
Abstract
Background
Secondary alveolar bone grafting (SABG) is essential for correcting alveolar defects in patients with cleft lip and palate. While clinical evaluation combined with 2-dimensional (2D) radiography is a practical and cost-effective method for assessing surgical success, inadequate grafting outcomes often necessitate repeat surgeries.
Objective
To evaluate the clinical variables influencing SABG outcomes in cleft patients using 2D radiographic images.
Materials and Methods
This retrospective study reviewed data from 63 patients who underwent SABG at the Faculty of Dentistry, Prince of Songkla university between 2013 and 2023. Variables analyzed included age, cleft type/size, surgical techniques, graft materials, and orthodontic timing. Efficacy was assessed via 2D radiographs (18 conventional, 45 digital) using the Chelsea scale for bone bridging and ImageJ software for bone density. Statistical analyses involved Chi-square tests and multiple logistic regression (P < 0.05).
Results
Overall analysis revealed that patient age and cleft type were the only significant predictors of SABG success, with odds ratios of 10.46 and 5.19, respectively. Subgroup analyses indicated that the timing of post-surgical orthodontic movement was the most significant factor in the conventional radiography group, whereas cleft type was the primary determinant in the digital group.
Conclusion
Patient age and cleft type significantly impact SABG outcomes. Patients aged 10-12 years and those with unilateral cleft deformities exhibit significantly higher success rates compared to other age groups and bilateral deformities.
Introduction
Patients with cleft lip and palate often encounter various issues related to the abnormal anatomy of their jaw and face. In the area of the alveolar cleft, problems may include oronasal fistula, the malposition or abnormal eruption inside the alveolar cleft of canine and lateral incisors, and hypernasality sound, particularly with larger defects. 1 Therefore, alveolar bone grafting in this region is crucial. The primary objective is to correct the defect so that it functions properly and has a suitable shape. Furthermore, there are additional benefits, including offering bone support to teeth adjacent to the cleft, facilitating eruption of adjacent teeth, ensuring proper upper jaw and alveolar bone contour, achieving appropriate arch width, enhancing stability of maxilla, correcting alveolar ridge abnormalities, closing oral-nasal communication, and contributing to harmonious facial and nasal esthetics. 2
The procedure of secondary alveolar bone grafting (SABG) was first described by Boyne and Sands in 1972 and has since become a standard surgical protocol for alveolar bone grafting. SABG is typically performed on children aged 2 and above, with the procedure commonly performed between the ages of 7 and 11. This age range corresponds to the eruption of lateral incisor and canine teeth in the oral cavity and the near completion of vertical and horizontal growth of the upper jaw. Therefore, bone grafting during these early ages may minimize the impact on the subsequent growth of the upper jaw. 3
The bone used for grafting, harvested from autogenous sources, can be obtained from various areas, but the gold standard location is the anterior iliac crest. This is due to its strong osteogenic potential and immune-compatible bone cells. Therefore, it is commonly utilized for areas affected by cleft lip and palate defects. 4
To validate the success of bone grafting, surgeons typically employ various assessment methods. These include evaluating tooth eruption in relation to the defect, assessing the periodontal status, and considering the esthetic appearance of the face. However, the use of radiographic images is an important tool for assessing surgical outcomes. 5 Periapical and occlusal radiographs are utilized in many studies. Nevertheless, they come with limitations. One disadvantage is that these radiographs are 2-dimensional (2D), thus they cannot accurately assess bone volume. Additionally, they may have distortion. 6
Therefore, another method that can be used for evaluation is computed tomography (CT) radiographic images. The advantage of CT images is that they can assess bone volume, but the disadvantage is that they are costly and expose patients to unnecessary radiation. However, in practical terms, the combination of 2D radiographic images with physical examination is sufficient for evaluating surgical outcomes because it is easy to perform and cost-effective. 7
The success of alveolar bone grafting holds significance because insufficient bone graft amounts, particularly concerning orthodontic tooth movement, may require additional grafting, leading to the possibility of multiple surgeries for some patients. To mitigate these challenges, numerous studies aim to identify factors affecting the success of alveolar bone grafting. From the previous studies, these factors encompass the age at which the grafting is performed, the type and width of the cleft, the surgical technique, the type of bone graft, the use of a membrane, autologous growth factors, and the duration of orthodontic treatment. Inadequate bone grafting, insufficient for tooth eruption or orthodontic movement, has been identified as a potential factor requiring repeat surgery. This recurrence introduces increasing risks and side effects, including increased anesthesia and surgery-related expenses, along with prolonged hospital stays.2,3,8–10
While previous studies have evaluated individual predictors of SABG success,10,11 few have simultaneously examined orthodontic treatment timing12,13 or compared the predictive performance of conventional and digital radiographic modalities using a combined bone-bridge and bone density composite score. Therefore, this retrospective study aims to investigate factors influencing the success of SABG using 2D radiographic images, aiming to aid treatment planning and predict outcomes in patients with cleft lip and palate defects.
