
Abstract
Objective
To systematically evaluate reported nasal morphological changes following Le Fort I osteotomy in individuals with cleft lip and palate (CLP).
Design
Systematic review.
Setting
Not applicable.
Participants
Adolescents (>16 years) and adults with nonsyndromic CLP undergoing maxillary orthognathic surgery.
Interventions
Le Fort I osteotomy, performed either in isolation or in combination with bilateral sagittal split osteotomy.
Main Outcome Measures
Postoperative nasal morphological changes, including alar base width, nasal tip projection, nasal length, and nasolabial angle. Additional synthesized outcomes included alar symmetry and soft tissue response ratios when available.
Results
Eight observational studies (one prospective, one cross-sectional, and six retrospective), including 201 individuals with CLP, were analyzed. Risk of bias was high in five studies and moderate in three. Across heterogeneous study designs and assessment methods, Le Fort I osteotomy was associated with improvements in alar symmetry and increases in the nasolabial angle (up to +16.0°). Alar widening (up to 3.0 mm) and variable changes in nasal tip projection, ranging from −2.22 to +2.40 mm, were also reported. Soft tissue responses varied substantially, with the nasal base following approximately 55% to 57% of maxillary advancement, nasal tip response ranging from −0.36 to +0.28 mm/mm of maxillary advancement, and nasolabial angle changes reaching 2.61° per millimeter of advancement.
Conclusions
Le Fort I osteotomy is associated with postoperative nasal morphological changes in individuals with CLP. Improvements in alar symmetry and nasolabial angle were reported, although alar widening and variable changes in nasal tip projection and nasal length were also observed. Given methodological heterogeneity and moderate-to-high risk of bias, findings should be interpreted cautiously.
Introduction
Le Fort I osteotomy is the gold standard procedure for correcting maxillary hypoplasia in patients with cleft lip and palate (CLP), aiming to restore both occlusal function and facial harmony. 1 However, maxillary repositioning can induce significant and sometimes undesirable secondary changes in nasal morphology, affecting tip projection, alar base width, nasolabial angle, and nostril exposure.2–4 These changes occur due to the close anatomical interdependence between the maxilla, which serves as the structural base for the nose, and the overlying soft tissues. 5
The response of soft tissues to maxillary movements is complex, 3-dimensional (3D), and multifactorial, and is influenced by the magnitude and direction of bone displacement, tissue thickness and tonicity, as well as patient-related factors such as age and ethnicity.6–8 Recent systematic reviews have evaluated nasolabial soft tissue changes after Le Fort I osteotomy using 3D analysis methods, such as stereophotogrammetry and cone-beam computed tomography (CBCT), improving understanding of postoperative tissue response in noncleft populations. However, the available evidence specifically addressing individuals with CLP remains limited and methodologically heterogeneous.9–11
In this context, a systematic review dedicated to this specific population becomes necessary, since the presence of scar tissue and fibrosis resulting from primary surgeries substantially alters the biomechanical behavior of soft tissues and skeletal stability, 12 and may enhance understanding of tissue behavior in these individuals, improve surgical planning, and guide future research using more standardized methodologies.
Therefore, this systematic review aimed to analyze the nasal changes resulting from Le Fort I osteotomy in individuals with CLP, while considering the evaluation methods used, surgical techniques, and the main aesthetic outcomes reported in the literature, including changes in alar base width, nasal tip projection, and nasolabial angle.
Methods
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines and registered in the PROSPERO database (CRD420261293481). 13 The search strategy was developed by the review team and peer-reviewed by an experienced researcher with expertise in systematic review methodology and search strategy design. Feedback from this review was incorporated into the final search syntax.
