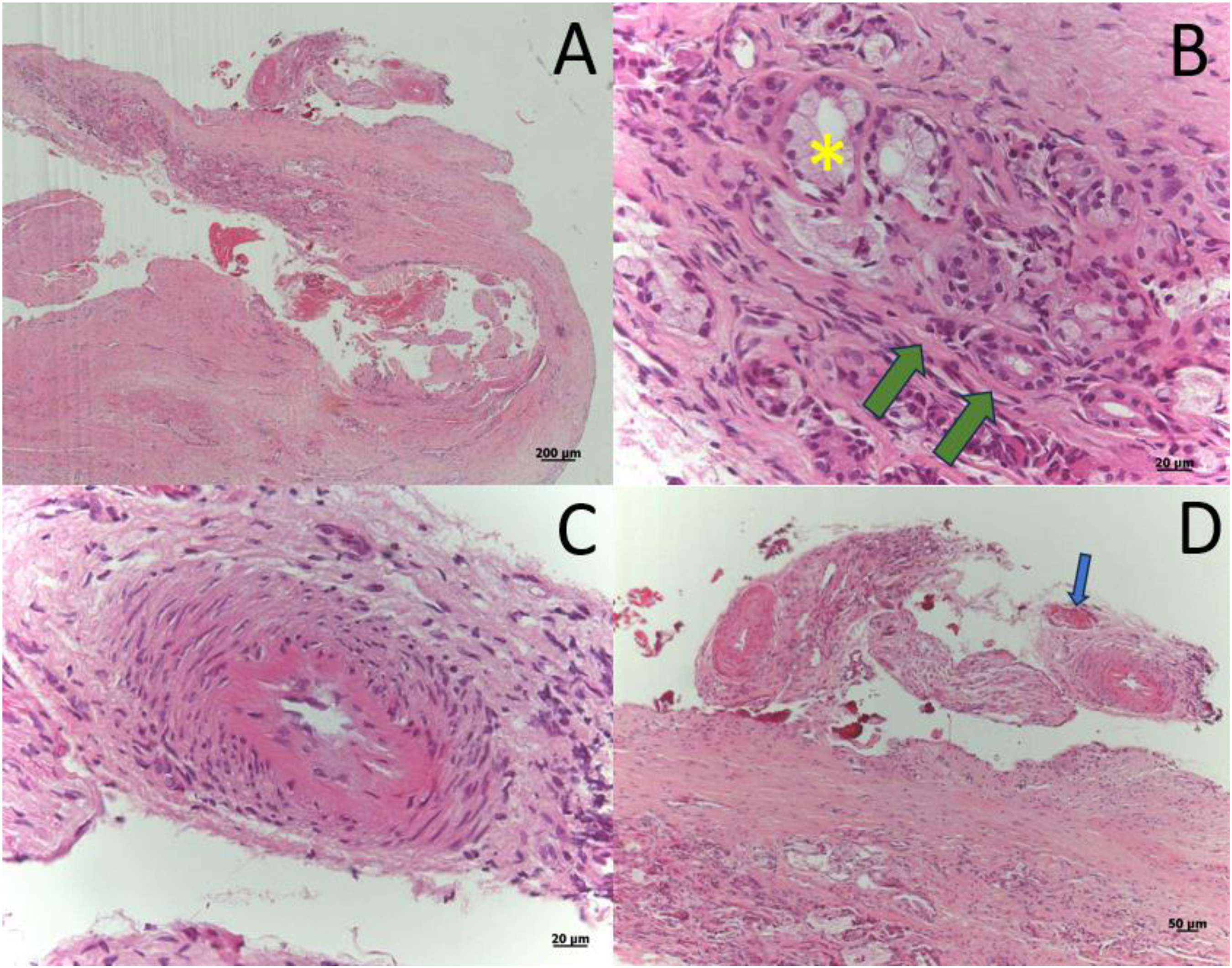
Photomicrographs (hematoxylin–eosin staining): (A) 200× HE: cystic cavity with fibrous capsule; (B) 20× HE: mucous cells (asterisk) and glandular ducts (green arrows); (C) 20× HE: neurovascular bundle; (D) 50× HE: dilated blood vessels (blue arrow).
