
Abstract
Objectives
We aimed to quantify the prevalence of perioperative complications attributable to external activation ports in pediatric posterior cranial vault distraction osteogenesis (PCVDO) and to evaluate the influence of distraction protocol parameters on complication risk.
Methods
Following PRISMA 2020 guidelines, six databases (2009-2025) were searched for studies reporting complications in children (<18 years) undergoing PCVDO.
Results
Across 25 eligible studies, 154 adverse events were reported, yielding a pooled overall complication rate of 28.1%. Wound infection was most common (13.7%), followed by broken external activation ports (4.5%) and loosened footplates (3.1%). Mechanical failures accounted for 35.7% of all adverse events and frequently necessitated unplanned surgical intervention: 40% required intraoperative adjustment or premature removal of the distraction system. Each additional day of active distraction increased the risk of footplate loosening by 17%, while each additional day of consolidation increased the risk of breakage of the external activation ports by 1%, indicating cumulative mechanical stress on the distraction. External activation ports were associated with an elevated risk of wound infection, mechanical failure, and unplanned return to the operating room in pediatric PCVDO. The mechanical analyses demonstrated that off-axis loading, torque transmission through skin exits, and cumulative cyclic forces during prolonged distraction and consolidation phases could negatively impact device stability and vector fidelity.
Conclusions
These findings highlight the inherent mechanical limitations of externalized subcutaneous craniofacial distraction systems and underscore the need for next-generation, fully internalized, external port-free distraction technologies that optimize biomechanical alignment, reduce soft-tissue morbidity, and enhance clinical reliability.
Introduction
For more than three decades, craniofacial distraction osteogenesis (DO) has predominantly relied on externalized subcutaneous distraction systems with external activation ports protruding through the skin. 1 Since 2009, these systems have been widely adopted in the management of complex craniosynostosis to expand intracranial volume, normalize elevated intracranial pressure (ICP), and correct craniofacial deformities.2,3 Although posterior cranial vault distraction osteogenesis (PCVDO) is clinically effective, external activation ports pose a potential risk of complications, including wound infection, skin necrosis, distraction system exposure, broken external activation ports, loosened footplates, mechanical failure, and lack of compliance among patients and their caregivers, as well as the significant psychological and social burdens for older children because of the visible cosmetic impact.3–6
This systematic review and proportional meta-analysis aimed to: (1) quantify the pooled prevalence of complications related to external activation ports—including overall complication rates, wound infection, exposed distraction system, loosened footplates, premature removal of the distraction system, and unexpected return to the operating room (OR) and (2) examine the influence of key moderators—such as patient age, latency, active distraction and consolidation periods, and total time the distraction system remained in situ—on complication rates, thereby highlighting their effects on surgical outcomes and patients’ quality of life. Through this comprehensive evaluation, we sought to inform optimal patient selection and surgical planning and to highlight opportunities for refinement and innovation in craniofacial distraction technology to enhance mechanical safety and clinical efficacy.
Methods
Systematic Literature Search
A systematic literature review was conducted in accordance with the PRISMA 2020 reporting guidelines. 7 We searched the Medline/PubMed, Google Scholar, Web of Science, Scopus, and Embase databases for studies published between 2009 and 2025 that evaluated perioperative complications associated with external activation ports of craniofacial distraction systems in pediatric patients (<18 years) undergoing PCVDO for craniosynostosis.
A perioperative complication was defined as any adverse event occurring intraoperatively or at any point during the postoperative period up to completion of distraction and subsequent removal of the distraction system. The search strategy incorporated keywords related to craniosynostosis, cranial / craniofacial distraction, and specific complications, including wound infection, wound dehiscence, skin necrosis, distraction system exposure, loosened footplates, broken external activation ports, and mechanical failure.
Inclusion and Exclusion Criteria
Studies were eligible for inclusion if they met the following criteria: (1) involved pediatric patients (<18 years); (2) were peer-reviewed research articles published between 2009 and 2025; (3) reported perioperative complications in two or more patients with craniosynostosis undergoing PCVDO; and (4) were written and published in English. We excluded single case reports, letters to the editor, technical notes, narrative or systematic reviews, preclinical or animal studies, and articles that did not meet the predefined inclusion criteria.
Data Extraction
All retrieved studies were initially screened based on their titles and abstracts. Articles that appeared relevant were subsequently reviewed in full to confirm data availability and adherence to the inclusion criteria. For each eligible study, the following variables were extracted: first author's surname, year of publication, country of origin, study design (retrospective or prospective), study period, sample size, patient sex, age at distractor implantation, duration of follow-up, craniosynostosis type (syndromic or non-syndromic), and details of the distraction protocol (number of distractors used, distraction rate and frequency, latency period, active distraction period, consolidation period, total duration of hardware implantation, and total distraction distance). The latency period was defined as the interval between hardware implantation and initiation of distraction, whereas the consolidation period referred to the interval between completion of distraction and hardware removal. Perioperative complications included wound infection, wound dehiscence, skin necrosis, distraction system exposure, loosened footplates, and broken external activation ports. Data on premature device removal and unexpected return to the OR were also collected.
Data Synthesis
Data from all eligible studies were aggregated into a structured spreadsheet for further systematic evaluation. A qualitative synthesis was first performed to integrate the extracted information and identify recurring patterns across study methodologies, patient demographics, and reported outcomes. This comparative assessment enabled the development of a coherent narrative summarizing the overall evidence.
For the quantitative analysis, mean values were calculated for patient age, follow-up duration, latency, active distraction, and consolidation periods, total time the distraction system remained in situ, total distraction distance, and intracranial volume gain. These summary metrics provided a concise overview of central tendencies across studies and facilitated comparison of key clinical and operative parameters.
Quality Assessment
Study quality was appraised using the Newcastle-Ottawa Scale (NOS), which evaluates observational studies across three domains. 8 The Selection domain assesses factors such as cohort representativeness, sample size, and response rates; comparability examines the adequacy of methods used to control for confounding; and outcome assessment evaluates the robustness of outcome measurement and appropriateness of statistical analyses. The NOS assigns up to four stars for selection, two stars for comparability, and three stars for outcome assessment, for a maximum score of nine. Based on total scores, studies were categorized as low quality (0-3 stars), moderate quality (4-6 stars), or high quality (7-9 stars).
Statistical Analysis
All statistical analyses were performed using R-Studio, Version 2025.09.2 + 418. All meta-analysis computations—including proportional meta-analysis, heterogeneity evaluations, meta-regression modeling, and publication bias assessments—were conducted using the Metafor and Meta packages. A two-tailed P < .05 was considered indicative of statistical significance.