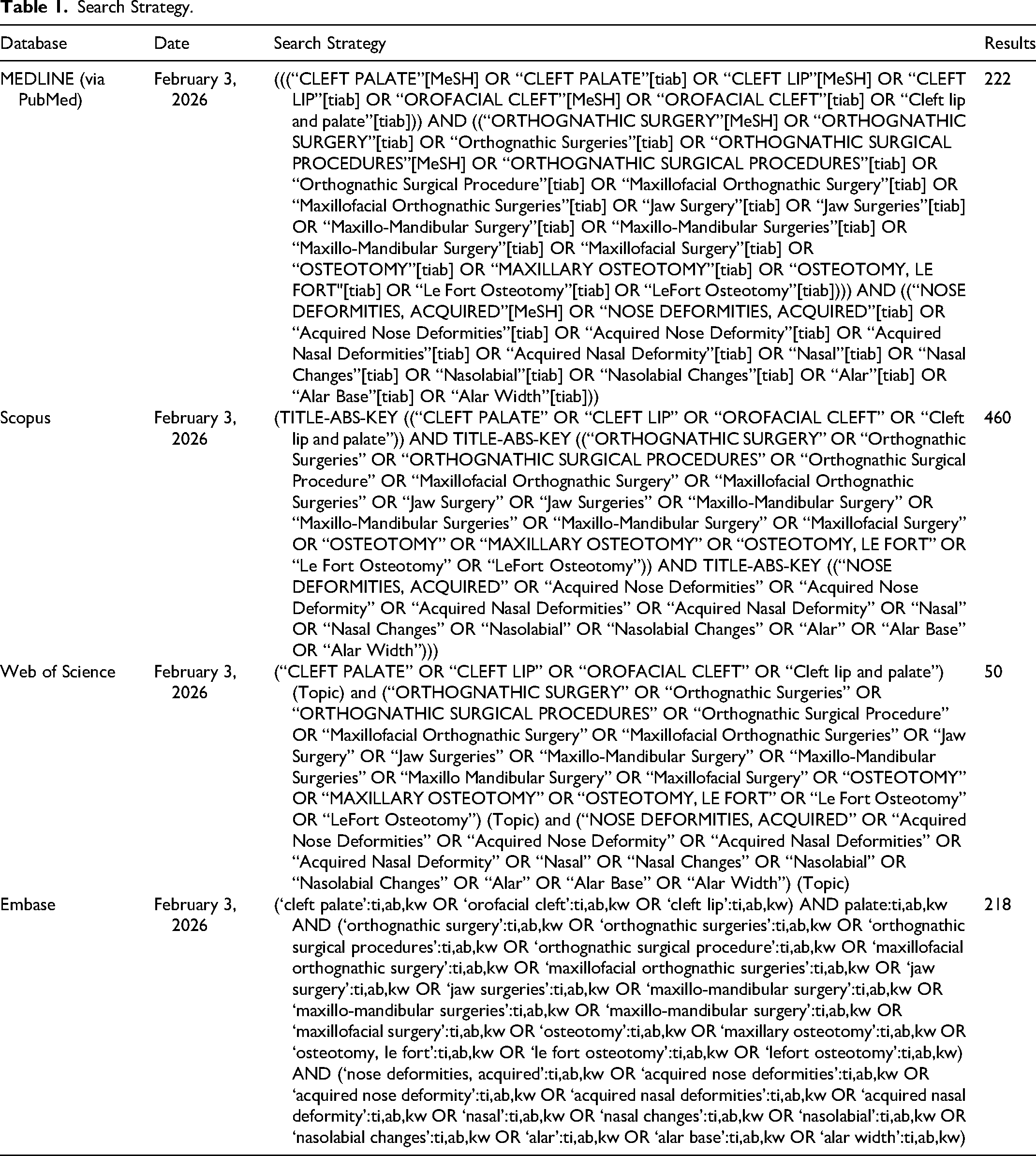
A highly sensitive, database-specific search strategy was developed to maximize the retrieval of potentially eligible studies and account for variability in terminology related to CLP, orthognathic surgery, and nasal morphological outcomes. Searches were conducted in the MEDLINE (via PubMed), Web of Science, Scopus, and Embase electronic databases until February 3, 2026. Full search syntaxes for each database are provided in Table 1 to ensure reproducibility.
Search Strategy.
The PICO strategy was defined as follows: population (P): adolescents and adults with nonsyndromic CLP; intervention (I): Le Fort I osteotomy; comparison (C): preoperative versus postoperative condition and/or comparison with noncleft controls when available; outcome (O): postoperative nasal morphological alterations, specifically changes in alar base width, nasal tip projection, nasal length, and nasolabial angle. Additional study-specific outcomes, including alar symmetry and side-specific soft tissue response ratios, were descriptively synthesized when available.
Search Strategy
The search strategies used in each database are presented in Table 1.
Selection of Studies
Study selection and data collection were performed by 2 independent reviewers (L.R.A.C. and C.P.O.G.). An initial screening of titles and abstracts was conducted to identify potentially eligible studies according to predefined inclusion criteria. Full-text articles were subsequently assessed for eligibility using the same criteria.
Eligibility criteria included: (1) studies involving individuals older than 16 years with nonsyndromic CLP; (2) randomized and nonrandomized clinical trials, cohort studies (prospective or retrospective), and case series with ≥15 participants; (3) mono- or bi-maxillary orthognathic surgery involving the maxilla; (4) evaluation of nasal soft tissue changes following Le Fort I osteotomy; (5) use of 2-dimensional (2D) or 3D soft tissue analysis methods; (6) reporting of quantitative data on soft tissue response to skeletal movement; and (7) minimum follow-up of 6 months.
For the purpose of this review, “objective data” were defined as quantitative, measurable outcomes derived from imaging-based or anthropometric assessments. This included linear, angular, surface, or volumetric measurements of nasal morphology obtained through 2D cephalometry, 3D stereophotogrammetry, laser scanning, or CBCT, as well as calculated soft tissue response ratios relative to skeletal movement.
Disagreements at any stage of study selection were resolved through discussion and consensus. When consensus could not be reached, a third senior reviewer (R.Y.F.Y.) made the final decision.
A manual search of the reference lists of included studies was performed to identify additional eligible articles not captured by the electronic search.
The review was conducted in accordance with the registered PROSPERO protocol (CRD420261293481). Any protocol amendments were documented; however, no major deviations affecting eligibility criteria, outcomes, or synthesis methods were introduced during the review process.
Data Collection
The information extracted from the selected studies was organized into summary tables (Tables 2-4). Two reviewers (L.R.A.C. and C.P.O.G.) independently extracted study-level data, including demographic and clinical characteristics (sample size, age, sex distribution, cleft phenotype, and dentofacial deformity), methodological characteristics (study design, imaging modality, image registration protocol, software used, and follow-up duration), surgical variables (type of orthognathic procedure, magnitude and direction of maxillary movement, and adjunctive procedures such as alar cinch, V-Y closure, and anterior nasal spine [ANS] management), and postoperative nasal morphological outcomes (alar base width, nasal tip projection, nasal length, nasolabial angle, symmetry, and soft tissue response ratios). Disagreements were resolved through discussion, with arbitration by a third reviewer (R.Y.F.Y.) when necessary.
Demographic Data.
