
Abstract
Objective
To determine the changes in felt needs of caregivers of children with cleft lip and/or palate (iCL/P) from first clinic presentation to first surgical intervention.
Design
Longitudinal observational study.
Setting
A tertiary hospital in Nigeria.
Patients, Participants
Caregivers of children with nonsyndromic CL/P (iCL/P) managed at a tertiary hospital in Nigeria from January 2023 to December 2024.
Intervention
Multiple semistructured counseling sessions.
Main Outcome Measures
Caregivers felt needs at time of first clinic presentation (T1) and at time of first surgical intervention (T2).
Results
Eighty caregivers, all mothers of children with iCL/P were included. Their mean age was 31.1 ± 6.24 years. At T1, information on etiology of iCL/P, surgical intervention, feeding and potential speech challenges were considered very significant needs. Feeding was also considered a primary concern for most participants. At T2, after counseling sessions, there was a statistically significant reduction in the proportion of caregivers who considered information on surgical intervention, improvement in family and community acceptance and improvement in clinical psychology as very significant needs, while potential speech challenge became the primary concern of most caregivers. Caregivers of children below 1 month of age were also found to have significantly higher felt needs compared to those with older children.
Conclusions
The waiting period between birth and first corrective surgery can be stressful for caregivers of children with iCL/P. Repeated counseling from first clinic visit to first surgical intervention may be beneficial to caregivers and should focus on the domains of needs highlighted in this study.
Introduction
The incidence of cleft lip and palate (CL/P) in Nigeria has been estimated to be about 0.5 in 1000 births, although worldwide this value is placed at 1:750 live births.1,2 Having a child with CL/P in a low-middle-income country (LMIC) has additional parental socioeconomic and psychological impact compared to high-income countries. A few studies3,4 have explored the quality of life of both the child and parents of children with CL/P specifically in the context of a country like Nigeria, with results showing that caring for a child with CL/P significantly reduces the quality of life of the caregivers in all domains. Delivering adequate information to the caregivers during counseling to address their needs and primary concerns is likely to have a significant impact on their ability to cope with taking care of the child.
Felt need/want is an individual's perception of his/her healthcare needs. 5 It may be defined as that quantity of medical service that people feel they ought to consume over a relevant period based on their own perception of their health needs. 6 Meanwhile, expressed need/demand is what patients ask for 5 while normative needs are what the clinician perceives the patient should need based on expert judgment and professional assessment. 6 Patients’ present to the hospital for different reasons, which in some cases may be at variance with what the clinician, in his/her expert opinion, perceives the patient needs and is paramount to the patient's well-being. For an individual to express satisfaction in services received at a health facility, there must be a strong convergence in felt need and the normative need of the patient.5,6
Clinicians are trained to diagnose and attend to the normative needs of their patients. 6 However, in cases of CL/P, which has been shown to be associated with psychological distress for the parents/guardian, attending to the felt need in addition to the normative need, may substantially improve the quality of life of the parents/guardian. This is especially important due to the delay between the birth of a child with CL/P and the first surgical intervention, which is usually at 3 months of age for the repair of the cleft lip, and 12 months of age for the cleft palate. This waiting period can be a time of considerable psychological distress for the parents, as the visible cleft of the lip and the functional nasal regurgitation from the cleft palate remain unrepaired. Hence, this waiting period is crucial to the psychological and emotional well-being of the parents and provides a window of opportunity for the cleft team to provide long-lasting support to reduce strain and anxiety.7,8 This is of particular importance in LMICs, where parents manage economic burdens from caring for a child with CL/P and societal stigmatization and discrimination ascribed to the condition. 9
However, the effectiveness of the support provided is based on the understanding of the needs of the parent, which have been shown in a study by Chuacharoen et al, 6 to vary at different times within the first 12 months of the patient's life. Major areas of need identified in their study included financial support, feeding of the child, information about surgery and speech. The study 6 also recommended parental counseling during the waiting period to address psychological and emotional stress associated with the delay. Also, Kuttenberger et al, 10 identified repetition of information provided as an important felt need among caregivers of children with CL/P, stating further that it would be helpful if all information were provided at one central place as opposed to multiple clinics during multidisciplinary cleft care. Their study 10 also recommended the provision of information on surgery, feeding and etiology of cleft during counseling sessions.
There are peculiar challenges to having a child with CL/P in a LMIC like Nigeria, these challenges include discrimination and stigmatization, inadequate widespread access to care, among others,9,11-14 and these peculiarities make our study population fundamentally different from the populations in other similar studies referenced above. Therefore, there is a need to identify the felt needs of parents of children with nonsyndromic cleft lip and/or cleft palate (iCL/P) in our environment and assess the evolution of these needs following counseling. With this in view, the objectives of this study were to determine the felt needs of caregivers of children with CL/P at first presentation before caregivers receive counseling, and to determine their felt needs at the time of first surgical intervention, to allow for an examination of the possible evolution of these needs following counseling.
Methodology
Study Design
This study was a longitudinal observational study without a control group conducted at the multidisciplinary cleft clinic of a tertiary hospital in Lagos, Nigeria. This study was approved by the institution’s Health Research and Ethics Committee, and informed consent was obtained from all study participants prior to enrollment into the study.
Participant Selection and Eligibility
The study participants were primary caregivers of children with CL/P who attended the hospitals’ multidisciplinary cleft clinic. The inclusion criteria were caregivers of children with iCL/P; aged less than 6 months, who had not received any prior counseling; with no prior surgical intervention for iCL/P; and caregivers consent to participate in the study. The exclusion criterion was caregivers of children with Tessier facial cleft or syndromic orofacial cleft. The study period extended from January 2023 to December 2024, and sample size was based on new patients attendance to the clinic within this study period.
Intervention
Intervention was semistructured counseling sessions conducted by a specialized team which included an oral and maxillofacial surgeon, a dietician, a social worker, and a registered nurse. These counseling sessions were independent, separate, and in addition to the general counseling performed by the cleft care team at the various cleft clinics at the study center: oral and maxillofacial surgery cleft clinic, pediatric cardiology cleft clinic, orthodontics cleft clinic, and ear, nose and throat cleft clinic. The decisions to conduct independent counseling sessions at a central location and to conduct counseling sessions at multiple timepoints were adopted from the recommendations of the study by Kuttenberger et al, 10 and Chuacharoen et al, 6 respectively.