Pooled Proportional Estimation
A proportional meta-analysis was performed on 25 studies, comprising 582 pediatric patients with craniosynostosis treated with PCVDO. The primary outcome was the total number of perioperative complications; secondary outcomes included wound infection, broken external activation ports, loosened footplates, distraction system exposure, premature removal of the distraction system, and unexpected return to the OR.
We applied a random-intercept logistic regression model—a generalized linear mixed model (GLMM) with a logit link and binomial distribution—to account for differences in event rates and sample size across studies. 9 This approach incorporated both within- and between-study variability, thereby yielding more robust pooled estimates than traditional inverse-variance methods. Between-study heterogeneity was modeled through a random intercept estimated via maximum likelihood (ML). 10 Pooled proportions were reported with 95% confidence intervals (CIs), derived by back-transforming estimates from the logit scale.
Heterogeneity Quantification
Residual heterogeneity and between-study variability were evaluated by comparing models fitted with and without random effects. 11 We reported several measures of heterogeneity on the logit scale, including between-study variance (τ2), standard deviation of true effects (τ), proportion of total variability attributable to between-study differences (I2), and the ratio of total to within-study variability (H2). 12 The I2 statistic ranges from 0%-100% and is conventionally interpreted as low (0%-25%), moderate (25%-50%), substantial (50%-75%), or considerable (75%-100%) heterogeneity. 12
However, the observed wide confidence intervals surrounding I2 estimates reflect inherent uncertainty, influenced by the number of included studies, low event rates, and variation in sample size. Under such conditions, I2 becomes an imprecise heterogeneity indicator because it depends on the Q statistic, which has limited power and high sampling variability. Consequently, interpretation of heterogeneity based solely on I2 should be supplemented with more sensitive likelihood-based approaches.
To this end, we employed the likelihood ratio test (LRT) to assess whether incorporating random effects improved model fit. The LRT provides greater sensitivity for detecting between-study heterogeneity, and discrepancies between I2-based assessments and LRT results underscore the advantages of likelihood-based methods in mixed-effects meta-analysis and their ability to identify heterogeneity that may be missed by traditional Wald-type Q tests.
Publication Bias and Small-Sample-Size Effects
Potential publication bias and small-sample-size effects were evaluated using Egger's regression test, a post hoc diagnostic based on a weighted linear regression model. 13 Inverse-variance weights were calculated from the observed sampling variances. The resulting intercept, its standard error, and corresponding p-value were reported. A negative intercept suggests that smaller studies tend to report disproportionately higher event rates, consistent with small-study or publication-related biases.
Mixed-Effects Meta-Regression Analysis of Moderators
Random-effects meta-regression analyses were conducted using the GLMM framework to investigate associations between study-level moderators and both primary and secondary outcomes. 11 The moderators examined included patient age at distraction system implantation, latency period, active distraction period, consolidation period, and total time the distraction system remained in situ.
Model outputs were reported as regression coefficients (β), standard errors (SE), z-statistics, P-values, and 95% CIs. A statistically significant coefficient was interpreted as evidence of an association between the moderator and the outcome rate across studies, beyond what would be expected from random variation alone.
Dealing with Missing Data
The GLMM in the Metafor package relies on an available-case analysis for handling missing data. When a covariate is absent for a given study, that study is excluded only from analyses requiring the missing variable, but remains included in all other model components for which its data are complete. In contrast, studies lacking outcome data cannot contribute to the likelihood and are therefore omitted from the corresponding analysis.
Because the GLMM framework uses ML estimation, only observed data are modeled. Consequently, in meta-regression analyses, studies missing values for a moderator are excluded from the meta-regression but may still contribute to the intercept-only (base) model. This approach results in listwise deletion at the moderator level rather than excluding the entire study.
Results
A total of 1572 studies were retrieved (Supplementary Figure 1). Twenty-five studies, comprising 582 patients, met the inclusion criteria. Only five studies were prospective.2,14–17 Of the 25 studies included, 12 were rated as high quality,5,14,17–26 while the remaining 13 were classified as moderate quality,2,4,15,16,27–35 reflecting notable methodological limitations, particularly within the comparability domain. All studies employed sampling strategies representative of the target population and clearly defined both surgical interventions and primary outcomes. Most also reported adequate follow-up, with detailed documentation of postoperative results, including complications, reoperations, and quantitative measures such as volumetric and morphometric changes (Supplementary Table 1).
The mean age at the time of surgical implantation of the distraction system was 26.4 months (range, 3-105.6 months). Male patients accounted for 44.6% of the cohort. The mean follow-up period was 36.6 months (range, 9.2-94.8 months) (Table 1). Syndromic craniosynostosis was documented in 431/582 (74%) patients. Among those, approximately 40% were unspecified. Apert syndrome was the most common diagnosis (23.2%), followed by Crouzon syndrome (15.8%), Muenke syndrome (8.4%), Saethre-Chotzen syndrome (7.8%), and Pfeiffer syndrome (4.8%). Elevated ICP was reported in 203/548 (37%) patients.
Eligible Studies.