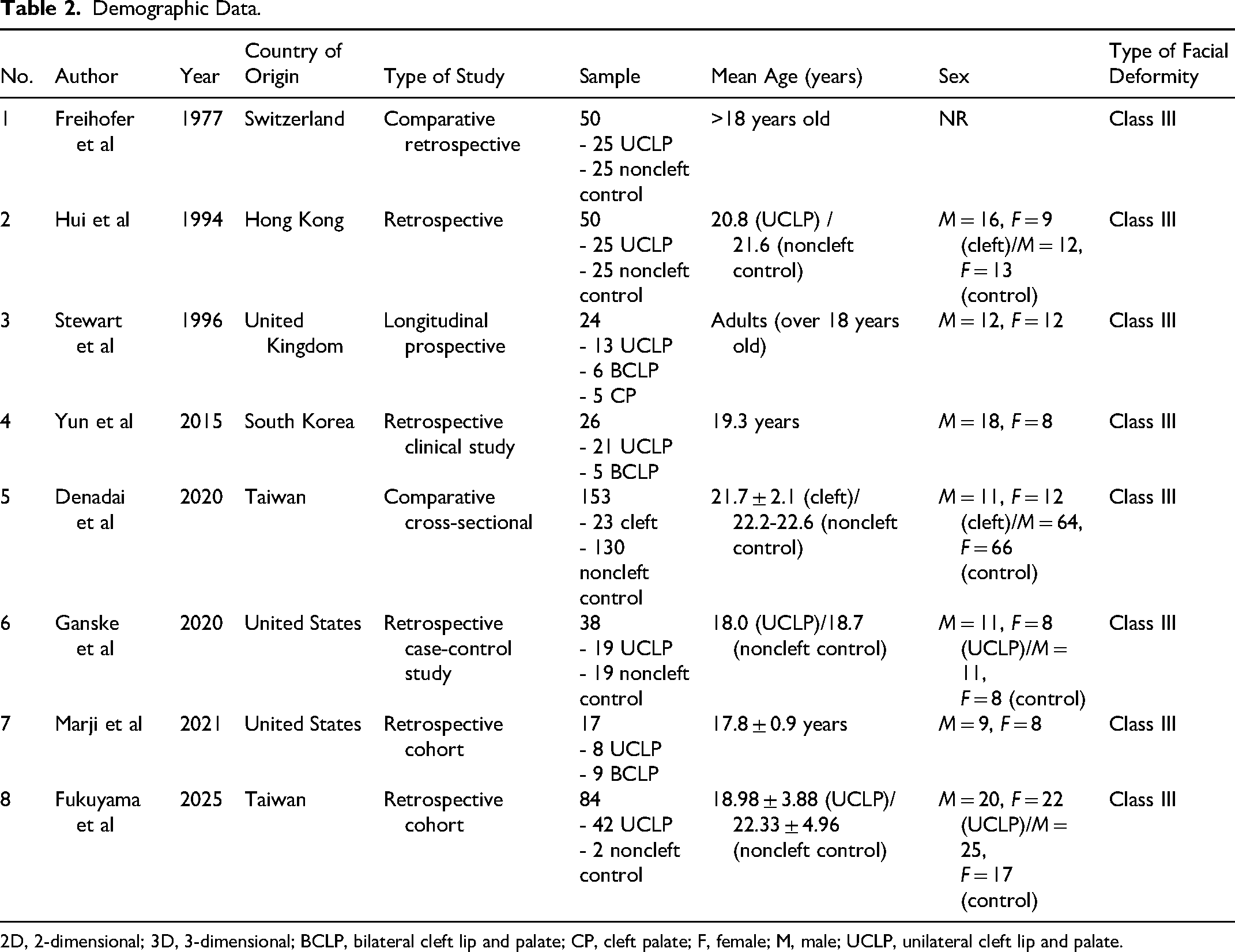
2D, 2-dimensional; 3D, 3-dimensional; BCLP, bilateral cleft lip and palate; CP, cleft palate; F, female; M, male; UCLP, unilateral cleft lip and palate.
Imaging Acquisition and Method of Analysis.
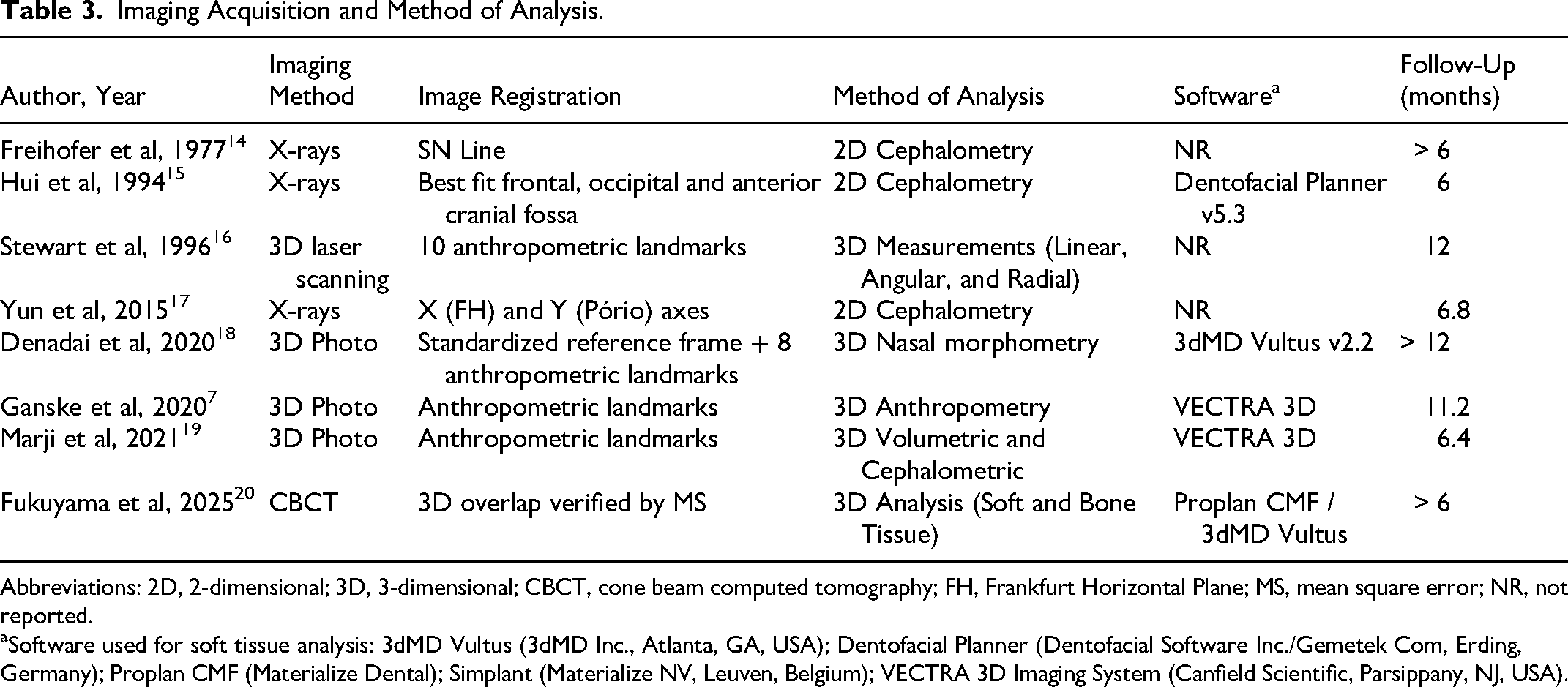
Abbreviations: 2D, 2-dimensional; 3D, 3-dimensional; CBCT, cone beam computed tomography; FH, Frankfurt Horizontal Plane; MS, mean square error; NR, not reported.
