
Abstract
Congenital palatal fistula is a rare embryologic anomaly, occurring in one percent of cleft cases, often causing hypernasality and nasal regurgitation. We report a 3-year-old male with an isolated fistula at the hard-soft palate junction. Repair was performed using a combined technique: a turnover hinge flap for the nasal layer and Z-plasty flaps for the oral layer. A fistula at this area is difficult to manage because of paucity of tissue. The two layer closure that we describe is a refinement of technique with practical applications.
Introduction
Congenital palatal fistula (CPF) is among the rarest entities along the continuum of embryologic disorders in palatogenesis. 1 CPF is a very rare entity with an estimated incidence of 6-17% among patients presenting with submucous cleft palate. 2 True isolated congenital clefts of the hard palate have also been described which is exceedingly rare in the incidence (<1% of the cases).3-6 Congenital fistula of the palate was first reported by Veau in 1931. 7 Lynch et al hypothesized that isolated CPF result from localized developmental disruptions, specifically in the fusion process of palatine shelves in early fetal development. 5 Patients present with speech disturbance, hypernasality, and oronasal regurgitation, leading to poor weight gain and failure to thrive. 7 Treatment is usually surgical. The aims of the surgery remain the separation of nasal and oral cavities, rearrangement of palatal muscles, and lengthening of the soft palate.
Case Report
A 3-year-old boy presented with a history of a small aperture in the center of the palate. The parents had noticed the fistula at birth. The child had no difficulty in feeding, with infrequent episodes of nasal regurgitation. They waited initially and visited us when they realized that it would not close on its own. There was no history of systemic illnesses, speech abnormalities, trauma, or surgery. There was no family history of cleft lip or palate. During the pregnancy, there was no incidence of maternal exposure to radiation, antiepileptics, smoking, and alcohol abuse. On examination, a 5 mm diameter, full-thickness fistula was present at the hard palate and soft palate junction and no type of cleft lip and palate accompanying the fistula (Figure 1: Isolated congenital palatal fistula at hard palate and soft palate junction). The posterior one third of the secondary palate was well developed, and there was no bifid uvula. Systemic examination was normal.
The patient underwent palatal fistula closure using a unique technique in which we combined the median palatal mucoperiosteal flap 8 for repairing the nasal layer, with Z-plasty flaps for the oral layer. According to the weight of the patient, only a single dose of injection augmentin was given before giving the incision. A flap-based posteriorly on the anterior margin of the cleft, extending up to the incisive foramen and as wide as the cleft is marked out on the palate (Figure 2(a): Illustrates marking of turn down flap and mucosal Z-plasty flaps), and the flap is turned over 180° as if on a hinge, to close the inner lining (nasal layer) of the defect (Figure 2(b): Depicting the median palatal mucoperiosteal flap for nasal lining). Following this, we raised bilateral mucosal Z flaps. On raising the flaps, we found that the muscles were joined together and were in their normal orientation (Figure 2(b)). The nasal layer was closed with interrupted 4-0 Vicryl sutures. The oral layer was reconstituted above this with the Z flaps interposing (Figure 2(c): Z-flap inter-positioning). The interposition opened up lateral raw areas bilaterally, which was left for secondary healing (Figure 3: Oral layer closed with mucosal Z-plasty flaps). The parents were advised to feed the child clear liquids via a spoon for 2 weeks and then to start a soft semi-solid diet. To maintain oral hygiene, instructions were given to cleanse the mouth after every meal with clear water. The postoperative period was uneventful. At 9 months follow-up, the child had a well-healed palate (Figure 4).

Isolated congenital palatal fistula at hard palate and soft palate junction.
