
Abstract
Objective
To examine relationships between Psychosocial Assessment Tool-Craniofacial Version (PAT-CV) scores and patient demographic and clinical characteristics; to evaluate changes in PAT-CV scores over time.
Design
Retrospective chart review.
Setting
US pediatric academic medical center.
Participants
Caregivers of 1323 children (mean age 6.78 ± 4.87 years, 54% male) with craniofacial conditions presenting for a team visit; 414 children had 2 consecutive visits, an average of 1.1 years apart.
Main Outcome Measures
PAT-CV scores.
Results
Cross-sectionally, higher PAT-CV total scores were associated with older child age, public insurance, craniofacial conditions other than cleft, and other chronic conditions (all P < .05). PAT-CV total scores were stable, with no significant differences for total scores and risk classification categories over about a year.
Conclusions
Demographic and clinical characteristics were significantly related to PAT-CV scores at baseline, and scores were stable over a 1-year period. Craniofacial psychosocial screening can be informed by identified risk factors within universal screening.
Introduction
Craniofacial conditions are associated with psychosocial risks, including anxiety, depression, learning disabilities, and social stigmatization related to speech and/or appearance differences.1–4 Families also face stressors related to accessing care for their children, such as financial costs, time away from work for medical appointments, and emotional distress.5,6 In recognition of these psychosocial challenges, interdisciplinary care is recommended for craniofacial conditions, 7 which ideally includes routine screening for emotional, social, and behavioral concerns, and family adjustment and coping. However, few assessment tools exist to systematically screen for psychosocial risks specific to craniofacial populations.
In recent years, a craniofacial version of the Psychosocial Assessment Tool (PAT), a reliable and valid screening instrument used across many pediatric conditions, 8 was developed and validated for use in craniofacial populations.9,10 This measure can be used to identify risks related to child, sibling, and caregiver mental health, craniofacial-specific risks (eg, speech problems, teasing), family resource needs, social support, and caregiver beliefs about the child's medical condition and related care. 9
The development and validation of the PAT Craniofacial Version (PAT-CV) were important steps towards improving risk screening in craniofacial clinics using a standardized approach. A recent quality improvement (QI) study that involved integration of the PAT-CV into the screening protocol for a high-volume cleft and craniofacial team observed improvements in psychosocial risk identification for families presenting for annual team evaluations. 11 Further, use of the PAT-CV helped to increase the percentage of at-risk families who received a consultation with the team's social workers and/or psychologists from 72% to 90%. 11
Currently, little is known about relationships between demographic and clinical characteristics and PAT-CV scores. A cross-sectional study observed that PAT-CV scores varied significantly by insurance type and syndromic versus non-syndromic diagnosis in a sample of 217 children with craniofacial conditions. 10 However, this study was limited by its sample size and potential selection bias, as families were participants in validating the PAT-CV. There remains limited data about how PAT-CV scores vary by demographic and clinical characteristics or changes over time. This information is needed to further refine and evaluate screening practices and risk assessment in craniofacial clinics.
The present study was designed to address these gaps by (1) cross-sectionally examining relationships between PAT-CV psychosocial risk scores and patient demographic and clinical characteristics in a large sample; and (2) evaluating changes in PAT-CV risk scores and factors associated with change over time.