Software used for soft tissue analysis: 3dMD Vultus (3dMD Inc., Atlanta, GA, USA); Dentofacial Planner (Dentofacial Software Inc./Gemetek Com, Erding, Germany); Proplan CMF (Materialize Dental); Simplant (Materialize NV, Leuven, Belgium); VECTRA 3D Imaging System (Canfield Scientific, Parsippany, NJ, USA).
Qualitative Data Regarding Nasal Changes.
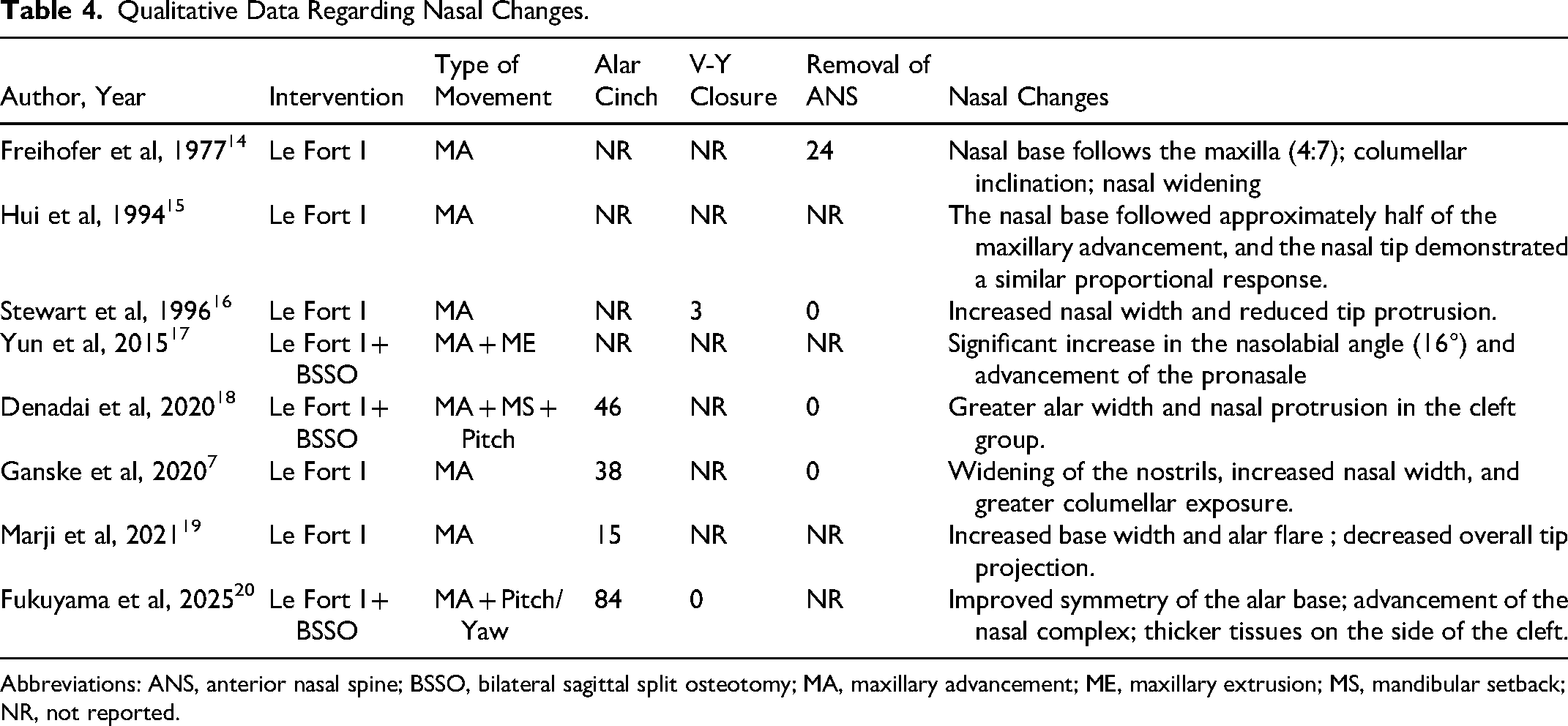
Abbreviations: ANS, anterior nasal spine; BSSO, bilateral sagittal split osteotomy; MA, maxillary advancement; ME, maxillary extrusion; MS, mandibular setback; NR, not reported.