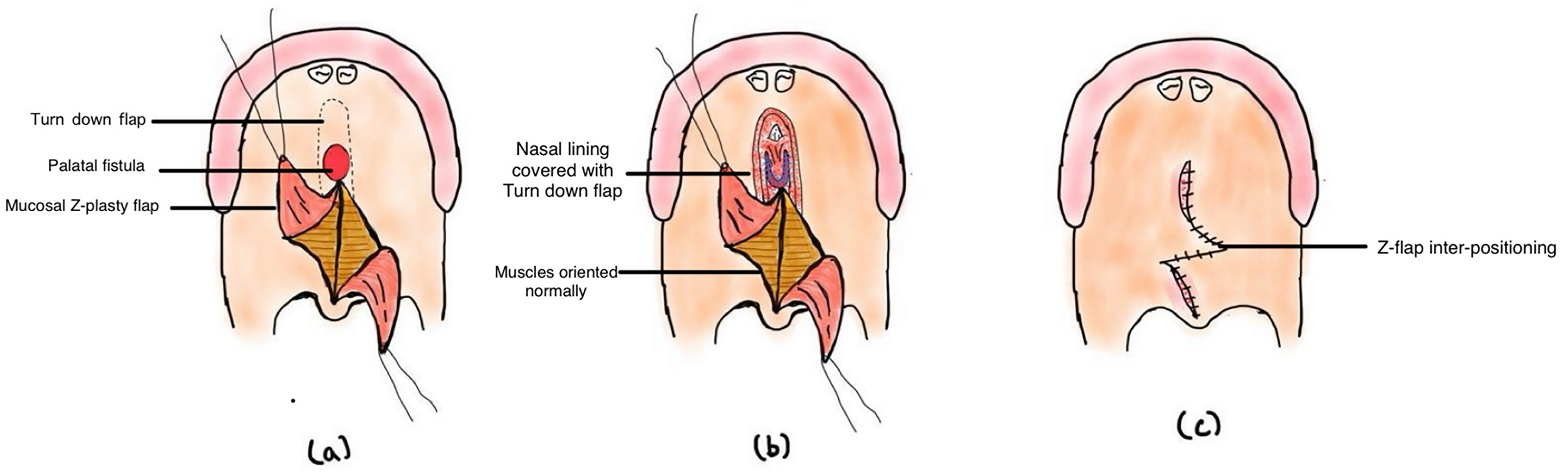
(a) Turn down flap and mucosal Z-plasty flaps, (b) depicting the median palatal mucoperiosteal flap for nasal lining and mucosal Z plasty flaps for oral layer, muscles were oriented normally, and (c) Z-flap interpositioning.
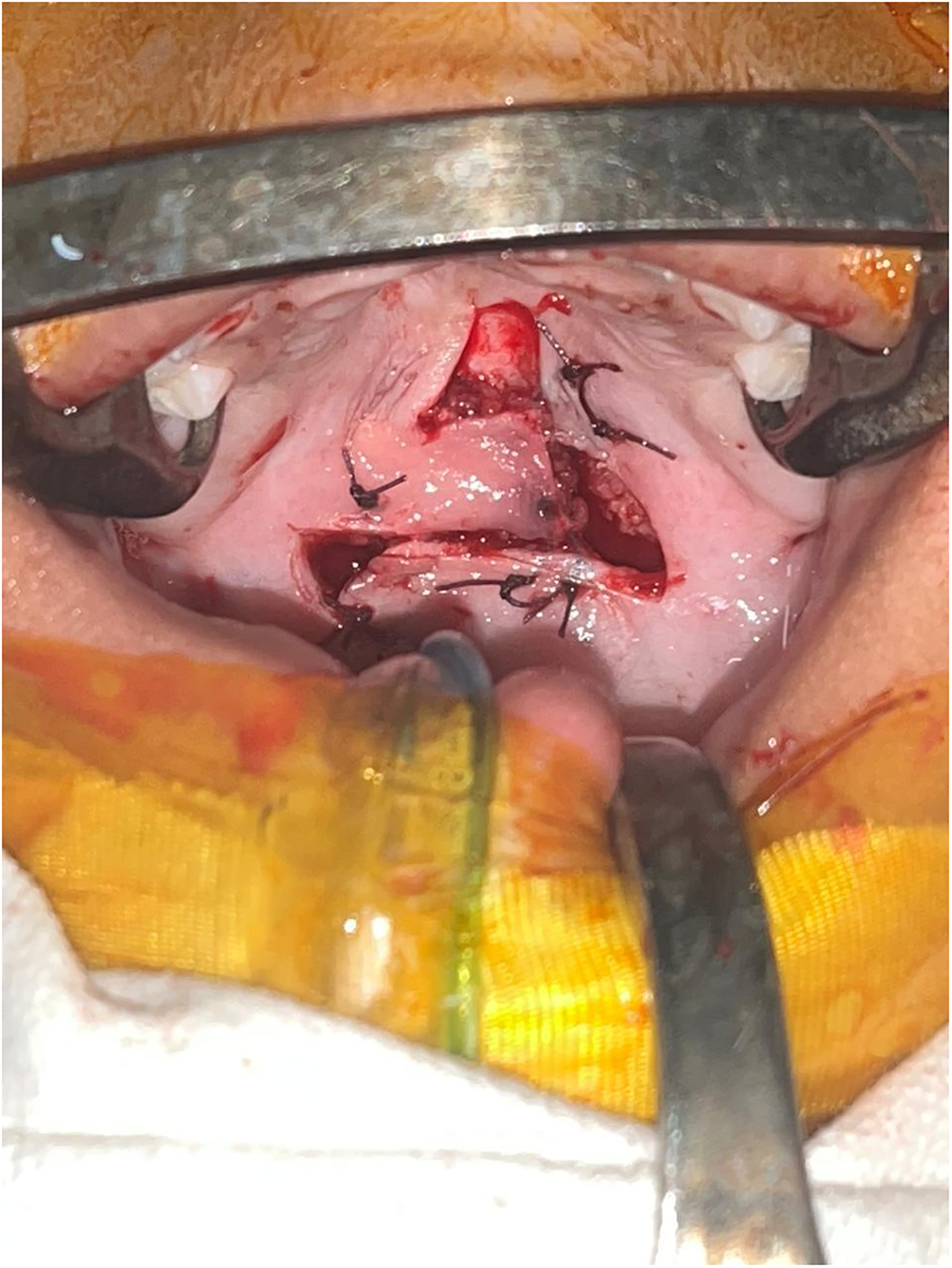
Oral layer closed with mucosal Z-plasty flaps.

Follow-up photograph: 9 months after the surgery.
Discussion
CPF is an extremely rare deformity. It is the rarest deformity in clefts as described by Millard (1980). Cheng and Zhou have suggested that congenital fistula of the palate should be accepted as a failure of the palatal differentiation of the human fetus, which is not caused by an accident or an artificial factor. 9
In 1935, Burian performed closure with a unilateral palatal mucoperiosteal flap. Repair with a pharyngeal flap was reported by Fara (1971). Fara suggested that the repair should combine closure of the fistula with a push-back of the shortened soft palate. To decrease the enlarged pharyngeal cavity, a superiorly based pharyngeal flap and a realignment of the palatal muscles were performed.
Cheng and Zhou performed “von Langenbeck” palatal repair in three cases of congenital fistula of the palate. In all of them, no appreciable velopharyngeal function could be achieved. They stated that the aim is not only the closure of the deformity, but also the lengthening of the soft palate and the reconstruction of palatal muscular connection. 9
Karacan et al stated that CPF can be managed conservatively, and the surgical intervention may be postponed up to 18 to 24 months, the ideal repair time in cleft palate surgery, because of likelihood of spontaneous closure. 4
Gulati et al reported a case of unilateral CPF which was repaired by use of Bardach's palatoplasty along with intravelar veloplasty.