Method
This study utilized data from a QI project including PAT-CV administration to consecutive patients seen for an interdisciplinary visit at a US-based academic medical center's cleft and craniofacial team between 8/1/2017 and 12/31/2019. 11 IRB approval was obtained to retrospectively review medical charts to collect demographic and clinical data. Inclusion criteria were: (1) the patient was <18 years at the time of their clinic visit; (2) the patient had been diagnosed with a congenital craniofacial condition; and (3) the patient had a caregiver complete a PAT-CV as part of a cleft/craniofacial team visit. Patients were excluded if they were not being seen for a team visit (eg, post-operative appointment with the surgeon only); their parent and/or guardian could not complete a PAT-CV form in English (the PAT-CV was only available in English at the time of the QI project); or if they declined to complete the PAT-CV. Chart reviews were conducted using a Research Electronic Data Capture System (REDCap) 12 data abstraction form by 2 trained research assistants under the supervision of the senior author. Information about the team's triage procedures for psychology and social work consultations has been previously described. 11
Variables of Interest
PAT-CV Total and Subscale Scores
The PAT-CV is a concise tool that relies on caregiver input to screen for psychosocial risk. The PAT-CV generates a total score and subscale scores corresponding to risks in the following domains: (1) Family Structure and Resources (eg, caregiver marital, education, and employment status; endorsement of financial or transportation problems); (2) Caregiver Problems (eg, experiencing legal, mental health, or other stressors); (3) Social Support (eg, access to emotional, financial, or other supports); (4) Child Problems (eg, child worries or problems with development/learning); (5) Sibling Problems (eg, sibling(s) mental health/developmental concerns); (6) Child Problems due to their Craniofacial Condition (eg, speech difficulties, teasing); (7) Caregiver Confidence (eg, confidence in ability to cope with the child's condition/care); and (8) Caregiver Beliefs about Child's Condition (eg, does the caregiver blame themselves for the child's craniofacial condition). 9 PAT-CV subscale item scores are averaged and range from 0 to 1 with higher scores reflecting greater risk. Total scores range from 0 to 8 and are generated from subscale scores. Total scores classify psychosocial risk into: (1) Universal (0 to <1.00), indicating no identified risks for poor coping or adaptation to the child's condition/care; (2) Targeted (1.00-1.99), where the family has at least one risk factor that could warrant monitoring or intervention in one domain; and (3) Clinical (≥2.00), indicating the presence of several risk factors across domains requiring more intensive support and interventions. The PAT-CV has good criterion and construct validity along with acceptable test-retest reliability and internal consistency. 9
Demographic and Clinical Variables
Data abstracted from the electronic health record included the child's craniofacial diagnosis (eg, cleft palate, craniosynostosis); other chronic medical conditions (eg, chronic otitis media, scoliosis, asthma, congenital heart defects, obesity, diabetes); psychological diagnoses (eg, anxiety, depression, attention deficit-hyperactivity disorder); insurance type (eg, employer-sponsored or private insurance; government-sponsored insurance such as Medicaid); race; and ethnicity. Craniofacial team visit characteristics such as whether a patient was scheduled to receive a psychology and/or social work consult at their team visit were also abstracted from clinic schedules and/or medical charts.
Study Sample
A total of 1400 children had craniofacial team visits within the specified time frame. Seventy-seven patients were excluded from analysis as they did not meet eligibility criteria (n = 44) or had missing data on the PAT-CV (n = 33). Eligible patients who had at least one team visit during the study period and who had a completed and scorable PAT-CV were included in the cross-sectional analysis (N = 1323). A subgroup of children (n = 414) with a second team visit within the specified time frame were included in the longitudinal analysis.
Analyses
Patient demographic and clinical characteristics and PAT-CV total and subscale scores were examined descriptively (eg, means, frequencies).
Cross-sectional Analyses
Pearson correlations were run to describe bivariate linear relationships between study variables. Bivariate correlations examined relationships between PAT-CV total scores and scheduled social work and psychology consultations. Multivariable generalized linear regression analyses described the effect of demographic and clinical variables (ie, patient age, sex, race, health insurance, craniofacial diagnosis, other health conditions, and psychological diagnoses) on PAT-CV total and subscale scores. The beta (β) values for specific variables from significant regression analyses were reported.
Longitudinal Analyses
Paired t-tests and Chi-square analyses were used to examine changes in PAT-CV scores (for continuous and categorical risk scores, respectively) between assessments for patients who had 2 visits within the study period.
Results
Cross-sectional Sample
The mean age of children in the cross-sectional sample was 6.78 ± 4.87 years and 54.12% were male (n = 716). Most of the sample were White (78.76%), and 611 (46.18%) participants had a cleft lip and/or palate diagnosis (Table 1). Most patients (84.81%) had other chronic medical conditions (eg, chronic otitis media with effusion, gastroesophageal reflux, asthma, club foot), and 36.21% (n = 479) had a documented psychological diagnosis (eg, anxiety, depression) in their medical chart (Table 1).
Cross-Sectional Sample Demographic and Clinical Characteristics (N = 1323).