Analysis of Changes in Nasal Soft Tissues
Changes in the soft tissues of the nasal region following Le Fort I osteotomy were evaluated by comparing data before surgery (T0) with those obtained after at least 6 months of postoperative follow-up (T1). The type of surgical intervention was taken into consideration. Data regarding additional procedures, such as alar cinch, V-Y soft tissue closure, and removal of ANS, were also recorded, as well as qualitative changes in the nasal region after orthognathic surgery.
Quality Assessment
Risk of bias was assessed using the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) tool, following its domain-based framework. Each study was independently evaluated by 2 reviewers across all 7 domains: (1) confounding, (2) selection of participants, (3) classification of interventions, (4) deviations from intended interventions, (5) missing data, (6) measurement of outcomes, and (7) selection of reported results.
Each domain was rated as low, moderate, serious, or critical risk of bias according to the ROBINS-I guidance. Disagreements at the domain level were resolved through discussion and consensus, with arbitration by a third reviewer when necessary.
Overall ROBINS-I judgment followed the structured domain-based guidance, with final consensus reached after consideration of the most severe domain-level concerns and their likely impact on overall credibility.
Results
Search Strategy and Study Selection
The initial search of electronic databases was conducted in February 2026, yielding 950 records (MEDLINE via PubMed, n = 222; Scopus, n = 460; Web of Science, n = 50; Embase, n = 218). After removal of duplicates, records were screened independently by 2 reviewers based on titles, resulting in 19 potentially eligible studies. One record was excluded during abstract screening due to unavailable abstract/full metadata. Following abstract screening, 18 studies were selected for full-text assessment. After full-text review, 8 studies met the predefined inclusion criteria and were included in the final synthesis. The remaining 10 studies were excluded for the following reasons: non-nasal outcomes (n = 4), ineligible intervention (n = 3), and unstratified data (n = 3). Manual screening of reference lists did not identify additional eligible studies. The study selection process is summarized in Figure 1.
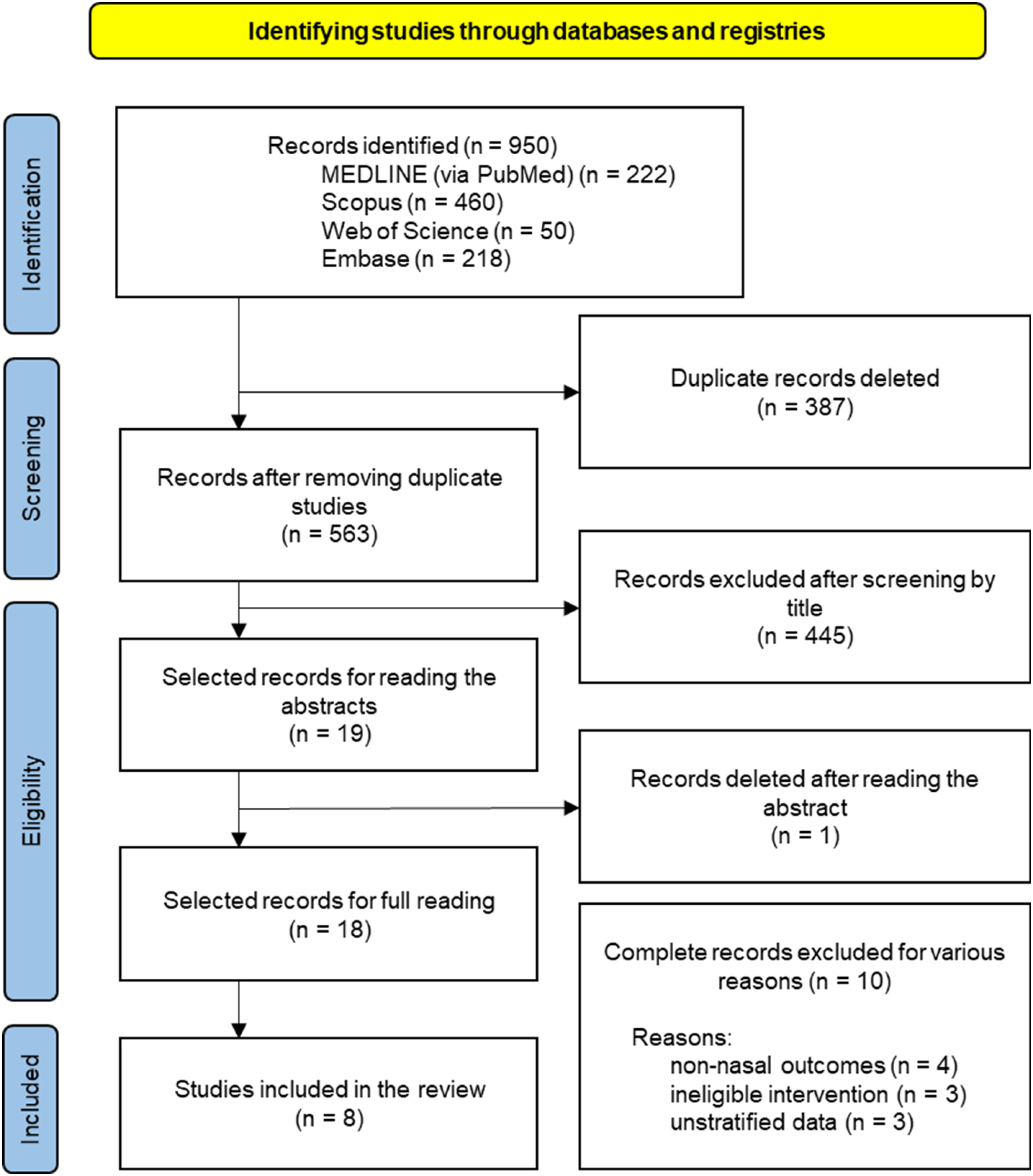
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flowchart.