Materials and Methods
Ethical Approval and Study Design
This retrospective study was approved by the Institutional Human Research Ethics Committee of the Faculty of Dentistry, Prince of Songkla University (Approval Number: EC6512-045). The study was registered with the Thai Clinical Trials Registry (TCTR20240325001). Due to the limited target population, a consecutive samplimg method was employed to include all eligible patients between 2013 and 2023. A total 63 patients were included in this study.
Data Collection and Participant Selection
Data were collected from medical records, surgical reports, and periapical radiographs (both conventional and digital) spanning a period of 10 years and 3 months (January 1, 2013 to March 31, 2023). Participants included patients diagnosed with cleft lip and palate who underwent SABG at a Faculty of Dentistry, Prince of Songkla University. Regarding the preoperative clinical status, all included patients (100%) presented with an oronasal fistula prior to the SABG procedure. Inclusion criteria consisted of patients with high-quality postoperative periapical radiographs showing clear anatomical structures taken 6-12 months after surgery. Patients with incomplete records or poor-quality radiographs that precluded interpretation were excluded.
Variables and Outcome Assessment
Data related to SABG success were gathered from dental treatment, medical, and orthodontic records. Eight factors were analyzed: age at grafting (10-12 years vs. others), type of cleft (unilateral vs. bilateral), cleft width (< 6.3 mm vs. ≥ 6.3 mm, measured according to Kawakami et al (2002) 14 ; Figure 1), surgical technique (trapezoidal flap vs. others), bone graft type (iliac crest vs. others), use of collagen membrane (yes vs. no), use of autologous growth factors (yes vs. no), and orthodontic treatment timing after surgery (< 3 months vs. ≥ 3 months).
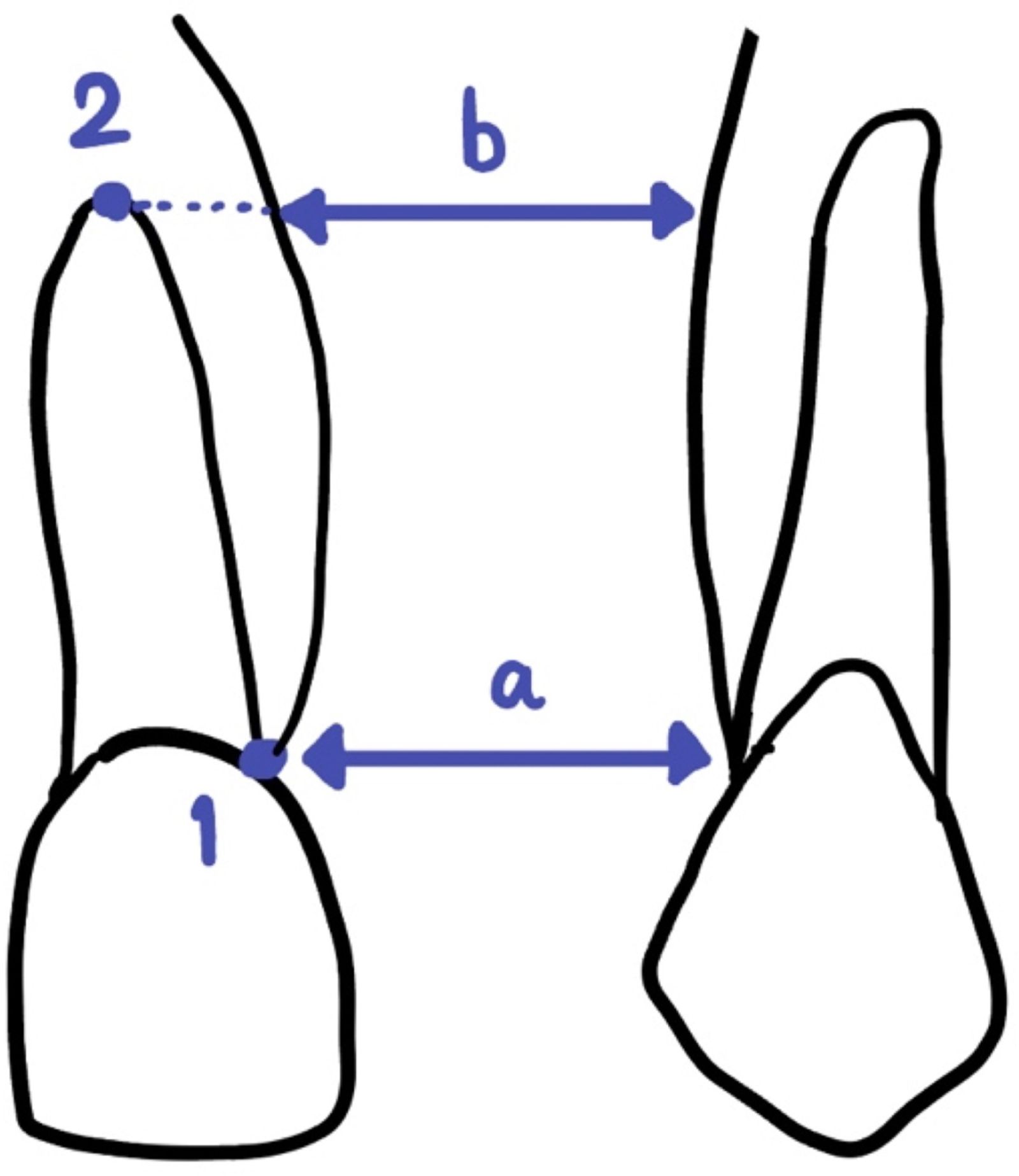
Radiographic measurement of the cleft width. Point 1 represents the distal cementoenamel junction (CEJ) of the tooth adjacent to the mesial aspect of the cleft. Point 2 indicates the root tip of the same tooth. Distances “a” and “b” represent the narrowest widths measured from Point 1 and Point 2, respectively. The cleft width was calculated using the formula: (a+b)/2.