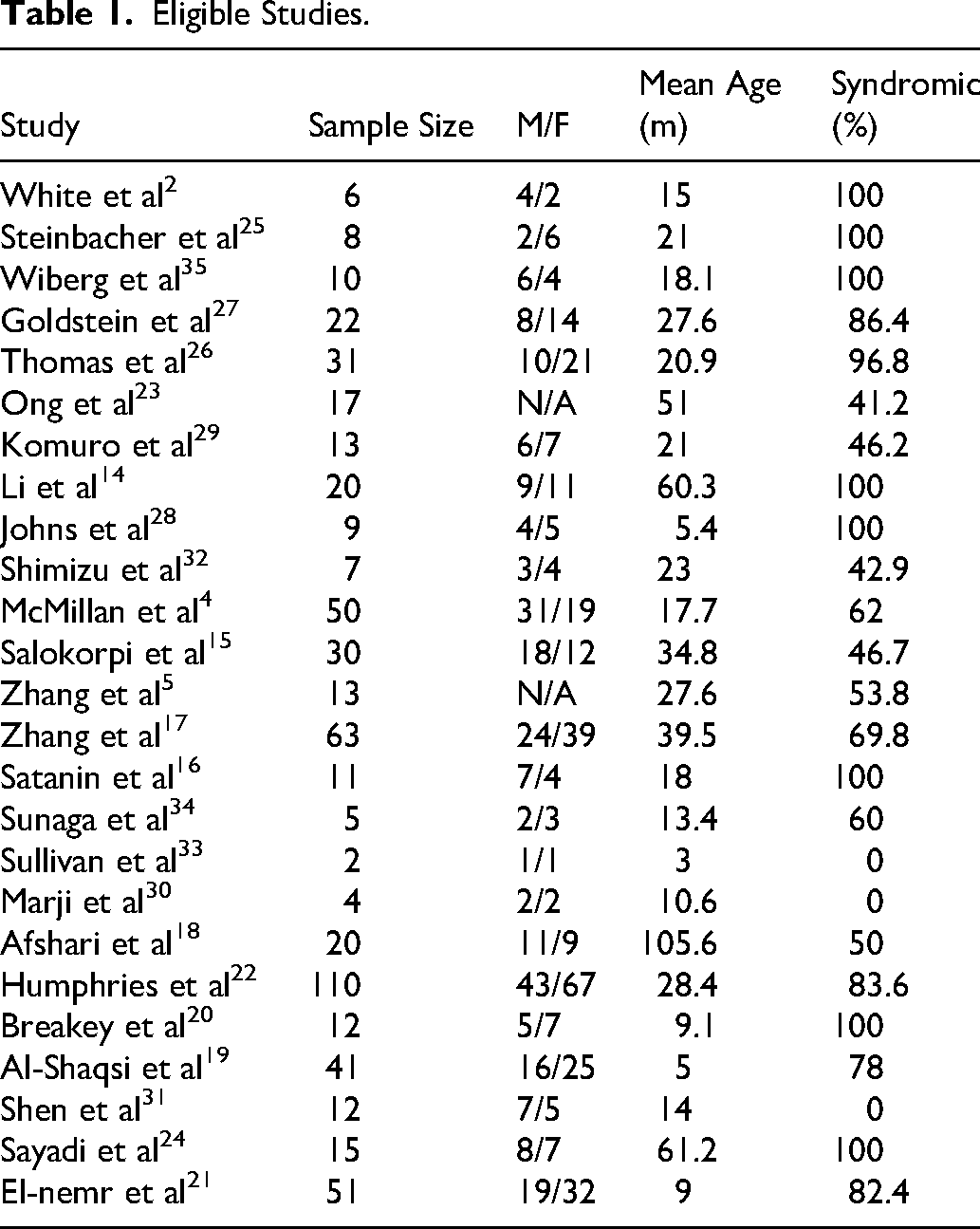
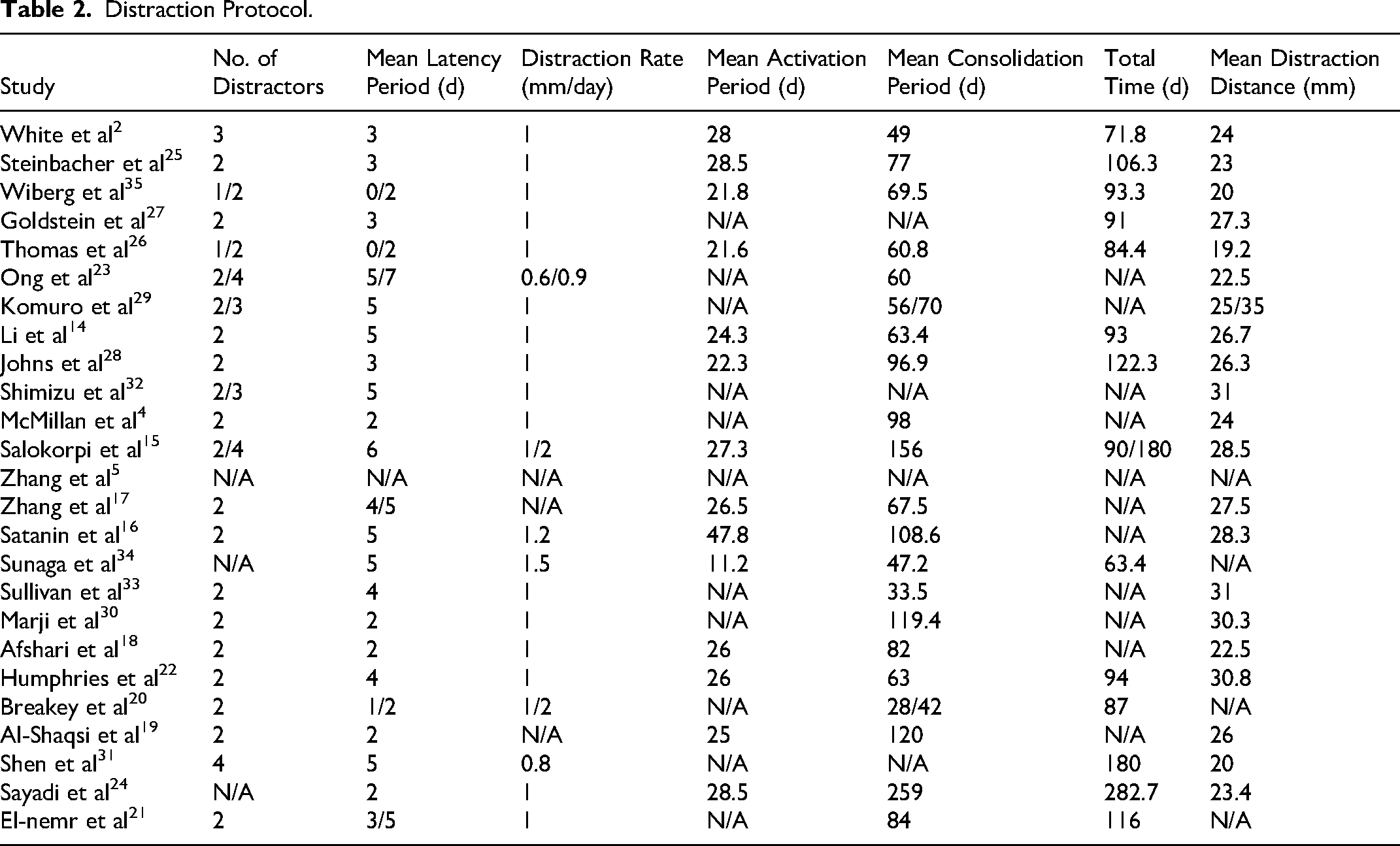
The use of two distractors was reported in 80% of studies. The mean latency, active distraction, consolidation periods, and total time the distraction system remained in situ were 3.7 days (range, 0-7 days), 26 days (range, 11.2-47.8 days), 90.2 days (range, 33.5-259 days), and 114.2 days (range, 63.4-282.7 days), respectively. The mean distraction distance achieved was 25.6 mm (range, 19.2-35 mm) with an average gain in intracranial volume of 218.55 cm3 (Table 2).