Study Characteristics
The 8 included studies comprised predominantly retrospective designs, with 1 prospective longitudinal study and 1 cross-sectional study, published between 1977 and 2025. Sample sizes ranged from 17 to 42 patients with CLP, totaling 201 individuals undergoing orthognathic surgery involving Le Fort I osteotomy, either alone or in combination with bilateral sagittal split osteotomy.
Most studies reported sex distribution, with an overall male-to-female ratio of 105:96. Mean age ranged from 17.8 to 22.3 years across studies. All included samples involved patients with Class III dentofacial deformity associated with maxillary hypoplasia or retrusion. Regarding cleft phenotype, some studies included exclusively unilateral CLP (UCLP), while others also reported bilateral CLP (BCLP) and cleft palate (CP) subgroups (Table 2).
Image Acquisition and Facial Analysis Methods
Data regarding image acquisition and facial analysis methods are summarized in Table 3. The included studies employed heterogeneous methodologies for the assessment of nasal morphological changes, with follow-up periods ranging from 6 months to longer than 12 months.
Image acquisition techniques included 2D lateral cephalometry, 3D laser scanning, stereophotogrammetry, and CBCT with soft tissue reconstruction. Earlier studies predominantly relied on 2D cephalometric analyses, whereas more recent investigations used 3D imaging modalities enabling more detailed assessment of nasal surface morphology and volumetric changes.
Assessment of preoperative and postoperative changes (T0-T1) was performed using linear and angular measurements in 2D studies, while 3D studies additionally included surface, volumetric, and symmetry-based analyses of nasal structures such as the alar base and nasal tip.
Surgical and Adjunctive Characteristics
The surgical interventions performed in the 201 patients with CLP included isolated Le Fort I osteotomy or Le Fort I combined with bilateral sagittal split osteotomy (Table 4). Mean maxillary advancement ranged from 4.2 to 7.5 mm across the included studies. Alar cinch suturing was reported in the majority of cases (approximately 183 patients). V-Y closure was rarely applied, being reported in only 3 cases, while 1 study explicitly reported its nonuse. 20 Management of the ANS varied between studies; however, most preserved the ANS, with Freihofer 14 reporting cases in which ANS removal was performed (n = 24).
Nasal Base and Alar Changes
Changes in the nasal base were consistently reported across studies. Fukuyama et al 20 demonstrated that the subnasale (Sn) point followed maxillary advancement with a mean soft tissue response ratio of 0.55 per 1 mm of skeletal movement.Soft tissue response was asymmetric, with a higher correlation on the noncleft side (0.77 mm/mm) compared with the cleft side (0.56 mm/mm), indicating reduced predictability of soft tissue adaptation in cleft regions.
Alar base widening was reported in several included studies, with magnitude varying according to surgical protocol and measurement method. Marji et al 19 reported mean increases of 2.01 mm in alar base width and 1.37 mm in alar flare. Stewart et al 16 reported even greater increases, reaching up to 3.0 mm.
Nasal Tip Projection
Changes in nasal tip projection were heterogeneous across studies. Reported outcomes included increases ranging from 0.44 to 2.40 mm and decreases ranging from 1.1 to 2.22 mm.16,17,20
Freihofer 14 and Hui et al 15 reported nasal tip response ratios ranging from 0.25 to 0.28 relative to maxillary advancement.
Nasolabial Angle
Only 1 study reported detailed angular changes of the nasolabial region. Yun et al 17 observed a mean postoperative increase of 16.0°, with the nasolabial angle changing from 72.7° preoperatively to 88.7° postoperatively, indicating a tendency toward a more obtuse nasolabial profile.
Symmetry and Additional Outcomes
In patients with UCLP, Fukuyama et al 20 observed improved alar base surface symmetry after orthognathic surgery with yaw rotations, reducing inter-side discrepancy from 1.42 to 0.96 mm (p = .013). In a follow-up of more than 12 months, Denadai et al found that the cohort of patients with CLP exhibited smaller nasal length (N-Prn) and tip projection angle (Sn.N.Prn) (39.6 mm and 20.1°, respectively; p < .001) compared to the reference values of the control group (42.2 mm and 23.0°). Furthermore, the alar width (linear distance between the Alare points) was greater in the cleft group (42.2 mm; p < .001) than the average observed in individuals without cleft (38.8 mm). 18
Quantitative normalized soft tissue response ratios relative to maxillary advancement are summarized in Supplemental Table S1. This supplementary table was created to facilitate comparison of study-level soft tissue responses relative to the magnitude of maxillary advancement.