The first counseling session was conducted at the participants’ first presentation to the orofacial cleft clinic. Subsequent counseling sessions were repeated monthly until the first surgical intervention. The counseling sessions were individualized and were delivered to each participant in a dedicated room at the cleft clinic during their visit. Counseling sessions were conducted after one of their cleft clinic appointments to avoid multiple trips to the study center and to avoid additional financial burden from participating in this study. All counseling sessions were conducted by the same team.
These counseling sessions involved 3 major topics:
Reassurance: Caregivers were reassured that the condition of their ward was manageable and they were encouraged to have a positive disposition towards treatment. Myths and beliefs on the etiology of the iCL/P condition were dissuaded and caregiver education on the predisposing factors of iCL/P was conducted.15,16
Management of iCL/P outcomes: caregivers were counseled on the potential challenges associated with feeding, growth, speech, hearing, dentition, and quality of life often seen in patients with iCL/P. 17 Caregivers were educated on the proper methods of feeding children with iCL/P. This included proper infant head positioning during breastfeeding (the head supported and positioned upright), frequency of feeding, and the use of specialized feeding bottles (eg, Haberman Feeder). Importance of routine checkups for early detection of potential complications was reiterated to the caregivers.
Multidisciplinary and multistage management: At the study center, the management of iCL/P involves the collaborative efforts of surgeons, nurses, dieticians, geneticists, pediatricians, cardiologists, orthodontists, pediatric dentists, and social workers.18,19 In addition, management of iCL/P involves multiple hospital visits with surgical and nonsurgical interventions spanning from less than 1 month of life (presurgical infant orthopedics) to adolescence (permanent dentition orthodontic treatment). Caregivers were counseled on the implications of this management plan in order to manage their expectations at every stage of treatment and encourage positive health-seeking behaviors and regular hospital visits.
Caregiver counseling was done at the first presentation at the cleft clinic. This counseling was repeated monthly until the first surgical intervention. The counseling was delivered by the same team members at every encounter, the nutrition counseling by the team registered dietician and was tailored to the child's need and growth progress, psychosocial counseling was delivered by the team social worker, and the general cleft childcare counseling was delivered by the team staff nurse, while counseling on treatment protocol and outcome expectations was delivered by the clinician. Counseling was individualized and was delivered to each participant in a dedicated room at the cleft clinic during their visit (Figure 1).
Method of Data Collection
Data was collected at 2 timepoints: first was at first presentation at the cleft clinic prior to any intervention, and second was 24 h before the first surgical intervention. Data collection was done using a 2-part interviewer-administered questionnaire, one for each time point.
The first part of the questionnaire, used at the first timepoint, included a section on sociodemographic characteristics such as caregivers age, religion, marital status, level of education, occupation, and age of child with iCL/P. The 3 categories of labor; unskilled, semi-skilled and skilled, according to Castillo, 20 were used to classify the occupation of participants. The questionnaire also included a section for the children with iCL/P: data on iCL/P characteristics and family history of cleft were collected. Data on caregivers’ felt needs was also collected.
Caregivers’ felt need was assessed using 8 questions, 7 on a Likert scale and one open-ended. The Likert scale section included questions on need for information on etiology of iCL/P, feeding, potential speech challenges, surgical intervention, improvement in family and community acceptance, psychosocial concerns with stigmatization, and financial support related to the care of their child with iCL/P. The open-ended question was a guiding question on the primary concern of caregivers in relation to children with iCL/P. The open-ended question allowed caregivers to express their own primary concerns not addressed with the Likert scale. Participants’ responses were then grouped into 6 categories of primary concern: feeding, speech, child physical appearance, family acceptance, finances, and undecided participants. These questions were extracted from the methodology of a similar previously published study by Chuacharoen et al. 6 A pretest of the questionnaire was conducted on 20 caregivers of children who had been treated for iCL/P at the same center. This was done to determine if the questionnaire tested for felt needs in accordance with the objectives of the study. The interviewer-administered nature of data collection plus changes made to syntax and context errors for clarity ensured the validity of the questionnaire.
The Likert scale ranged from 1 to 3, with 1 representing the lowest possible response (not a significant need) and 3 representing the highest possible response (very significant need). The total felt need score was calculated as the sum of the score for each felt need parameter. The minimum obtainable total felt need score was 7 and the maximum was 21. The mean total felt need score was calculated; participants with scores lower than the mean were classified as having low felt needs while participants with scores higher than the mean were classified as having high felt needs. This mean score was also used to determine low and high felt needs at the second time point.
The second part of the questionnaire, used at the second time point, collected data on the time elapsed between the first visit to the cleft clinic and the first surgical intervention, the age of the child with iCL/P at the time of first surgical intervention, the type of surgery, and caregivers’ felt need at the time of surgical intervention. Caregivers’ felt need was assessed using the same questions used at the first timepoint.
Statistical Analysis
Data entry, analysis and validation were performed using the IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, N.Y., USA). Descriptive analyses were conducted using frequency and proportions for categorical variables and mean and standard deviation, median and interquartile range for numerical variables. Kolmogorov–Smirnov test was used to test the normality of numerical variables, mean and standard deviation were used for normally distributed numerical variables while median and quartiles were used for numerical variables not normally distributed. Univariate analyses were conducted using Pearson's chi-square test, Fisher's exact test, and Mann–Whitney U test, where applicable, to test for the relationship between independent variables (sociodemographic characteristics, iCL/P characteristics, preoperative parameters, and timepoint) and dependent variable (caregivers’ felt need). A preset level of significance of P < .05 was adopted. The Spearman correlation coefficient was computed to determine the correlation between primary concern at timepoint 1 and primary concern at timepoint 2. Correlation coefficient r < 0.3 was considered as weak, > 0.3 to 0.5 as moderate, > 0.5 to 0.8 as strong, and > 0.8 as very strong positive correlation. Negative correlations were similar but with negative numbers. Probability values less than 5% conferred statistical significance.