Discussion
Radiolucent cystic lesions of the jaws encompass a broad spectrum of odontogenic and nonodontogenic entities. Careful assessment of lesion location, relationship with adjacent teeth and anatomical structures, and clinical history is essential for establishing an appropriate differential diagnosis. In patients with cleft lip and palate, this evaluation becomes more challenging due to anatomical variations, particularly involving the incisive canal, which may alter the expected radiographic presentation of lesions.5,8,9
Among odontogenic cysts, the radicular cyst is the most common lesion affecting the anterior maxilla. It arises from inflammatory processes associated with nonvital teeth. Radiographically, disruption of the lamina dura and loss of pulp vitality are key features supporting this diagnosis. In the present case, the preservation of the lamina dura and normal pulp sensibility tests effectively excluded an inflammatory periapical origin.8,10,11
Once odontogenic inflammatory lesions are ruled out, the NDC becomes the most likely nonodontogenic cyst in this region. The NDCs are typically located in the midline, associated with the incisive canal, and may present as well-defined radiolucencies exceeding the normal diameter of the canal. However, anatomical variations, especially in patients with cleft lip and palate, may result in displacement or distortion of the canal, leading to atypical lesion positioning and increased diagnostic complexity.1,5
Although the occurrence of odontogenic keratocysts in grafted alveolar cleft regions has not been reported and is uncommon in the anterior maxilla, it was considered in the differential diagnosis due to its radiographic presentation as a well-defined radiolucent lesion. 8
In patients with a history of alveolar bone grafting, the surgical ciliated cyst must also be considered. This lesion is believed to arise from the implantation of respiratory epithelium during surgical procedures, presenting as a well-demarcated radiolucency in previously operated areas. Therefore, clinical history plays a crucial role in narrowing the differential diagnosis in such cases.7,12,13
Another relevant aspect of the present case is the history of alveolar cleft grafting with rhBMP-2. Although rhBMP-2 has been used as an alternative to autogenous bone grafting in selected craniofacial applications, its use in skeletally immature patients remains off-label. 14 In addition, rhBMP-2 is a potent osteoinductive agent and has been associated with several clinical adverse effects, including postoperative inflammation, ectopic bone formation, osteoclast-mediated bone resorption, osteolysis, and altered tissue remodeling.15,16 These biological effects may contribute to heterogeneous bone repair and radiographic changes in previously grafted areas, potentially complicating the distinction between postoperative remodeling, graft-related alterations, and cystic pathology.
Concerns regarding the interaction between BMP signaling and abnormal tissue growth have also been raised, particularly because rhBMP-2 is a growth factor involved in cellular differentiation and tissue repair. However, current evidence regarding carcinogenicity remains conflicting, and a causal association between rhBMP-2 and new malignancy has not been established. 17 Nevertheless, this reinforces the importance of cautious indication, especially in off-label pediatric craniofacial applications, and long-term radiographic follow-up. 18
A limitation of this report is the absence of an identifiable epithelial lining in the histopathological analysis. This finding may be attributed to epithelial detachment during surgical removal or histotechnical processing. Nevertheless, the lesion's anatomical relationship with the incisive canal and the presence of neurovascular structures within the cystic wall strongly support the diagnosis of NDC.
Conclusion
Nasopalatine duct cysts may present with atypical radiographic features when arising in grafted alveolar cleft regions due to anatomical displacement of the incisive canal. This variation increases diagnostic complexity and may mimic other odontogenic and nonodontogenic cysts. Local surgical trauma related to alveolar bone grafting may represent a contributing factor. Accurate diagnosis relies on careful radiographic assessment combined with clinical and histopathological correlation.
Footnotes
Ethical Approval and Informed Consent
This study was approved by the Research Ethics Committee of The Hospital for Rehabilitation in Craniofacial Anomalies of the University of São Paulo with approval number: 71112123.0.0000.5441. The patient provided written informed consent for the publication of clinical and imaging data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior [Finance Code 001].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.