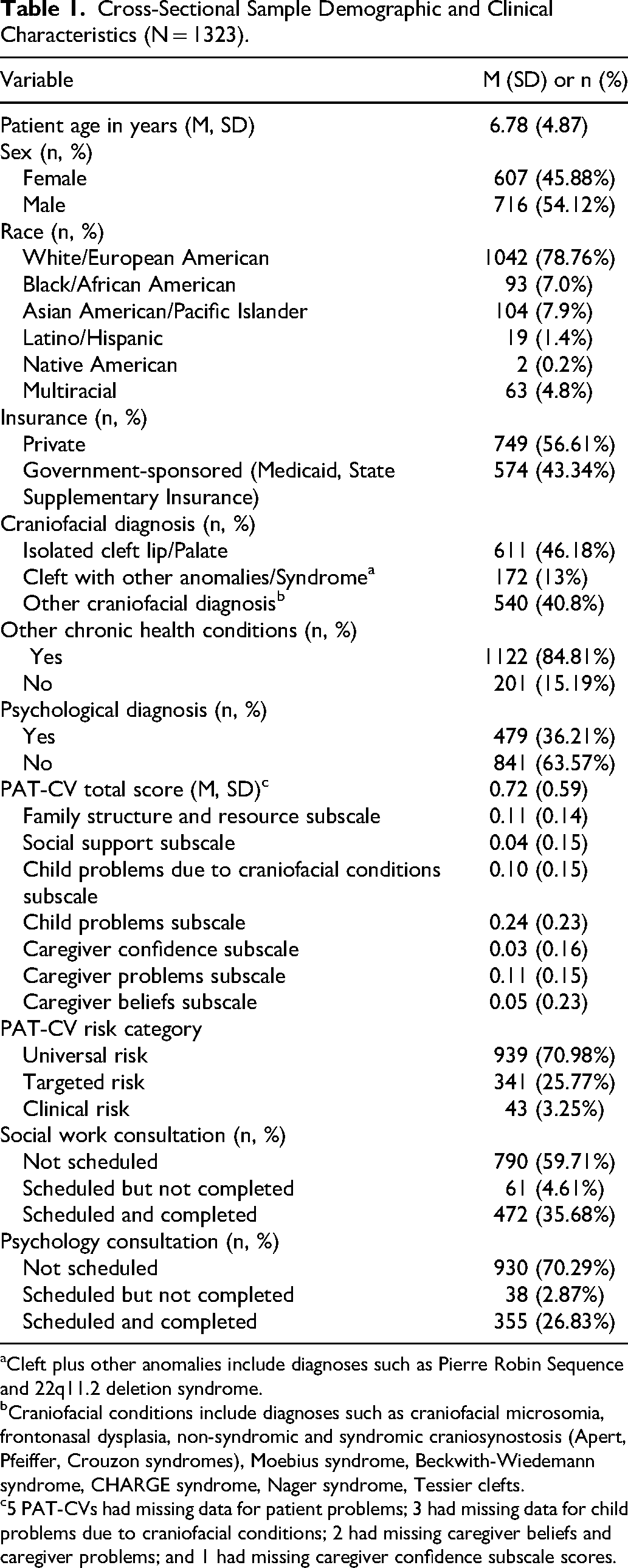
Cleft plus other anomalies include diagnoses such as Pierre Robin Sequence and 22q11.2 deletion syndrome.
Craniofacial conditions include diagnoses such as craniofacial microsomia, frontonasal dysplasia, non-syndromic and syndromic craniosynostosis (Apert, Pfeiffer, Crouzon syndromes), Moebius syndrome, Beckwith-Wiedemann syndrome, CHARGE syndrome, Nager syndrome, Tessier clefts.
5 PAT-CVs had missing data for patient problems; 3 had missing data for child problems due to craniofacial conditions; 2 had missing caregiver beliefs and caregiver problems; and 1 had missing caregiver confidence subscale scores.
The mean PAT-CV total score was 0.72 ± 0.59, with 70.98% of participants (n = 939) having scores classified as within the universal risk range, with 25.77% (n = 341) and 3.21% (n = 43) within the targeted and clinical risk ranges, respectively. The Child Problems subscale had the highest score, indicative of greater risks in this domain relative to other subscales (see Table 1).
Table 1 presents the number of patients for whom social work and/or psychology consultations were scheduled prior to the child's team visit. Significant bivariate correlations between PAT-CV total scores and scheduled social work (r = 0.34, P < .001) and psychology consultations (r = 0.46, P < .001) were observed, such that PAT-CV scores indicative of greater psychosocial risk were associated with having scheduled (vs unscheduled) psychosocial consultations.