Bone graft success was evaluated using a composite score derived from 2D radiographic images analyzed with ImageJ software (Version 1.53k; NIH, USA). The composite score included:
Composite Scoring Criteria for Secondary Alveolar Bone Grafting Success.
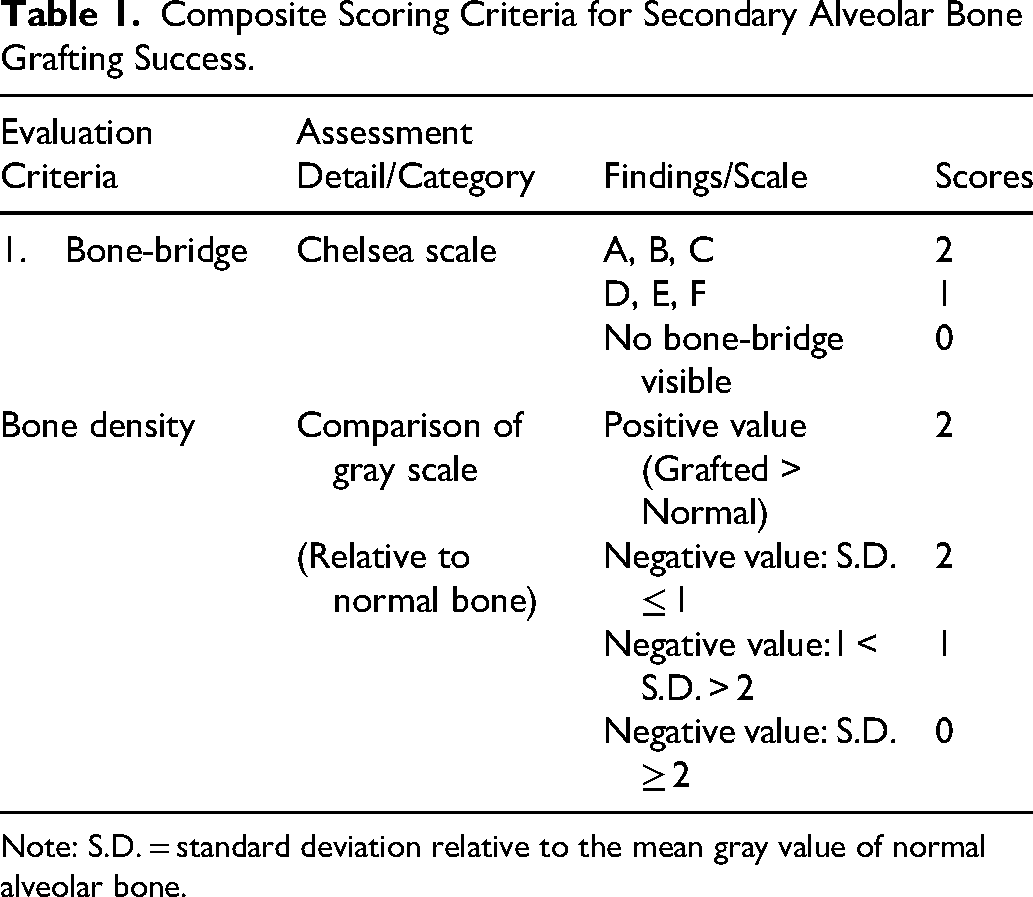
Note: S.D. = standard deviation relative to the mean gray value of normal alveolar bone.
The total composite score of bone-bridge and bone density of 0-1 indicated an unsatisfying outcome while a total score of 2-4 indicated a satisfactory outcome.