Results
Participants
Parents/Caregivers: A total of 80 caregivers met the inclusion criteria during the study period and were included in the study. Their age ranged from 17 to 44 years with a mean age of 31.1 ± 6.24 years. All the caregivers who participated in this study were mothers and 76% (n = 61) were married, while 20% (n = 16) were single, and 3.8% (n = 3) were separated or widowed. Forty percent (n = 32) had tertiary level education, while 42.5% (n = 34) had secondary level education, and 17.5% (n = 14) had only primary level education. The categories of labor of participants were skilled (27.5%), semiskilled (57.5%), unskilled labor (1.3%), and unemployed (13.7%).
Children: The participants’ children had an age range of 7 days to 5.3 months with a mean age of 1.5 ± 1.34 months at first presentation. Fifty-five percent (n = 44) of the children were female. Children were mostly either the first (32.5%) or second (27.5%) of their parents’ children, in families that consisted mainly of 1 (30.0%) or 2 (30.0%) children in total. Only 7.5% (n = 6) of the children had a positive family history of orofacial cleft, which included mothers (2/6, 33.3%), fathers (1/6, 16.7%), siblings (3/6, 50.0%), cousins (1/6, 16.7%) and aunties (1/6, 16.7%). Forty percent (n = 32) of the children had cleft lip and alveolus only (iCLA), 28.7% (n = 23) had cleft lip, alveolus and palate (iCLAP), and 31.3% (n = 25) had cleft palate only (iCPO).
Surgery timing: For children with iCLA and iCLAP, (55/80, 68.7%), the time from first presentation to time of surgical intervention ranged from 21 days to 8.8 months, with a mean time of 3.3 ± 1.55 months. At the time of surgery, these children had an age range of 3 to 9 months, with a mean age of 4.7 ± 1.26 months. Surgical intervention was primary cleft lip repair. For children with iCPO, (25/80, 31.3%), the time from first presentation to surgical intervention ranged from 6.9 to 11.8 months, with a mean time of 10.3 ± 1.25 months. At time of surgery, these children had an age range of 11 to 13 months with a mean age of 12.1 ± 0.49 months. Surgical intervention was primary cleft palate repair. Table 1 shows the sociodemographic characteristics of participants according to the cleft diagnosis of their index child.
Sociodemographics According to Cleft Diagnosis.
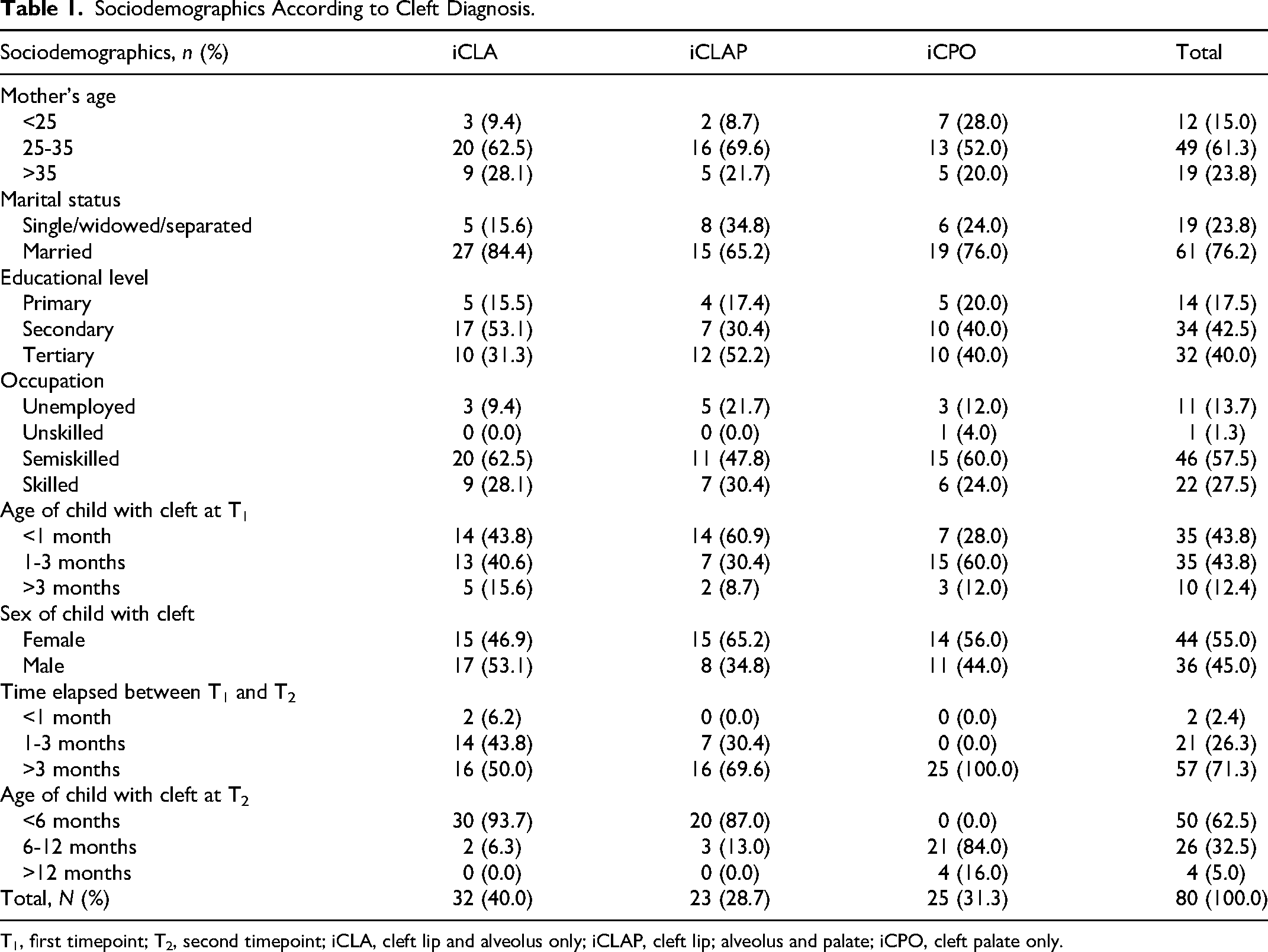
T1, first timepoint; T2, second timepoint; iCLA, cleft lip and alveolus only; iCLAP, cleft lip; alveolus and palate; iCPO, cleft palate only.