Distraction Protocol.
A total of 154 adverse events were documented in all eligible studies. Wound infection (69/154) was the most frequently reported adverse event, accounting for 44.8% of all adverse events. Broken external activation ports (30/154) and distraction system exposure (30/154) ranked second, each accounting for 19.5%, followed by loosened footplates (25/154, 16.2%).
Among the 69 patients who developed wound infections, 39 (56.5%) were successfully managed conservatively with local wound care, irrigation, and intravenous (IV) antibiotics. The remaining 30 (43.5%) patients required intraoperative intervention. Of these, 9 (30%) underwent surgical wound debridement, while 21 (70%) required early removal of the distraction system.
Of the 55 patients who experienced either broken external activation ports or loosened footplates, 15 (27.3%) required early removal of the distraction system due to mechanical failure. Seven (12.7%) underwent intraoperative adjustment of the distraction system under general anesthesia, and eight (14.5%) had their external activation ports replaced in the outpatient clinic. The remaining 25 (45.5%) patients were managed conservatively until distraction was completed. Notably, all 30 patients with exposed distraction systems were treated successfully with conservative wound care alone.
Proportional Meta-Analysis
Using a random-effects model, we conducted a proportional meta-analysis of 25 studies comprising 582 patients and 154 reported adverse events. The pooled overall complication rate was 28.1% (95% CI: 19.8%-38.2%) (Figure 1A). Among the secondary outcomes, wound infection was the most frequent complication, with a pooled rate of 13.7% (95% CI: 9.6%-19.1%) (Figure 1B). This was followed by broken external activation ports (Figure 2A) at 4.5% (95% CI: 2.6%-7.8%), loosened footplates (Figure 2B) at 3.1% (95% CI: 1.4%-6.9%), and exposed distraction system at 1.9% (95% CI: 0.51%-6.6%) (Supplementary Figure 2). The pooled estimates for premature removal of the distraction system and unexpected return to the OR were 4.1% (95% CI: 1.8%-8.8%) and 7.2% (95% CI: 3.7%-13.6%), respectively (Supplementary Figures 3 and 4).
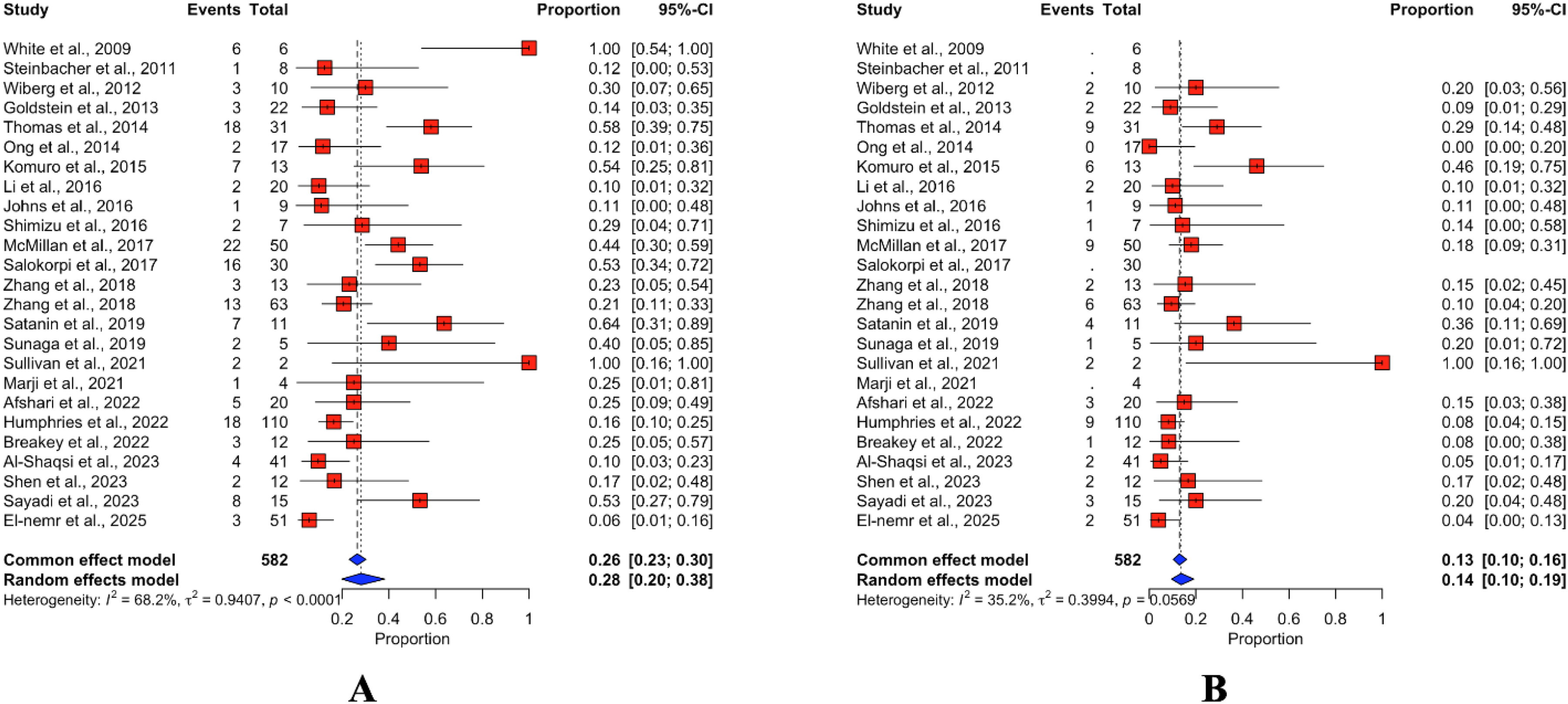
Forest plot of proportional meta-analyses for adverse events attributable to the external activation ports in children who underwent PCVDO using externalized subcutaneous craniofacial distraction systems. This forest plot presents the individual study-level estimates and pooled event proportions with 95% confidence intervals (CIs) for (A) total adverse events and (B) wound infection. The red squares represent individual study proportions, with the size of each square proportional to the study's weight. Horizontal lines indicate 95% CIs for each study. The blue diamond symbols at the bottom of each panel represent the summary estimates for the common and random-effects models, based on a generalized linear mixed model (GLMM) with a logit link and a binomial distribution. The size of the diamond reflects the precision and degree of variance among studies. The smaller the diamond, the lower the variance between studies. Between-study heterogeneity is quantified by τ2 (between-study variance) and I2 (the percentage of variation due to heterogeneity).