To ensure measurement consistency, intra-examiner reliability was verified by re-evaluating 15 randomly selected radiographs (23.8%) after a 2-week interval. 16 Cohen's Kappa coefficient was calculated.
Statistical Analysis
Data analysis was performed using SPSS Statistics (version 26.0; IBM Corp., Armonk, NY, USA). Chi-square tests and multivariate logistic regression were used to determine relationships among the eight factors. Cohen's Kappa statistics assessed the reliability of data collection and analysis. Statistical significance was set at P < 0.05.
Result
Reliability and Patient Demographics
Intra-examiner reliability was assessed using a representative subset of the data (23.8%), achieving a Cohen's Kappa coefficient of 0.87, indicating strong agreement suitable for clinical research analysis. The study population consisted of 63 patients with cleft lip and palate who underwent SABG. Participants were categorized based on the radiographic technique used: conventional (n = 18) and digital (n = 45). Representative cases of satisfactory and unsatisfactory outcomes are illustrated in Figure 2. Detailed demographic characteristics and clinical factors are summarized in Table 2.
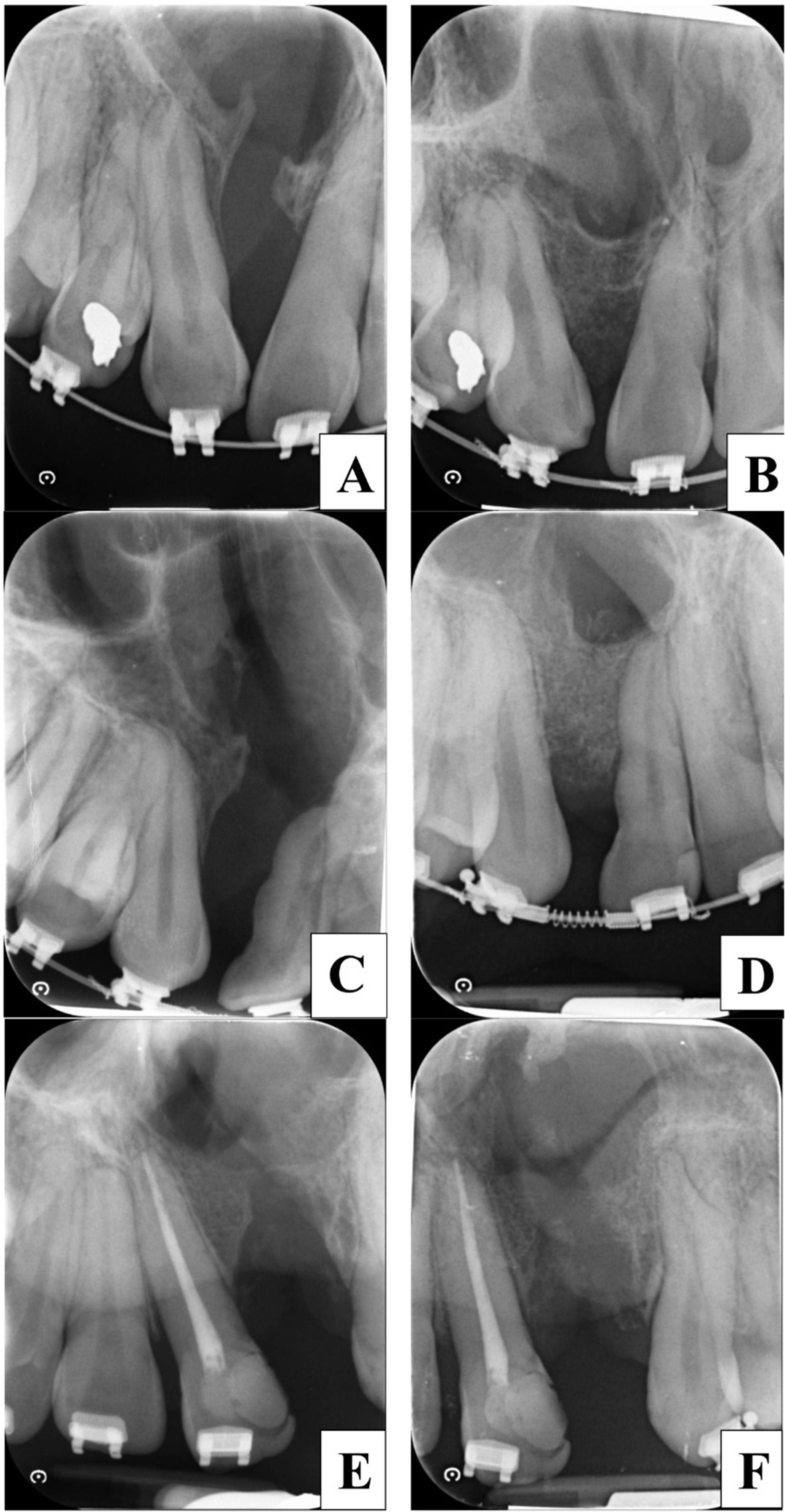
Representative periapical radiographs of secondary alveolar bone grafting outcomes. (A, C, E) Preoperative radiographs showing the initial alveolar cleft defects in three different patients. (B, D) Postoperative radiographs at 6–12 months showing satisfactory outcomes with robust bone bridging (Chelsea scale A-C) and integrated bone density. (F) Postoperative radiograph illustrating an unsatisfactory outcome characterized by incomplete bone bridging and graft resorption.