Cross-sectional Relationships between Demographic and Clinical Characteristics and PAT-CV Scores
Table 2 includes correlations between PAT-CV scores and demographic and clinical characteristics to show linear relationships between individual study variables. The multiple regression analyses identified several significant relationships (Table 2). Older child age was significantly associated with higher PAT-CV total scores (β = 0.11, P < .0001) and higher Social Support, Child Problems due to Craniofacial Condition, Child Problems, and Caregiver Confidence subscale scores. A higher PAT-CV total score was also associated with the presence of other chronic medical conditions (β = 0.18, P = .01). Other chronic medical conditions were significantly associated with higher scores on the Child Problems due to Craniofacial Condition and Child Problems subscales and significantly lower Caregiver Belief subscale scores (β = −0.20, P = .01) (see Table 2). Private health insurance was associated with lower PAT-CV total scores (β = −0.45, P < .0001) and significantly lower subscale scores (Table 2), except for the Caregiver Beliefs subscale. Having a craniofacial diagnosis other than isolated cleft (eg, syndromic and non-syndromic craniosynostosis) was associated with higher PAT-CV total scores (β = 0.11, P = .03), Child Problems due to their Craniofacial Condition (β = 0.32, P < .0001), and Child Problems (β = 0.16, P = .002) subscale scores. The presence of a psychological diagnosis was also associated with higher PAT-CV total scores (β = 0.73, P < .0001), along with higher scores for the Family Structure and Resources, Child Problems due to Craniofacial Conditions, Child Problems, and Caregiver Problems subscales (Table 2).
Associations Between Demographic and Clinical Characteristics and PAT-CV Total and Subscale Scores (N = 1323).
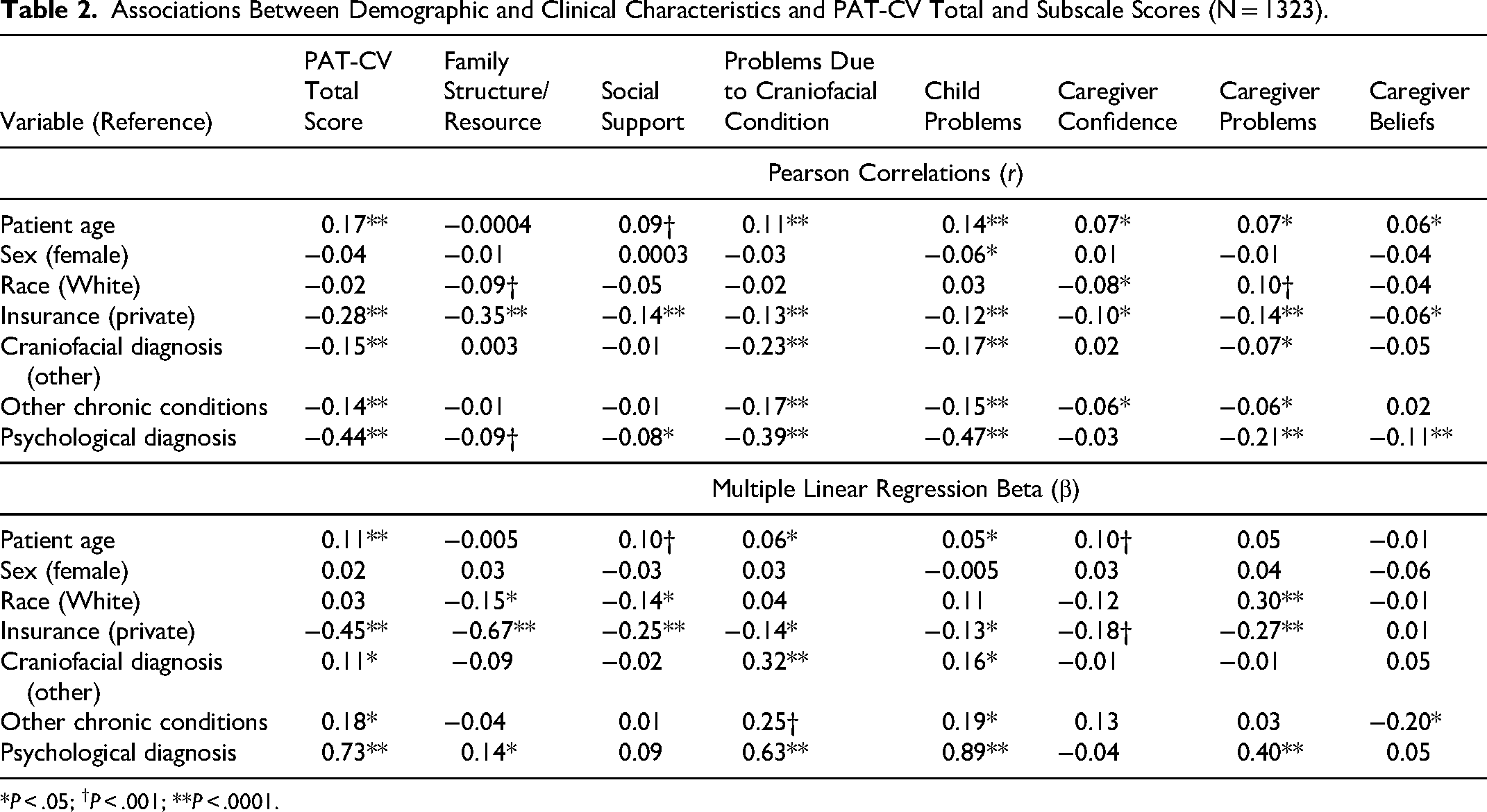
*P < .05; †P < .001; **P < .0001.