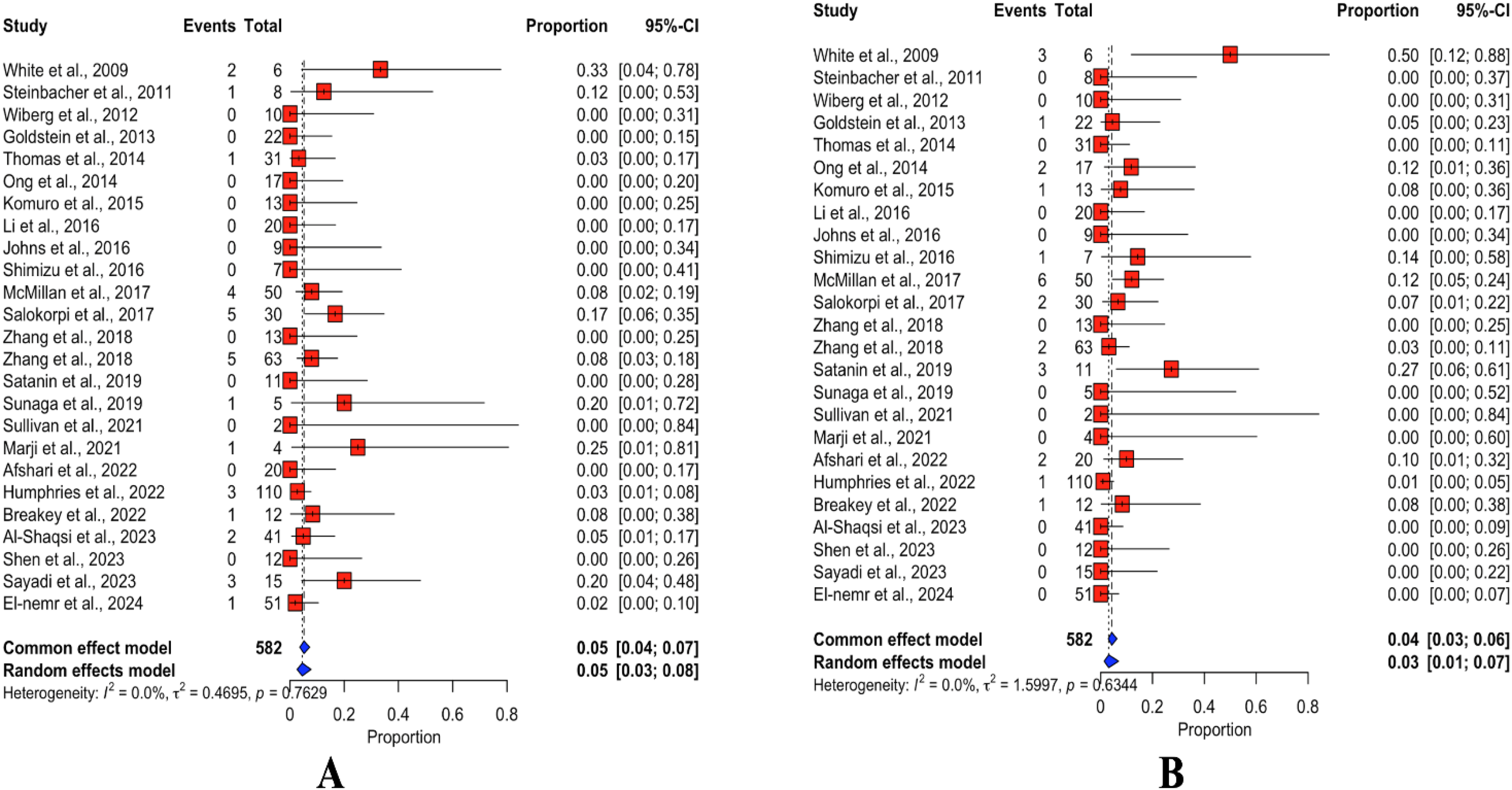
Forest plot of proportional meta-analyses for (A) broken external activation ports and (B) loosened footplates attributable to the external activation ports in children who underwent PCVDO using externalized subcutaneous craniofacial distraction systems.
We observed significant variability across studies depending on the outcomes assessed. For the overall number of adverse events, substantial heterogeneity was observed. The random-effects model estimated a τ2 of 0.94 (τ = 0.97), with an I2 of 68.2% (95% CI: 51.8%-78.9%), and an H value of 1.77 (95% CI: 1.44-2.18). Both the Wald-type Q test (Q = 75.35, df = 24, P < .0001) and the likelihood ratio test (LRT = 108.23, df = 24, P < .0001) confirmed statistically significant heterogeneity. For wound infection, heterogeneity was moderate based on Q-derived metrics with estimated τ2 = 0.4 (τ = .63), I2 = 35.2% (95% CI: 0.0%-61.8%); an H value = 1.42 (95% CI: 1.00-1.62); and non-statistically significant Wald-type Q test (Q = 30.87, df = 20, P = .06). However, the LRT showed a substantial improvement in model fit upon including a random-effects term (LRT = 45.2, df = 20, P = .001), indicating statistically significant between-study heterogeneity that was not fully captured by the Q statistic.
Across distraction system-related outcomes, Q-derived metrics consistently suggested no detectable heterogeneity. For broken external activation ports, the estimated τ2 was 0.47 (τ = 0.69) with an I2 of 0.0% (95% CI: 0.0%-43.9%) and an H value of 1.00 (95% CI: 1.00-1.33). The Wald-type Q test was not statistically significant (Q = 18.79, df = 24, P = .76). Similar patterns were observed for loosened footplates (τ2 = 1.6, τ = 1.26, I2 = 0.0%, 95% CI: 0.0%-43.9%; H = 1.00, 95% CI: 1.00-1.33; Q = 21.07, df = 24, P = .63). For distraction system exposure, Q-derived estimates again showed no heterogeneity, despite a comparatively larger variance (τ2 = 3; τ = 1.73; I2 = 0.0%, 95% CI: 0.0%-46.2%; H = 1.00, 95% CI: 1.00-1.36; Q = 19.53, df = 21, P = .55). In contrast to these Q-based metrics, the LRT consistently demonstrated substantial improvement in model fit upon including a random-effects term. This was evident for broken external activation ports (LRT = 39.25, df = 24, P = .03), loosened footplates (LRT = 51.43, df = 24, P = .0009), and distraction system exposure (LRT = 67.9, df = 21, P < .0001).