Quality Assessment
The risk of bias was classified as high in 5 studies and moderate in 3 studies, with no studies identified as having a critical or low overall risk of bias, according to the ROBINS-I tool (Figure 2). The main methodological criteria that contributed to the increased risk of bias were the heterogeneity of surgical interventions, the absence of stratification regarding the type and magnitude of maxillary movement, and the lack of standardization in the use of auxiliary techniques, such as alar cinch and V-Y closure. Furthermore, limitations related to outcome measurement and the selection of reported results were observed in several studies. The studies that presented a moderate risk of bias used more robust 3D methods and described the evaluation protocols more consistently, although they were still limited by their observational design.
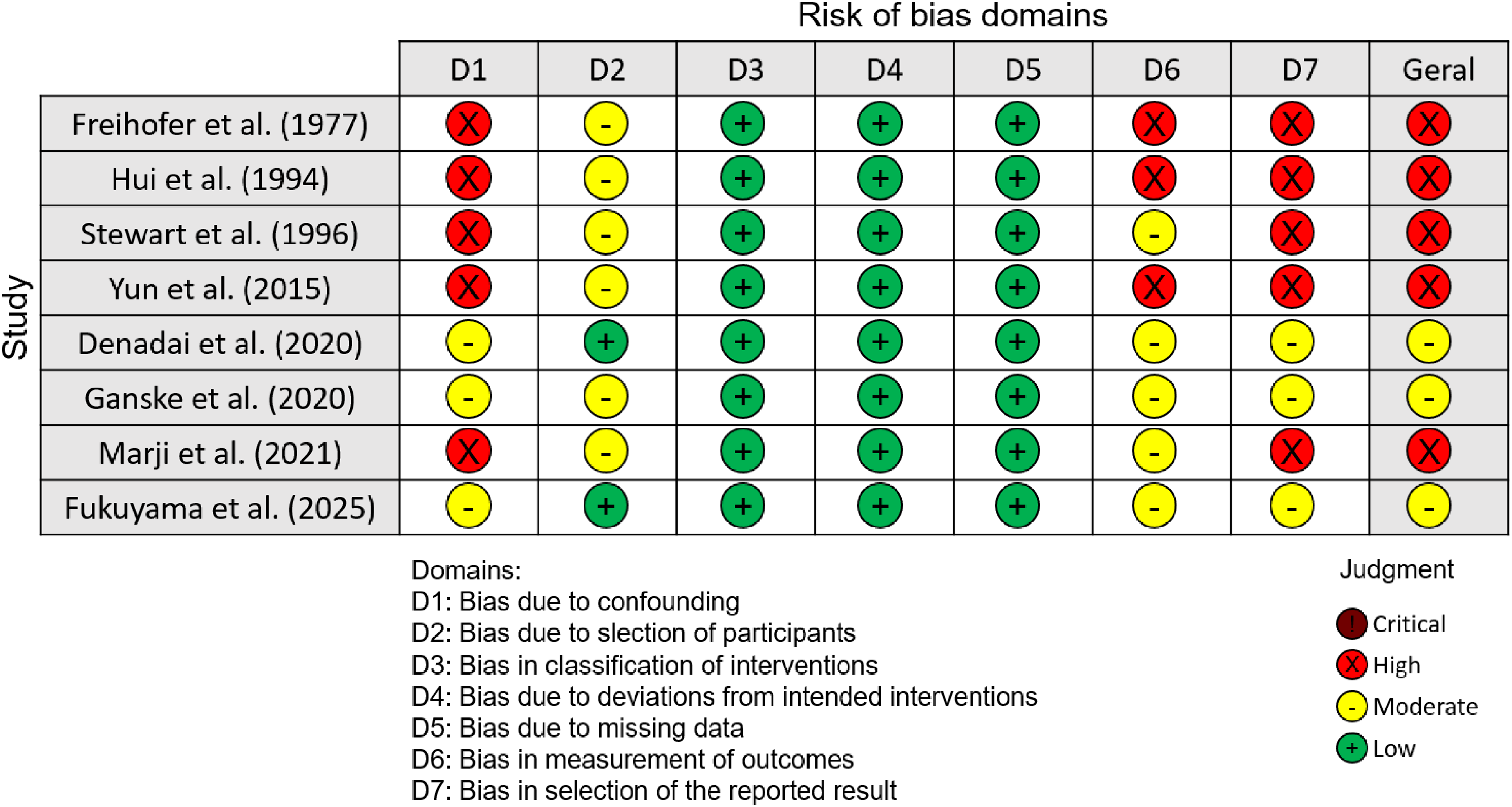
Evaluation of the risk of bias of the individual studies included in the systematic review according to the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) assessment tool.
Discussion
This review identified recurring patterns of morphological changes in the nasal region in individuals with CLP undergoing Le Fort I osteotomy. The search strategy in the MEDLINE (via PubMed), Web of Science, Scopus, and Embase databases was designed to maximize identification of potentially eligible studies for systematic assessment. However, the methodological quality analysis using the ROBINS-I tool revealed that the included studies presented moderate to high risk of bias, requiring cautious interpretation and limiting confidence in the strength and generalizability of the reported observations.
In general, the included studies demonstrated that Le Fort I osteotomy was associated with measurable changes in nasal base width, nasal tip projection, and nasolabial angle, although with considerable variations in the magnitude and direction of these changes. Freihofer 14 and Hui et al, 15 in classic studies based on 2D cephalometry, reported anterior displacement of the nasal base and tip following maxillary advancement, although with high individual variability, a characteristic frequently observed in patients with CLP due to previous scars and altered nasal anatomy related to the various types of cleft.14,15
With the advancement of 3D methodologies, more recent studies have allowed more detailed assessment of soft tissue response. Stewart et al 16 reported a significant increase in nasal width associated with a reduction in nasal tip projection after maxillary advancement, with findings suggesting greater lateral expansion of the alar base relative to anterior displacement of the nasal tip. Similar results were observed by Ganske et al 7 who, even with the systematic use of alar cinch and V-Y closure, identified widening of the nostrils, indicating that auxiliary techniques, although useful, may reduce but do not fully prevent nasal changes induced by surgery.