Felt Needs of Parents/Caregivers
Very significant needs at Timepoints 1 and 2: Table 2 shows the proportion of participants at Timepoints 1 and 2 (T1 and T2) who rated each felt needs item as a “very significant need.” For all felt needs parameters assessed, the proportion of participants who considered each need as very significant, reduced from T1 to T2. Specifically, there was a statistically significant reduction in the proportion of participants who considered information on speech challenges (T1:63.7%, T2:46.3%, U = 2629.5, P = .031), information on surgical management (T1:67.5%, T2:40.0%, U = 2244.0, P < .0001), improvement in family and community acceptance (T1:48.7%, T2:17.5%, U = 1877.0, P < .0001), and improvement in clinical psychology (T1:47.5%, T2:23.8%, U = 2291.0, P = .001) as very significant needs.
Caregivers’ Felt Needs at Timepoints 1 and 2.
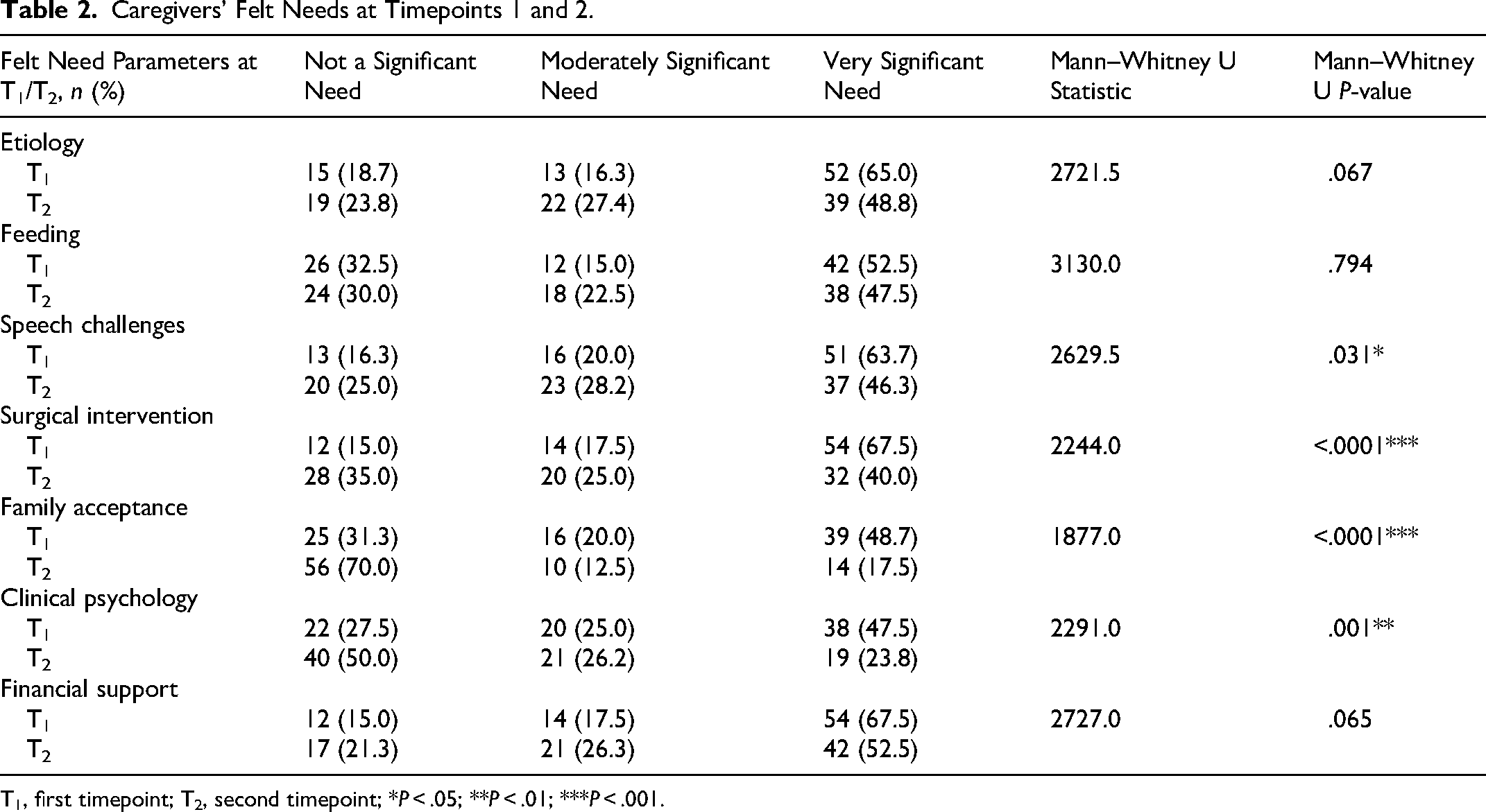
T1, first timepoint; T2, second timepoint; *P < .05; **P < .01; ***P < .001.
Total felt need at Timepoint 1 (T1): The minimum total felt need score at first presentation was 7 (2.5%), maximum score was 21 (22.5%), and mean score was 16.6 ± 4.05. Thirty-five (43.7%) participants had scores lower than the mean and were classified as having low felt needs while 45 (56.3%) participants had scores higher than the mean and were classified as having high felt needs. Table 3 shows the relationship between sociodemographics and caregivers' felt needs at T1. There was no statistically significant relationship between caregivers’ age, marital status, educational level, occupation, sex of index child, type of cleft of index child, and caregivers’ felt need scores at T1 (P > .05 for all associations). However, caregivers presenting with children less than one month of age had significantly higher felt need scores compared to caregivers who presented with older children (P = .011).