Demographic Characteristics of Patients.
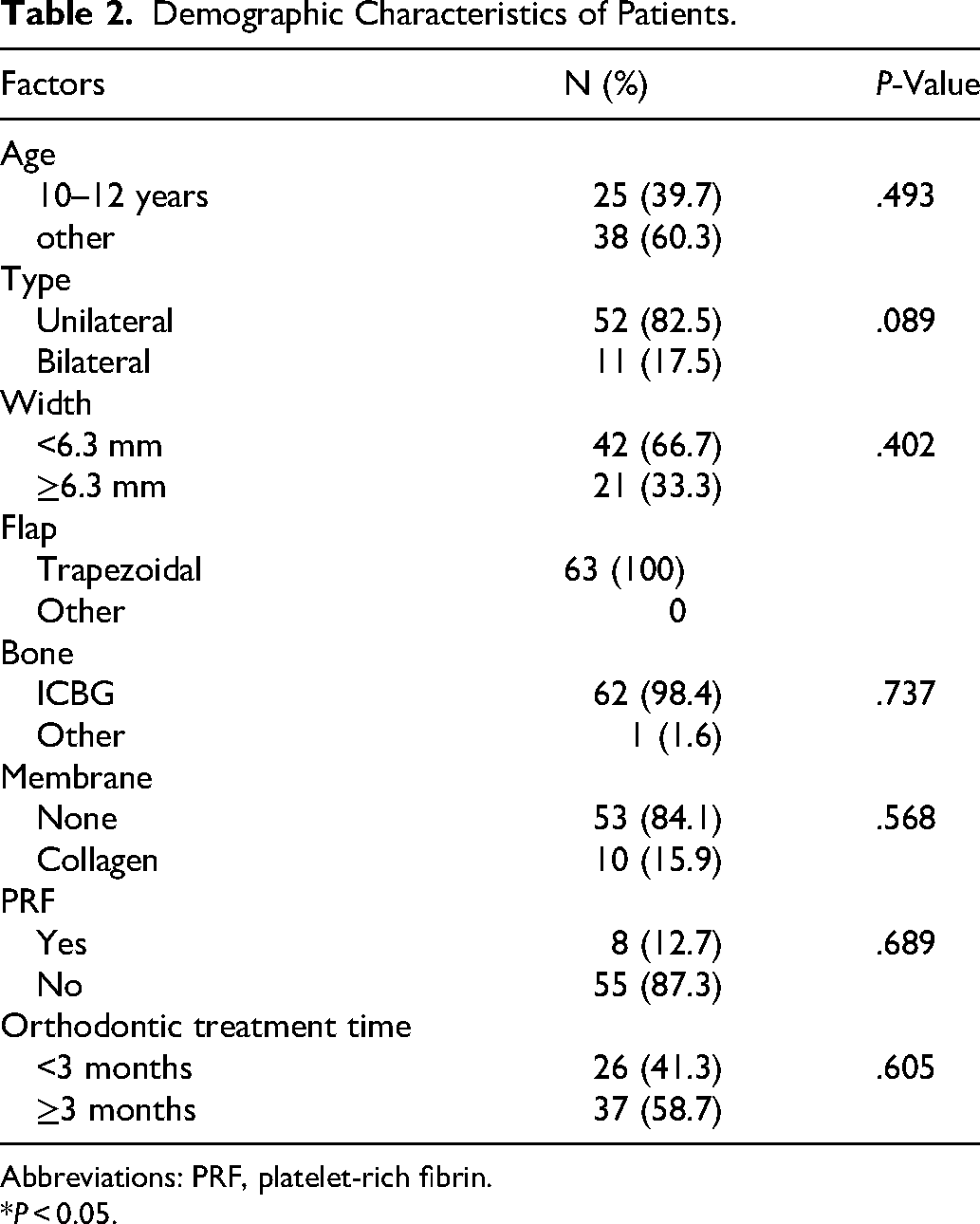
Abbreviations: PRF, platelet-rich fibrin.
*P < 0.05.