Longitudinal Sample
The average time between 2 consecutive PAT-CV administrations for 414 patients was 1.11 ± 0.31 years. About half of the sample was male (n = 211, 50.97%). Patients were primarily White (n = 299, 72.2%), had private insurance (n = 258, 62.3%), had a primary diagnosis of a cleft (n = 220, 53.1%), and the majority (n = 348, 84%) had an additional chronic health condition.
As shown in Table 3, the mean age at the baseline assessment for this cohort was 6.62 ± 4.44 versus 7.64 ± 4.50 years (P < .001) at the second assessment. There was no significant change in the mean PAT-CV total score of 0.63 ± 0.58 as compared to 0.67 ± 0.58 at the second visit (P = .30). Similarly, subscale scores including the Child Problems due to Craniofacial Conditions, Child Problems, Caregiver Confidence, and Caregiver Problems scores demonstrated small, non-significant increases from their baseline to the second visit assessment.
Longitudinal Cohort Characteristics by Time Point (N = 414).
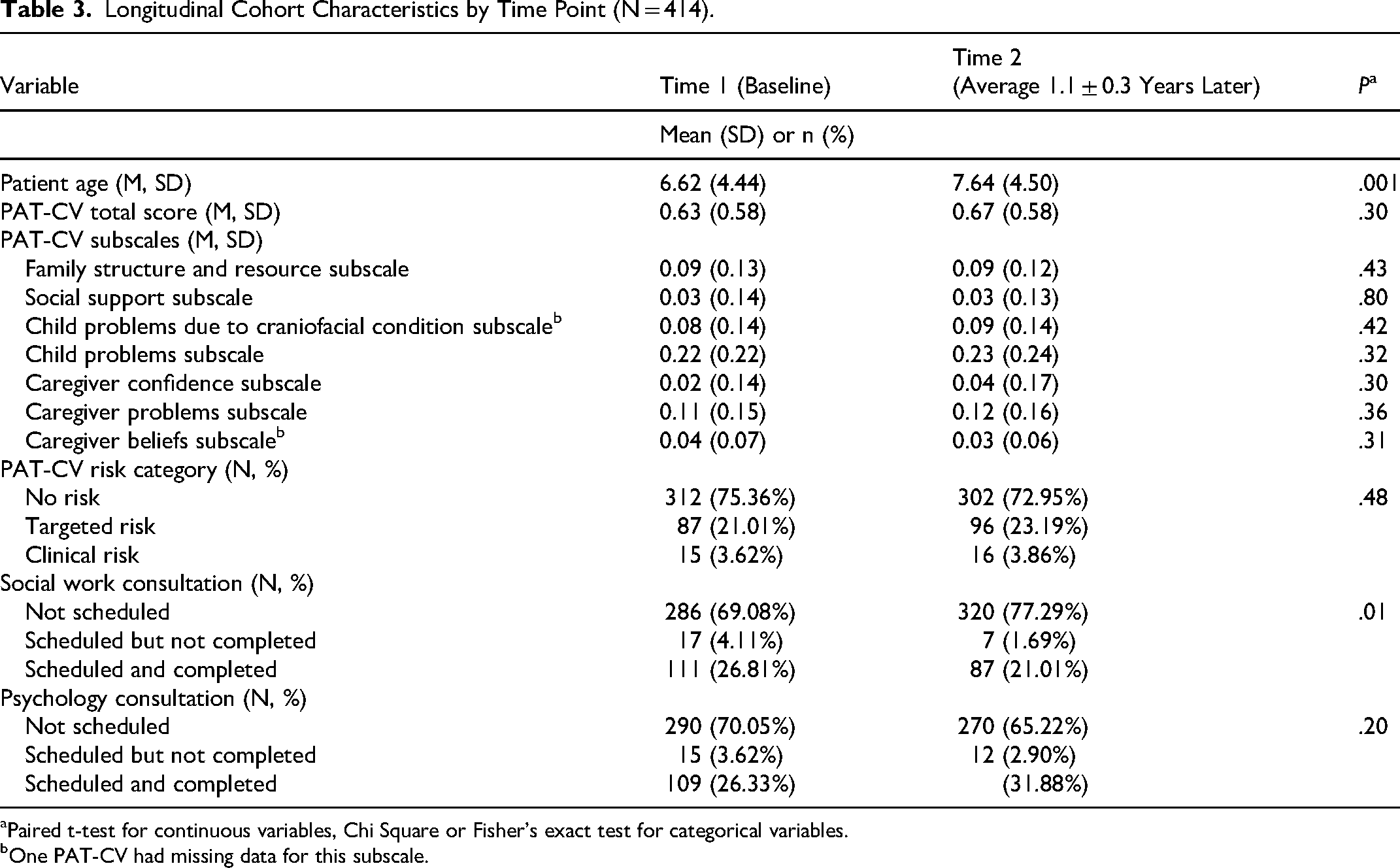
Paired t-test for continuous variables, Chi Square or Fisher's exact test for categorical variables.
One PAT-CV had missing data for this subscale.
Small changes in the percentages of PAT-CV total scores classified as Universal, Targeted, and Clinical were observed from baseline to the second visit. There was a decrease in the number of scores falling within the Universal risk range (75% to 72%), with correspondingly small increases noted for the Targeted (21% to 23.2%) and Clinical risk groups (3.6% to 3.8%). However, these differences were not statistically significant (Table 3). Due to the small, non-significant changes in both continuous and categorical PAT-CV scores across the 2 assessments, demographic and clinical characteristics were not examined as predictors of change.
Discussion
This study evaluated PAT-CV scores cross-sectionally and longitudinally using a large sample of children attending craniofacial team visits within a US-based pediatric academic medical center. Cross-sectionally, older child age, craniofacial diagnosis other than a cleft, having other chronic medical conditions or psychological diagnoses, and public insurance were significantly related to higher PAT-CV total scores. Total PAT-CV and categorical risk scores remained stable over an average of a year, with no significant differences observed in total PAT-CV scores or changes in categorical risk levels over time.