For premature removal of the distraction system, moderate heterogeneity was observed across studies (τ2 = 1.75; τ = 1.32; I2 = 32.2%, 95% CI: 0.0%-58.4%; H = 1.21, 95% CI: 1.00-1.55). The Wald-type Q test approached but did not reach statistical significance (Q = 35.4, df = 24, P = .06), whereas the LRT identified a significant improvement in model fit, indicating statistically significant between-study heterogeneity (LRT = 62, df = 24, P < .0001). For unplanned return to the OR, our analysis revealed low heterogeneity (τ2 = 1.77; τ = 1.33; I2 = 24.5%, 95% CI: 0.0%-53.9%; H = 1.15, 95% CI: 1.00-1.47. The Wald-type Q test did not reach statistical significance (Q = 31.79, df = 24, P = .13), yet the LRT again detected statistically significant heterogeneity (LRT = 74.48, df = 24, P < .0001). These results indicate that although conventional heterogeneity metrics failed to detect variability across studies, the LRT revealed underlying between-study differences that were not captured by Q or I2 statistics, highlighting the greater sensitivity of likelihood-based approaches in GLMM-based meta-analyses.
Egger's test for funnel plot asymmetry showed statistically significant evidence of small-sample-size effects and publication bias across 25 studies reporting loosened footplates (τ = −2.46, bias intercept = −1.37, SE = 0.56, P = .02) and 22 studies reporting distraction system exposure (τ = −3.85, bias intercept = −1.76, SE = 0.46, P = .001) (Figure 3). On the other hand, the test showed neither small-sample-size effects nor publication bias among 25 studies reporting the total number of adverse events (t = −0.13, df = 23, bias intercept = −0.1, SE = 0.87, P = .9); 21 studies reporting wound infection (t = −.04, df = 19, bias intercept = −.03, SE = 0.79, P = .47), 25 studies reporting broken external activation ports (t = −1.47, df = 23, bias intercept = −0.7, SE = 0.48, P = .15), 25 studies reporting premature removal of the distraction system (t = −1.55, df = 23, bias intercept = −0.91, SE = 0.59, P = .14), and 25 studies reporting unexpected return to the OR (t = −0.85, df = 23, bias intercept = −0.5, SE = 0.6, P = .4).
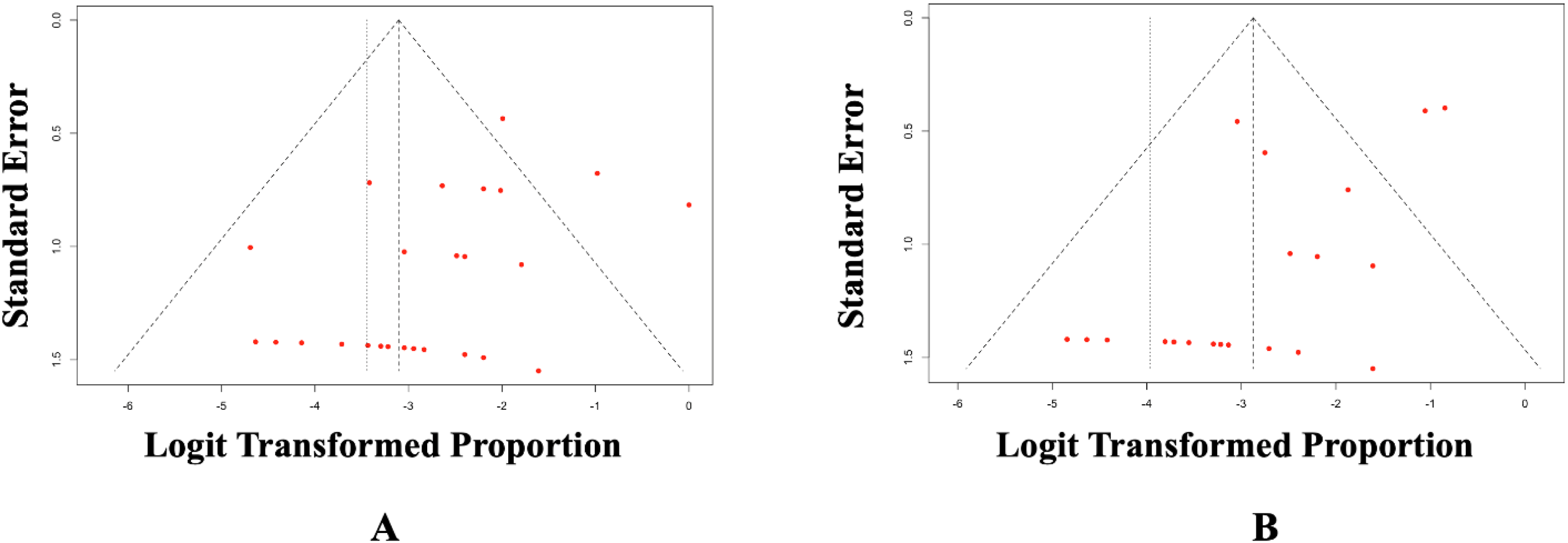
Funnel plots assessing publication bias and small-sample-size effects in (A) 25 studies reporting loosened footplates and (B) 22 studies reporting distraction system exposure in patients who underwent PCVDO using an externalized subcutaneous craniofacial distraction system. This funnel plot displays the relationship between study precision (standard error on the vertical axis) and logit-transformed event proportions (horizontal axis). Each red dot represents an individual study. Studies positioned asymmetrically, particularly those clustering on the right side with a smaller sample size, suggest potential small-sample-size effects. This asymmetry is supported by Egger's regression test, which demonstrated statistically significant evidence of small-sample-size effects and publication bias for (A) loosened footplates (τ = −2.46, SE = .56, bias intercept = −1.37, P = .02) and (B) Distraction System Exposure (τ = −3.85, SE = .46, bias intercept = −1.76, P = .0001).
Mixed-Effects Meta-Regression Analysis of Moderators
We identified a statistically significant positive correlation between active distraction and the risk of loosened footplates. The test for moderators was statistically significant (QM = 4.70, df = 1, P = .03) and the regression coefficient (β = 0.16, 95% CI: .015-0.299; OR = 1.17; SE = .07; z = 2.17; P = .03) indicated that longer active distraction durations were independently associated with an increased likelihood of footplate loosening. In practical terms, for every additional day of active distraction, the odds of footplate loosening increase by ∼ 17% (Figure 4A).