Sociodemographics and Caregiver's Felt Need Score at Timepoint 1.
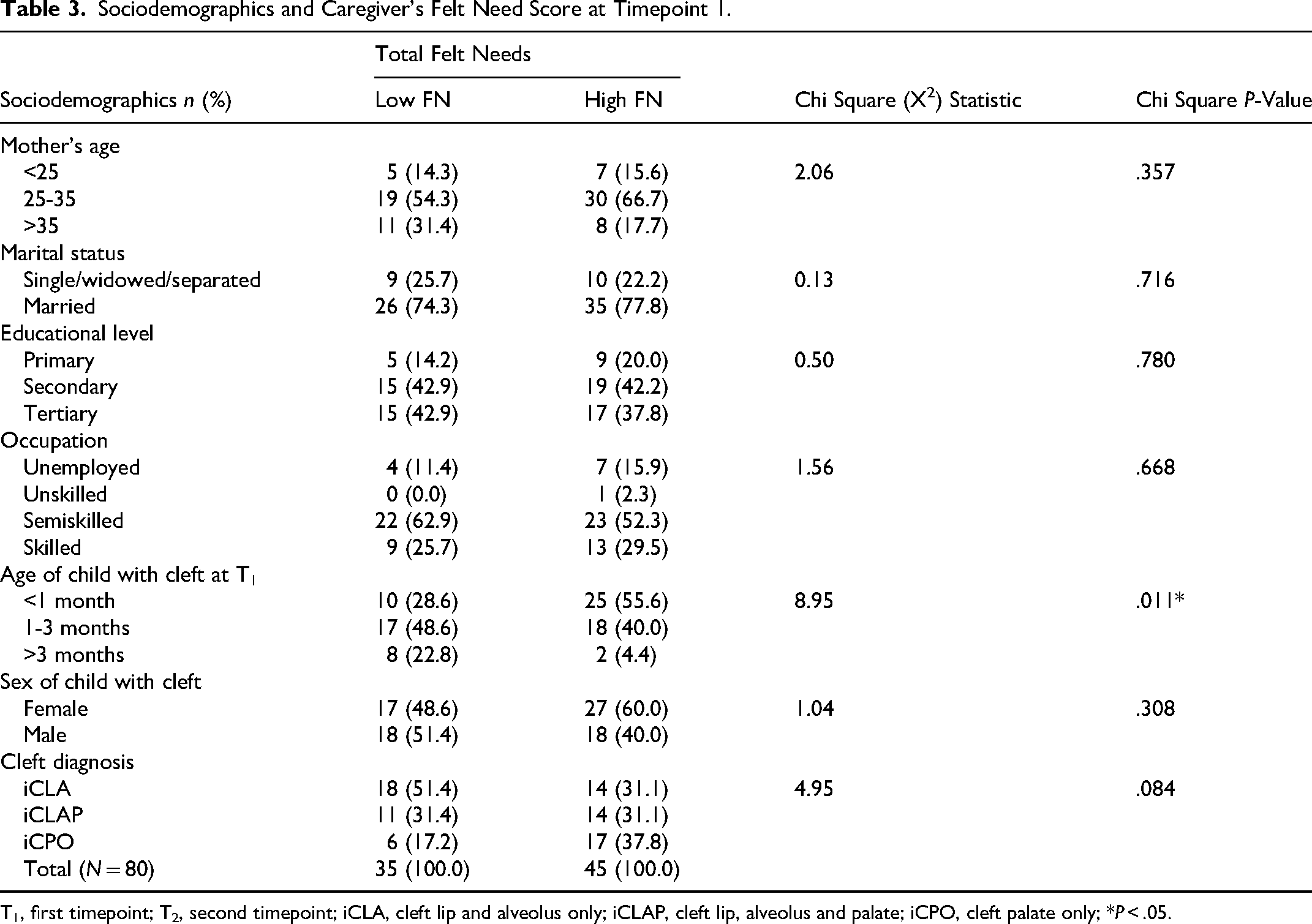
T1, first timepoint; T2, second timepoint; iCLA, cleft lip and alveolus only; iCLAP, cleft lip, alveolus and palate; iCPO, cleft palate only; *P < .05.
Total felt need at Timepoint 2 (T2): The minimum total felt need score after counseling sessions, 24 h before the first surgical intervention, was 7 (2.5%), the maximum score was 21 (6.3%), and the mean score was 14.2 ± 3.58. Fifty-nine (73.8%) participants had scores lower than the mean score from the first timepoint (16.6) and were classified as having low felt needs while 21 (26.3%) participants had scores higher than 16.6 and were classified as having high felt needs. There was no statistically significant relationship between time elapsed from time of first presentation to time of surgical intervention, patients’ age at the time of surgery, surgical intervention planned, and caregivers’ felt need at the second time point (P > .05 for all associations) (Table 4).
Preoperative Parameters and Caregiver's Felt Need Score at Timepoint 2.