Our findings are consistent with a prior study of the PAT-CV conducted at this institution. Kapa et al. 10 observed in their sample of 242 caregivers of 217 children with craniofacial conditions that PAT-CV scores varied significantly by type of insurance and craniofacial diagnosis. Similarly, families with past social work or behavioral health consults had higher PAT-CV scores than those without consultations. The current study, which included a larger sample of consecutive families presenting for craniofacial care (rather than a smaller group consenting to participate in research), appears to confirm these findings, including significant associations between PAT-CV total scores and scheduled psychology and social work consultations.
The present study also observed that higher PAT-CV scores were associated with older child age and the presence of other health and psychological comorbidities. Regarding age, as children grow and develop, the impacts of their craniofacial condition may become more evident as they navigate social situations, school, and the need for additional treatment and interventions. Families of children with craniofacial conditions other than cleft (including those with syndromes) or other medical and/or psychological comorbidities may have additional treatment-related burdens and stressors which could be reflected in higher PAT-CV scores. Prior studies have documented that having other health or psychological conditions can affect psychosocial outcomes, including risks for reduced quality of life, anxiety, and depression in cleft and craniofacial populations. 13
While our results point towards some significant associations between clinical and demographic factors and psychosocial risk cross-sectionally, in the broader literature, findings appear to be mixed. Verma et al. 14 did not identify clinical or demographic factors as significant predictors of risk scores in a sample of families of children with complex medical conditions. In contrast, Hearps et al. 15 observed significant relationships between parental education and PAT scores. Similar to our findings, a study of families of children with cystic fibrosis reported significant associations between higher PAT scores and public insurance and lower levels of parental education, with lower PAT scores associated with private health insurance. 16 In craniofacial populations, clinical and demographic factors appear to have some influence on psychosocial risk scores. However, no single characteristic may be sufficient to reliably identify patients at greatest risk, thus underscoring the need for psychometrically sound screening instruments like the PAT-CV.