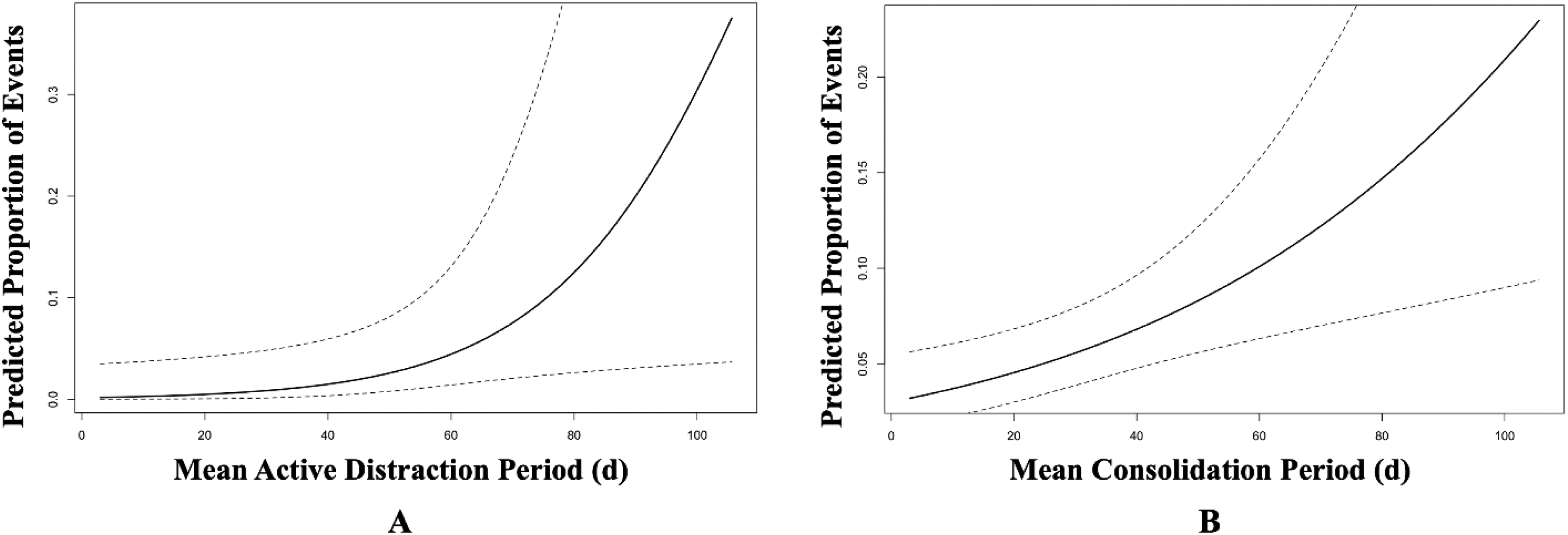
(A) Predicted probability of loosened footplates as a function of the mean active distraction period, based on mixed-effects meta-regression. The model identifies a statistically significant positive association (β = .16, 95% CI: .015-.299; OR = 1.17; SE = .07; z = 2.17; P = .03), indicating that each additional day of active distraction increases the odds of footplate loosening by approximately 17%. (B) Predicted Probability of External Activation Port Breakage as a Function of the Mean Consolidation Period, Based on Mixed-Effects Meta-Regression. The expected risk increases steadily with longer consolidation periods, reflecting a statistically significant association between the consolidation period and mechanical failure due to broken external activation ports (β = .0097, 95% CI: .0034-.0162; OR = 1.00985; SE = .0033; z = 3.01; P = .003). The model indicates that even modest extensions of the consolidation period could lead to a measurable increase in the risk of external activation port breakage.
A similar pattern was identified between the consolidation period and the risk of broken external activation ports. The duration of the consolidation phase emerges as an independent statistically significant predictor of broken external activation ports (QM = 8.9, df = 1, P = .003). The positive regression coefficient (β = .0097, 95% CI: .0034-.0162; OR = 1.00985; SE = .0033; z = 3.01; P = .003) indicated that each additional day in the consolidation phase was associated with 1% increased risk of external activation port breakage (Figure 4B). Together, these findings imply a temporal vulnerability in the mechanical integrity of the distraction system, whereby prolonged active distraction and consolidation phases may progressively compromise the hardware's structural stability.
Discussion
In this systematic review and proportional meta-analysis, we examined the clinical and mechanical burden associated with external activation ports in children who underwent PCVDO for complex craniosynostosis using externalized subcutaneous craniofacial distraction systems. We found that approximately 28% experienced an adverse event at some point during the course of distraction, with wound infection emerging as the most commonly reported adverse event. Although many patients with wound infection were managed conservatively using local wound care and IV antibiotics, almost half of these patients required surgical intervention. Moreover, 3 out of every 10 patients with wound infection required premature removal of the distraction system, underscoring the clinical burden of soft tissue morbidity associated with external activation ports. Similarly, mechanical failure attributable to either loosened footplates or broken external activation ports accounted for 35.7% of all adverse events. Interestingly, four out of every 10 patients with mechanical failure required surgical intervention, either to adjust loosened footplates under general anesthesia or to prematurely remove the distraction system and abort the distraction process.
The meta-regression analysis identified two temporal risk factors with serious mechanistic implications. The likelihood of footplate loosening increased by approximately 17% for each additional day of active distraction, indicating cumulative cyclic loading at the bone-device interface. Similarly, the risk of breakage of external activation ports was directly proportional to the length of the consolidation period. Together, these findings place surgeons in an inherent paradox. On the surface, one might infer that accelerating distraction protocols, transitioning, for instance, from 0.5 mm twice daily to 2 mm once a day, could reduce the exposure of the hardware to the repetitive, cyclic mechanical loading and thereby mitigate the risk of these mechanical complications. However, the biomechanics of distraction osteogenesis do not support this intuitive solution. Slow distraction protocols—typically 0.5 mm once or twice a day—offer substantial mechanical and biological advantages over accelerated distraction protocols (eg, 2 mm/day).36–43
Mechanically, smaller increments minimize viscous resistance within the surrounding soft tissues, allowing a greater portion of the applied torque to translate into effective tensile strain within the regenerate across the distraction gap rather than being dissipated as energy loss. Since viscoelastic damping scales with distraction velocity, fast distraction produces disproportionately elevated torque spikes and higher peak forces, increasing the risk of loading stress, footplate loosening, and subsequently mechanical failure.25,44–47 Experimental torque-force measurements support this principle: even a modest acceleration from 0.5 mm to 0.75 mm increases torque requirements by ∼15-20%, demonstrating the steep energetic penalty of elevated distraction velocities. 39 In contrast, slower rhythmic increments generate smoother activation profiles, lower peak forces, and more predictable mechanical control.