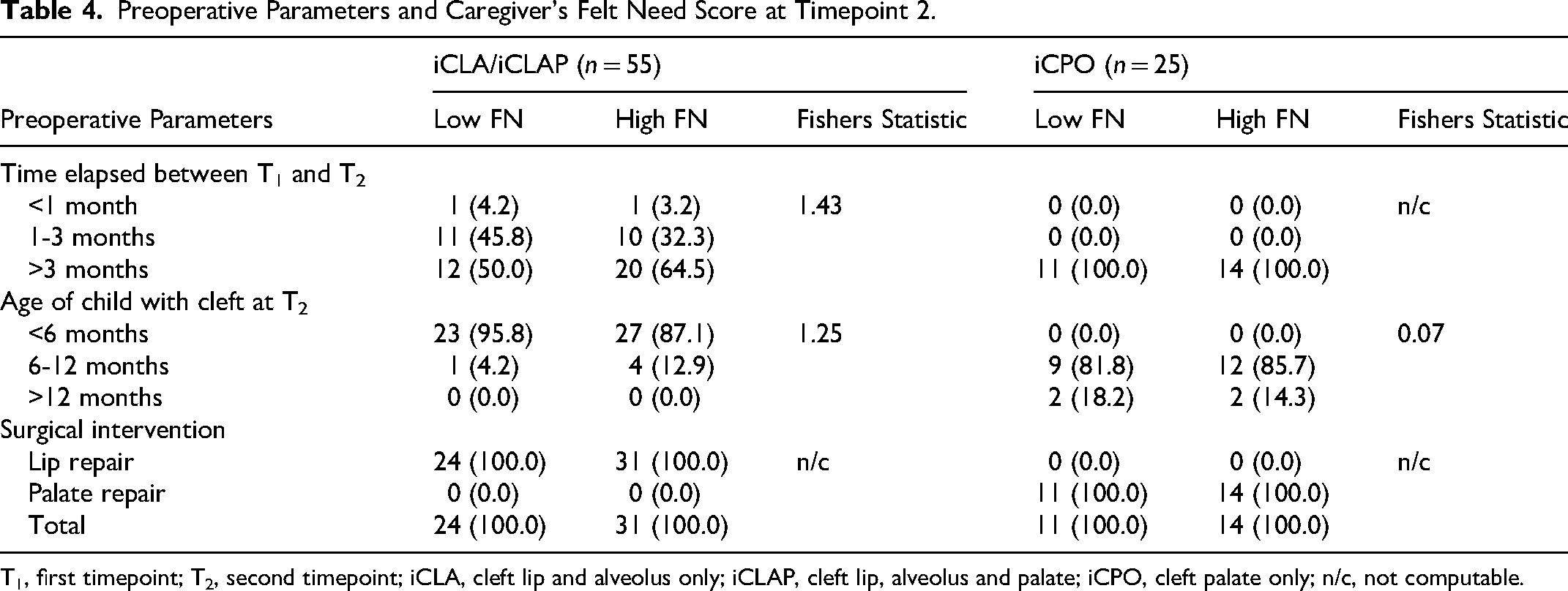
T1, first timepoint; T2, second timepoint; iCLA, cleft lip and alveolus only; iCLAP, cleft lip, alveolus and palate; iCPO, cleft palate only; n/c, not computable.
Primary concern at Timepoints 1 and 2 (T1 and T2): At both timepoints (T1 and T2), feeding (35% and 18.8%), speech (26.3% and 33.8%), child’s physical appearance (22.5% and 20.0%), and finances (8.8% and 21.3%) were the top 4 primary concerns reported by caregivers. Other responses included concerns regarding family acceptance (3.8% and 1.3%) and undecided primary concerns (3.8% and 5.0%). The proportion of caregivers who reported speech and finances as primary concerns increased from T1 to T2 while the proportion of caregivers who reported feeding, child physical appearance, and family acceptance as primary concerns and participants who were undecided decreased from T1 to T2. There was a weak, significant, positive correlation between feeding as a primary concern at T1 and at T2: the proportion of caregivers who reported feeding as a primary concern significantly reduced between the timepoints (rs (78) = .18, P = .020). Also, there was a weak, significant, negative correlation between finance as a primary concern at T1 and at T2: the proportion of caregivers who reported finance as a primary concern significantly increased between the timepoints (rs (78) = −.18, P = .027). Table 5 shows the correlation between primary concerns at timepoints 1 and 2.
Discussion
Correlation of Primary Concerns of Caregivers at Timepoints 1 and 2.
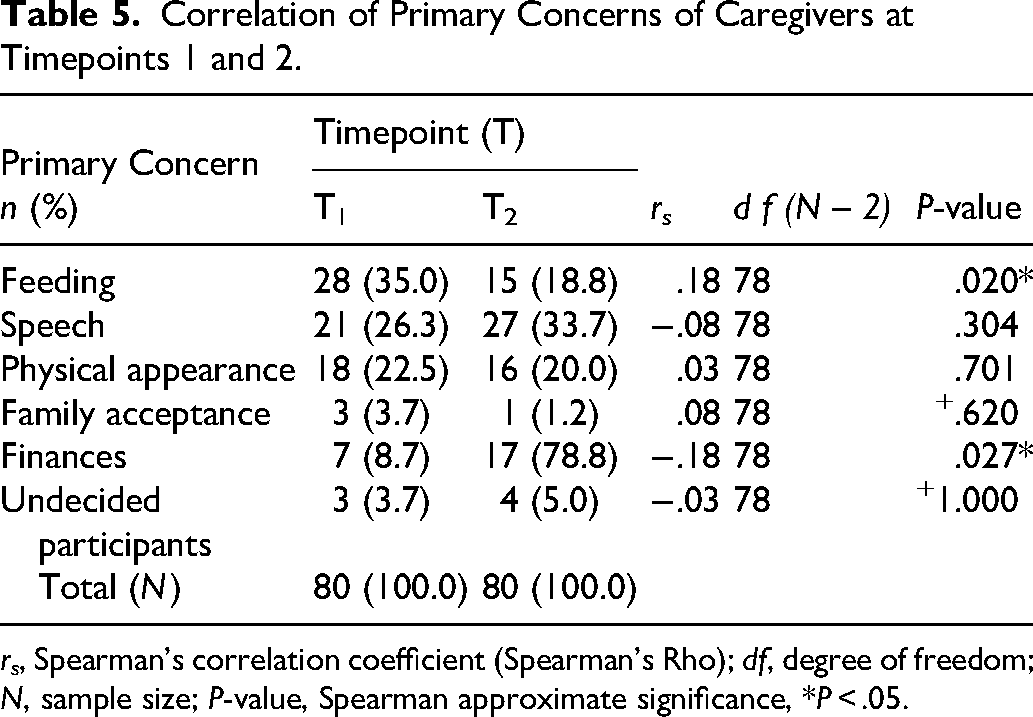
rs, Spearman's correlation coefficient (Spearman's Rho); df, degree of freedom; N, sample size; P-value, Spearman approximate significance, *P < .05.