Factors Associated with Satisfactory Outcomes: Univariate Analysis
Univariate logistic regression demonstrated that age and cleft type were significantly associated with satisfactory SABG outcomes across the entire cohort (P < 0.05). Specifically, patients aged 10-12 years were 12.48 times more likely to achieve a satisfactory outcome compared to other age groups (OR: 12.48; 95% CI: 1.51-102.9). Similarly, unilateral clefts were associated with a 6.6-fold increase in the likelihood of success compared to bilateral clefts (OR: 6.60; 95% CI: 1.62-26.92). Subgroup analysis further revealed distinct significant factors; in the conventional group, both age (OR: 1.83;P = 0.036) and the timing of orthodontic tooth movement (OR: 0.05;P = 0.009) showed significant correlations with success. Conversely, in the digital group, age (OR: 1.38; P = 0.021) and cleft type (OR: 8.25; P = 0.009) were significant predictors, while orthodontic timing showed a non-significant trend (OR: 0.36; 95% CI: 0.075-1.77) (Table 3).
Factors Associated with Satisfactory SABG Outcomes: Univariate Analysis.
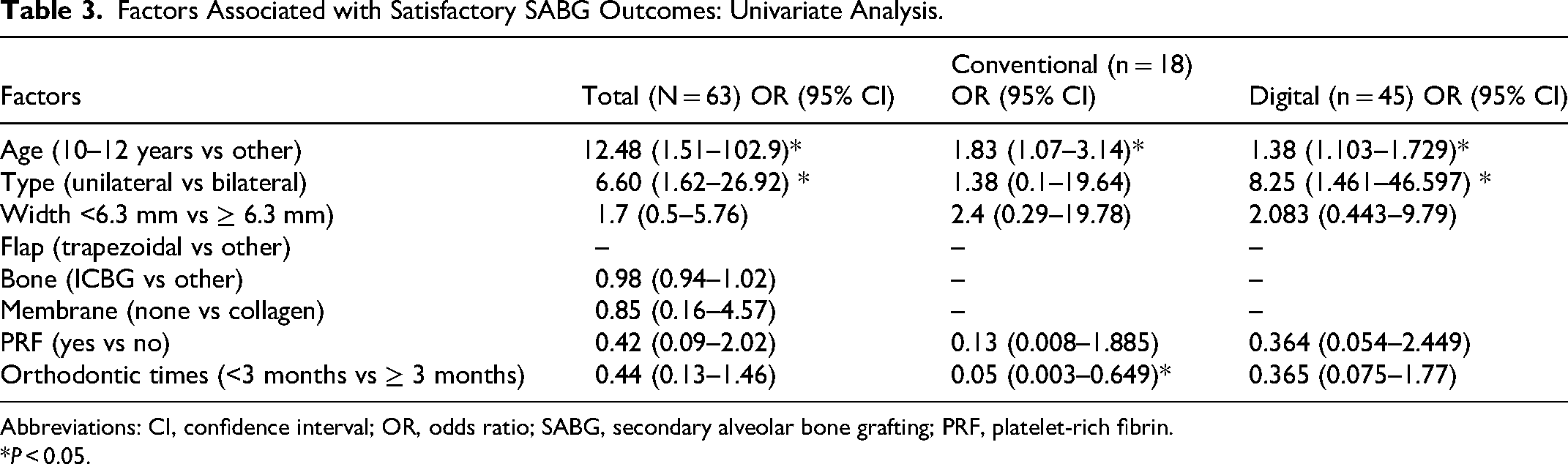
Abbreviations: CI, confidence interval; OR, odds ratio; SABG, secondary alveolar bone grafting; PRF, platelet-rich fibrin.
*P < 0.05.
Predictors of Secondary Alveolar Bone Grafting Success: Multivariate Logistic Regression
A multivariate model using backward stepwise elimination was constructed, initially encompassing 8 variables: age at grafting, cleft type, cleft width, surgical technique, bone graft type, membrane use, autologous growth factors, and orthodontic timing. In the final overall model, age and cleft type remained the primary significant predictors of success. Patients aged 10-12 years exhibited a 10.46-fold higher likelihood of success (adjusted OR [aOR]: 10.46; 95% CI: 1.22-89.52; P = 0.032), while unilateral clefts showed a 5.19-fold higher likelihood of success (aOR: 5.19; 95% CI: 1.15-23.42; P = 0.032) after controlling for confounding variables. This model accounted for 20.2% of the variance in SABG outcomes (Nagelkerke R2= 0.202).
Further analysis of the radiographic subgroups identified distinct primary predictors (Table 4). In the conventional group, the most significant predictor was the timing of orthodontic tooth movement (aOR: 0.05; 95% CI: 0.003-0.65; P = 0.023), explaining 31.3% of the variance. For the digital group, cleft type was the sole significant predictor (aOR: 17.01; 95% CI: 1.81-160.05; P = 0.013), which explained 30.2% of the variance in this specific subgroup.
Predictors of Satisfactory SABG: Multivariate Logistic Regression.