Biologically, slow distraction better preserves the osteogenic strain window required for optimal bone formation. Smaller, more frequent increments (1) maintain tensile strains within the optimal 2-10% daily range of the osteogenic strain window, (2) activate YAP/TAZ, and (3) sustain osteoprogenitor proliferation. 48 Slower distraction also permits viscoelastic relaxation between sessions, reducing cumulative tissue stress and supporting coordinated remodeling of muscle, periosteum, and vascular networks—an essential prerequisite for high-quality bone formation in craniofacial regions where soft-tissue constraints are inevitable. In contrast, high-velocity distraction (>15-20% strain/day) risks exceeding tissue tolerance, disrupting angiogenesis, and favoring fibrous or fibrocartilaginous tissue formation. 49
Paradoxically, therefore, ultra-fast distraction protocols intensify—rather than alleviate—the very mechanical failure modes surgeons seek to avoid. The conflict between statistically significant temporal risk factors—prolonged active distraction and consolidation periods—and mechanobiological constraints highlights a fundamental clinical dilemma: prolonged active distraction and consolidation periods increase cumulative loading stress on the distraction system, yet accelerating distraction protocols destabilizes the mechanobiological environment required for optimal bone formation. The solution, therefore, cannot be found in simply adjusting the distraction rate, but instead demands device design innovation and protocol adjustment grounded in mechanistic and biological understanding rather than intuition.
The Mechanical Impact of External Activation Ports
In addition to their clinical implications, external activation ports also pose serious mechanical challenges. Precise intraoperative alignment of the distraction system with the sagittal axis is essential for achieving the desired distraction and optimal bone formation, both in quality and quantity. When the distraction system is oriented such that
When external activation ports are not perfectly coaxial with the intended distraction vector, the distraction system could be rotated or translated to accommodate skin exit. This introduces an effective orientation angle (
Additionally, when the external activation ports exit the skin at a non-collinear angle to the body of the distraction system, each activation session generates off-axis torque due to skin drag, port bending, or asymmetric cutaneous tension. Notably, these forces are transmitted to the footplates as torsional moments and lateral bending loads.53,54 Such torsional loading disrupts pure translational mechanics, causing micro-rotations around hinge lines near the skull base or mandibular ramus. In cranial vault distraction, this may lead to anterosuperior or posterolateral rotational drift, whereas in mandibular distraction, it contributes to anterior open bite, segmental divergence, or condylar displacement—all reported consequences of imperfect vector control.50–52,55 Thus, even if the distractor is initially placed with meticulous alignment, soft-tissue-mediated off-axis torques during activation gradually degrade mechanical precision.
These disadvantages are further magnified in multi-vector distraction systems, where symmetric distraction of paired devices is required for stability. Asymmetry in external activation port position—whether in trajectory, skin tension, or ease of access—results in unequal lateral force components and divergent rotational couples between devices. Over the course of distraction, the cumulative effect of small inter-device asymmetries leads to rotational drift and substantial deviations from planned trajectories.50,56
These externally activated distraction systems are therefore constrained by fundamental geometric issues: the distractor must orient itself to satisfy both (1) the planned biomechanical vector and (2) the external skin-level port geometry. Because the latter cannot be optimized due to soft-tissue thickness, neurovascular proximity, or scarring, surgeons are often forced to improvise, which may compromise biomechanical optimality. Even with virtual surgical planning, the mechanical disadvantages of external activation ports remain, as any intraoperative or postoperative deviation—throughout the course of distraction—from coaxial alignment transforms a uniaxial distraction system into a combined loading device, delivering axial tension, lateral shear, and torsional moment simultaneously.
Study Limitations
Despite the use of rigorous methodological approaches in designing and executing this systematic review and proportional meta-analysis, several limitations must be acknowledged when interpreting the findings.
Conclusion
In this study, we found that approximately one in four children undergoing PCVDO experiences at least one adverse event during the course of distraction, with wound infection representing the most frequent complication. Mechanical failures constituted more than one-third of all adverse events. These complications often necessitated surgical intervention: four out of every ten patients with mechanical failure required either intraoperative adjustment under general anesthesia or early termination of distraction and premature removal of the distraction system. Such findings underscore that mechanical reliability remains a major vulnerability of the current distraction systems.
The mechanical analysis presented in this study demonstrated that the current externalized subcutaneous craniofacial distraction systems impose geometric compromises that may potentially degrade alignment fidelity and distort force transmission. Even when osteotomies are meticulously executed and planned vectors are precise, the external activation ports themselves may predispose off-axis loading, bending moments, and frictional torque, all of which accumulate over the course of distraction, eroding mechanical accuracy and diminishing regenerate's quality.
These limitations highlight that accurate vector control will remain unattainable as long as external, skin-traversing activation ports remain integral to distraction system functionality. Future studies should focus on innovation in distraction system design. A shift toward a fully internalized, port-free actuation—magnetic actuation, for instance—would potentially contribute to reduced risk of wound infection, misalignment, and mechanical failure. Such systems would allow distractor placement to be dictated solely by biomechanical principles rather than by percutaneous accessibility, restoring the ability to maintain strict collinearity with the planned vector, minimizing parasitic shear, and creating a more uniform and osteogenic strain environment. Eliminating the need for external activation ports is therefore not a minor refinement but a major design innovation. By decoupling actuation from external geometry, next-generation distraction systems have the potential to improve mechanical precision, reduce complication rates, enhance patient comfort, and ultimately deliver higher-quality bone regeneration and better clinical and morphological outcomes. The future of distraction osteogenesis depends not only on refinements in surgical technique or postoperative management but on the development of distraction systems whose mechanics consistently support—rather than undermine—the biological principles that drive successful bone formation.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261460851 - Supplemental material for The Negative Impact of External Activation Ports on Cranial Distraction: Systematic Review of the Literature and Proportional Meta-Analysis
Supplemental material, sj-docx-1-cpc-10.1177_10556656261460851 for The Negative Impact of External Activation Ports on Cranial Distraction: Systematic Review of the Literature and Proportional Meta-Analysis by Mohammed A. Fouda, David Dostal and Caitlin E. Hoffman in The Cleft Palate Craniofacial Journal
Footnotes
Human Ethics and Consent to Participate Declarations
Not applicable.
Authors Contributions
All authors contributed to the conception and design of the study. MAF and DD performed material preparation, data collection, and analysis. MAF wrote the first draft of the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical Trial Number
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.