In a multidisciplinary cleft care team aiming to deliver comprehensive cleft care, each team member has a contribution to the overall success of the management of the patient with a cleft. At the time of delivery of counseling and information to the parent, each discipline will present information aimed at a specific goal aligned with their specialty, as it should be; for example, the nutritionist goal is for the child to receive adequate nutrition in order to meet anthropometric growth milestones, the orthodontist goal is to achieve significant result measured by defect gap reduction from dentoalveolar molding and nasal recontouring as may be required. All the information delivered to the caregivers is based on the judged normative needs of the child from the perspective of the attending team member. There is considerable psychosocial pressure on parents of children with cleft, and this pressure is likely to drive their needs, which may not necessarily be in alignment with the needs being addressed by the cleft care team during counseling. In this study, we sought to identify the felt needs of the caregivers of children with cleft presenting to our facility and to examine the changes in these needs that may occur following counseling during the waiting period for definitive surgical intervention.
We found that information on the etiology of orofacial cleft was considered a significant need by two-thirds of the caregivers sampled, and this did not change significantly between the 2 time points. This is significant, as studies have shown that having a child with orofacial cleft in an LMIC is associated with significant discrimination and stigmatization, and myths surrounding the etiology of orofacial cleft are still persistent.11,13,14 It is understandable that a significant number of caregivers were interested in knowing if the condition was a result of something they did during pregnancy, as some may have experienced or be experiencing family and societal stigmatization.14,21-23 In contrast to our finding, the study by Kuttenberger et al, 10 conducted in Switzerland, which evaluated the needs and expectations of parents of children with cleft from the initial counseling received after the birth of the child, less than half (44%) of the respondents considered information on the etiology of the cleft as an important need of the parents to be addressed during the first counseling session after birth of the child.
About two-thirds of the participants considered information about the surgical repair of the cleft to be a very significant need at the first interview, however, this proportion reduced to about a third of the participants by the second interview, a statistically significant change. Also, just over 20% of the sample population considered the appearance of their child as their primary concern. The relatively high proportion of respondents who considered information about surgical repair significant at the first visit is not surprising as an orofacial cleft is a defect with significant esthetic and functional components, it is expected that information on the repair of the defect would be of significant priority to the caregivers. Corroborating our results, the report of the study by Kuttenberger et al, 10 showed that 80% of the parents in their study considered information about surgery as important and should be given during the initial counseling session. However, our result showing a statistically significant reduction in the proportion of caregivers who considered their need for information on surgical intervention for iCL/P as a very significant need between the first and second interview timepoints is in contrasts with the report of Chuacharoen et al, 6 a study conducted in Thailand to assess the felt needs of parents of children with cleft aged 0 to 3 months, they reported that the larger proportion of participants in their study population considered information on surgery to be very important at not just the first visit, but also at the second and third interviews, until after the surgical intervention.
Also, about two-thirds of respondents in our study considered information about financial support very important, and this proportion did not change significantly at the second timepoint. Although less than 10% of the sample population considered financial challenges their primary concern at the first timepoint, this proportion doubled by the second timepoint, which would most likely be because the caregivers are beginning to realize the real economic impact of taking care of their child. This is not surprising considering that in most LMICs where prenatal diagnosis is not the norm, the child's cleft is not identified until birth, resulting in an unanticipated additional financial burden to the household. Unpublished data from our group suggests that both direct (hospital fees) and indirect costs (time off work, cost of feeding, clinic visits, etc) can be a significant burden to these families. However, the relatively low proportion of participants who considered the financial burden of care as a primary concern may be attributed to the relieve experienced by this families from not having to pay out of pocket for hospital fees at our center, as the hospital fees and in some cases expenses related to associated care of these patients are sponsored by local and international non-governmental organizations, 18 and the caregivers are made aware of this from the time of first presentation.
About half of the participants in this study considered information on feeding to be very important at both the first and second interviews with no significant change, with about a third of the sample population considering it their primary concern at the first visit, which reduced significantly by the second interview. Similarly, Chuacharoen et al, 6 also reported that the most frequent aspect of need mentioned in their study in every period was information on feeding the child with a cleft. Also, more than 60% of respondents in the study by kuttenberger et al, 10 also considered information on feeding a child with a cleft as an important need of the parents that should be addressed at the first counseling session. The need for information and support by caregivers regarding feeding a child with orofacial cleft has been established in literature23-26 including in the population in which this current study was conducted.27,28 Issues around feeding and malnutrition are also considered a nominal need from the perspective of clinical care providers, especially as nutrition and weight gain affect the key anthropometric parameters used in the assessment of the patient for fitness for surgical intervention. Hence, various interventions have been developed to address this key concern of both caregivers and clinicians26,29,30 including advocating for the addition of a registered dietitian to the care team from first patient assessment to ensure the child consumes adequate macro and micronutrient intake, and to maximize growth and development. 31 Despite this, feeding remains a key concern for caregivers of children with cleft especially at the early stages of care as seen by the result of our study and that of Chuacharoen et al, 6 hence, clinical care providers should pay attention to clear delivery of information, and find effective ways of reinforcing this information, including practical intervention.
We found statistically significant reduction in the proportion of caregivers who considered their needs on improvement in family and community acceptance and improvement in need for psychological support as very significant needs between the first and second interview timepoints. The significant change in the need for family and community acceptance may be due to the African family structure where extended family members help parents of newborn babies in childcare within the first 3 to 6 months, hence it is likely that close relatives may have followed the parents for clinic visits and may have been present during counseling on need for family support, in addition, the visit of extended family members may have also exposed them to other cases at various stages of management, hence possibly positively altering their perception of the condition. Also, repeated exposure to counseling and interaction with other caregivers of children with cleft at various stages of management during clinic visits may have contributed significantly to the positive change seen in the felt need of the participating caregivers for psychological support.