Overall, we observed that more families in the current study had PAT-CV scores in the universal risk range relative to a prior investigation (∼71% vs 60%), 9 although the distribution of families falling within risk categories was similar (eg, the majority had universal risk scores). It is likely that the PAT-CV risk rates reported here are more representative of actual risk levels given the larger sample size and reduced risks for selection bias as we used data for consecutive patients seen over a 2-year period.
Longitudinally, PAT-CV scores were largely stable over an average of a year, with no significant differences in total or subscale scores or changes in categorical risk observed. No other published studies have examined PAT-CV score stability and change over time. Our findings are consistent with studies of PAT score change in other pediatric populations.17,18 For example, a study of children and adolescents with newly diagnosed cancer reported no significant differences in PAT risk levels over a 6-month interval, and 63% of families had scores within the same risk level at their follow-up assessment. 17 Consistent with our findings, there was a small percentage of families who experienced changes in categorical risk level over time. Collectively, these findings suggest that while most families’ risk levels are stable within about a year or less, the optimal interval between psychosocial risk screening requires further evaluation.
The relative stability of PAT-CV scores observed in this study reflects how this instrument is designed to assess several characteristics which may be less likely to change over a 12-month period (eg, family structure). Some variation is likely on the PAT's individual items and total scores, with expected stability for overall risk score classifications. 19 This study's findings suggest that the PAT-CV performs within expectations and demonstrate its utility for identifying families who may benefit from regular contact with psychosocial providers.
Limitations
While data reported here are from a large sample, they were collected at a single craniofacial center. Further, large sample sizes facilitate detection of small differences, which may have less clinical significance. Replication of our findings in other settings is warranted. The PAT-CV was available only in English at the time this study was conducted. As a result, non-English-speaking caregivers and, relatedly, psychosocial risk scores for families from linguistically diverse backgrounds, are not represented in this sample. Higher risk levels on the PAT have been observed among Spanish-speaking families in other populations, 8 underscoring the need for a Spanish version of the PAT-CV. While scores remained relatively stable over a period of approximately 1 year, it remains unknown how scores vary over longer time periods. On average, children in this study were 6 to 7 years of age. Given that craniofacial care typically spans infancy through early adulthood, future studies are needed to understand how psychosocial risk changes over time, across and within developmental stages, and in response to interventions that may lessen overall risk (eg, mental health treatment). Finally, data were derived from an existing dataset that did not include PAT-CV item-level data, including caregiver characteristics (sex, marital status, age).
Clinical Implications
Results from this study underscore the need for routine risk assessments, particularly for older children with non-cleft craniofacial conditions. Our findings support the need for routine monitoring of psychosocial risk in children with cleft and craniofacial conditions, particularly as they age through childhood and adolescence. Screening practices and access to social work and mental health providers vary widely across teams, and some may not routinely utilize formal screeners such as the PAT-CV. This study highlights clinical and demographic factors associated with higher psychosocial risk that may aid in triage practices and identification of families who may benefit from psychosocial services. Regardless, in line with the ACPA Parameters of Care, 7 screening is recommended to begin in infancy and continue throughout young adulthood for all patients and their families. While this study demonstrated some stability in risk scores, ongoing monitoring is indicated, particularly as children and their families may encounter additional condition-related impacts over longer periods of time.
Conclusions
Demographic and clinical characteristics including age, diagnosis, and insurance were significantly related to PAT-CV scores at baseline, although scores appear to be stable over a year. These findings imply that risk assessment and psychosocial service provision within the context of craniofacial care should establish procedures for routine screening during childhood and adolescence with a particular focus on children with syndromes or other medical complexity. A better understanding of these relationships can improve triage processes for psychosocial consultations and inform craniofacial team psychosocial service delivery.
Footnotes
Acknowledgments
We extend our gratitude to Adrienne Moetenalo and Meghan O’Brien who assisted with data collection, and Dr. Josh Bricker for his assistance with supplemental analyses.
Author's Note
Preliminary results from this project were presented during the 79th Annual Meeting of the American Cleft Palate Craniofacial Association, Ft. Worth, TX.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.