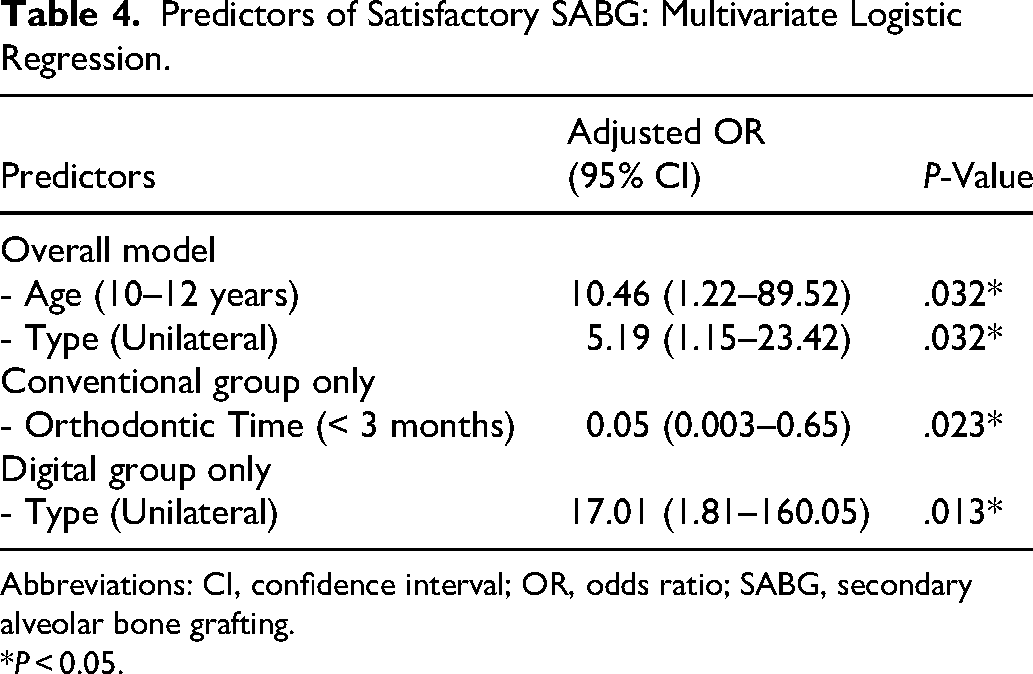
Abbreviations: CI, confidence interval; OR, odds ratio; SABG, secondary alveolar bone grafting.
*P < 0.05.
Discussion
The success of SABG is critical in patients with cleft lip and palate, as it corrects the defect to promote proper function and esthetics. There are various factors influencing the success of SABG. The factors affecting the success of alveolar bone grafting considered in this study include the age at bone grafting,17–19 the type11,20 and width of cleft,2,21 surgical techniques, 11 the type of bone used,10,22,23 the use of a membrane for stabilization, 24 autologous growth factors,25,26 and the orthodontic treatment time.12,13 Particularly, previous research has not extensively studied the orthodontic treatment time; however, it is deemed significant in determining the success of SABG. SABG remains a cornerstone in the comprehensive management of patients with cleft lip and palate, aimed at restoring both functional integrity and facial esthetics. The findings of the present study identify patient age and cleft type as the primary determinants of SABG success, while also revealing the significant role of orthodontic treatment timing, which is a factor that has been less extensively explored in previous literature. Furthermore, this study employed a composite scoring system integrating the Chelsea bone-bridge classification with quantitative bone density measurement and provided a direct comparison of conventional versus digital radiographic subgroups that identified modality-dependent predictors.
During the age range of 10-12 years, there is a higher chance of success in SABG compared to other age groups. Our results consensus that the optimal period for performing SABG is between 10 and 12 years of age.17,18 Performing the procedure during this window, typically before the eruption of the permanent maxillary canines, optimizes the environment for bone integration. As evidenced by Calvo et al (2014), the application of orthodontic forces during canine eruption facilitates more effective bone remodeling and stimulation than grafting performed after the tooth has already emerged. 27 Furthermore, cleft morphology was found to be a critical predictor, with unilateral defects exhibiting significantly higher success rates compared to bilateral cases. The increased surgical complexity of bilateral clefts, which are characterized by compromised blood supply and the need for more extensive soft tissue mobilization from both oral and nasal aspects, inherently elevates the risk of wound dehiscence and subsequent graft failure.3,11 These findings emphasize the necessity of detailed preoperative counseling for parents of children with bilateral defects, specifically regarding the potential need for revision surgeries in the premaxillary region. 20
An important observation in this study was the influence of orthodontic treatment timing, particularly within the conventional radiograph subgroup. While orthodontic timing is frequently overlooked in retrospective analyses, our multivariate model demonstrated it to be a significant predictor (P = 0.023) when using conventional films. This suggests that the duration between surgical intervention and the initiation of tooth movement may impact long-term graft stability. The variation in significance between the conventional and digital subgroups might also be attributed to the inherent differences in film properties and their impact on radiographic interpretation. Digital radiography systems offer a wider dynamic range and superior contrast resolution compared to conventional film, which likely enhanced the sensitivity of bone density measurements and facilitated a clearer identification of cleft morphology as a significant predictor in this subgroup.28,29 Despite these technological differences, the biological trend suggests that early and well-timed orthodontic intervention is beneficial across both modalities.