There was no significant change in the proportion of those who considered potential speech challenges as a primary concern or who considered information on this concern as very significant between the 2 timepoints. The proportion of caregivers in this category tallies roughly with the proportion of caregivers with children diagnosed with CPO, although our result did not present a correlation, a limitation which we acknowledge, however, we may infer that this category of caregivers is more concerned with issues surrounding functional outcomes of intervention, as this can have a lasting psychosocial impact on both the child and the caregivers.
The use of a quantitative approach for data collection in this study may have hampered deeper exploration of the concerns and needs of the caregivers, however, the data presented in this study provides a basis for future exploration. Also, the perspective of the clinical care providers on the nominal needs of the patients and caregivers was not sought, this would have been valuable data to gauge the gap that may exist between caregiver expectations and service delivery. Although this study did not record attrition or missing data throughout the study period, the longitudinal nature of the study could have resulted in participants adapting to the conditions of their children which may have affected their reported felt need at the second timepoint. Also, the increase in financial concerns of caregivers from the first to the second timepoint may suggest a pertinent need for financial support for caregivers of children with CLP as multiple counseling sessions may not be a sufficient substitute. Lastly, this study did not examine the impact of the various elements of counseling on felt needs to determine what aspects were therapeutic and not just informative. It was therefore not possible to determine if counseling had any impact on felt need changes, or if the same changes would have been seen in families that did not receive counseling.
Conclusion
In conclusion, data from this study have provided a unique perspective into the felt needs of a population of primary caregivers of children with iCL/P in a LMIC, showing similarities with other population groups on needs surrounding information on feeding and surgical intervention, and notable differences in the need for information on etiology, functional outcomes of repair, family and community acceptance. Caregivers presenting with children with iCL/P below 1 month of age were also found to have significantly higher felt need than those presenting with older children. Our result provides preliminary data that will be useful in tailoring counseling of caregivers of children with iCL/P in LMIC, to address their peculiar felt needs and concerns. Further in-depth exploration of this subject using methodologies which will allow caregivers to better express their primary concerns would be beneficial, in addition to studies identifying the gaps between felt needs and normative needs.
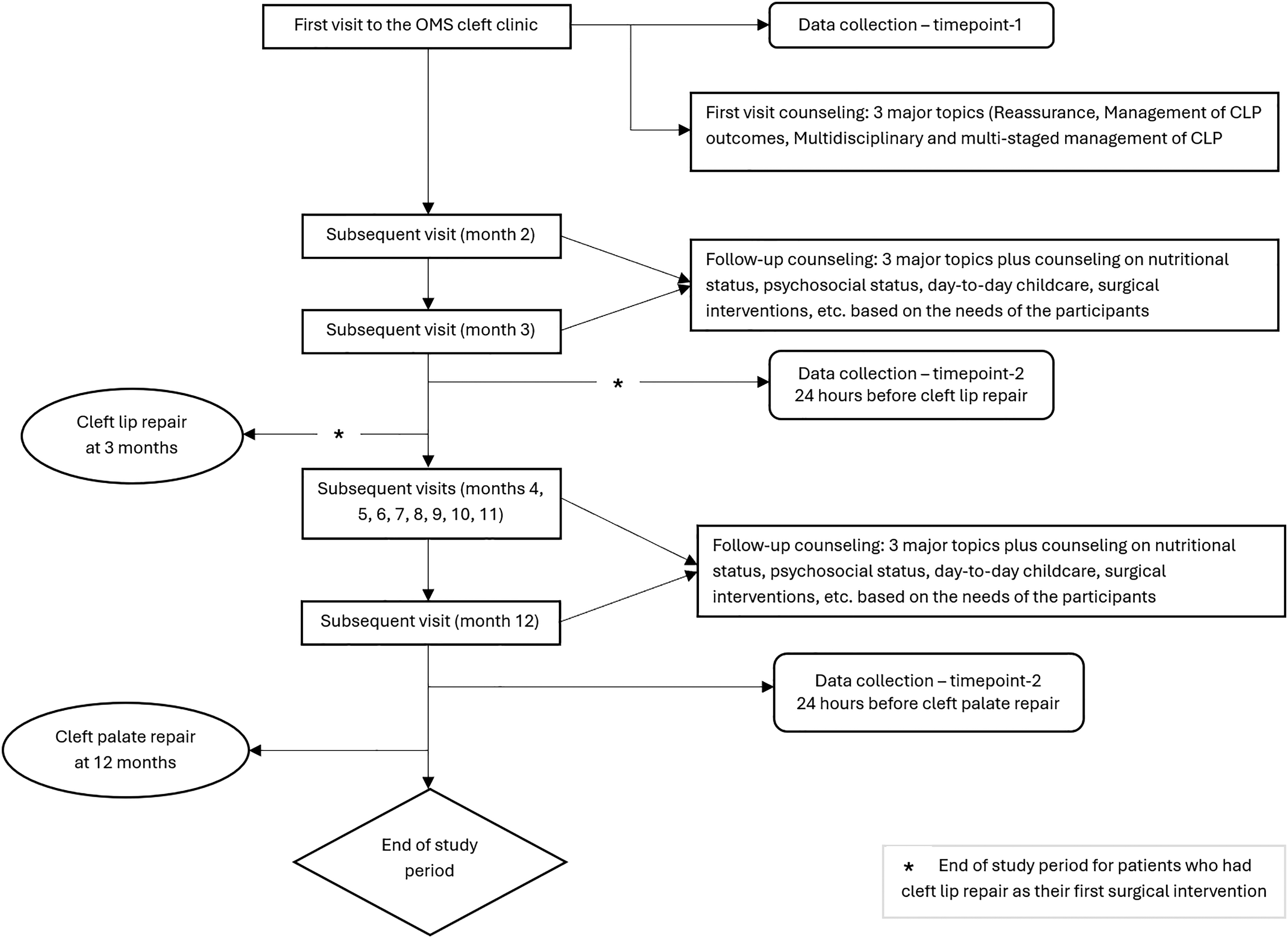
Flow chart.
Footnotes
Acknowledgments
Our sincere appreciation to all caregivers who participated in this study.
Ethical Considerations
This study was approved by the Health Research Ethics Committee of the institution (ADM/DSCST/HREC/APP/5259).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.