Marji et al 19 and Denadai et al 18 reported findings broadly consistent with these observations by demonstrating increased alar width and modifications in nasal tip projection and nasolabial angle, in addition to associating morphological changes with subjective outcomes of aesthetic satisfaction. These observations suggest potential clinical relevance of nasal alterations, since small dimensional variations can have a significant impact on aesthetic perception, particularly in individuals with CLP, in whom nasal symmetry is already a preoperative challenge. Additionally, the magnitude of maxillary displacement can directly influence the predictability of tissue response.
Fukuyama et al observed that, in maxillary advancements between 6 and 10 mm, the correlation between bone and soft tissue movement is strong on the side without cleft (r = 0.83), but reduces to moderate on the side with the cleft (R = 0.58). 20 In this scenario, the average soft tissue response rate is significantly lower on the cleft side (0.56 ± 0.30) than on the noncleft side (0.77 ± 0.33). 20 Although it is suggested that the soft tissue response rate may be slightly higher in more significant advancements, substantial interindividual variability remains an important limitation for precise prediction.14,15
Fukuyama et al 20 demonstrated improved alar base symmetry after surgery, particularly in patients with UCLP, using CBCT-based 3D analysis. This finding suggests that, in addition to inducing dimensional changes, Le Fort I osteotomy may be associated with redistribution of nasal soft tissues toward improved symmetry in selected cases, although the effects on other variables, such as nasal projection and angles, have not been detailed. On the other hand, Yun et al 17 showed that, in bimaxillary surgeries, the increase in the nasolabial angle may be related not only to maxillary advancement but also to the interaction with mandibular movements, reinforcing the complexity of the soft tissue response in combined approaches.
Taken together, the available studies suggest that nasal changes after Le Fort I osteotomy in individuals with CLP are multifactorial, being influenced by the type and magnitude of maxillary movement, the use of auxiliary techniques, and individual soft tissue characteristics. Although Le Fort I osteotomy is not primarily intended as a nasal corrective procedure, awareness of its potential postoperative nasal effects may assist surgical planning and patient counseling, particularly when adjunctive nasal procedures are being considered in patients with CLP. Direct comparison across studies remains limited not only by differences in imaging modality, surgical adjunctive procedures, and outcome reporting methods, but also by the intrinsic heterogeneity of cleft phenotypes and the current lack of larger controlled studies in this population. Direct quantitative comparison across studies was limited by differences in follow-up duration, imaging protocols, surgical techniques, and outcome measures. In addition, incompatibility of effect measures and inconsistent outcome definitions precluded quantitative synthesis (meta-analysis).
Furthermore, the ROBINS-I assessment indicated moderate to high risk of bias across the included studies, mainly related to retrospective designs, limited sample sizes, and heterogeneity in surgical protocols and outcome assessment. These methodological limitations limit confidence in the consistency and external generalizability of the reported observations and require cautious interpretation of observed trends. The inclusion of both 2D and 3D studies reflects the limited available evidence and the historical evolution of assessment methods in cleft orthognathic research. Although this increased methodological heterogeneity, it allowed broader descriptive synthesis of clinically relevant nasal outcomes. Future prospective studies using standardized imaging protocols and outcome definitions, preferably with larger controlled cohorts, are needed to improve comparability and allow more reliable assessment of clinical predictability.
Conclusions
Le Fort I osteotomy is associated with postoperative nasal morphological changes in individuals with CLP. Although improvements in alar base symmetry and nasolabial angle have been reported, alar widening and variable changes in nasal tip projection and nasal length are also observed. Given the methodological heterogeneity and moderate-to-high risk of bias of the available studies, these findings should be interpreted cautiously. Future prospective studies with standardized protocols are necessary to improve the prediction of postoperative nasal soft tissue outcomes in this population.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261462303 - Supplemental material for Nasal Changes After Le Fort I Osteotomy in Individuals With Cleft Lip and Palate: A Systematic Review
Supplemental material, sj-docx-1-cpc-10.1177_10556656261462303 for Nasal Changes After Le Fort I Osteotomy in Individuals With Cleft Lip and Palate: A Systematic Review by Luciano R. de A. Carvalho, Caroline de P. O. Gringo, Isabela T. T. Da Silveira, Bhárbara M. Barcellos, Peterson R. Garcia, Osny Ferreira Júnior and Renato Y. F. Yaedú in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656261462303 - Supplemental material for Nasal Changes After Le Fort I Osteotomy in Individuals With Cleft Lip and Palate: A Systematic Review
Supplemental material, sj-docx-2-cpc-10.1177_10556656261462303 for Nasal Changes After Le Fort I Osteotomy in Individuals With Cleft Lip and Palate: A Systematic Review by Luciano R. de A. Carvalho, Caroline de P. O. Gringo, Isabela T. T. Da Silveira, Bhárbara M. Barcellos, Peterson R. Garcia, Osny Ferreira Júnior and Renato Y. F. Yaedú in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
The authors gratefully acknowledge the institutional support provided by the Hospital for Rehabilitation of Craniofacial Anomalies (HRAC-USP) and the Bauru School of Dentistry, University of São Paulo (FOB-USP).
ORCID iDs
Ethical Approval
This study is a systematic review of previously published studies and did not involve human participants directly. Therefore, ethical approval and informed consent were not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received partial financial support from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil, through the Programa de Demanda Social (Grant No. 88887.877179/2023-00).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article. Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.