Regarding biological enhancements, the utilization of platelet-rich fibrin (PRF) and collagen membranes through guided bone regeneration (GBR) techniques showed favorable trends in maintaining grafted bone height.30,31 However, it is noteworthy that some cases involving PRF were associated with suboptimal soft tissue healing and scar formation. To mitigate this, we propose that PRF be prepared as a membrane and specifically applied along the nasal layer to improve soft tissue coverage and healing. Our data further suggest that the combination of GBR and collagen membranes is highly effective for unilateral clefts of appropriate dimensions. Future prospective studies should investigate whether the expansion of this technique to wider or bilateral clefts can yield comparable high success rates.
The strengths of this study lie in its practical applicability, utilizing routine 2D radiographs to provide a cost-effective and accessible composite scoring system for clinical practice. However, several limitations must be acknowledged. The retrospective design presented challenges in standardizing film quality and ensuring complete longitudinal data. Additionally, 2D imaging cannot assess the Bucco-lingual dimension of the bone graft, and the lack of calibration in some historical records could introduce measurement error. Nevertheless, the high intra-examiner reliability achieved (κ = 0.87) supports the validity and reproducibility of our scoring method. This is particularly relevant for orthodontic and community-based practices where cone beam computed tomography (CBCT) is not routinely available or justifiable; the proposed composite score allows clinicians to monitor graft outcomes during orthodontic treatment planning using standard periapical radiographs, minimizing both cost and radiation exposure.
Moving forward, the integration of 3-dimensional imaging, such as CBCT, would allow for a more precise evaluation of bone volume and quality. Future research should also incorporate intra-oral and extra-oral surface scanning to evaluate the esthetic outcomes of the maxillary arch and alar base symmetry. Clinically, our findings advocate for a standardized protocol that prioritizes intervention during the optimal age window of 10 to 12 years. In developing countries, empowering primary healthcare units to facilitate early referrals is essential for ensuring that cleft patients receive treatment during this critical period. Ultimately, while non-modifiable factors like cleft type pose inherent challenges, the clinician's role in optimizing modifiable variables such as age at grafting and orthodontic timing remains paramount for achieving successful long-term outcomes.
Conclusion
Age and cleft type significantly influence the success of SABG. Patients outside the ideal criteria should be informed preoperatively about the potential need for additional surgery to improve the treatment result.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261464276 - Supplemental material for Factors Related to the Outcomes of Secondary Alveolar Cleft Bone Grafting Using Two-Dimensional Radiographic Analysis: A Retrospective Study
Supplemental material, sj-docx-1-cpc-10.1177_10556656261464276 for Factors Related to the Outcomes of Secondary Alveolar Cleft Bone Grafting Using Two-Dimensional Radiographic Analysis: A Retrospective Study by Danaiya Supakanjanakanti, Wasinee Khetphan, Teepawat Witeerungrot, Kanokporn Santavalimp, Warintorn Puangcharoen and Pawornwan Rittipakorn in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
The authors would like to express their gratitude to the Faculty of Dentistry, Prince of Songkla University Hospital, for providing access to the medical records and radiographic data necessary for this retrospective analysis. We thank the clinical and administrative staff at the Faculty of Dentistry for their assistance in data collection. We also appreciate the guidance provided by the Human Research Ethics Committee and the support from the Thai Clinical Trials Registry. During the preparation of this manuscript, the authors used AI-based language tools, Claude (Anthropic, San Francisco, CA, USA), and Gemini (Google, Mountain View, CA, USA), to assist with language editing, improve readability, and check the logical flow and structure of the text. These tools were used in an assistive capacity only and did not contribute to the study design, data collection, analysis, interpretation, or conclusions. The authors reviewed and edited all output and take full responsibility for the content and integrity of the manuscript.
Ethical Approval and Informed Consent
This retrospective study was approved by the Human Research Ethics Committee of the Faculty of Dentistry, Prince of Songkla University (Approval Number: EC6512-045). The study was registered with the Thai Clinical Trials Registry (TCTR20240325001). As this was a retrospective study utilizing existing medical records, the requirement for informed consent was waived by the ethics committee.
Author Contributions
DS contributed to data collection, methodology, formal analysis, and writing—original draft. WK contributed to data collection and writing—original draft. TW contributed to data collection and validation. KS contributed to data collection. WP contributed to data collection. PR contributed to conceptualization, methodology, supervision, and writing—review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.