A fistula is best closed in two layers, which ideally means two flaps. A midline fistula at the junction of the hard and soft palates is difficult to close, because of the paucity of local tissue. Appukuttan et al performed a random pattern tongue-shaped flap, which flipped 180 degrees onto the hard palate soft palate junction, to ease the closure. This flap was pedicled on the anterior aspect of the fistula itself. In the present case, we began by raising such a flap. After flipping it as if on a hinge, this flap lay on the nasal floor. The raw area on the undersurface of the flap was visible from the oral side. The Z flaps on the oral side of the soft palate were elevated, to examine the orientation of the muscles. These were raised at a level just above the soft palate musculature. These were then interposed to resurface the fistula in the center on the oral side.
The surgical technique that we have described is a refinement of previously described techniques. The advantage of our technique was that it permitted the formation of two layers in the midline. A limitation of this technique is that it left secondary defects which had to heal by mucosal re-epithelialization. In the follow-up pictures at 3 months (Figure 5) and at 9 months (Figure 4), we can see well-healed palate with no evidence of fistula breakdown or recurrence. Also, functional investigations such as nasometry were not employed. These should be considered as limitations of the report.

The follow-up photograph is 3 months after the surgery showing well-healed palate.
Conclusion
Congenital fistula of the palate is a rare anomaly. Most of the previous reports have shown poor velopharyngeal function after fistula repair. Being a case of rare entity, our method of surgical repair is also different from previously reported cases. We have combined the median palatal mucoperiosteal flap technique for the nasal layer with bilateral Z-plasty flaps for oral layer closure, achieving an effective fistula repair.
Supplemental Material
Footnotes
Ethical Approval
Our institution does not require ethical approval for reporting individual cases.
Informed Consent Statements
Written informed consent was provided by the legally authorized representative.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.